
Abstract
Wang, Man, Mengxue Liu, Jia Huang, Dan Fan, Shengzhong Liu, Tao Yu, Keli Huang, Xinchuan Wei, and Qian Lei. Long-term high-altitude exposure does not increase the incidence of atrial fibrillation associated with organic heart diseases. High Alt Med Biol. 22:285–292, 2021.
Background:
Atrial fibrillation (AF) is one of the most common arrhythmias and is associated with several complications following cardiac surgery. However, the differences in the incidence of AF associated with organic heart diseases between highland and lowland populations have not been comprehensively studied.
Methods:
In this retrospective study, a total of 2,316 highland and lowland patients who underwent cardiac surgery between January 2013 and December 2018 in a single center were enrolled. According to the altitude of residence, patients were divided into high-altitude (>1,500 m) and low-altitude (<1,500 m) groups. A propensity score matching analysis was performed to estimate the association of lifetime high-altitude exposure with AF.
Results:
Among the enrolled patients, 239 (10.9%) were from a high-altitude plateau, while 1,946 (89.1%) were from a low-altitude area. There were statistical differences in age, gender, European System for Cardiac Operative Risk Evaluation, and other factors, between the two groups (p < 0.05). According to the propensity score, 237 patients in the high-altitude group were successfully matched to 237 patients in the low-altitude group without significant difference in baseline data (p > 0.05). Among the matched patients, 125 patients (26.4%) suffered from AF, with 66 (27.8%) in the high-altitude group and 59 (24.9%) in the low-altitude group. The incidence of AF was statistically similar between the two groups and not significantly influenced by long-term high-altitude exposure (odds ratio 1.07; 95% confidence interval 0.71–1.60, p > 0.05).
Conclusion:
Long-term high-altitude exposure did not significantly increase the occurrence of AF in patients with organic heart diseases. Clinical Trial No. ChiCTR1900028612
Introduction
Atrial fibrillation (AF) is the most prevalent sustained cardiac rhythm disorder seen in clinical practice (Furberg et al., 1994). AF has now developed into a global epidemic, driven by a large and growing number of cases. According to epidemiological investigations, the current estimated prevalence of AF in Asia is ∼0.4%–1.9%, with higher prevalence observed in Australia, the United States, and Europe (1%–4%) (Zulkifly et al., 2018).
AF is a risk factor in many diseases, increasing the risk of stroke, heart failure, and patient mortality (Wolf et al., 1978; Benjamin et al., 1998; Wang et al., 2003). The symptoms of AF in organic heart disease are severe. When the ventricular rate is >150 beats/minutes, it can induce angina pectoris and mitral valve stenosis in patients with coronary heart disease, acute pulmonary edema in patients with pre-existing cardiac dysfunction, and acute heart failure (Staerk et al., 2017). Functional tricuspid insufficiency with a structurally normal tricuspid may be secondary to chronic AF (Utsunomiya et al., 2017).
Understanding the pathogenesis of AF is of great significance for the clinical treatment of AF. Studies have found that exposure to high altitude is proarrhythmic and could potentially contribute to an increased risk of sudden cardiac death (Woods et al., 2008; Burtscher and Ponchia, 2010). Acute exposure to high altitude can cause acute hypoxia, leading to increased sympathetic excitability (Hansen and Sander, 2003). Interestingly, this excitability continues for a period of time after leaving the high-altitude environment, while people who live in high-altitude areas show lifelong sympathetic activation (Lundby et al., 2018). Overactivation of the sympathetic nervous system is a primary induction mechanism of AF (Choi et al., 2017). However, arterial remodeling is also an important mechanism for AF and studies have found that high-altitude exposure in lowlanders causes persistent impairment in vascular function (Lewis et al., 2014).
Yet differences in AF incidence rates between residential highlanders and lowlanders have not been comprehensively studied. This study sheds new light on AF by comparing incidence rates between people living at high altitude and people living at low altitude. This new research direction may be able to further elucidate the pathogenesis of AF. We hypothesized that a high-altitude environment could increase the risk of AF and mortality after routine cardiac surgery in Chengdu, a plain metropolis in Sichuan Province, China, which is adjacent to the Qinghai-Tibet high-altitude plateau. The objective of this study was to examine the association between high-altitude environment and the risk of AF with the first use of a propensity score-matched analysis.
Methods
Study population and data collection
With the approval of the Institutional Review Committee, 2,316 consecutive patients who underwent cardiac surgery from January 2013 to December 2018 in Sichuan Provincial People's Hospital were retrospectively reviewed. The database was established to investigate the relationship between high-altitude exposure and the occurrence of AF associated with organic heart diseases, as well as the mortality and morbidity after cardiac surgery. Exclusion criteria were patients with incomplete baseline (n = 131). A total of 2,185 patients were enrolled.
Demographic, preoperative, intraoperative, and postoperative data were collected from an electronic medical record database.
Definition of high-altitude cases
The patient's address of residence was available from an electronic medical record database. We obtained the corresponding altitude of the address region according to Google satellite area. The patients born in high-altitude areas with household registration were classified into the highlanders group. All participants in the highlanders group were born and permanently residing at high-altitude between 1,500 and 5,000 m (mean ± standard deviation [SD] 2,477.18 ± 719.10 m). The patients who were born and lived close to sea level (<1,000 m) and had not been to high altitude for >2 weeks were classified in the lowlanders group. Individuals born in low-altitude areas, but living in high-altitude areas after adulthood were excluded.
Outcome assessment
Preoperative AF was defined as AF occurring before cardiac surgery, based on documentation of AF episodes lasting ≥30 seconds during continuous telemetry throughout hospitalization, as assessed by electrocardiography (ECG), Holter, or event monitors. Survival status was obtained from review of medical records.
Statistical analysis
Data were analyzed using SPSS 22.0 software and propensity score matching was performed using the SPSS 22.0 PS matching plug-in. Continuous variables following a normal distribution are expressed as mean ± SD. To control for possible skew, data were compared by using the Wilcoxon rank-sum test. The Mann–Whitney U test was used to compare medians. Categorical variables were presented as counts with percentages and compared using the χ2 or Fisher exact test, where indicated. Multiple regression binary logistic regression, with a backward stepwise method, was performed to evaluate the relationship between high-altitude environment and the occurrence of AF. Significance was set at 0.05. Data are presented as odds ratios (ORs) with 95% confidence intervals (CIs).
Propensity score matching
To reduce the potential for imbalance in baseline covariates, propensity score matching was used to control for differences in baseline characteristics of patients. Each highlander was matched to a patient living in a lowland area based on propensity score without replacement using the greedy matching protocol with a fixed caliper width of 0.02. After matching, we assessed balance within the matched pairs using the standardized differences in covariate means and proportions. The absolute standardized differences for all baseline variables were <10%, indicating acceptable balance. Adjusted variables were age, sex, body mass index, and European System for Cardiac Operative Risk Evaluation (Euro SCORE).
Results
Patient characteristics
Baseline characteristics and surgical procedure details of the 2,185 patients enrolled are shown in Table 1. The mean (SD) age of the study cohort was 46.6 (16.9) years and 58.1% were female. Among them, 829 patients (37.9%) exhibited rheumatic heart disease, 468 patients (21.4%) exhibited non-rheumatic valve disease, 523 patients (23.9%) exhibited congenital heart disease, 148 patients (6.8%) exhibited coronary heart disease, 72 patients (3.3%) presented with aortic dissection, and the remaining 6.7% exhibited valvular heart diseases with other heart diseases.
Baseline Characteristics of the 2,185 Study Patients and Propensity Score Matching
AF, atrial fibrillation; ASA, American Society of Anesthesiologists classification; BMI, body mass index; CABG, coronary artery bypass grafting; NYHA, NEW York Heart Association classification; SD, standard deviation; TV, tricuspid.
Matched cohort
Propensity score matching matched 237 patients 1:1 between high-altitude (n = 239) and low-altitude (n = 1,946) patients based on similar propensity scores. Figure 1 shows that the 237 people came from different altitudes, among which the total number of people with an altitude of more than 2,500 accounted for 44.3%. The specific components used to estimate the propensity score along with a description of their distributions are shown in Table 1. The standardized differences of all covariates before and after matching are shown in Table 2. After propensity score matching, no statistically significant baseline characteristics between the highlander group and lowlander group were observed.

The percentage of people with different altitudes in the matched population.
Comparison of Standardized Differences Before and After Propensity Score Matching
Surgical data and surgical complications
After matching, surgical data, such as cardiopulmonary bypass (CPB) duration (126.06 ± 59.5 vs. 113.79 ± 47.03 minutes; p = 0.029), aortic cross-clamping time (81.59 ± 43.34 vs. 73.56 ± 37.45, p = 0.038), and the rate of automatic heart resuscitation (87.3% vs. 82.7%); p = 0.004) did differ between lowland and highland patients. The rate of postoperative complications, apart from the incidence of postoperative surgical reentry into the intensive care unit (ICU) (0.8% vs. 5.1%; p = 0.006), did not differ significantly, including the prevalence of postoperative surgical re-exploration for bleeding (1.3% vs. 3.0%; p = 0.169), re-ventilation (1.3% vs. 2.1%; p = 0.362), renal dialysis (2.1% vs. 2.5%; p = 0.500), and postoperative AF (26.2% vs. 27.4%). However, the postoperative mortality rate in the matched cohort was 7.2%, and did differ significantly between the two groups (3.0% vs. 7.2%, p = 0.029; Table 3).
Comparison of Outcomes Between the Lowlander and Highlander Groups Following Propensity Score Matching
CPB, cardiopulmonary bypass; IABP, intra-aortic balloon pump; ICU, intensive care unit.
Comparison of patient outcomes
Among the 2,185 subjects in the study, 719 (32.9%) developed AF before surgery. In the propensity-matched cohort, the overall incidence of AF was 27.2%. Cohort analysis revealed that AF occurred more frequently in the high-altitude group (27.8% vs. 26.6%; Fig. 2), but there was no statistically significant difference between the high-altitude group and the low-altitude group (p = 0.418). Patients living at high altitudes were just as likely to develop AF as those who did not live at high altitudes (unadjusted hazard ratio, 1.07; 95% CI, 0.71–1.60; Fig. 3). Lifetime high-altitude exposure did not influence the risk of AF. Females were more likely to develop AF than males (unadjusted OR, 1.664; 95% CI, 1.067–2.596). Additional risk factors were age and NEW York Heart Association (NYHA) classification (Fig. 4).

The difference of incidence of AF in different altitude groups before and after matched. AF, atrial fibrillation.
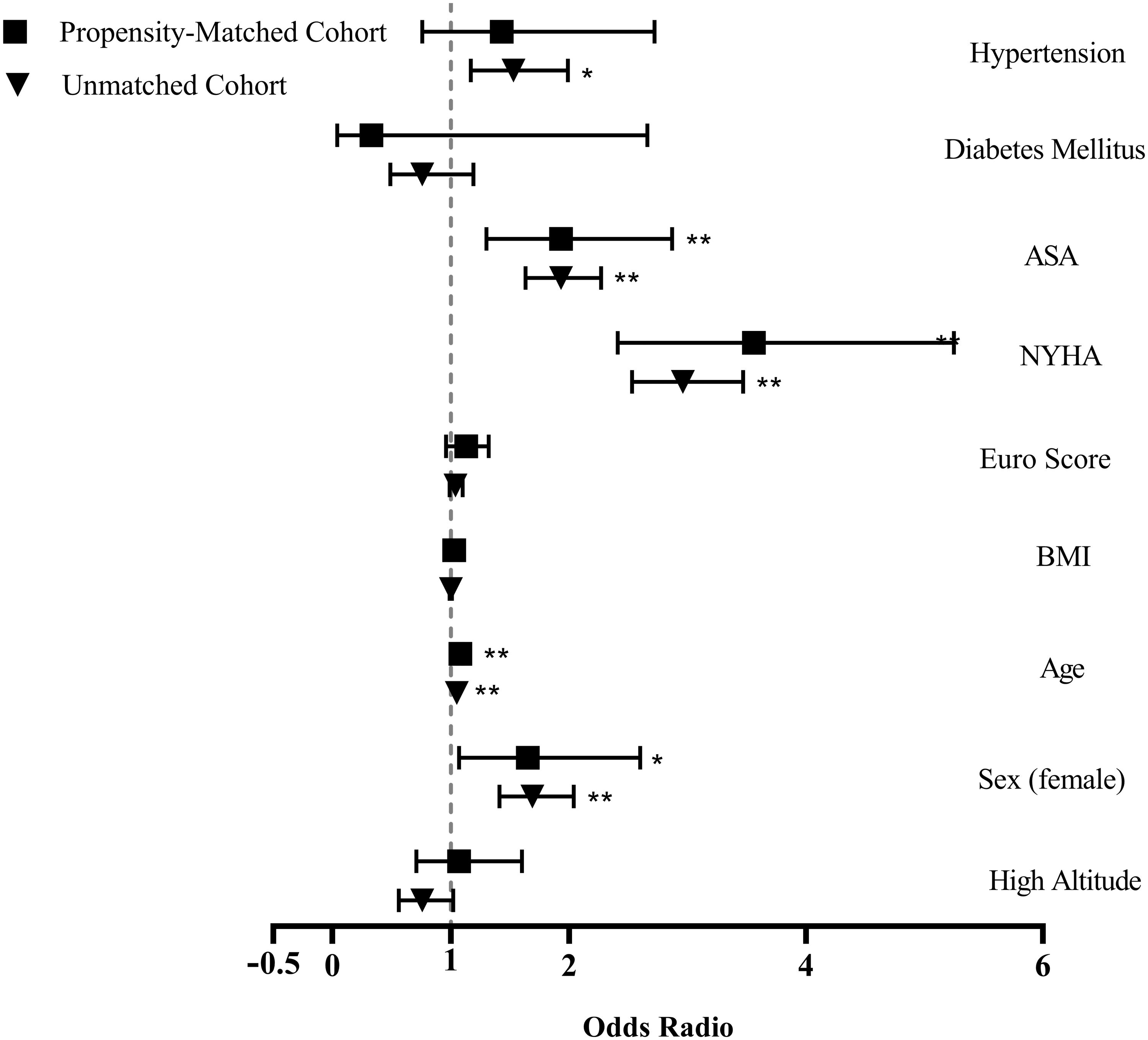
Univariable logistic regression analysis for predicting AF after a lifetime high-altitude exposure. Adjusted ORs (95% CIs) regarding the prevalence of risk factors among a lifetime high-altitude exposure and lifetime low-altitude exposure. *p < 0.05, **p < 0.001. CIs, confidence intervals; OR, odds ratio.
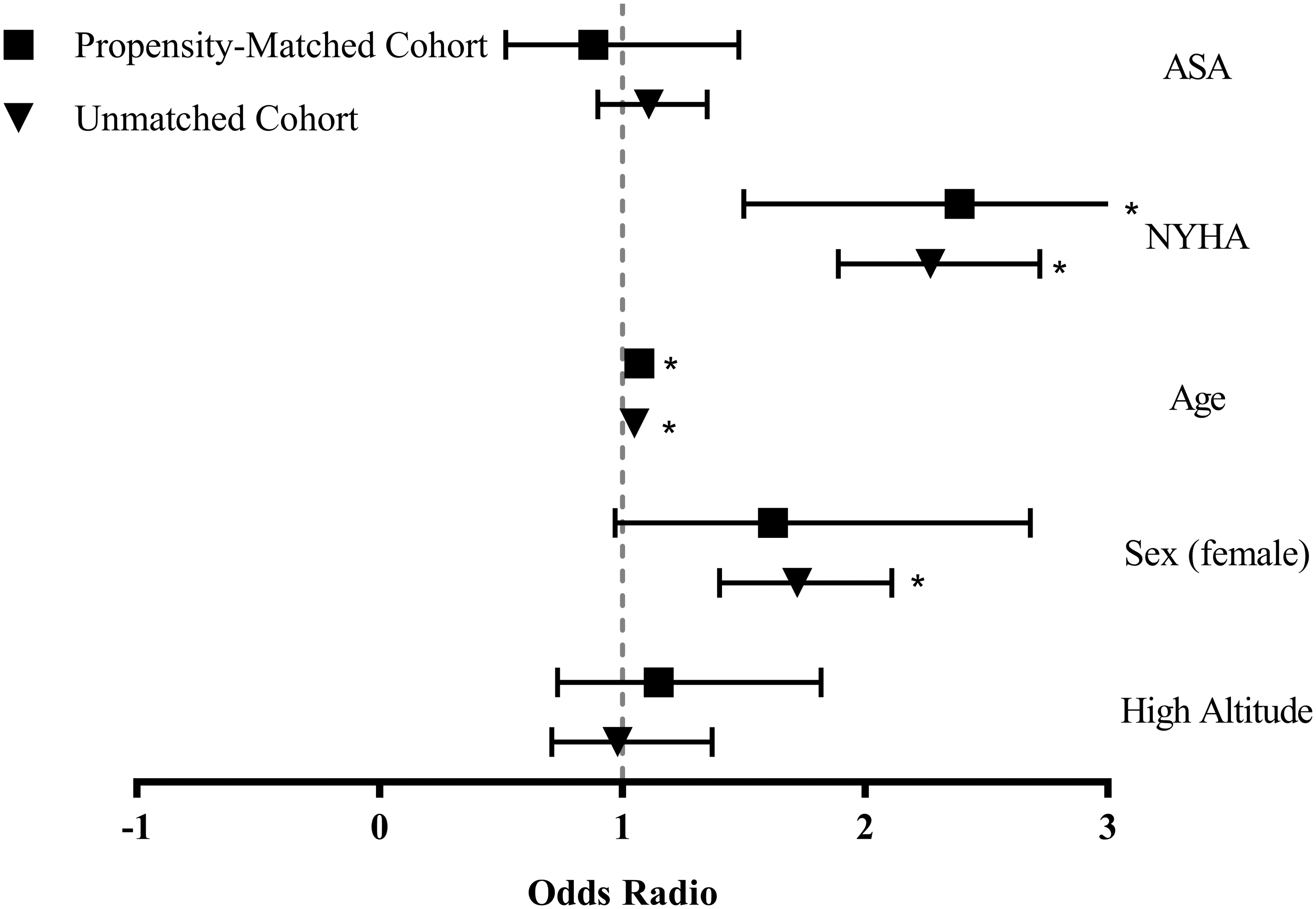
Backward multivariable logistic regression model for predicting AF after a lifetime of high-altitude exposure. Adjusted ORs (95% CIs) regarding the prevalence of risk factors among a lifetime high-altitude exposure and a lifetime low-altitude exposure. *p < 0.05.
Discussion
To our knowledge, this is the first study to evaluate the effect of high-altitude exposure to the development of AF associated with organic heart diseases. In this large propensity score–matched cohort study, we found that the rate of AF did not differ between highlanders and lowlanders. Further, multivariate logistic regression analysis also revealed that a lifetime of high-altitude exposure was not a risk factor in the development of AF. The independent risk factors that were identified were age and NYHA classification. These findings strongly underscore the concept that a lifetime of high altitude or a lifetime of low-oxygen exposure is not a potential risk factor for AF.
Mechanism of AF
The importance of autonomic nerve activity in the genesis and maintenance of AF has long been recognized. Increased cardiac sympathetic activation is considered to be an important cause of AF (Kapa et al., 2010). Sympathetic activation leads to an increase in catecholamine levels, and catecholamine oversupply can shorten the effective refractory period in the atria (Shen et al., 2011; Shen and Zipes, 2014). The increase of Ca2+ in cardiac sympathetic activation is also considered to be another important cause of AF (Patterson et al., 2006). In addition, remodeling of the ultrastructure of atrial myocytes and atrial myointerstitium are also key factors in the maintenance of AF (Iwasaki et al., 2011).
Oxygen is essential to sustaining life. In high-altitude plateau environments, the human body can undergo an oxygen reaction, which can cause a series of physiological and visceral events from lack of oxygen and histomorphological changes, including changes in the cardiovascular system changes during acclimatization. Compensatory mechanisms play an important role in this process. Studies have found that chronic intermittent hypoxia (CIH) is a major risk factor for developing AF (Bober et al., 2018; Zhang et al., 2018).
CIH can enhance the activation of parasympathetic nerves, and at the same time, lead to increased atrial vulnerability, as shown by heightened electrophysiological responses of the atrial myocardium to carbachol and isoproterenol, dampened responses to propranolol, and increased atrial M2 receptor protein levels. Zhibing (Lu et al., 2013) constructed a stable and controllable hypoxia model that can simulate the important pathophysiological and electrophysiological changes in sleep apnea patients. They found AF could be readily induced or spontaneously occur following hypoxia. It is proposed that the mechanisms underlying AF associated with sleep apnea include the following: (1) ischemia and hypoxemia; (2) increase in atrial pressure; (3) inflammation; and (4) imbalance of autonomic activity.
High altitude and AF
A number of physiological changes occur with increasing altitude, with hypoxia likely being the most important effect. At 3,650 m, the resting oxygen saturation may be 85%, and at 5,300 m, the partial pressure of oxygen is half that at sea level (Woods et al., 2008). The heart is very sensitive to hypoxia. Some studies have found significant arrhythmias occur at high altitude (Sutton et al., 1988).
However, this type of study primarily compared ECG changes after lowlanders' exposure to high-altitude areas and did not compare the incidence of AF in highlanders and lowlanders alone. P-wave dispersion (PWD) is a well-recognized electrophysiological feature in patients with AF. PWD has a predictive value for AF (Perez-Riera et al., 2016). The PWD and QT parameters of healthy individuals at high altitudes and at sea level were compared. Akcay (Akcay, 2018) found that the QRS duration and corrected QT time and that the Tp-e interval and Tp-e/QT ratio were statistically significantly higher in the 1,500–2,500 m altitude group. However, P wave maximum, minimum time, and PWD were similar in both groups.
The study of Guntekin also supported the results. Guntekin (Guntekin et al., 2008) found there was no significant difference in respect of PWD values by comparing 12-lead electrocardiographies of 38 healthy people living at sea level (Antalya, Turkey) and 38 healthy people living at high altitudes (Van, Turkey; 1,700–1,800 m).
In our study, we compared the incidence of AF between the two groups and found no significant difference between the incidence of AF in the two groups. This can better explain the influence of lifelong exposure to hypoxic environments on the heart and further reveal the mechanism of AF. In this study, there was no significant difference between the incidence of AF in the two groups, suggesting that the human heart may undergo adaptive changes after prolonged exposure to low-oxygen environments, limiting its ability to induce AF.
Chantal (Dedobbeleer et al., 2015) explored left ventricular (LV) function in recently acclimatized lowlanders, healthy highlanders, and highlanders with chronic mountain sickness. They found short-term altitude exposure in lowlanders altered indices of LV systolic function and increased sympathetic nervous system tone, while life-long altitude exposure in highlanders was associated with similar sympathetic hyperactivity. These results suggest excellent tolerance of LV function to chronic lifelong hypoxic exposure in healthy highlanders. Another study of highlanders (Simpson et al., 2019), specifically the Sherpa, showed that Sherpa have a lower vascular sympathetic baroreflex operating point and lower vasoconstrictor drive.
Highlanders may have adapted to high altitude to require lower sympathetic outflow for homeostatic control of blood pressure. Such differences represent another example of a beneficial hypoxic adaptation in this highland population. For lowlanders, vascular sympathetic baroreflex resetting and heightened sympathetic activity can protect against orthostatic hypotension at high altitude. Sympathetic hyperexcitation is an important mechanism for AF. Therefore, it is easy for lowlanders to have AF induced when they enter a high-altitude environment, while a lifetime of high-altitude exposure does not easily induce AF.
A separate study (Lewis et al., 2014) found that high-altitude exposure in lowlanders was associated with impairments in both endothelial and smooth muscle function, and that such impairment and altered structure likely translated to an elevated cardiovascular risk. However, a lifetime of high-altitude exposure neither attenuates nor intensifies the impairments in vascular function observed with short-term exposure in lowlanders. Arterial remodeling is an adaptive response to chronic high-altitude environments. The extent to which these changes may potentially translate into an elevated cardiovascular risk remains to be determined.
High altitude and postoperative mortality
We found significant survival advantages in lowlanders versus highlanders with regard to postoperative mortality. This is not reflected in postoperative mortality. High-altitude patients are more likely to have postoperative deterioration and re-admission to the ICU. However, there was no significant difference in postoperative bleeding or renal failure.
There are a number of well-defined changes that occur in the cardiovascular system after acute and chronic acclimatization to altitude, such as high-altitude pulmonary edema, pulmonary hypertension with possible heart failure, and renal disease (Savla et al., 2018). These injuries, caused by prolonged exposure to high altitudes and low oxygen, may be less resistant to healing after heart surgery. The reason for the significant difference in mortality, we suspect, may be that prolonged exposure to high altitudes leads to changes in respiratory, cardiovascular, and hematological systems. These changes may affect blood viscosity and reduce circulatory capacity.
Strengths and limitations
The major strength of this study is its large sample size. Because of the unique geographical terrain of Sichuan Province, we were able to obtain more natural data of highland patients. However, due to our study's observational design, our data cannot prove causation. Yet it directs attention in a more logical direction. In addition, AF was not randomly assigned, and therefore may have been subject to selection bias and uncontrolled confounding. To reduce this possibility, we considered a range of potential pretreatment confounders through the use of a comprehensive propensity score model. Our study has some limitations. First, we cannot rule out possible effects of residual confounding from an imbalance of unmeasured baseline covariates. Second, our study is a retrospective, single-center study, making it prone to bias. For example, there were discrepancies observed in some of the patients' previous medical history.
Conclusions
Our study shows that high altitude is not associated with a higher incidence of AF, suggesting that a lifetime of high-altitude exposure may provide better cardiac adaptation than short-term exposure, as in lowlanders.
Footnotes
Author Disclosure Statement
The authors declare no competing financial interests.
Funding Information
This work was supported by the National Natural Science Foundation of China (81500281), Sichuan Science and Technology Program (2019YJ0577), Science and Technology Project of the Health Planning Committee of Sichuan (20ZD011, 19PJ126), and Science and Technology Project of Sichuan Overseas Students (2019-58).