
Abstract
Broadhead Geoffrey K., Henry E. Wiley, David Peprah, Kenneth Olumba, and Alisa T. Thavikulwat. Proliferative retinopathy associated with repeated high-altitude exposure in a patient with sickle cell trait. High Alt Med Biol. 23:369–371, 2022.—Sickle cell trait (SCT), a carrier state characterized by one normal copy of the beta-globin gene (producing hemoglobin A) and one abnormal variant (producing hemoglobin S), is typically asymptomatic and very low risk for manifestations of hemoglobinopathy, including development of retinopathy. Reported cases of proliferative retinopathy in patients with SCT have occurred in the context of concurrent ocular or systemic disease. We report a case of an otherwise healthy patient with SCT who developed proliferative retinopathy requiring surgical intervention in the setting of significant exposure to high altitude through increased work hours as a flight attendant in the month leading to her presentation. Significant high-altitude exposure may contribute to development of retinopathy in patients with sickle trait. Practitioners should consider the possibility of sickle cell retinopathy in patients with sickle trait in these circumstances.
Introduction
Sickle cell disease (SCD) is a hemoglobinopathy resulting from homozygous or double heterozygous inheritance of certain abnormal variants of the beta-globin gene. The prototypical form of the condition, resulting from homozygous variants producing hemoglobin S (HbSS disease), involves pathological change in red blood cell (RBC) shape into a crescent “sickle” form capable of microvascular injury and vaso-occlusion facilitated by certain conditions. Pathological findings of SCD manifest in numerous organ systems, including the eye, where it produces a characteristic retinopathy. In the retina, localized microvascular occlusion leads to local ischemia, which upregulates proteins such as vascular endothelial growth factor and can lead to proliferative sickle cell retinopathy (PSR).
PSR is classically categorized using the Goldberg scale based on severity, starting with peripheral arterial occlusion (stage 1) and peripheral arteriovenous anastomoses (stage 2). At the border of nonperfusion, which typically occurs in the retinal periphery, extraretinal neovascular and fibrous proliferation can occur (stage 3). These friable sea-fan-like neovascularization (NV) are prone to bleeding, which lead to vitreous hemorrhage (VH) (stage 4), whereas fibrous proliferation and contraction may cause tractional retinal detachment (TRD) (stage 5) (Abdalla Elsayed et al, 2019; Goldberg et al, 1971). PSR may be asymptomatic until stages 4 and 5 when central vision is affected.
Sickle cell trait (SCT), a carrier state characterized by one normal copy of the beta-globin gene (producing hemoglobin A) and one abnormal variant (producing hemoglobin S), is associated with a low risk of developing clinical manifestations of hemoglobinopathy, including minimal risk of developing PSR in the absence of other concurrent contributing pathologies (Nia et al, 2003; Tsaras et al, 2009). Rarely, cases of proliferative retinopathy have been reported in patients with SCT in the setting of concurrent systemic or ocular disease that can cause local retinal hypoxia, such as diabetes or ocular trauma (Jackson et al, 1995; Nagpal et al, 1977).
Development of other classic manifestations of SCD, such as splenic infarction, in patients with SCT are also rare, but have been reported in the setting of alterations in blood oxygenation, such as that which occurs at high altitude (Gonzalez et al, 2020; Saad et al, 2020). Cabin air pressure on a commercial airflight is often maintained at an air pressure equivalent to a height of 1,800–2,400 meters, which results in a decrease in the partial pressure of oxygen and consequently a reduction in oxygen saturation. In this study, we report a case of a patient with SCT but without other significant systemic or ocular disease, who presented with VH secondary to PSR after a period of prolonged exposure to high-altitude conditions through her work as a flight attendant.
Case
A 52-year-old African American woman presented to her local retinal specialist with 3 days of decreased vision of the right eye and new-onset floaters. Past medical history included a prior lower-limb sporting injury 7 years prior, and past ocular history was notable for high myopia with prior laser refractive surgery to both eyes >10 years previously. She had been employed as a flight attendant for 25 years and for the past 2 months had been working in the air ∼120 hours/month, significantly increased compared with a prior schedule of ∼70–80 hours/month.
Visual acuity was count fingers in the right eye and 20/25 in the left eye, with intraocular pressures of 14 mm Hg bilaterally. Dilated fundus examination demonstrated VH without a view of the retina of the right eye. Inferior preretinal hemorrhage and inferotemporal retinal NV were observed in the left eye, alongside peripheral lattice degeneration. Hemoglobin electrophoresis revealed the presence of 63.3% adult hemoglobin A1, 33.8% HbSS, and 2.9% hemoglobin A2 consistent with a diagnosis of SCT. Evaluations for diabetes mellitus, hypertension, syphilis, sarcoidosis, and tuberculosis were negative for disease.
Given the degree of visual impairment and the limitations to exclusion of underlying pathology such as a retinal tear, pars plana vitrectomy was performed for the right eye and hemorrhage was removed. During the procedure, the posterior segment of the eye was entered through ports inserted at the level of the pars plana and the hemorrhage in the vitreous cavity was removed. Intraoperative examination demonstrated areas of NV and fibrous traction nasally and temporally, and laser photocoagulation was applied to these areas and to regions of peripheral nonperfusion to prevent progression. The left eye was observed. The patient healed well and vision returned to 20/25 one month postoperatively. Her in-flight hours were reduced to the prior typical level of ∼70 hours/month.
Two years after vitrectomy of the right eye, her VA remained 20/25 in both eyes. Dilated fundus examination demonstrated no evidence of VH in either eye, with temporal and nasal peripheral laser photocoagulation scars and areas of regressed NV in the right eye (Fig. 1). Examination of the left eye showed peripheral areas of regressed NV, as well as patches of lattice degeneration with a flat atrophic hole temporally. Fluorescein angiography demonstrated areas of nonperfusion inferiorly in the right eye, with regressed NV in regions of peripheral laser scarring (Fig. 1). The left eye had regressed NV in the inferonasal periphery (Fig. 1). Laser photocoagulation was recommended in the left eye to surround the areas of NV and to treat peripheral retinal nonperfusion to reduce the risk of potential progression to VH or TRD.
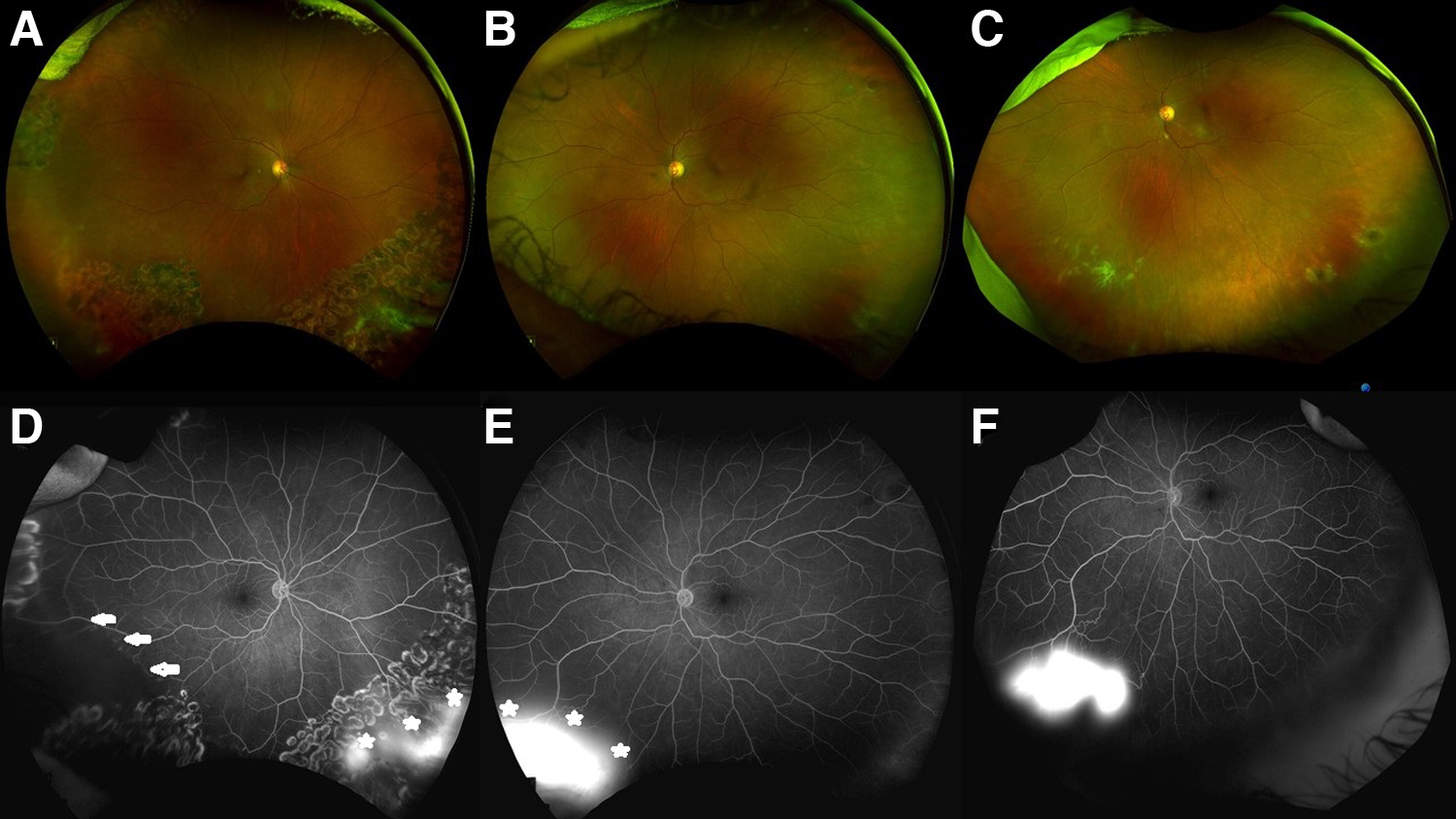
Ultra-widefield retinal imaging of proliferative retinopathy in both eyes. From top left:
Discussion
Our patient with SCT presented with proliferative retinopathy in both eyes, and symptomatic VH and early peripheral TRD managed with vitrectomy and peripheral scatter laser photocoagulation in the right eye. High myopia was judged to be associated with the lattice degeneration and the atrophic hole in the left eye, but was not felt to represent a risk factor for the development of retinopathy.
NV in SCT has been rarely reported in the presence of other ocular or systemic conditions (Jackson et al, 1995; Nagpal et al, 1977). Under conditions of tissue hypoxia, acidosis, increased viscosity, dehydration, or hypothermia, increased RBC sickling and polymerization can occur in those with SCT (Tsaras et al, 2009). The presence of concurrent disease may produce microvascular conditions and hypoxemia that lead to RBC sickling and subsequent vascular injury and a variable degree of retinopathy in patients with SCT.
To our knowledge, this is the first reported case of proliferative retinopathy in a patient with SCT, but without other systemic or ocular risk factors, and for which the identifiable risk may be prolonged exposure to high altitude. The lower atmospheric pressure at high altitudes decreases oxygen diffusion into the vascular system (Sarkar et al, 2003). Although populations that are acclimated to living at high altitudes have developed adaptations to maintain oxygenation, exposure to high altitudes for those that are usually at sea level, such as our patient, results in oxygen deprivation and hypoxic stress.
There are rare reports in the literature of other sickle cell complications due to high-altitude exposure, with the most commonly reported complication being splenic infarction (Gonzalez et al, 2020), and pulmonary embolism (DeLoughery, 2021; Saad et al, 2020). Although high-altitude complications of SCT remain rare, it is important to be aware that these may occur, and to consider lifestyle modifications such as avoidance of prolonged exposure to hypoxic conditions, to prevent subsequent events.
Patients with SCT can rarely develop retinopathy and NV, which usually occur in the context of concurrent vascular disease. Although retinopathy may be underdiagnosed in patients with SCT as it remains asymptomatic until severe disease, no population-based studies including testing with fluorescein angiography exist to assess the prevalence of early retinopathy in this population. High-altitude exposure may also represent a risk factor for development of retinopathy. Clinicians should consider screening for SCT in patients without obvious other causes of retinopathy and should manage these cases similarly to that of sickle cell retinopathy to minimize the risk of vision-threatening complications.
Footnotes
Authors' Contributions
G.K.B. performed conception of this study, data collection, data analysis and interpretation, and drafting of this article. A.T.T. performed conception of this study, data analysis and interpretation, and critical revision of this article. D.P. performed drafting of this article. K.O. and H.E.W. performed data analysis and interpretation and critical revision of this article. All authors approved the final version of this article to be published.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This study was funded by the National Institutes of Health Intramural Research Program. David Peprah was funded by the NIH Medical Research Scholars Program, a public–private partnership supported jointly by the NIH and contributions to the Foundation for the NIH from the Doris Duke Charitable Foundation, Genentech, the American Association for Dental Research, the Colgate-Palmolive Company, and other private donors.