
Abstract
Zhong, Xin, Wenqiong Du, Zhaowen Zong, Renqing Jiang, Yijun Jia, Zhao Ye, and Haoyang Yang. Features of coagulo-fibrinolytic derangement due to bleeding in nonacclimatized rabbits acutely exposed to high altitude. High Alt Med Biol. 24:68–75, 2023.
Background:
The present study aimed to observe the time course of coagulo-fibrinolytic derangement due to bleeding in rabbits acutely exposed to high altitude (HA).
Materials and Methods:
Forty-eight rabbits were randomly divided into four groups and were subjected to minor bleeding at low altitude, major bleeding at low altitude, minor bleeding after acute exposure to HA, and major bleeding after acute exposure to HA. To produce minor and major bleeding, 10% and 30% of the total blood volume was removed, respectively. At designated time points, samples were taken for laboratory examination.
Results:
While minor bleeding at low altitude led to minor coagulo-fibrinolytic derangements, it led to complicated derangements at HA, which presented as an early hypercoagulable state and transition to hypocoagulable and hyperfibrinolytic states with lower clot firmness. Major bleeding at HA resulted in greater derangements of the R time, K values, the D-dimer concentration, the alpha angle, maximum amplitude, and the concentration of fibrinogen than were observed at low altitude.
Conclusions:
The extent of coagulo-fibrinolytic derangements due to bleeding in rabbits after acute exposure to HA was more severe and complicated than that at low altitude. Therefore, proper resuscitation should be applied based on these changes.
Introduction
Severe hemorrhage and hemorrhagic shock remain the leading causes of preventable death in trauma and are responsible for up to 40% of trauma-related mortality rate (Nardi et al., 2015). Efforts to achieve hemostasis are complicated by trauma-induced coagulopathy (TIC), and resuscitation protocols have evolved constantly with the deepened understanding of the pathophysiological process of hemorrhagic shock and TIC (Chesebro et al., 2009; Lustenberger et al., 2010; Cohen and West, 2011; Frith and Brohi, 2012; Gando and Otomo, 2015). Initially, resuscitation of patients with major bleeding included immediate volume support with crystalloid and/or colloid. Research in the last 20 years supports judicious crystalloid administration in conjunction with early consideration of the administration of platelets, fresh fried plasma, and packed red blood during the resuscitation phase (Gerhardt et al., 2016; Schöchl et al., 2016; Prat et al., 2017).
However, later studies found that this strategy might lead to increased morbidity and costs (Görlinger et al., 2012; Gerhardt et al., 2016; Schöchl et al., 2016; Prat et al., 2017). More recently, viscoelastic test-driven coagulation management algorithms with fibrinogen (Fib) concentrate and prothrombin complex concentrate have been found to reduce the transfusion requirements for blood products and improve outcome (Nardi et al., 2015; Theusinger et al., 2015; Fabbro et al., 2017; Kozek-Langenecker et al., 2017; Spahn et al., 2019).
The time courses of TIC are diverse according to the injury type, the extent of bleeding and shock, and the injury severity (Lustenberger et al., 2010; Mulier et al., 2012; Duan et al., 2014; van Zyl et al., 2016; Wu et al., 2017). Wu et al. (2017) found that while rabbits with hemorrhage-liver injury demonstrated shorter clot initiations (R times) and lower clotting angles than those in normal rabbits and rabbits with hemorrhage-liver injury/intestinal injury-peritonitis, the clot strength was weaker only in rabbits with hemorrhage-liver injury/intestinal injury-peritonitis, whereas the R time was longer only in rabbits with hemorrhage. These findings show that the time courses of TIC are diverse and should be monitored closely to establish a more precise resuscitation protocol to obtain a better outcome and to decrease the incidence of thromboembolic events (Cohen and West, 2011; White et al., 2014; Kozek-Langenecker et al., 2017; Spahn et al., 2019).
Besides the injury type and severity, the natural environment, such as high altitude (HA), is another factor that might influence the time course of TIC. The reduction in barometric pressure, low oxygen pressure, and low temperature at HA have profound effects on physiology, including on the coagulation system (Rocke et al., 2018; Wang et al., 2019; Zhong et al., 2022). For instance, it has been reported that acute exposure or an extended stay at HA provokes a prothrombotic or hypercoagulable phenotype in healthy tourists and mountain climbers. It has also been shown that rats acutely exposed to HA suffered less uncontrolled blood loss, more severe acidosis, an inferior tissue oxygen supply, and lower survival rates than those in low altitude (Zhao et al., 2018).
However, there are currently no data on the effects of HA on TIC after bleeding and hemorrhagic shock. In the current study, we observed the natural time course of coagulo-fibrinolytic derangement due to bleeding in nonacclimatized rabbits acutely exposed to HA and explored the possible mechanism, with a view to establish an effective resuscitation protocol.
Materials and Methods
All of the procedures involving animals were approved by the Ethics Committee of the Army Medical University of China PLA and were performed in accordance with the relevant regulations of the Ethics Committee of the Army Medical University of China PLA, P.R. China.
Animal group, instrumentation, animal model, and sample collection
Forty-eight rabbits of both sexes (weight 2.56 ± 0.32 kg; 9.1 ± 0.42 months old) were matched for body weight and age, and were then randomly divided into four groups (n = 12 per group). Group A and group B rabbits were subjected to minor and major bleeding at low altitude (400 m above sea level), respectively, and group C and group D rabbits were subjected to minor and major bleeding at HA (4,200 m above sea level), respectively. For rabbits in groups C and D, all experimental procedures were performed 2 days after arrival at HA. The animals were housed at a temperature of 18°C–20°C.
Rabbits were anesthetized with 1% pentobarbital sodium at a dose of 5 ml/kg body weight. The left carotid artery was then cannulated to allow for continuous recording of mean arterial pressure (MAP), heart rate (HR), and blood gas laboratory sampling. The right internal jugular vein was cannulated with a 5-Fr flow-directed thermodilution triple-lumen catheter to allow a blood sample to be taken for a traditional coagulation test, thromboelastography (TEG) analysis, full blood count (FBC), and enzyme-linked immunosorbent assay (ELISA). The left femoral artery was surgically exposed and cannulated to allow for rapid arterial hemorrhage. All the ends of the catheters were tunneled subcutaneously, exteriorized between scapulae, and secured. A 12-Fr Foley catheter was inserted in the urinary bladder.
After instrumentation, the animals were allowed to equilibrate for a period of 15 minutes, and baseline measurements were obtained (Kozek-Langenecker et al., 2017). The catheter was flushed with 50 μl of 0.9% NaCl without an anticoagulant after each sampling to prevent clot formation.
A fixed ratio of blood relative to body weight was removed at a fixed speed of 100 ml/min. In group A and group C rabbits, 10% of the total blood volume, for example, 8% × 10% body weight (kg) × 1,000 (ml), was removed; in group B and group D rabbits, 30% of the total blood volume, for example, 8% × 30% body weight (kg) × 1,000 (ml), was removed. To observe the natural time course of coagulopathy, no resuscitation was performed.
Blood samples were obtained at the following five time points: baseline after instrumentation (0 hours) and 1, 2, 4, and 8 hours after hemorrhage. If any rabbit died during the experiment procedure, the data at the time points before its death were used. Eight hours after injury and after the blood samples were taken, the surviving rabbits were humanely killed by an overdose injection of potassium chloride intravenously. Immediately after death, biopsies were performed to establish the presence of developmental malformations, anatomical malformations, and acute mountain sickness-related changes (e.g., pulmonary edema and brain edema), and samples of the lung, brain, heart, and aorta were fixed with 10% formaldehyde for further histological analysis if needed. At the time point of 0 hours, if any abnormality of hypercoagulable disorders/coagulation defects and FBC was found, the rabbits were ruled out and substitute rabbits were used.
Arterial blood gas analysis
According to the manufacturer's recommended procedure, 1 ml of arterial blood was analyzed by a mobile blood gas analyzer (300-g; Flextronics Manufacturing, Singapore). Parameters of saturation of oxygen (SO2%) and the lactate concentration were recorded (Zhong et al., 2022).
Full blood count
FBC analysis was performed using an automatic full blood analyzer (BC-5180 CRP; Mindray, Inc., Shenzhen, China) within 1 hour of blood collection (Jia et al., 2022; Zhong et al., 2022). The number of red blood cells (RBCs) and platelets was recorded.
TEG analysis
TEG analysis was performed with 340 μl of venous blood using a TEG analyzer (CFMS LEPU-8800; Le Pu Medical Science Technology, Inc., Beijing, China), according to the manufacturer's instructions (Prat et al., 2017; Jia et al., 2022; Zhong et al., 2022). The results of TEG testing were recorded, including the R value®, alpha angle (α), K value (K), and maximum amplitude (MA) after the MA was reached.
Traditional coagulation test
Citrated venous blood (5 ml) was collected at designated time points and centrifuged immediately at 2,500 g for 15 minutes. The supernatant was pipetted into a 10-ml propylene centrifugation tube, before centrifuging the plasma again at 2,500 g for 15 minutes. Then, the collected plasma was used to perform the traditional coagulation test with an automatic coagulation analyzer (rac-030; Shenzhen Rayto Life Science Co., Ltd., Shenzhen, China) (Jia et al., 2022; Zhong et al., 2022). The Fib concentration and D-dimer level were recorded.
Enzyme-linked immunosorbent assay
The plasma collected in the above steps was used to examine the plasma concentrations of activated protein C (APC), P-selectin, plasminogen activator inhibitor-1 (PAI-1), prothrombin fragment 1 + 2 (PF1 + 2), and syndecan-1 by ELISA. All ELISA kits were purchased from Signalway Antibody LLC (MD).
The ELISA procedures were performed in accordance with the manufacturer's manual, and the absorbance of the samples was measured at 450 nm with a microplate reader (MR-96A; Mindray, Inc.) (Jia et al., 2022; Zhong et al., 2022).
Statistical analysis
All of the data are expressed as mean ± standard deviation. Statistical analysis was performed using SPSS statistics software, version 17.0 (SPSS, Inc., Chicago, IL). We used the Kolmogorov–Smirnov test to assess whether the data followed a normal distribution. Multigroup comparisons were then conducted by one-way ANOVA if the data followed a normal distribution, and bivariate correlation analysis calculating the Pearson correlation coefficient was used to check the association between the TEG parameters and the parameters of FBC, traditional coagulation test, and ELISA. The confidence interval was set at 95%. A p-value ≤0.05 was considered significant.
Results
Mortality rate and hemodynamic and physiologic parameters of rabbits at HA and low altitude
No rabbits died in group A; one rabbit died between 4 and 8 hours after bleeding in group B; two rabbits died between 4 and 8 hours after bleeding in group C; and one rabbit died between 2 and 4 hours after bleeding, and four rabbits died between 4 and 8 hours after bleeding in group D. No developmental malformations, anatomical malformations, or acute mountain sickness-related changes (e.g., pulmonary edema and brain edema) were found (data not shown).
The values of the hemodynamic parameters, physiologic parameters, and coagulo-fibrinolytic parameters followed a normal distribution according to assessment by the Kolmogorov–Smirnov test. The baseline values of the physiologic and hemodynamic parameters varied between rabbits at low altitude and at HA (Table 1). The mean MAP, HR, and RBC count of rabbits at low altitude were slightly lower than those in rabbits that were acutely exposed to HA but with no statistically significant difference (Table 1). After bleeding, the changes in these four parameters in all four groups showed similar trends, for example, the MAP value and the RBC count decreased and the HR increased when compared with the baseline values in the same group (Table 1).
Values of Hemodynamic and Physiologic Parameters in Rabbits of Each Group
p < 0.05: compared with group B at the same time point, △△p < 0.01: compared with group B at the same time point; ▲p < 0.05: compared with group A at the same time point, ▲▲p < 0.01: compared with group A at the same time point.
The values of MAP, HR, and RBC in group C were lower than those in group A after bleeding, but with no statistically significant differences. At 2, 4, and 8 hours after bleeding, the values of MAP, HR, and RBC in group C were significantly lower than those in group D (Table 1).
Before bleeding, the platelet count of the rabbits in groups C and D was significantly lower than that of rabbits in groups A and B. After minor and major bleeding, the platelet count decreased gradually at the examined time points, and the counts were higher in rabbits at low altitude than those in rabbits at HA at each time point (Table 1).
The baseline lactate concentration in rabbits at HA was higher than that in rabbits at low altitude. After bleeding at the same percentage, the lactate concentrations were higher in rabbits that were acutely exposed to HA than in rabbits at low altitude (Table 1).
The baseline SO2% in group A and group B rabbits was higher than that in group C and group D rabbits, but with no statistically significant differences. After bleeding at the same percentage, the SO2% was lower in rabbits that were acutely exposed to HA than in rabbits at low altitude (Table 1).
Acute exposure to HA aggravated coagulo-fibrinolytic derangements after bleeding
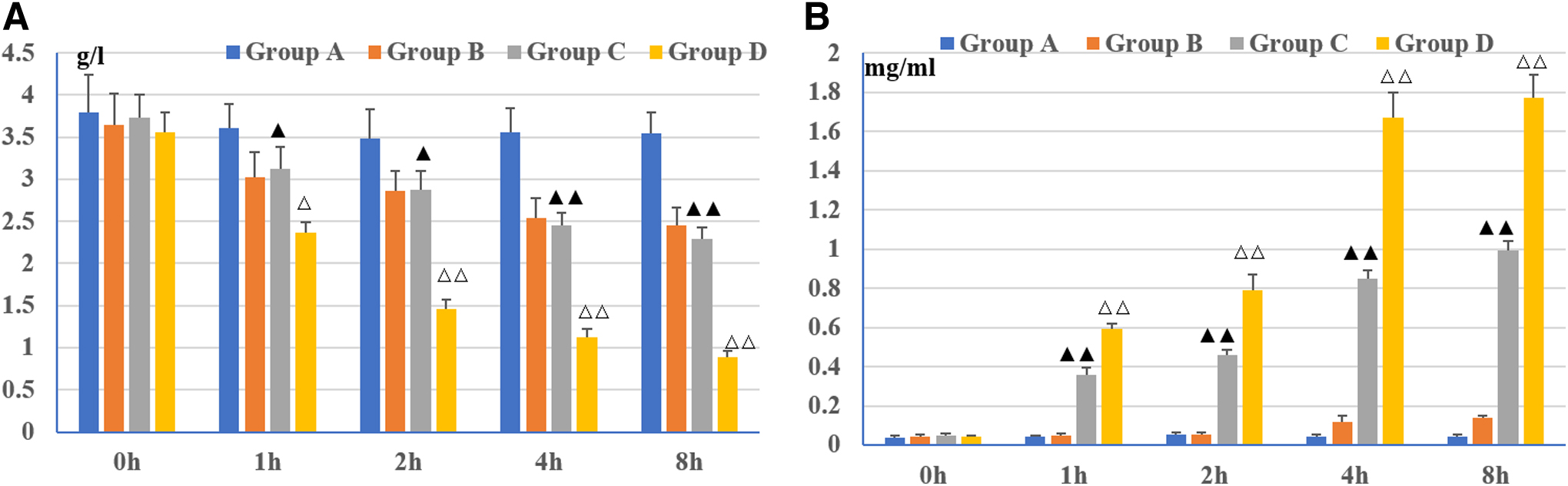
In rabbits at low altitude, minor bleeding led to minor changes in coagulo-fibrinolytic parameters, including the R value, K values, alpha angle, MA, Fib, and D-dimer (Table 2 and Fig. 1). In contrast, minor bleeding of rabbits at HA led to different effects on the coagulo-fibrinolytic system. One hour after bleeding, the R values were significantly decreased, but they then increased at the later time points when compared with the baseline values in the same group and with the values at the corresponding time points in group A (Table 2). At each time point after minor bleeding, the K value and the concentration of D-dimer were significantly higher in group C rabbits than in group A rabbits, whereas the alpha angle, MA, and Fib concentration were significantly lower in group C rabbits than those in group A rabbits (Table 2 and Fig. 1).
Values of each parameter examined by the traditional coagulation test in the rabbits of each group.
Values of Thromboelastography in Rabbits of Each Group
p < 0.05: compared with group B at the same time point, △△p < 0.01: compared with group B at the same time point; ▲p < 0.05: compared with group A at the same time point.
In rabbits at low altitude, major bleeding led to obvious changes in the coagulo-fibrinolytic system. One hour after bleeding, the R values were significantly decreased, but were then increased 2, 4, and 8 hours after bleeding compared with the baseline values in the same group (Table 2 and Fig. 1). In group B rabbits, the K values and D-dimer concentration significantly increased after bleeding, whereas the alpha angle, MA, and the concentration of Fib decreased after bleeding compared with the baseline values in the same group (Table 2 and Fig. 1).
In group D rabbits, the baseline R values were significantly lower than those in group B rabbits (Table 2). One hour after bleeding, the R values decreased and were significantly lower than those in group B rabbits (Table 2). The hypercoagulable state then switched to a hypocoagulable state at the later time points, and the R values were significantly higher than the baseline values in the same group and when compared with the values at the corresponding time points in group B (Table 2). Moreover, in group D rabbits, the change patterns of the K values, D-dimer concentration, alpha angle, MA, and Fib concentration were similar to those in group B rabbits, although with increased values observed in group D rabbits (Table 2 and Fig. 1).
In addition, the platelet count and the concentration of Fib positively correlated with the MA values (r = 0.271, p < 0.01, and r = 0.436, p < 0.01, respectively) and the alpha angle (r = 0.422, p < 0.01, and r = 0.458, p < 0.01, respectively).
Enzyme-linked immunosorbent assay
The level of syndecan-1, a biomarker for endothelial injury, is upregulated by hypoperfusion and hypoxia. Hypoxia caused by acute exposure to HA led to an increased baseline level of syndecan-1 (Table 3), contributing to more severe coagulation (decreased R values) in group C and D rabbits 1 hour after bleeding. This was supported by the decreased R value and the increased level of PF1 + 2, a measure of total thrombin generation, in rabbits in groups C and D (Table 3). After bleeding, the level of syndecan-1 continued to increase gradually in the four groups at the later time points, and the level was higher in rabbits in groups C and D at the same time points compared with that in rabbits in groups A and B.
Plasma Concentrations of Biomarkers in Rabbits of Each Group Determined by Enzyme-Linked Immunosorbent Assay
p < 0.05: compared with group B at the same time point, △△p < 0.01: compared with group B at the same time point; ▲p < 0.05: compared with group A at the same time point, ▲▲p < 0.01: compared with group A at the same time point.
This contributed to the shift from a hypercoagulable state to a consumptive hypocoagulable state; and a more severe hypocoagulable state was found in rabbits in groups C and D, as indicated by the higher R values (Table 2) and the decreased level of PF1 + 2 (Table 3).
After acute exposure to HA, the level of APC increased in rabbits in groups C and D, and hypoperfusion further increased the level of APC (Chesebro et al., 2009; van Zyl et al., 2016). The level of APC was higher in rabbits in groups C and D at the same time points compared with that in rabbits in groups A and B (Table 3). APC has potent anticoagulant effects, and a positive correlation was found between the level of APC and R values (r = 0.376, p < 0.01). In addition, APC could inhibit PAI-1 (Chesebro et al., 2009; van Zyl et al., 2016).
The levels of PAI-1 were lower in rabbits in groups C and D at the same time points compared with those in groups A and B (Table 3), and a negative correlation was found between the level of APC and PAI-1 (r = −0.432, p < 0.01). The decreased level of PAI-1 in turn activated fibrinolysis, as confirmed by increased D-dimer concentrations (Hayakawa et al., 2017). A positive correlation was found between the level of APC and D-dimer (r = 0.276, p < 0.01), and a negative correlation was found between the level of PAI-1 and D-dimer (r = −0.389, p < 0.01).
In addition, the number of platelets decreased 1 and 3 days after acute exposure to HA due to platelet activation (Lehmann et al., 2006), as confirmed by the increased concentration of P-selectin (Table 3); this may explain the reduced baseline platelet count in rabbits in groups C and D.
Discussion
In this study, we found that the natural time course of coagulo-fibrinolytic derangement due to bleeding in nonacclimatized rabbits acutely exposed to HA was different from that in rabbits at low altitude. While minor bleeding led to minor changes in the coagulo-fibrinolytic parameters of rabbits at low altitude, it led to complicated coagulo-fibrinolytic derangement in rabbits that were acutely exposed to HA. This coagulo-fibrinolytic derangement presented as an early hypercoagulable state (1 hour after bleeding) and transition to hypocoagulable and hyperfibronolytic states with lower clot firmness (lower MA) (2, 4, and 8 hours after bleeding). Major bleeding in rabbits at low altitude resulted in a similar trend on the coagulo-fibrinolytic system as that in rabbits at HA; however, when major bleeding occurred at HA, the extent was more severe than that observed in rabbits at low altitude.
Several factors contributed to the different features of coagulo-fibrinolytic derangement due to bleeding at HA compared with that at low altitude. First, hypoxia and acidosis at HA induce further injury to the endothelium in addition to hypoperfusion (Maegele et al., 2014; Lafuente et al., 2016; Friedrich et al., 2019; Zeineddin et al., 2021), which induces a stronger coagulation process than that observed in rabbits at low altitude. Second, platelet activation at HA further initiates the coagulation process (Lehmann et al., 2006). These two factors lead to stronger coagulation in rabbits acutely exposed to HA than in those at low altitude. Third, this hypercoagulable state at the hyperacute stage exhausted more coagulation factors, platelets, and Fib in rabbits in groups C and D than in rabbits in groups A and B, resulting in consumptive hypocoagulability (Mulier et al., 2012; Duan et al., 2014; Wu et al., 2017).
Fourth, hypoxia along with hypoperfusion led to greater activation of APC in rabbits in groups C and D. APC exerts anticoagulation effects and promotes fibrinolysis by inhibiting PAI-1 (van Zyl et al., 2016). Fifth, the decreased platelet count and Fib concentration observed in rabbits in groups C and D resulted in lower MA, for example, lower clot firmness.
The findings of the current study have practical significance. First, the extent of coagulo-fibrinolytic derangement after acute exposure to HA was more severe than that observed in rabbits at low altitude; even minor bleeding led to obvious coagulo-fibrinolytic derangement in rabbits acutely exposed to HA, which could lead to death. This reminds us that patients with bleeding (even minor bleeding) should be treated cautiously, at HA. Second, coagulo-fibrinolytic derangement after bleeding in rabbits acutely exposed to HA presented as significantly decreased Fib, R values, and MA, as well as increased fibrinolysis, indicating that point of care coagulation management with early calculated goal-directed therapy is necessary, as is targeted resuscitation to increase Fib, prothrombin complex concentrate, and platelets and to inhibit hyperfibrinolysis (Görlinger et al., 2012; Nardi et al., 2015; Kozek-Langenecker et al., 2017; Spahn et al., 2019).
Third, the causes of death in rabbits after acute exposure to HA have clinical significance. While no developmental malformations, anatomical malformations, and acute mountain sickness-related changes were found in the deceased animals, the extent of blood loss, hypovolemic shock, and coagulo-fibrinolytic changes was more striking in group B and group D animals, in which the mortality rates were higher than those in group A and group B, respectively. Thus, we postulated that the deaths were mainly caused by blood loss and hypovolemic shock in animals after acute exposure to HA. Given the important role of coagulo-fibrinolytic changes in blood loss and hypovolemic shock, we postulated that reversion of the coagulo-fibrinolytic changes could help to relieve the extent of blood loss and hypovolemic shock, and in turn reduce the mortality rate of the animals.
The current study has several limitations. First, only rabbits that were acutely exposed to HA were investigated. The baseline physiological and coagulation parameters of acclimated and inhabitants are different from those who are acutely exposed to HA (Kotwal et al., 2007; Rocke et al., 2018), and thus, the effects of bleeding on coagulo-fibrinolytic derangement may also be different. We plan to investigate this further in future work. Second, the longest time point observed in the current study was 8 hours. The main reason for this is that increased sampling will have similar effects as bleeding and will complicate the results.
Third, TIC is a complex pathophysiological process that can be caused by either a single factor (e.g., hemorrhagic shock) or multiple factors (e.g., combined trauma and hemorrhagic shock) (Chesebro et al., 2009; Duan et al., 2014; Kornblith et al., 2019). In real clinical practice, trauma and hemorrhage occur simultaneously, and the mechanism and extent of TIC are different from those observed in simple hemorrhage (Chesebro et al., 2009; Duan et al., 2014). Indeed, Chesebro et al. (2009) demonstrated that mice with combined trauma and hemorrhage had a significantly elevated activated partial thromboplastin time compared with those with simple hemorrhage. To better control the volume of bleeding, we only observed the feature of coagulo-fibrinolytic derangement due to bleeding, but not due to combined trauma and bleeding. Future research on the influence of combined trauma and hemorrhage on coagulo-fibrinolytic derangement will be performed to offer more practical information from a clinical perspective.
Fourth, accumulating evidence suggests that sex differences might lead to difference in post-traumatic pathophysiological conditions, including hemorrhagic shock and TIC (Brown et al., 2012; Taghavi et al., 2021; Smith et al., 2022). However, the existing data are conflicting, with one study reporting that severely injured women with hemorrhagic shock had a higher survival rate compared with their male counterparts (Haider et al., 2010), while another found that there was no difference in survival rate between male and female injured patients (Taghavi et al., 2021; Smith et al., 2022) or even an increased mortality rate in women with acute traumatic coagulopathy when compared with males (Brown et al., 2012).
In our experiments, we found no significant difference in the examined coagulation parameters between male and female rabbits; thus, the data of male and female rabbits were reported together. However, as the number of male and female rabbits was limited (six male and six female rabbits in each group, respectively), further research should be conducted on the influence of sex on coagulo-fibrinolytic derangement due to bleeding at HA.
In summary, the extent of coagulo-fibrinolytic derangement in rabbits after acute exposure to HA was more severe than that in rabbits at low altitude, which may result in a high mortality rate. Therefore, proper resuscitation should be applied based on these changes.
Footnotes
Acknowledgment
Authors' Contributions
All coauthors have reviewed and approved the article before submission. The authors' contributions are as follows: X.Z.: development of animal models and data analysis; Z.Z.: conceptualization, original draft, data interpretation, and funding acquisition; R.J.: traditional coagulation test; Y.J.: arterial blood gas analysis; Z.Y.: full blood count and TEG analysis; W.D.: ELISA; Haoyang Yang: data collection.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Key logistics scientific project of the “Thirteenth Five Year Plan” of Medical Research of PLA (ALJ19J001), Key Clinical Innovation Project of Army Medical University and XinQiao Hospital (CX2019JS107/2018JSLC0023).