
Abstract
Guo, Hai, Linjie Cheng, Dilihumaier Duolikun, and Qiaoling Yao. Aerobic exercise training under normobaric hypoxic conditions to improve glucose and lipid metabolism in overweight and obese individuals: a systematic review and meta-analysis. High Alt Med Biol. 24:312–320, 2023.
Background:
Obesity is a critical public health issue around the world, reaching epidemic proportions in some countries. However, only a few studies have examined the effects of hypoxic training on metabolic parameters in an obese population. This systematic review and meta-analysis aimed to determine the effects of aerobic exercise training under normobaric hypoxic conditions versus normoxic training in improving glucose and lipid metabolism in obese individuals.
Methods:
A systematic search of PubMed, EMBASE, Web of Science, and Wan Fang databases (up to August 2021) was performed to identify randomized controlled trials (RCTs) of overweight or obese human subjects eligible for inclusion. Main study endpoints were changes in body mass index (BMI), waist/hip (W/H) ratio, leptin, blood glucose and insulin levels, as well as blood lipids between hypoxic and normoxic conditioning.
Results:
Fourteen RCTs with a total of 413 subjects qualified for inclusion. Pooled analyses revealed that BMI (d = 0.38), W/H ratio (d = 0), blood glucose (d = 0.01), and triglyceride (d = −2.27) were not significantly different between aerobic exercise training under hypoxic and normoxic conditions. However, significant differences were found in heart rate at rest (d = −4.50) between aerobic exercise training under hypoxic versus normoxic conditions.
Conclusions:
In conclusion, no significant benefits were noted in aerobic exercise training under hypoxic conditions over normoxic conditions in overweight or obese individuals. However, the maximum training heart rate mm was significantly higher under hypoxic conditions than under normoxic conditions. Future studies with larger samples controlling for exercise-related parameters, and addressing the potential modifying effects of level of hypoxia, sex, or age on the role of hypoxic exercise training are warranted. PROSPERO registration number: CRD42020221680
Introduction
Obesity is currently a critical public health problem around the world, and is noted for leading to chronic metabolic diseases and reducing life expectancy (Di Cesare et al., 2019). A recent study reported that 2.3 billion adults are overweight globally, 80% of whom are diagnosed with diabetes and hyperlipidemia (Landecho et al., 2019). The prevalence of overweight and obesity continues to increase in both developing and developed countries, often reaching epidemic proportions. The obesity epidemic has increased dramatically over the past few decades, largely as a result of unhealthy diet, physical inactivity, sedentary lifestyle, and lack of sleep (Bressan et al., 2013). The pathophysiology of obesity is multifactorial, including individuals' genetic background, demographics, lifestyles, and socioeconomic status (Lin and Li, 2021). Clinically, a body mass index (BMI) above 30 kg/m2 is classified as obese; BMI is calculated by dividing weight by height (kg/m2) (Landecho et al., 2019). Maintaining a precise balance between food intake and energy expenditure is regarded as the key to sustaining metabolic balance and avoiding the development of overweight or obese status (Yeung and Tadi, 2022).
Obesity is associated with increased risk of various chronic conditions, including cardiovascular diseases (CVDs), obstructive sleep apnea, certain cancers, and chronic inflammatory diseases, all of which lead to a shortened life span (Landecho et al., 2019).2 In addition, obesity is a risk factor for multiple neurological consequences, such as dementia and Alzheimer's disease. Obesity is also comorbid in psychiatric disorders affecting behavior, cognition, and mood, which suggests that common biochemical pathways in the central nervous system may be involved in obesity. Previous studies have also pointed out that excess weight can increase the burden on the joints, which may lead to osteoarthritis and seriously affect the quality of life (Camacho-Cardenosa et al., 2018; Kong et al., 2016). Therefore, effective interventions are needed to prevent and treat obesity. An increased heart rate was observed under hypoxic conditioning. Even at the same heart rate, the exercise load is relatively lower than that of a normoxic environment, which is reported to be beneficial toward reducing the risk of bone and joint damage caused by obesity.
Several studies have shown that aerobic exercise training in a hypoxic environment benefits weight loss and improves the components of metabolic syndrome (Camacho-Cardenosa et al., 2018; Kong et al., 2016).
Behavioral changes toward a healthy life style are thought to be an ideal way to prevent or reduce overweight and obesity, including carefully controlled food intake and an appropriate amount of exercise (Di Cesare et al., 2019; Landecho et al., 2019; Yeung and Tadi, 2022). Exercise for the purpose of losing weight is initially effective, but when the exercise is discontinued, the weight tends to return to its original state (Landecho et al., 2019; Yeung and Tadi, 2022). A previous study showed that people living at high altitudes had lower rates of obesity-related diseases than people living at low altitudes, suggesting that hypoxic conditions may be beneficial for weight loss (Kayser and Verges, 2013). Several other studies have reported that a hypoxic environment reduces appetite. Another previous study showed that elevated plasma leptin levels at intermediate altitudes were associated with reduced food intake and weight loss (Yang et al., 2018). Furthermore, another previous study demonstrated that exposure to hypoxic environments significantly increased fasting plasma leptin and postprandial glucagon-like peptide-1 levels compared with normoxic environments, which together inhibited appetite (Shobatake et al., 2019).
Hypoxia-inducible factor-1 (HIF-1) is a key factor regulating oxygen homeostasis in human and animal organisms. Under hypoxic conditions, HIF-1 is translocated to the cellular nucleus and activates multiple downstream genes that regulate glucose uptake and transport, glycolysis, lactate production, oxygen transport and appetite, while ultimately contributing to weight loss (Chu et al., 2019).
Hypoxic therapy, including hypoxic exposure or hypoxic exercise intervention, has been used to treat and prevent diabetes by affecting glucose uptake, insulin sensitivity, and vascular health. Insulin resistance is improved by training in both hypoxic and normoxic conditions. An animal study showed that training in hypoxic conditions increased muscle mass and decreased fat mass, which then increased insulin sensitivity and improved insulin resistance in rats (Little et al., 2014). Exercise intervention also has the potential to enhance glycemic control and cardiovascular status. Recently, many studies investigating the treatment of diabetes by applying hypoxic conditions have shown that exercising at high altitudes reduces the risk of diabetes, CVD, and obesity-related diseases compared with exercising at low altitudes (normoxic conditions). Therefore, artificial hypoxia conditioning with exercise training appears to be a potential treatment strategy for obesity. However, another study reported that training in a hypoxic environment did not lead to excess weight loss (Kong et al., 2017).
A previous systematic review evaluating the effect of hypoxic training was greatly limited by the inclusion of nonrandomized studies and end of search in 2017 (Hobbins et al., 2017). The review also lacked comprehensive comparisons of blood metabolic biomarkers. Furthermore, eight more randomized controlled trials (RCTs) (Camacho-Cardenosa et al., 2019; Camacho-Cardenosa et al., 2018; DE Groote et al., 2018; Fernández Menéndez et al., 2018; Klug et al., 2018; Mai et al., 2020; Park et al., 2019; Shin et al., 2018; Yang et al., 2018) have been published since 2017. In the present study, we aimed to systematically review the current evidence reported in RCTs regarding the effects of aerobic exercise training under normobaric hypoxic conditions among overweight and obese individuals, and to conduct a comprehensive evaluation of common metabolic biomarkers.
Materials and Methods
Study design and included studies
The present systematic review and meta-analysis was conducted under the guidance of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). The PROSPERO registration number is: CRD42020221680. Only RCTs were selected that were focused on overweight or obese participants (with BMI >25 kg/m2) with ages ranging from 12 to 80 years. Studies with patients having comorbid chronic orthopedic, neurological, cardiovascular, or respiratory diseases were excluded. Nonhuman studies and studies focused on infants, plateau residents, or athletes were also excluded. The intervention groups in the included studies received moderate-intensity aerobic exercise for a minimum of 30 min/day and 5 day/week in a monitored hypoxic condition (defined as oxygen pressure <20%). A hypoxic condition referred to simulation by artificial methods of a high plateau environment with hypoxia, including training modes such as: (1) living high and training low; (2) living low and training high; (3) living high, training high, and training low; and (4) intermittent hypoxic training. Control groups received aerobic exercise training under normoxic conditions.
Data sources and search strategy
A comprehensive literature research was performed using PubMed, EMBASE, Web of Science, and Wan Fang databases from inception until August 2021. The keywords and search strategy used for PubMed were: (“Intermittent hypoxia” OR “passive hypoxic exposure” OR “hypoxic training” OR “altitude training” OR “live-low train-high”) AND (obesity OR overweight OR “weight loss” OR “physiological response” OR “metabolic response” OR “cardiovascular response”).
Data extraction
Retrieved articles were reviewed for eligibility by two authors independently. If any discrepancies were found, the authors discussed and resolved them. The following data were extracted from the eligible studies: first author, baseline characteristics of the study subjects, and outcome measures.
Primary and secondary outcomes
Primary outcomes were body composition indicators, including BMI, body fat, and waist/hip (W/H) ratio. Secondary outcomes were heart rate and metabolic biomarkers, including blood glucose, insulin, leptin, and triglyceride levels.
Risk of bias assessment
Two authors evaluated the risk of bias across included studies independently. Risk of bias assessment was performed under the guidance of Cochrane Manual 5.1.0 (Gatterer et al., 2015).
Statistical analyses
All statistical analyses were conducted using Review Manager (RevMan®) software (Cochrane Systems). Outcome comparisons between intervention and control groups are presented as mean difference (MD) or standard MD with a 95% confidence interval (CI). Heterogeneity was evaluated through the I statistic, and between-study variance was evaluated using tau-square. A random-effects model was chosen when the I statistic revealed heterogeneity across studies, otherwise a fixed model was used. A p < 0.05 value was established as statistical significance. Publication bias was evaluated through an asymmetry Egger's test and a funnel plot.
Results
General characteristics of the included studies
The comprehensive study selection flow diagram is shown in Figure 1. A total of 805 studies from the aforementioned databases were initially identified, from which 541 duplicates were excluded. Among the remaining 264 articles, 227 were excluded for not conforming to the inclusion criteria after screening the titles and abstracts, leaving 37 articles for further screening at full-text level. Twenty-one studies were excluded for lacking follow-up date, no relevant outcomes, being guidelines or review articles, containing pediatric subjects, or comprising no treatment. Finally, 14 articles (5, 8, 10, 12–24) with a total of 322 subjects entered into systematic review and subsequent meta-analysis. Supplementary Table S1 provides an overview on the interventions and subjects' characteristics from each included study. Age and BMI of the study subjects ranged from 13.7 to 52.4 years and 22.5 to 36.7 kg/m2, respectively. Exercise durations ranged from 2 to 12 weeks. The level of FiO2 in hypoxic conditions ranged from 14% to 17.2% across the included trials.

Flow diagram of study selection.
Risk-of-bias assessment
The results of risk-of-bias assessment are shown in Figure 2. Specifically, 11 RCTs were conducted blindly, with proper randomization and allocation concealment.
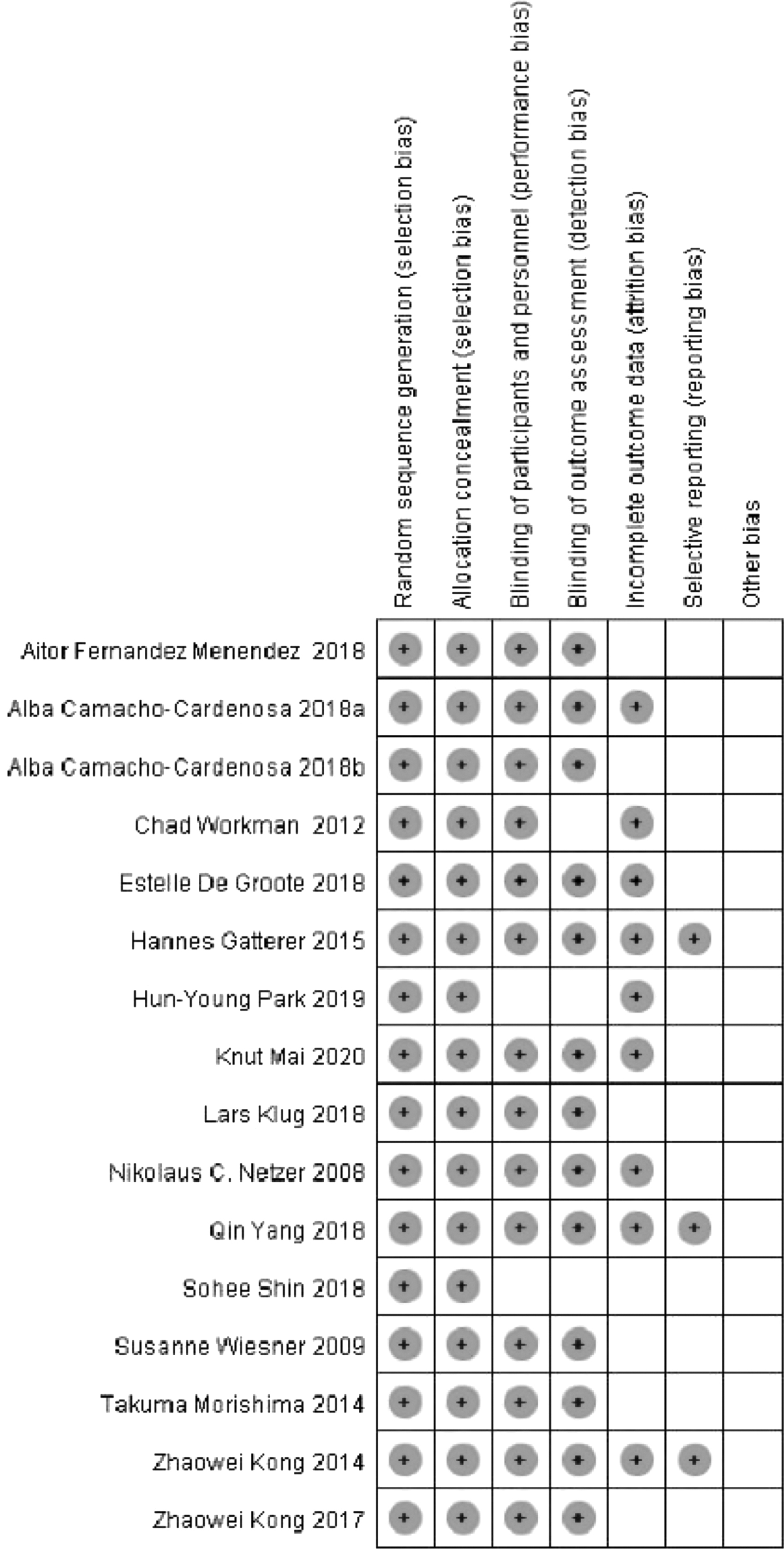
Risk of bias in the included studies.
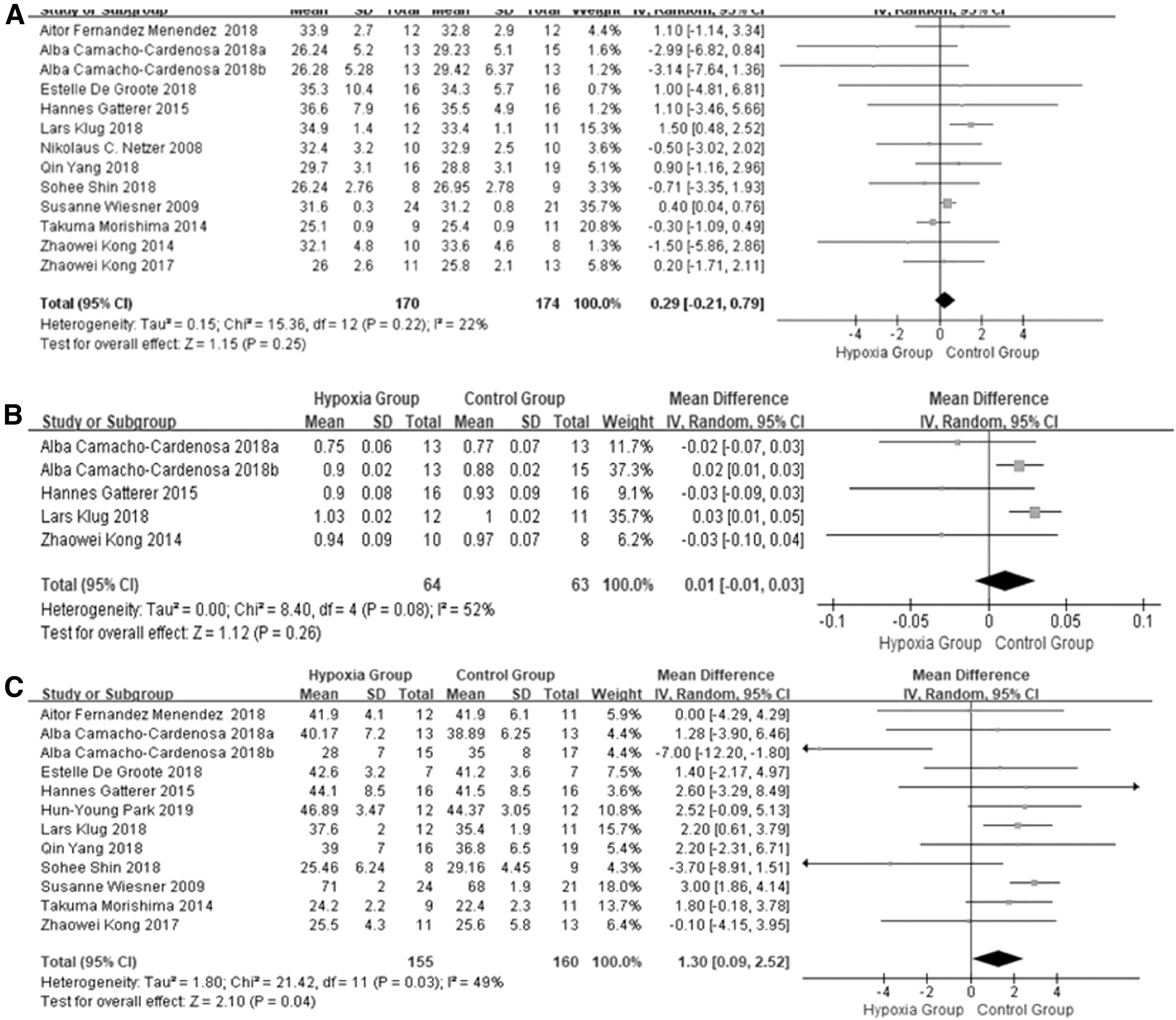
Differences in BMI, waist to hip ratio and fat mass between hypoxic and normoxic conditioning
Thirteen studies reported BMI after exercise training. Meta-analysis showed no significant differences in BMI between hypoxic and normoxic groups after training (MD: 0.38, 95% CI: −0.21 to 0.97; I2 = 11%; p = 0.33) (Fig. 3A). Four studies reported W/H ratio after exercise training. Meta-analysis showed no significant differences between the two groups (MD: 0, 95% CI: −0.04 to 0.03; I2 = 64%; p = 0.04) (Fig. 3B).
Differences in
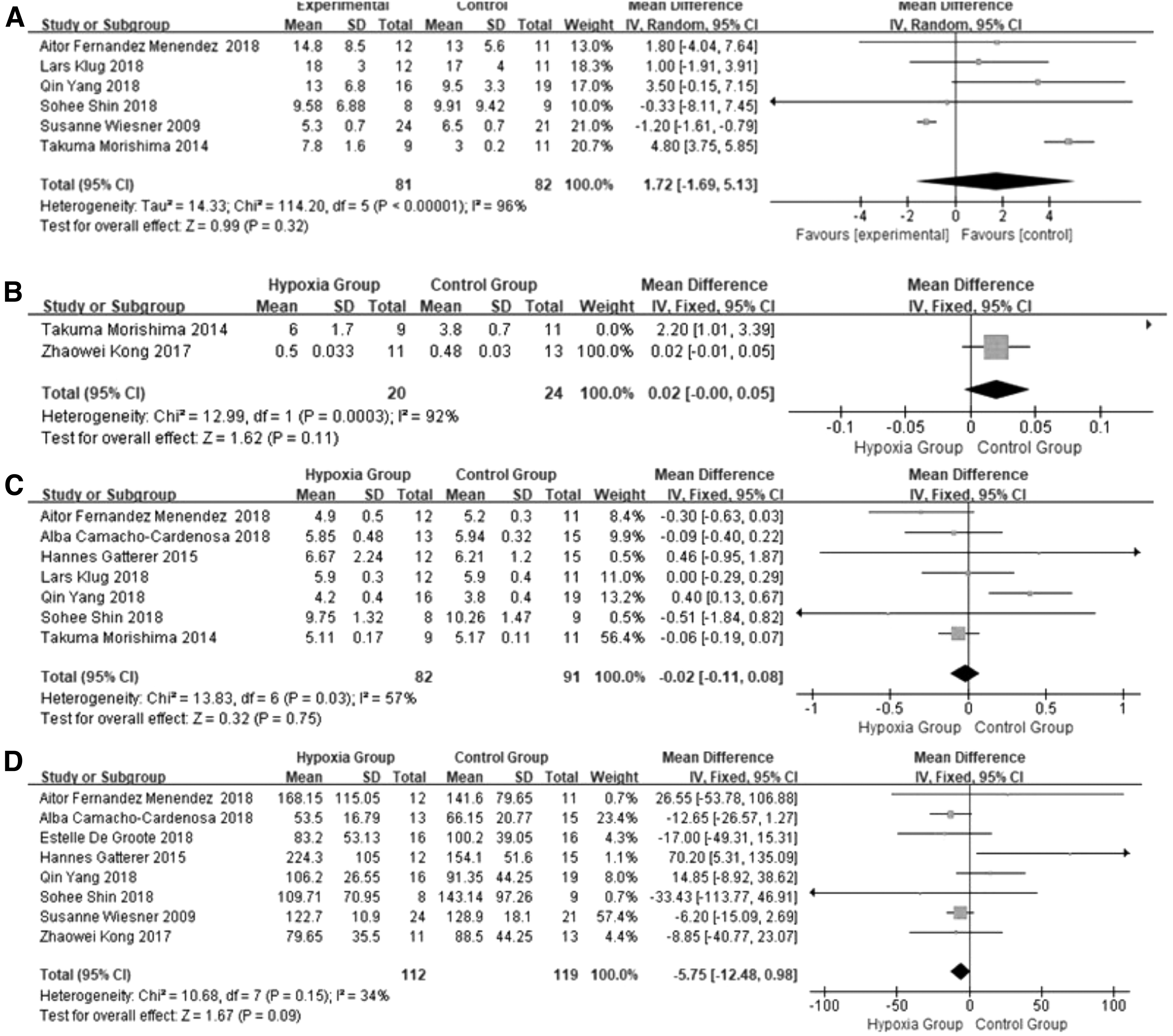
Differences in fasting blood glucose and triglyceride between hypoxic and normoxic conditioning
Nine studies reported fasting blood glucose levels after exercise intervention, and meta-analysis showed no significant differences between the two groups (MD: 0.01, 95% CI: −0.15 to 0.18; I2 = 48%; p = 0.05) (Fig. 4A). Ten studies reported triglyceride levels after exercise intervention. Meta-analysis still showed no statistically significant differences between the two groups (MD: −2.77, 95% CI: −13.35 to 8.82; I2 = 55%; p = 0.02) (Fig. 4B).
Differences in
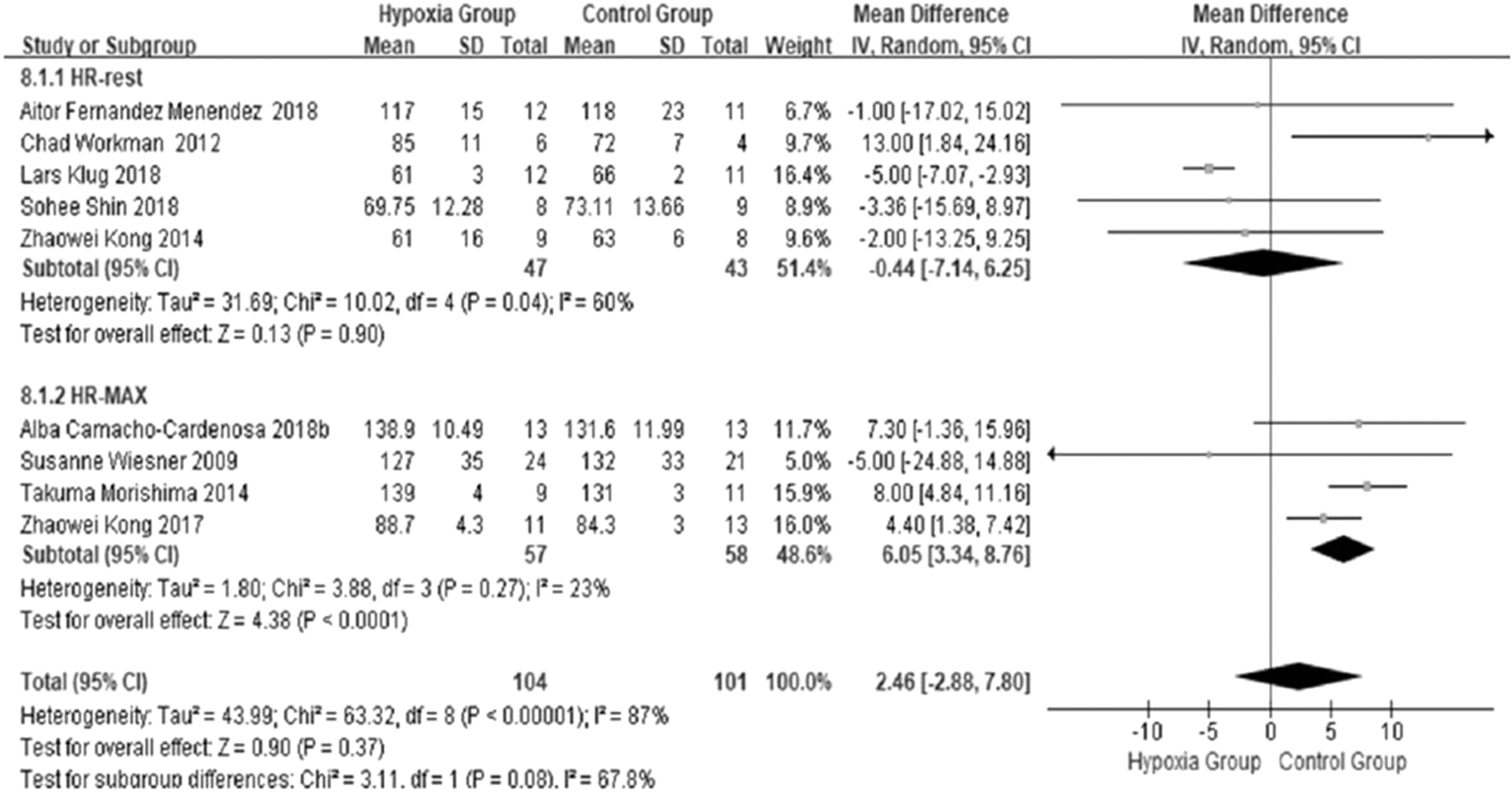
Differences in heart rate between hypoxic and normoxic conditioning
Four studies reported heart rate at rest after exercise training. The results showed significant differences in heart rate at rest between the two groups (MD: −4.50, 95% CI: −6.42 to −2.57; I2 = 0%; p = 0.60) (Fig. 5A).
Differences in heart rate between hypoxic versus normoxic conditioning.
Discussion
Hypoxic conditioning through exercise training has been speculated to be a potential therapeutic strategy for weight loss in obesity (Park et al., 2018). In recent years, interest has surged in the effects of hypoxic regulation and exercise training on weight loss, even though the findings were inconsistent between studies. Previous systematic reviews evaluating the effects of hypoxic training lacked more comprehensive comparisons. The present study aimed to systematically review the available evidence reported in previous RCTs on the effects of aerobic exercise training under normobaric hypoxic conditions on overweight and obesity. More specifically, this systematic review and meta-analysis compared the effects of aerobic training under hypoxic versus normoxic conditions on weight loss and metabolic parameters in overweight and obese subjects from previous studies.
A previous animal study reported that exposure to intermittent hypoxic conditions contributed to weight loss and appetite suppression in mice (Jun et al., 2014). The animal study of Olfert et al. (2001) found that training in hypoxic conditions reduced body weight or delayed the animals' growth. However, a human study noted a significantly lower incidence of obesity in people living at high altitudes (Voss et al., 2013). The Gaichuya people living in the Peruvian Andes at an altitude of 3600 meters have strong muscles and slender bodies, independent of socioeconomic factors (Toselli et al., 2001). Study on exercise physiology showed that training in hypoxic conditions significantly decreased body weight and fat mass in obese individuals when compared with normoxic conditions, and improved lipid metabolism in the liver (Kong et al., 2014; Lu et al., 2014). However, in the present study, no significant differences were found between hypoxic and normoxic training conditions in BMI, W/H ratio, blood glucose, insulin, or triglycerides after aerobic exercise training.
BMI has been identified as an indicator of obesity (Eissa et al., 2020), but it does not fully reflect body fat mass. The W/H ratio is also widely used to assess abdominal obesity (Joseph et al., 2021). BMI and W/H ratio are key predictors of obesity risk (Wajchenberg et al., 2019), and may change with exercise training. Several previous studies noted that training in hypoxic conditions conferred no significant benefits on BMI compared with training in normoxic conditions (Kong et al., 2017; Kong et al., 2014; Shin et al., 2018; Wiesner et al., 2010). In the present meta-analysis, BMI was significantly reduced after training under hypoxic conditions, but no statistical differences were observed between the hypoxic and normoxic groups. Different training times and total duration may have affected the results; however, given the relatively small number of studies included, we were unable to stratify subjects by duration of exercise program, a limitation of this study.
Another study showed that living at high altitudes resulted in weight loss and hypotension, and altered metabolic biomarkers (Lippl et al., 2010). These possible mechanisms include increased norepinephrine levels (Osaka, 2011), increased arteriolar diameter, induction of relaxation and peripheral vasodilation, lower blood pressure, increased GLUT4 glucose transporter, increased plasma serotonin, and inhibition of leptin levels, as reported previously (Wang et al., 2018). Another previous study indicated that fat oxidation was enhanced after 12 weeks of training under hypoxic conditions, but not under normoxic conditions (Balykin et al., 2004). The authors of that study emphasized that exposure to hypoxia has long-term effects on increasing fat metabolism and inhibiting hepatic glycolysis. Hypoxia inhibits insulin signaling, accelerates the release of free fatty acids and inhibits glucose uptake, thereby further reducing fat accumulation in body tissues (Urdampilleta et al., 2012; Wewege et al., 2017). In the present meta-analysis, no significant differences were observed in blood insulin or glucose levels between hypoxic and normoxic groups. Obese subjects often have insulin resistance, decreased glucose tolerance, and hyperglycemia.
The mechanisms underlying these changes include loss of muscle mass, systemic inflammation, and fat accumulation and are closely associated with circulating fatty acids and changes in metabolism. A previous study indicated that after performing endurance training, the expression of GLUT4 mRNA in skeletal muscle tissues was significantly increased, which was not affected by the intensity of motion (Montero and Lundby, 2016).
Leptin is an important regulator in energy metabolism and, accordingly, plays an important role in obesity and weight loss. Training under hypoxic conditions promotes leptin secretion and synthesis; moderate, intermittent training under hypoxic conditions increased serum leptin levels and enhances leptin receptor expression in mice (Mann et al., 2014). In the present meta-analysis, no significant differences were noted in postintervention leptin levels between the hypoxic and normoxic groups, however, the small number of studies analyzed limited further interpretation of the result.
Training under hypoxic conditions is reported to affect lipid metabolism, increasing triglyceride levels and enhancing lipid oxidation (Roels et al., 2007). Hypoxic conditions stimulate peroxisome proliferating receptor gamma and peroxisome-activated receptor coactivator 1, which both assist in the adaptive regulation of muscle fatty acid oxidation (Gilde and Van Bilsen, 2003). These factors also regulate both oxygen transport and lipid metabolism by increasing HIF-1 (Polotsky et al., 2003). A previous study indicated that triglyceride levels decreased more in a hypoxic group than in a normoxic group (Wiesner et al., 2010). In the present meta-analysis, no significant differences were observed in triglycerides between the hypoxic and normoxic groups after the training intervention, which may be explained by differences in study design between this review and that of individual studies mentioned above.
In addition, a previous study indicated that intermittent training in hypoxic conditions activates the sympathetic nerves, which increases the heart rate and hypertension, leading to hypoxic oxygen supply to organs (Urdampilleta et al., 2012). In the present review and meta-analysis, the maximum training heart rate under hypoxic conditions was significantly higher than that under normoxic conditions, consistent with results of the previous study (Urdampilleta et al., 2012). Also, under hypoxic conditions, there is a greater demand for oxygen due to reduced oxygen availability. The body may respond by increasing heart rate to compensate for the imbalance between oxygen demand and supply. This higher heart rate enables the cardiovascular system to transport oxygen to the organs and muscles at a faster rate (Heinonen, et al., 2016).
In the present meta-analysis, we did not specifically analyze the effect of sex and age in hypoxia conditioning. Several studies in the medical literature discussed the potential influences of sex or age on the response to hypoxia conditioning. In particular, responses to conditioning stimuli was considered to be sex specific, age dependent, and influenced by medical comorbidities (Verges et al., 2015). Variations in oxygen-regulated gene expression cause large interindividual differences in reaction to identical hypoxic stimulus (Verges et al., 2015). Previous data also indicated that young women have a greater compensatory vasodilator response to hypoxic exercise than males, and it was regarded that sex variations fade with age (Casey et al., 2014). Despite comparable oxygen desaturation levels, men had higher sympathetic responses to hypoxia exposure than females. Furthermore, in men but not females, the SpO2 response to resting hypoxia exposure was linked to maximal aerobic capacity (Botek et al., 2018). Nevertheless, this issue needs to be further investigated in the future.
In the present meta-analysis, we were not able to perform dose–response analyses according to levels of FiO2. The severity, duration, frequency, type (normobaric or hypobaric), and pattern of hypoxic presentation are the key factors that determine the hypoxic “dose.” An ideal “dose” should maximize the long-term physiological benefits while limiting any possible negative effects (Navarrete-Opazo and Mitchell, 2014). In the past, hypoxic training typically followed a standardized approach where everyone was exposed to the same level of hypoxia, represented by FiO2. However, few studies have directly compared the physiologic/metabolic/cardiovascular response to different FiO2 in hypoxic exercise training. Nevertheless, a recent study documented that, specifically, individuals show significant differences in their response to the same FiO2 level (Soo et al., 2020). Thus, the authors suggested using the SF index (i.e., SpO2 to FiO2 ratio), which is frequently employed in clinical settings, to assess an individual's response to hypoxia. The approach could potentially offer a more useful technique for classifying people into physiologically distinct categories.
Limitations
Several limitations are noted in the present meta-analysis. First, discrepancies in intensity, protocols, and durations of exercise training existed across the included studies and controlling for these was difficult. Levels of hypoxia by FiO2% were not precisely equal across the included studies, which may influence the outcomes differently. However, we were not able to perform dose–response analyses according to levels of hypoxia. Although sex and age may have potential effects on the response to hypoxia conditioning, subgroup analyses based on sex or age were not conducted due to the study number being limited. Some methodological limitations were presented in the included studies for systematically assessing the quality of the evidence. The overall risks of bias in each study were moderate to high, and there existed moderate-to-high heterogeneity across the studies in view of some outcomes. Overweight and obese subjects were not analyzed separately given that the population was small and some included trials did not provide such separate analysis.
Lastly, given the relatively small number of studies included, subjects could not be stratified by duration of exercise program and the effects of duration were therefore not analyzed. Future studies are still warranted to address the potential modifying effects of level of hypoxia, sex, or age on the role of hypoxic exercise training.
Conclusions
No significant differences are found in BMI, W/H ratio, or serum metabolic markers after aerobic training with hypoxic versus normoxic conditioning. However, the maximum training heart rate under hypoxic conditions is significantly higher than that under normoxic conditions. These findings need to be confirmed by future high-quality meta-analyses with larger samples and better control over exercise-related parameters.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the National Natural Science Foundation of China (Grant number 81860022; 81560020), State Key Laboratory of Pathogenesis, Prevention and Treatment of High Incidence Diseases in Central Asia Fund (Grant number : SKL-HIDCA-2022).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.