
Abstract
Speidel, Victor, Jan Christoph Purrucker, and Katarína Klobučníková. Manifestation of intracranial lesions at high altitude: case report and review of the literature. High Alt Med Biol. 22:87–89, 2021.—A 32-year-old man trekked to the South Everest Base Camp (5,364 m) in Nepal. On the last day of the ascent, he noticed some dysesthesia in his right leg and descended by helicopter. He suffered a generalized seizure shortly after his descent, followed by right-sided hemiparesis and speech arrest. Without the possibility of cerebral imaging, the patient was given dexamethasone intravenously who showed a marked improvement and regained the ability to speak. Magnetic resonance imaging later revealed a lesion in the left frontotemporal region with compression of brain parenchyma and minimal paralesional edema. A meningioma was later surgically resected. Although seizures are a common first manifestation of meningioma, we argue that the exposure to high altitude may have contributed to his symptoms, either by increasing the peritumoral edema by pathophysiology similar to high-altitude cerebral edema (HACE) or lowering the seizure threshold otherwise. This case shows a before unknown pre-existing condition becoming symptomatic at high altitude and illustrates the necessity for careful and immediate evaluation of every patient with new onset of unexplained focal neurological deficits or seizures at high altitude in addition to unspecific neurological symptoms commonly associated with HACE such as headaches, dizziness, lightheadedness, or ataxia.
Introduction
High-altitude cerebral edema (HACE) has been defined as a condition occurring in persons who have recently arrived at high altitude, usually secondary to acute mountain sickness or high-altitude pulmonary edema, and marked by disturbances of consciousness that may progress to deep coma, psychiatric changes of varying degree, confusion, and ataxia of gait (Hackett and Roach, 2004). However, global encephalopathy rather than focal findings characterizes HACE. Drowsiness is commonly followed by stupor while seizures are rare (Hackett and Roach, 2001).
Only scarce data exist about the manifestation of pre-existing brain lesions at altitude, a review of the literature showed a series of three cases of unknown pre-existing intracranial tumors, two cases of meningioma, and one malignant astrocytoma, suddenly becoming symptomatic at 3,000–4,000 m above sea level (Shlim et al., 1991). Another report describes the case of a benign subarachnoid cyst believed to be responsible for diplopia and ataxia at 4,200 m (Hackett, 2000). The lowered atmospheric pressure during commercial air travel has also been implicated in the manifestation of intracranial lesions (Zrinzo et al., 2006).
Case
A 32-year-old man in good health traveled from Slovakia to Lukla, Nepal (2,845 m), for a trek to the South Everest Base Camp (5,364 m). He did not take acetazolamide or other drugs during his trip. On the 8th day of the ascent, he noticed some dysesthesia in his right leg, self-medicated with low molecular weight heparin but was still able to complete the 8.5 km walk from Lobuche (4,940 m) to Base Camp. He sought treatment at the Everest Base Camp Clinic, operated by the Himalayan Rescue Association (Némethy et al., 2015). Physical examination revealed a right thigh painful upon palpation and he was advised to evacuate to Kathmandu for further evaluation of a possible deep vein thrombosis. The patient returned to Lukla by helicopter where he suffered a generalized seizure, followed by right-sided hemiparesis and speech arrest and presented to Pasang Lhamu Nicole Niquille Hospital in Lukla.
The examination showed normal eye movement and pupil reaction, no meningism but spontaneous tongue deviation to the right. Sensibility to touch was reduced on the right side of his body with marked impairment of motor function (upper right extremity 2/5, lower right extremity 1/5). Babinski reflex was negative bilaterally. The patient was evaluated as 11/15 on the Glasgow Coma Scale (GCS; E4, V1, M6) and 17/42 on the National Institutes of Health Stroke Scale (NIHSS).
Without the possibility of cerebral imaging, the patient was given 8 mg of dexamethasone intravenously and admitted for observation since nightfall prevented further transport.
Meanwhile, the patient showed a marked improvement 45 minutes after his arrival at the hospital with GCS assessed at 15/15 and NIHSS at 5/42. His condition deteriorated again 7 hours later before he was airlifted to Norvic International Hospital in Kathmandu (1,400 m) in the morning.
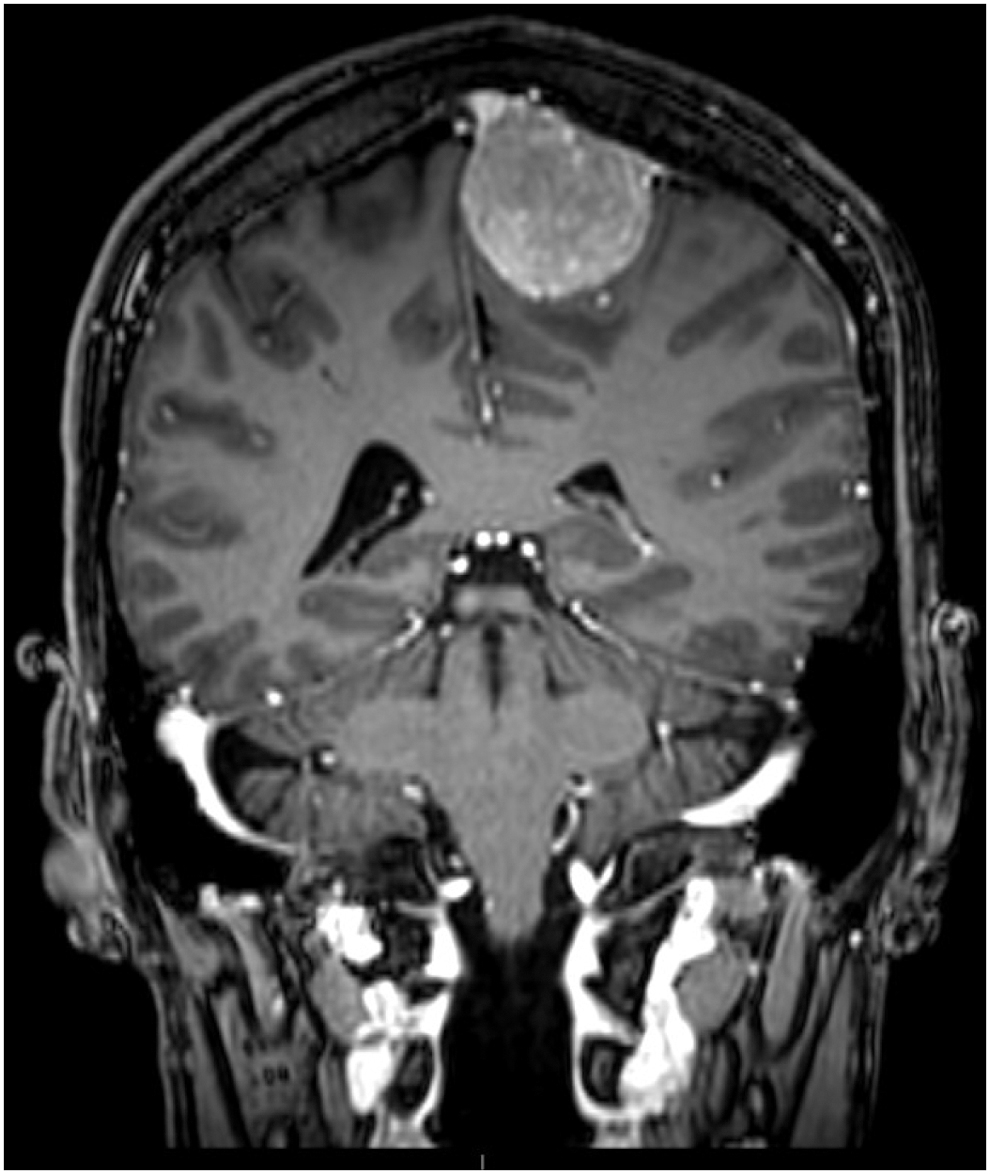
Gadolinium-contrast magnetic resonance imaging (Figs. 1 and 2) on the same day revealed an extra-axial enhancing dural-based lesion in the left parafalcine frontotemporal region with compression of adjacent brain parenchyma and minimal paralesional edema, suspicious of meningioma. There was evidence of mild slowing in the left frontal leads with an otherwise normal electroencephalogram, consistent with the lesion found in the magnetic resonance imaging (MRI). Persisting weakness of the right side of the patient's body was reported. He was discharged with a treatment of levetiracetam, dexamethasone, clonazepam, paracetamol, and esomeprazole and repatriated by air ambulance to Bratislava Comenius University Hospital in Slovakia. The meningioma was resected surgically followed by the evacuation of an epidural hematoma 3 days later. The hemiparesis had persisted up until the surgery and improved significantly during the postoperative period. The patient was discharged with a medication of levetiracetam and lamotrigine. He regained full motor function after 3 months and remains asymptomatic 2 years after the operation.
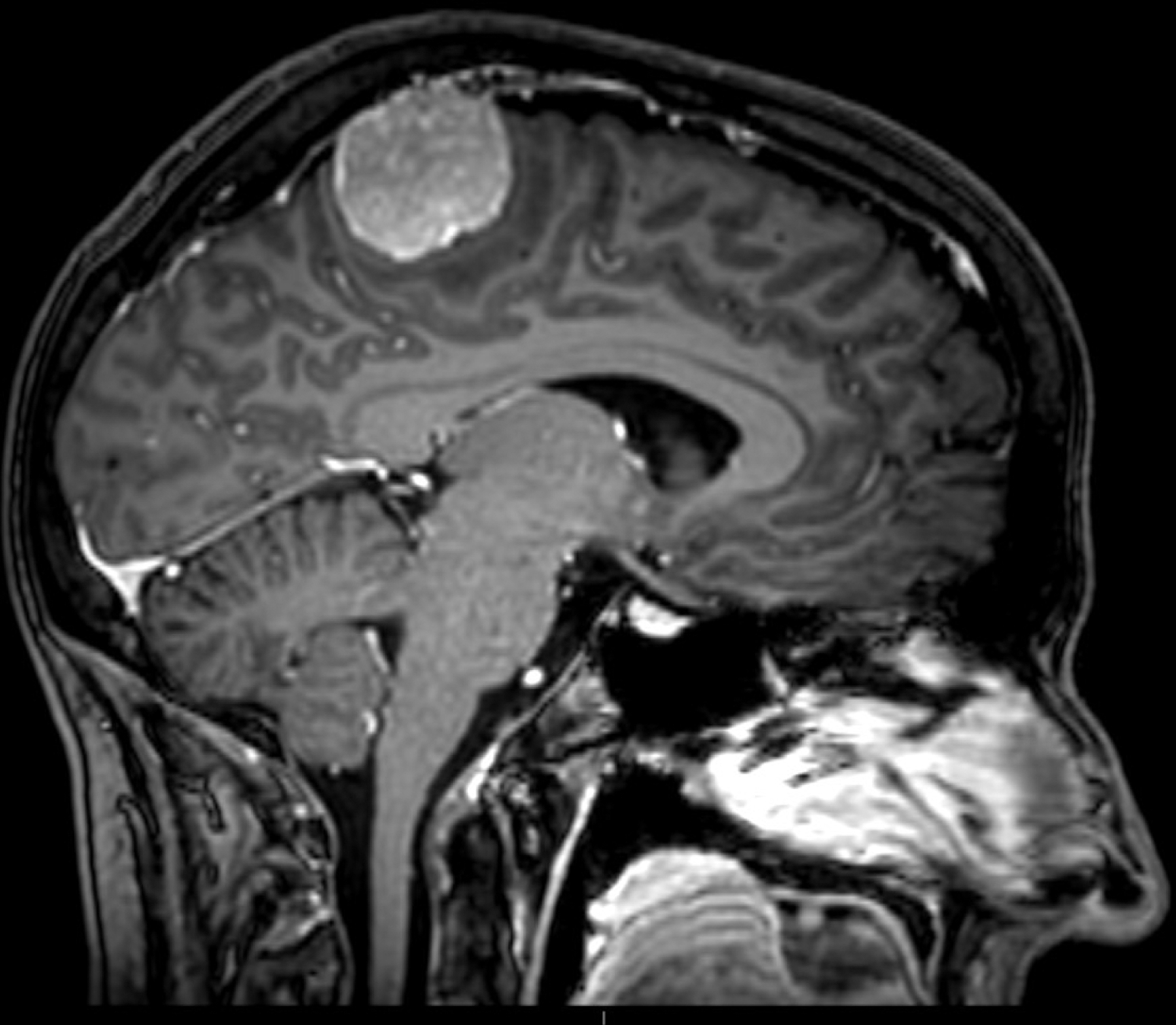
The patient's magnetic resonance imaging shows a dural-based lesion with some degree of mass effect but only limited peritumoral brain edema. The typical neuroimaging features of high-altitude cerebral edema including white matter changes, corpus callosum involvement, or diffuse microhemorrhages are not present.
The patient's magnetic resonance imaging shows a dural-based lesion with some degree of mass effect but only limited peritumoral brain edema. The typical neuroimaging features of high-altitude cerebral edema including white matter changes, corpus callosum involvement, or diffuse microhemorrhages are not present.
Discussion
It cannot be excluded that the seizure and associated symptoms developed solely due to the meningioma and peritumoral brain edema (PTBE) and that the altitude exposure played no role in the pathogenesis in this patient, however suggestive the timing of this first manifestation might seem. We believe the absence of significant PTBE seen in the MRI to represent the effect of treatment with dexamethasone and descent of ∼4,000 m before imaging.
The dysesthesia in the patient's leg at his first examination might have been a symptom of a focal seizure with secondary generalization.
Reports suggest that hyperventilation at altitude may trigger new epileptic seizures in the absence of acute mountain sickness or HACE (Daleau et al., 2006) or in patients with otherwise medically controlled epilepsy (Basnyat, 2001). The available evidence, however, for high-altitude–provoked seizures is observational and anecdotal but neither HACE nor intracranial lesions have been commonly found in these cases (Maa, 2011).
Conclusion
This case illustrates the necessity for careful and immediate evaluation of every patient with new onset of neurological symptoms at high altitude. The symptoms described in this case such as focal neurological deficits and seizures do not commonly occur in HACE and warrant further investigation.
The diagnosis and treatment of neurological disorders at high altitude remain a challenge and while the incidence of high-altitude illness is high, other pathologies must be taken into consideration. This case shows the additional possibility of an unknown pre-existing condition manifesting itself due to the exposure to high altitude.
We believe patients with intracranial lesions to be at an increased risk of developing PTBE and seizures at altitude. Patients with known lesions should, therefore, receive additional information about risks and management of cerebral edema or avoid ascending to higher altitudes altogether.
Footnotes
Acknowledgments
The authors thank the patient for his permission to publish this case and for providing them with all medical records.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was