
Abstract
Pigoń, Katarzyna, Ryszard Grzanka, Ewa Nowalany-Kozielska, and Andrzej Tomasik. Severe respiratory failure developing in the course of high-altitude pulmonary edema in an alpinist with COVID-19 pneumonia: a case report. High Alt Med Biol. 23:372–376, 2022.—The case of a 38-year-old Polish alpinist, evacuated from base camp (4,200 m) under Lenin's Peak due to severe high-altitude pulmonary edema (HAPE) and symptoms of acute mountain sickness/high-altitude cerebral edema (HACE), is presented. Starting the expedition, the man was asymptomatic and had a negative COVID-19 molecular test. After a few days of trekking, he developed typical HAPE and HACE. After evacuation to the hospital in Bishkek, a diagnosis of acute bronchopneumonia was made by computed tomography (CT) imaging. A COVID-19 test was not performed at that time. After returning to Poland, a complete noninvasive cardiac and pulmonary assessment disclosed no pathology. The initial chest CT reassessment was read as demonstrating the densities typical for COVID-19 pneumonia, and a SARS-CoV-2 antibody test corroborated the diagnosis. Pre-existing lung disease increases the risk of developing HAPE. In the era of the COVID-19 pandemic, people traveling at a high altitude and unaware of the infection are at particular risk.
Introduction
The decrease in atmospheric oxygen partial pressure with increasing altitude leads to a compensatory response to promote acclimatization, a physiological reaction to adapt to prevailing low oxygen conditions. The lack of acclimatization results in the development of acute mountain sickness (AMS) or potentially fatal high-altitude cerebral edema (HACE) and high-altitude pulmonary edema (HAPE) (Luks et al, 2017). A history of AMS, altitude of residency, recent preceding altitude exposure, or rate of ascent are the major AMS and eventually HACE predictors (Schneider et al, 2002).
The risk of HAPE increases with a history of its prior occurrence (Bartsch et al, 1991), altitude, ascent rate, exertion, male gender, age, infection, individual susceptibility, and comorbidities associated with pulmonary hypertension (Luks and Swenson, 2007). A concurrent respiratory tract infection is an additional risk factor for HAPE (Bärtsch and Swenson, 2013; Murdoch, 1995). In the COVID-19 pandemic era, it is essential to establish possible preventive measures for people traveling to high altitudes.
Case Report
A 38-year-old Polish alpinist was evacuated from base camp (4,200 m) under Lenin's Peak with symptoms of HAPE and AMS/HACE. He had previously been to similar altitudes uneventfully. On the 1st day of the trip from Bishkek to Osh (900 m), he was asymptomatic and had a negative COVID-19 antigen test. He was not vaccinated against COVID-19 at the time. The next day he reached the tourist base at an altitude of 3,800 m. That day he noticed a mild headache, which resolved without any analgesics.
From the 3rd day, he had mild dyspnea with occasional cough, progressively reduced physical capacity, and sleeplessness. At 4,100 m, he felt slight gurgling sounds in his lungs when he lay down. From the following morning, breathlessness caused him to rest every 10 steps. Eventually, he decided to leave the backpack and seek relief. At 4,200 m, already in the camp, he heard the gurgling sounds while breathing in a sitting position, and the cough worsened. Early on the sixth morning of the trip, he developed severe confusion. The finger O2 saturation was 38%, the capillary return was >5 seconds, and cyanosis was observed. A symptoms progression is presented in Figure 1.
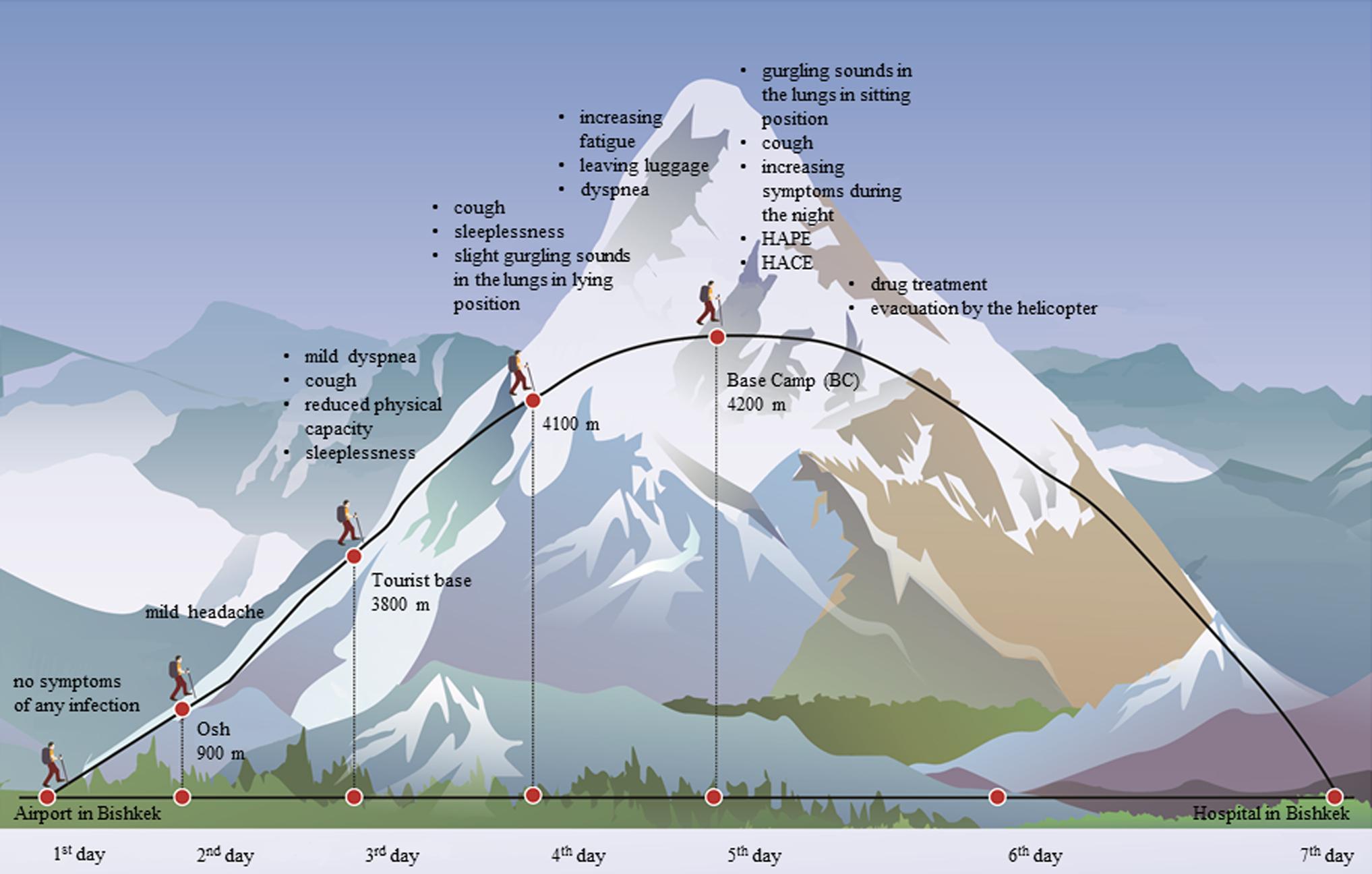
A graphical presentation of progressive respiratory symptoms during the initial phase of a climb of Lenin Peak in an alpinist with COVID-19 pneumonia. HACE, high-altitude cerebral edema; HAPE, high-altitude pulmonary edema.
The patient was the paramedic in one person. The rest of the crew was not experienced in parenteral drug administration, therefore, they started with tablets. He was given acetazolamide and nifedipine. In addition, he was administered intramuscular dexamethasone (8, 4, and 4 mg) after he vomited. No oxygen was supplied, and no portable hyperbaric chamber was used because they were unavailable. At the same day, as his condition had barely improved, he was evacuated by air services to Osh and next to hospital in Bishkek. He was administered O2 therapy during the transportation.
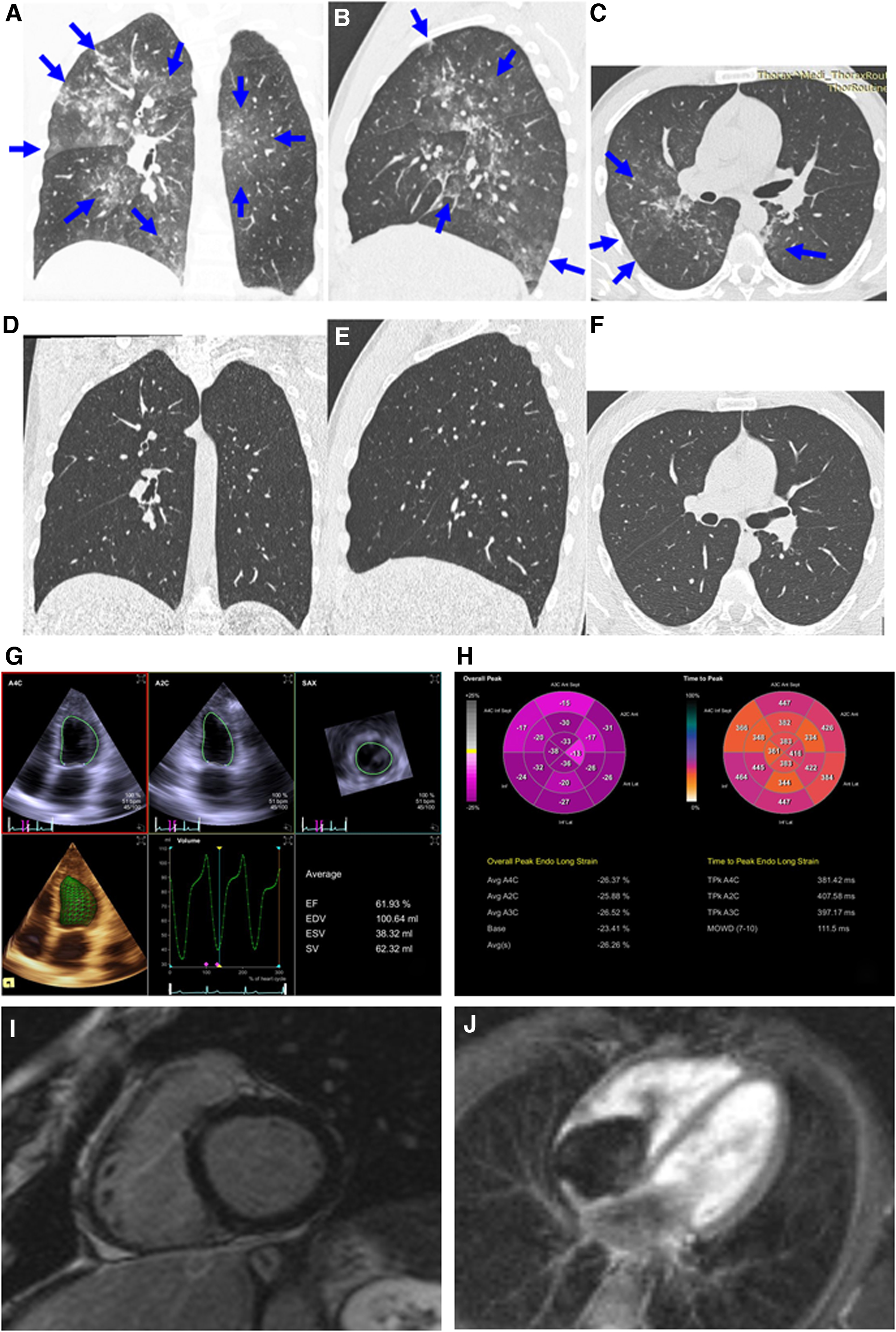
On admission, his axillary temperature was 36.5°C, blood pressure 110/70 mmHg, pulse rate 58/min, respiratory rate of 20 breaths/min, pulse oximetry saturation was 96% on O2 therapy at 5 L/min, and marked respiratory efforts were observed. The patient also received enoxaparin 0.4 mL two times per day. Computed tomography (CT) examination of the chest showed peripheral and subpleural ground-glass opacities (without consolidations) that were bilateral and multilobar (Fig. 2A–C, blue arrows). A diagnosis of acute bronchopneumonia was made. Neither on admission nor on discharge was chest X-ray performed.
Chest CT imaging features coronal—
A COVID-19 test was not performed at that time. He was discharged after 3 days not fully recovered. He returned to Poland with a scheduled flight and was admitted to the hospital immediately and stayed in the cardiology ward where he received oxygen therapy, steroid therapy, low-molecular weight heparin, and underwent diagnostics. Despite the lack of deviations in laboratory and imaging tests in medical and nursing courses, the patient reported weakness, deterioration of well-being, and anxiety. After 11 days, he was transferred to the pulmonology department for further diagnostics.
A reassessment of the initial chest CT images taken in Bischkek revealed the inflammatory lesions typical of COVID-19 pneumonia (Simpson et al, 2020), and a positive SARS-CoV-2 antibody test corroborated the diagnosis. The test was performed 25 days after the onset of symptoms (amount of the antibody: Immunoglobulin M 30.0 AU/mL, Immunoglobulin G 86.3 AU/mL). A complete noninvasive cardiac evaluation disclosed no pathology.
Echocardiography showed normal left ventricle volume and function (Fig. 2G), excellent contractility (Fig. 2H), pulmonary arterial pressure 21 mmHg, and normal magnetic resonance imaging (MRI) (Fig. 2I, J). Spiroergometry disclosed a VO2max of 56 mL/(min·kg). A chest radiograph performed on the 19th day after disease onset was normal, and a repeat chest CT performed 12 weeks later disclosed complete resolution of pulmonary lesions (Fig. 2D–F).
Discussion
We definitely interpret the case as COVID-19 infection that contributed to HAPE and AMS/HACE. As we have had some data on infection missing, we had to check for other noninfectious reasons for unexpected physical breakdown in an alpinist supposed to manage the climb uneventfully. To exclude any cardiac abnormality (myocarditis either), we have performed speckle tracking echo, and MRI (Lang et al, 2015).
Although there are clinical and radiographic similarities, COVID-19 and HAPE are two separate disease entities with different pathogenesis (Luks et al, 2020; Strapazzon et al, 2020). COVID-19 as a respiratory tract infection increases the risk of developing HAPE, which may lead to the coexistence and overlapping of clinical and radiological features of both diseases. This fact should be considered when making diagnostic and treatment decisions.
The ascent profile was extremely risky for AMS and HAPE. The alpinist went from 900 to 3,800 m in 1 day, then compounded the problem by not spending 2 nights at 3,800 m.
In the past, he was at similar altitudes many times, without any symptoms, although he often did not follow the acclimatization patterns. It was the first expedition in his mountaineering career, during which he felt weaker, moving slower than his colleagues.
The negative SARS-CoV-2 test on the predeparture day was misleading. Based on the short period from the beginning of the climb to occurrence of severe symptoms, the patient likely was infected at the time of testing, yet the viral load was still undetectable. Thus, viral replication led rapidly from an undiagnosed and asymptomatic respiratory infection to overt COVID-19 pneumonia. Combined with reduced oxygen content, the underlying pulmonary disease led to HAPE development. The patient may be concerned about the absence of fever. However, there are several reports of asymptomatic COVID-19 pneumonia.
Moreover, we do not know whether he had a fever because he did not take his temperature. Owing to his willingness to continue climbing, he also dissimulating. Thus, traveling in the era of the COVID-19 pandemic requires more caution and compliance with safety rules regarding mask wearing and physical distancing. Having a COVID-19 polymerase chain reaction test before flight regardless of traveler vaccination status and undergoing a minimum 5-day quarantine for self-observation after potential exposure are reasonable. Rapid antigen tests that are easily accessible and inexpensive could be used directly before setting off for the mountains and during the expedition.
An important aspect is also taking care to properly acclimatize. Any respiratory symptoms during ascent should draw attention and a reconsideration about continued climbing. Severe dyspnea and gurgling in the lungs should have prompted immediate descent and treatment of HAPE. Not carrying out a COVID-19 test at the hospital in Bishkek put everyone in contact with the alpinist at risk of infection.
Footnotes
Authors' Contributions
All authors have read and approved the article. K.P. contributed to study concept and design, data acquisition, data analysis, and drafting of the article. R.G. was involved in data analysis. E.N.K. carried out critical revision of the article and approval of the final article. A.T. was in charge of study concept and design, critical revision of the article, and approval of the final article.
Availability of Data and Materials
The data sets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Ethical board of Medical University of Silesia waived the approval.
Consent for Publication
Written informed consent for publication of the clinical details and/or clinical images was obtained from the patient.
Author Disclosure Statement
We declare no competing interests.
Funding Information
No funding was received for this article.