
Abstract
Berendsen, Remco R., Peter Bärtsch, Buddha Basnyat, Marc Moritz Berger, Peter Hackett, Andrew M. Luks, Jean-Paul Richalet, Ken Zafren, Bengt Kayser, and the STAK Plenary Group. Strengthening altitude knowledge: a Delphi study to define minimum knowledge of altitude illness for laypersons traveling to high altitude. High Alt Med Biol. 23:330–337, 2022.
Introduction:
A lack of knowledge among laypersons about the hazards of high-altitude exposure contributes to morbidity and mortality from acute mountain sickness (AMS), high-altitude cerebral edema (HACE), and high-altitude pulmonary edema (HAPE) among high-altitude travelers. There are guidelines regarding the recognition, prevention, and treatment of acute-altitude illness for experts, but essential knowledge for laypersons traveling to high altitudes has not been defined. We sought expert consensus on the essential knowledge required for people planning to travel to high altitudes.
Methods:
The Delphi method was used. The panel consisted of two moderators, a core expert group and a plenary expert group. The moderators made a preliminary list of statements defining the desired minimum knowledge for laypersons traveling to high altitudes, based on the relevant literature. These preliminary statements were then reviewed, supplemented, and modified by a core expert group. A list of 33 statements was then presented to a plenary group of experts in successive rounds.
Results:
It took three rounds to reach a consensus. Of the 10 core experts invited, 7 completed all the rounds. Of the 76 plenary experts, 41 (54%) participated in Round 1, and of these 41 a total of 32 (78%) experts completed all three rounds. The final list contained 28 statements in 5 categories (altitude physiology, sleeping at altitude, AMS, HACE, and HAPE). This list represents an expert consensus on the desired minimum knowledge for laypersons planning high-altitude travel.
Conclusion:
Using the Delphi method, the STrengthening Altitude Knowledge initiative yielded a set of 28 statements representing essential learning objectives for laypersons who plan to travel to high altitudes. This list could be used to develop educational interventions.
Introduction
Millions of people travel for work or leisure to altitudes >2,400 m each year (Luks et al, 2021) where they are at risk of developing several forms of acute-altitude illness (Bärtsch and Swenson, 2013b), including the relatively common and unpleasant, but benign, acute mountain sickness (AMS), as well as potentially life-threatening high-altitude cerebral edema (HACE) and high-altitude pulmonary edema (HAPE) (Bärtsch and Swenson, 2013a; Hackett and Rennie, 2002; Hackett and Roach, 2001, 2004; Luks et al, 2017).
Traveling to high altitude triggers a series of physiological responses, in most cases allowing individuals to acclimatize to lower ambient oxygen levels over several days to weeks, but occasionally leading to maladaptive responses predisposing to acute-altitude illness. The most common altitude illness is AMS, a syndrome characterized by nonspecific symptoms. Although some experts disagree on the deletion of the sleep disorder item in the 2018 consensus (Chen et al, 2021; Richalet et al, 2021a; Roach et al, 2018), headache is still considered to be the cardinal symptom (Roach et al, 2011), accompanied by one or more other symptoms, including gastrointestinal symptoms, dizziness, and/or fatigue. The most important risk factor for AMS is rapid ascent (≥400–500 m·d−1) >2,800 m without any rest days (Luks et al., 2019; Richalet et al, 2021b).
Despite the importance of rapid ascent as a significant risk factor for altitude illness, the reasons for this have received little attention. The choice of ascent profiles for trekking is driven by intrinsic factors, such as motivation and performance expectations, and extrinsic factors, such as peer pressure, time constraints and environmental characteristics, terrain steepness, and availability of overnight accommodation. Behavior is also a function of knowledge. Lack of knowledge can lead to behavior that increases the risk of altitude illness and can lead to poor management. Epidemiological studies have shown that poor knowledge is accompanied by an increased risk of altitude illness, while greater knowledge is associated with a lower incidence of altitude illness (Croughs et al, 2022; Gaillard et al, 2004; Hackett et al, 1976; Kayser, 1991; McDevitt et al, 2014; Shlim and Gallie, 1992).
Although a lack of knowledge may affect the risk of developing acute-altitude illness, no resources have defined the appropriate baseline level of knowledge about high-altitude physiology and medicine for laypersons traveling to high altitude. The overwhelming majority of consensus statements and guidelines are intended for health care professionals, trekking or expedition leaders, or mountain guides (Kupper, 2020; Kupper et al, 2012), and do not specifically target laypersons. The purpose of this study was to fill this gap, and establish a minimum set of essential knowledge items about the recognition and management of acute-altitude illness for laypersons planning to travel to high altitude to reduce altitude-illness–related symptoms.
Methods
We used the Delphi method to develop an expert consensus definition of the essential knowledge for safe travel to high altitude. The Delphi method is based on successive rounds of surveys among experts, who anonymously rate and adapt a series of statements, so that consensus is eventually reached (Hasson et al, 2000).
Definition of “altitude traveler”
For this study, laypersons were defined as travelers who had never previously been to high altitude and those who had traveled to high altitude but remained ill-informed about the risks of high-altitude travel.
Selection of experts
The group consisted of two moderators, a core group of experts and a plenary group of experts. Moderators and core experts were also part of a plenary group of experts. Individuals were deemed eligible to serve as core experts if they had published a minimum of nine articles identified in the Medline database with the phrase “acute mountain sickness” [All Fields] by May 2019. Further, experts were identified by screening the references of the articles by the moderators. The moderators personally selected the core experts based on their qualifications. The moderators approached the experts through automatically generated emails, followed by direct personal emails to limit attrition (Hsu and Sandford, 2007) (see Fig. 1 for schematic representation of expert selection).

Schematic representation of expert selection (n = number of identified experts).
Delphi process
Using their experience in teaching the principles of mountain medicine, the two moderators first formulated a preliminary version of the desired minimum knowledge in the form of a list of 36 statements. These statements were based on the current literature and grouped into five themes: (1) high-altitude physiology (n = 3); (2) sleep at high altitude (n = 3); (3) AMS (n = 18); (4) HACE (n = 6); and (5) high-altitude pulmonary edema (n = 6). The preliminary list of statements was then presented to core experts for revision and additional statements.
Using feedback from core experts, the moderators compiled a revised list of statements for the first Delphi round. This list of statements was subsequently presented to the plenary group to rate the suitability of each statement for inclusion using a Likert scale (1 = strongly disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, and 5 = strongly agree). The experts were required to comment on a statement if their rating was ≤3, and could also comment on any other statement.
In the subsequent rounds, the members of the plenary group were presented with the anonymized comments of the others on the prior versions of the statements, together with their own ratings and comments, and a quantitative breakdown of how many experts agreed or disagreed on retaining the statement for inclusion in the final list. Members of the plenary group were allowed to change or maintain their ratings during the new round and provide further comments. Between rounds, the moderators reviewed the comments of the plenary group and revised the statements for consideration by the plenary group in the next round.
Data security
A secure online survey system was used: NET core 3.1 (.NET Foundation, Redmond, WA). Each participant received a personal invitation with a nonpublic URL and a password. The Delphi survey was protected by unique identifiers to reference the data and create encrypted connections for users to modify the data. Each new survey had a unique identifier in the system. A link was created for the survey owner by using this identifier, which was then encrypted with a timestamp. Through this unique encrypted link, the survey owner can create Delphi statements and invite users to participate in the survey. Users were added with their email addresses and optionally with their names. A Delphi identity was created for each user using a unique identifier. Rijndael 256-bit cryptography was used for the encryption.
Delphi rounds
In Round 1, the first list of statements was presented to the plenary group without accompanying comments, except for general instructions. In Round 2, using the ratings and comments on the statements on which agreement had not been reached, a list of modified statements was presented to the plenary group. This list consisted of the revised statements and an explanation of each statement based on the results of the previous round to guide further review and comments. Some statements were retained in their original form, with an explanation of why they were shown again.
In Round 3, all remaining statements that were still under consideration were presented after incorporating the comments from the previous round(s). In this final round, the plenary members had to accept or reject each statement but also had an escape option: no opinion. Experts who did not respond to the invitation in the first round were not invited to participate in further rounds. Experts who completed the first round but did not respond to the second round were sent multiple reminders, including personal emails asking them to provide their input.
Criteria for inclusion of statements
We defined the level of agreement in Rounds 1 and 2 as the percentage of positive responses (“agree” or “strongly agree”). Reaching agreement was defined a priori as 65%–79% agreement, indicating moderate consensus, and ≥80% agreement, indicating strong consensus. The score for each statement was calculated using the mean Likert score. For a statement to be included in the consensus, ∼75% of the experts had to agree, and the average score had to be ≥3.5. Since Round 3 consisted of three choices, with “no opinion” as one of the choices, the agreement percentage in Round 3 was defined as the fraction of positive answers (“accept”). Again, there had to be ≥75% agreement with the statement to be included in the final list.
Data analysis and presentation
We entered the data into a database (version 18; FileMaker Pro, Santa Clara, CA), and analyzed it using Microsoft Excel for macOS (version 16.56; Microsoft®, Seattle, WA) and GraphPad Prism for macOS (version 9.3.1; GraphPad Software, San Diego, CA). We present the results descriptively (numbers, ratios, and mean ± standard deviation). We performed a Wilcoxon signed-rank test to gauge the effect of attrition (IBM SPSS Statistics for Macintosh, version 25.0; IBM Corp., Armonk, NY).
Results
We submitted an initial list of 36 statements prepared by the moderators for comments to 10 core experts, all of whom agreed to participate. Nine core experts completed the preliminary round. These nine experts rejected four statements: one because of similarity to another statement, one for irrelevance, and two for excess specificity. Based on the comments of the nine core experts, one new statement was added. The initial list for the first Delphi round contained 33 statements scored by the plenary group (Supplementary Table S1).
Results of Rounds 1–3
In Round 1, we presented 33 statements to the plenary group (including core experts). Of these, 41 completed the first round (response rate: 54%) (Fig. 2 and Supplementary Table S2). Three statements were rejected (average score 3.1 ± 0.4; agreement 50% ± 16%, yellow dots in Fig. 2). Of the remaining statements, 10 were accepted (average score 4.0 ± 0.4; agreement 80% ± 13%). Of these statements, three statements had not strictly met the a priori acceptance requirements but were nevertheless accepted (see Supplementary Data S1 for a comprehensive explanation). In Round 2, we presented 21 statements.
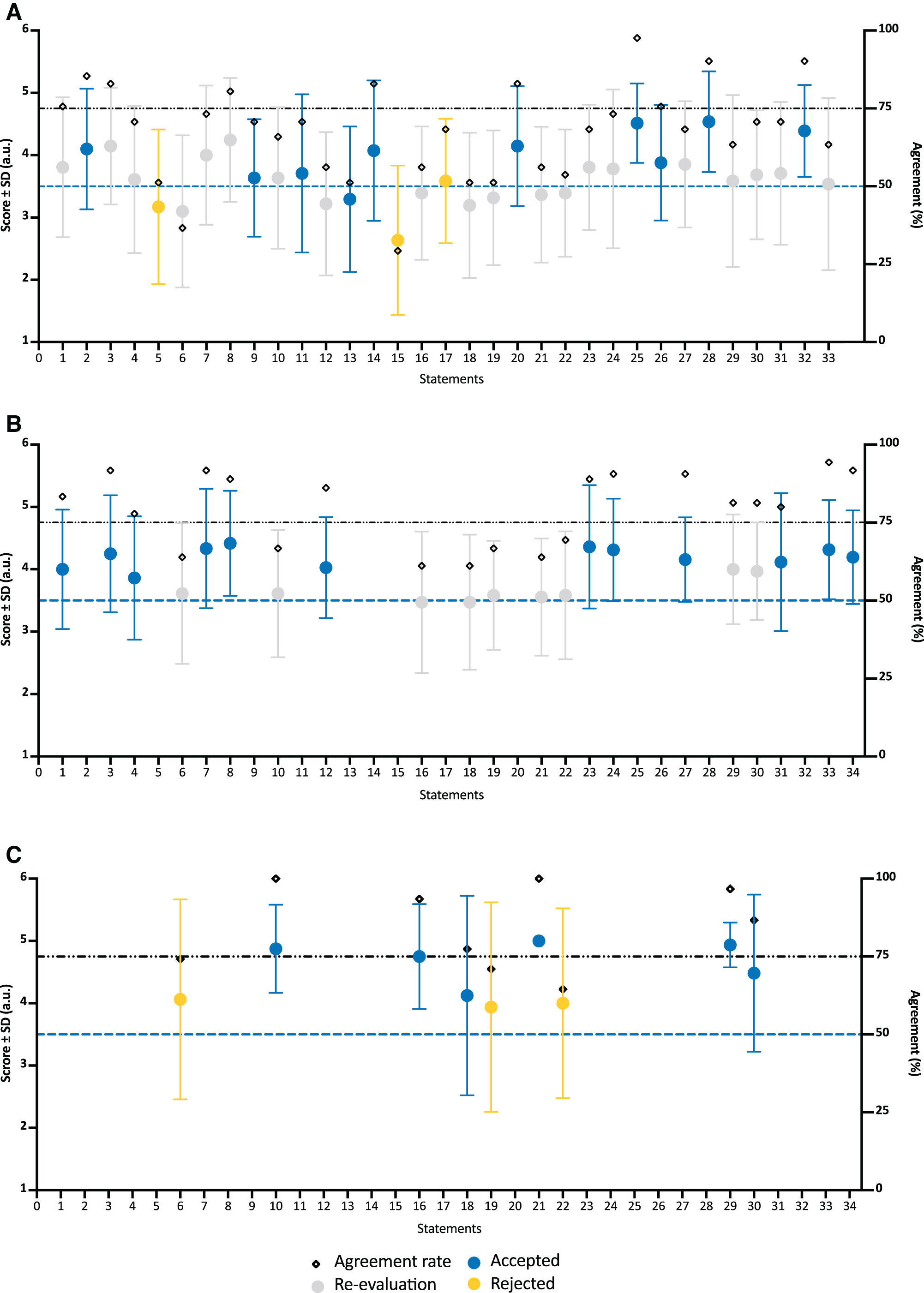
Mean scores and the agreement rates (%) of all statements. Yellow represents the rejected statements
Twelve statements (average score 4.2 ± 0.2; agreement rate 88% ± 5.1%) were accepted by 36 experts (88% response rate). In Round 3, three of the remaining nine statements (average score 4.0 ± 0.1; agreement rate 69% ± 3.1%) were rejected by 32 experts (78% response rate) (Supplementary Table S3). After the third and final Delphi round, there was a list of 28 statements on which 32 experts had reached consensus for their appropriateness as minimum desired knowledge for laypersons planning travel to altitude (Table 1 and Fig. 3).

Mean final scores and the agreement rates (%) of the accepted statements. The black dotted lines indicate the cutoff value for the score. The gray dotted lines indicate the cutoff value for the agreement rate. The table below the graph shows the data associated with the figure and indicates which original statement corresponds to which newly numbered statement.
List of the Final Statements
AMS, acute mountain sickness; HACE, high-altitude cerebral edema; HAPE, high-altitude pulmonary edema.
Assessment for bias
To assess for bias related to attrition from Rounds 1–3, a Wilcoxon matched-pairs signed-rank test was performed to compare the results with and without the experts who had dropped out. There were no statistically significant differences between the median scores of the statements with and without experts who dropped out for Rounds 2 and 3.
Discussion
The objective of this study was to reach a consensus among experts in mountain medicine and physiology on a minimum level of knowledge desirable for laypersons planning to travel to altitudes at which there is a risk of acute altitude illness. Three Delphi rounds were sufficient to reach consensus among 32 experts on a final set of 28 statements. This list of statements (Table 1) can now be used to formulate learning objectives for educational interventions, and provide a common basis for information and education strategies aimed at laypersons planning to travel to altitude.
Learning objectives on altitude illness for lay travelers to high altitude, when accompanied by educational guidelines and, ideally, evaluation of core competencies, would be expected to reduce the incidence of altitude illness and its complications. A recent survey among a representative panel of Dutch Mountain and Climbing Federation (NKBV) members about reasons why they could not continue their trekking found that 25% mentioned AMS as the cause, and 30% said that they were interested in learning more about AMS (RB, unpublished data).
A study among climbers attempting to climb Dhaulagiri explored their knowledge of altitude-related problems. The authors considered the knowledge level of the participants unsatisfactory. Although the number of participants was small (n = 17), the authors concluded that high-altitude mountaineers should be better educated about altitude illnesses (Mena et al, 2018). Another study suggested that more effort is needed to reinforce the message that trekkers should be able to recognize the symptoms and signs of AMS, and be made aware of their responsibilities (Subedi et al, 2008).
Improved knowledge levels are associated with a reduction in the incidence of altitude illness (Gaillard et al, 2004; Hackett et al, 1976; Kayser, 1991). One study concluded that physicians, travel companies, and other organizations sponsoring high-altitude activities should emphasize pretrip preparation and education (McDevitt et al., 2014). The study found that only 42% of trekkers on their way to the Thorong La (5,400 m) had basic awareness of AMS. Awareness of AMS was higher in a previous study in which participants received a lecture on altitude illness before answering questions about symptoms, signs, and treatments (Gaillard et al., 2004).
A structured, expert-supported, international education program for laypersons has not yet been developed. The statements in the list of minimum knowledge for laypersons planning to travel to altitude where there is a risk of altitude illness proposed in this article can serve as learning objectives for teaching/educational programs, and can be used to create information for travel guides and websites. This list of statements may serve as a benchmark for evaluating knowledge of altitude illness.
The information and educational materials will have to be specifically tailored for various populations, ranging from lay but literate people to lay illiterate people, such as Himalayan porters and pilgrims. Our study was not designed to assess the effects of any intervention on knowledge acquisition or retention. Ideally, any intervention should be followed by evaluation of the results. Such studies may yield inputs for adjustments to teaching programs as well as learning objectives. This may be necessary because there are probably too many statements for each to be a separate learning objective.
Limitations
A recurring problem in Rounds 1 and 2 was understanding the instructions. We asked the members of the plenary group to give their opinion on what laypersons traveling to altitude should know, not what they already know. However, several experts assessed the statements in the former way (e.g., “trekkers in the Himalayas do not know this”). Proficiency in English could have played a role, since 5% of the experts were from Asia, 54% from Europe, and 41% from North America. Comprehension could have played a role (Hoover and Gough, 1990), but also haste or disinterest while responding to the survey. The magnitude of this bias cannot be determined.
While the online version of the Delphi method made it possible to involve a large group of international participants while limiting cost, preserving anonymity, and decreasing the risk that a select group of participants would dominate the conversation, it took time to collect the responses, and attrition was frequent, problems that were likely exacerbated by collecting data during the COVID-19 pandemic. The concern of increasing attrition over subsequent rounds is that this could lead to a “false” consensus, as participants with dissenting views start dropping out (Humphrey-Murto and de Wit, 2019).
Another important limitation is that the method used to identify the most important learning objectives for laypersons does not identify the most effective teaching methods. However, assuming that what is learned will be practiced is not necessarily the case. Action is not always consistent with knowledge; a problem referred to as the knowledge-to-action gap (Kahlke et al, 2020; Knight et al, 2008). This may not be an immediate limitation but may become so when implementing the statements.
Conclusions
The STrengthening Altitude Knowledge (STAK) consensus, developed using the Delphi method, describes 28 learning objectives laypersons should know before traveling to altitude. The list of learning objectives can be used to develop information and teaching materials to increase the knowledge of this target population. Over time, new developments in the field of high-altitude medicine may provide new insights that make these learning objectives subject to modification.
Footnotes
Acknowledgments
We thank Marieke van Vessem, Rigo Hoencamp, and Leon Aarts for their input during the early design phase of the study, and Arjen de Blok for the development of the online Delphi software, and STAK panel members, excluding the moderators and core experts: J. Anholm,3 P.S. Auerbach,3,† B.A. Beidleman,2 K.E. Bloch,1 M. Brodmann,2 H. Brugger,3 M. Burtscher,3 C. Dehnert,3 L. Dumont,3 M. Faulhaber,3 R. Fischer,3 H. Gatterer,3 F. Gekeler,1 C.K. Grissom,3 M.P.W. Grocott,3 D. Hillebrandt,3 B. Honigman,3 C. Imray,1 M.S. Koehle,3 G.S. Lipman,2 J.A. Loeppky,3 M. Maggiorini,2 L.G. Moore,3 S.R. Muza,1 M. Pun,3 R.C. Roach,1 C. Sartori,3 U. Scherrer,3 G. Sikri,3 A.W. Subudhi,3 E.R. Swenson,3 A.A. Thompson,3 S. Verges,3 and D.R. Woods3 (1participated in the first round only; 2participated in two rounds; 3participated in all three rounds; †passed away after submitting his comments on the final round).
Authors' Contributions
R.R.B. and B.K. contributed to study design and methods, first version of the article, and data reduction and analysis. R.R.B., B.K., and core experts contributed to the experimental phase and final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this research.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.