
Abstract
Kharel, Sanjeev, Suraj Shrestha, Samriddha Raj Pant, Suman Acharya, Amit Sharma, Santosh Baniya, and Sanjeeb S. Bhandari. High-altitude exposure and cerebral venous thrombosis: an updated systematic review. High Alt Med Biol. 24:167–174, 2023.
Background:
High altitude (HA) may increase the risk of cerebral venous thrombosis (CVT). Differentiating it from other HA illnesses is crucial for prompt treatment and better outcomes. We aimed to summarize the clinical data, etiology, and risk factors of this poorly understood entity at an HA.
Materials and Methods:
A systematic literature search of various databases, including PubMed, Embase, and Google Scholar, was done using relevant keywords; cerebral venous thrombosis; HA, up to May 1, 2022.
Results:
A total of nine studies, including 75 cases of CVT at HA (3,000–8,848 m), with 66 males and 9 females, were included in this review. Headache and seizure were the most common clinical presentations. Smoking, drinking habits, and the use of oral contraceptive pills (OCP) were the most common risk factors for the development of CVT. Similarly, various underlying hypercoagulable states were also present among cases of CVT associated with HA exposure.
Conclusion:
Our review concludes that HA exposure can predispose individuals with risk factors such as preexisting hypercoagulable states, smoking, drinking habits, and use of OCP to an increased risk of CVT.
Introduction
Cerebral venous thrombosis (CVT) is caused by partial or complete occlusion of the major cerebral venous sinuses or the smaller feeding cortical veins, which predispose to the risk of venous infarction and hemorrhage (Ulivi et al., 2020). Young adults (median age of 37 years), children, and females of child-bearing age are commonly the affected population, with an estimated prevalence of 1.3–1.6 cases per 1,000,000 people and accounting for 0.5% of all stroke causes (Bushnell and Saposnik, 2014; Silvis et al., 2017).
CVT is frequently reported as a complication of high altitude (HA) exposure. Due to its rarity, diverse radiologic and clinical findings, and the symptomatic similarities shared with other more commonly occurring neurological conditions at HAs such as high-altitude cerebral edema (HACE), the diagnosis of CVT is often delayed (Coutinho et al., 2012). The increased propensity has been attributed to different factors at HA, including dehydration, vomiting, alteration of hemostasis secondary to hypoxia-induced polycythemia coupled with volume depletion, immobility, and congenital or acquired hypercoagulability (Zavanone et al., 2017).
As it is important to treat CVT as soon as possible, reducing the delay in diagnosis by a more thorough understanding of the clinical presentation will benefit patients in regions where medical services are often less available (Hassan et al., 2019). There are no guidelines for patients with neurological diseases traveling at HAs. Similar is the case for CVT with little evidence that HA exposure is a risk factor (Falla et al., 2021). A previous systematic review with only 17 cases could neither clearly describe HA as a risk factor nor estimate the incidence of CVT at high altitude (Zavanone et al., 2017).
Thus, we aimed to update the review and include new retrospective studies to give a brief overview of clinical symptoms, diagnostic assay, hypercoagulable assay, risk factors, and treatment; and discuss the multifactorial etiology for the occurrence of CVT.
Materials and Methods
Study design
This study is reported according to the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines (Liberati et al., 2009). A systematic review was conducted, including published scientific reports, original research, abstracts, case reports, case series, editorials, and commentary letters. Our research question was whether HA exposure can predispose to CVT.
Eligibility criteria
Original research articles published in English in all ethnic groups that reported on patients >18 years who met the following criteria were included:
Population: Adults of both sexes, all ages, and ethnic backgrounds diagnosed with CVT. Study designs: Case reports, case series, pooled studies, and prospective or retrospective studies published in English were deemed eligible for inclusion in this review. Exposure: We included every elevation above 3,000 m that was considered HA by the authors. The outcome of interest: CVT risk at HA and its prognosis.
The exclusion criteria were as follows:
Studies reporting CVT that did not consider HA within the analysis.
Studies reporting other venous thrombosis or deep vein thrombosis (DVT) in HAs.
Studies reporting unclear data or not enough data on altitude.
Studies published in a language other than English.
Search strategy
The studies were searched in PubMed, Google Scholar, and Embase up to the publication date of May 1, 2022. A database search was conducted using Boolean logic, and the Boolean search operators “AND” and “OR” were used to link search terms. For advanced PubMed and Embase searches, MeSH terms and Emtree terms were used. The search strategy for PubMed was as follows: (“Cerebral Venous Thrombosis” OR “Cerebral Venous Sinus Thrombosis”) AND (“high altitude” OR “altitude illness”). Similarly, the search strategy for Embase was: (“cerebral sinus thrombosis”/exp OR “cerebral sinus thrombosis”) AND (“altitude” OR “altitude disease”). The search was also expanded to include preprint servers and thesis repositories, and any additional references were found by hand-searching the reference lists from the selected articles.
Study selection
Two authors (SK and SS) initially screened the title and abstract of the selected studies that met our inclusion criteria and was subsequently verified with a third reviewer (S.A.). Articles passing the initial screen were later reviewed in full by two reviewers (S.K. and S.S.). Any uncertainties about including a specific article in the review were resolved by consensus.
Data extraction
The final included studies were compiled and the data were extracted by the two primary reviewers (S.K. and S.S.) using standardized data extraction formats. Reviewers matched data after extraction before returning to articles where disagreements arose. Any discrepancies were resolved with the help of the third reviewer (S.A.). The following information was extracted in three categories as follows: (1) Clinical characteristics: author, publication year, number of patients with CVT, mean age, male/female, average altitude, average stay, acclimatization days, hemoglobin level, clinical symptoms, hypercoagulable state, and predisposing risk factor. (2) Imaging characteristics: author, magnetic resonance imaging (MRI) findings, and CT venography (CTV)/magnetic resonance venography (MRV) findings. (3) Treatment and prognosis: author, treatment opted, and prognosis (modified Rankin Scale [mRS] score).
If any of the required data were missing, were not reported in the article, or were reported in an unusual format, the corresponding authors of the respective articles were contacted via email for clarification. In such cases, supplementary material related to the main article was also investigated.
Results
Search results and study selection
In total, 50 (PubMed-19, Embase-21, Google Scholar-10) articles were identified after a thorough database search (Fig. 1). After excluding duplicates and those not meeting the inclusion criteria, nine studies were reviewed for data collection (Hassan et al., 2019; Khan, 2016; Khanal et al., 2016; Khattar et al., 2019; Kim et al., 2017; Nair et al., 2016; Paliwal et al., 2019; Ye et al., 2017; Zavanone et al., 2017). We excluded all the case series and case reports published before July 2016. This is to prevent population overlap, as we included a study by Zavanone et al. (2017), which is a pooled study of all case reports and series published up to July 2016. Figure 1 shows the results of our literature search and selection.
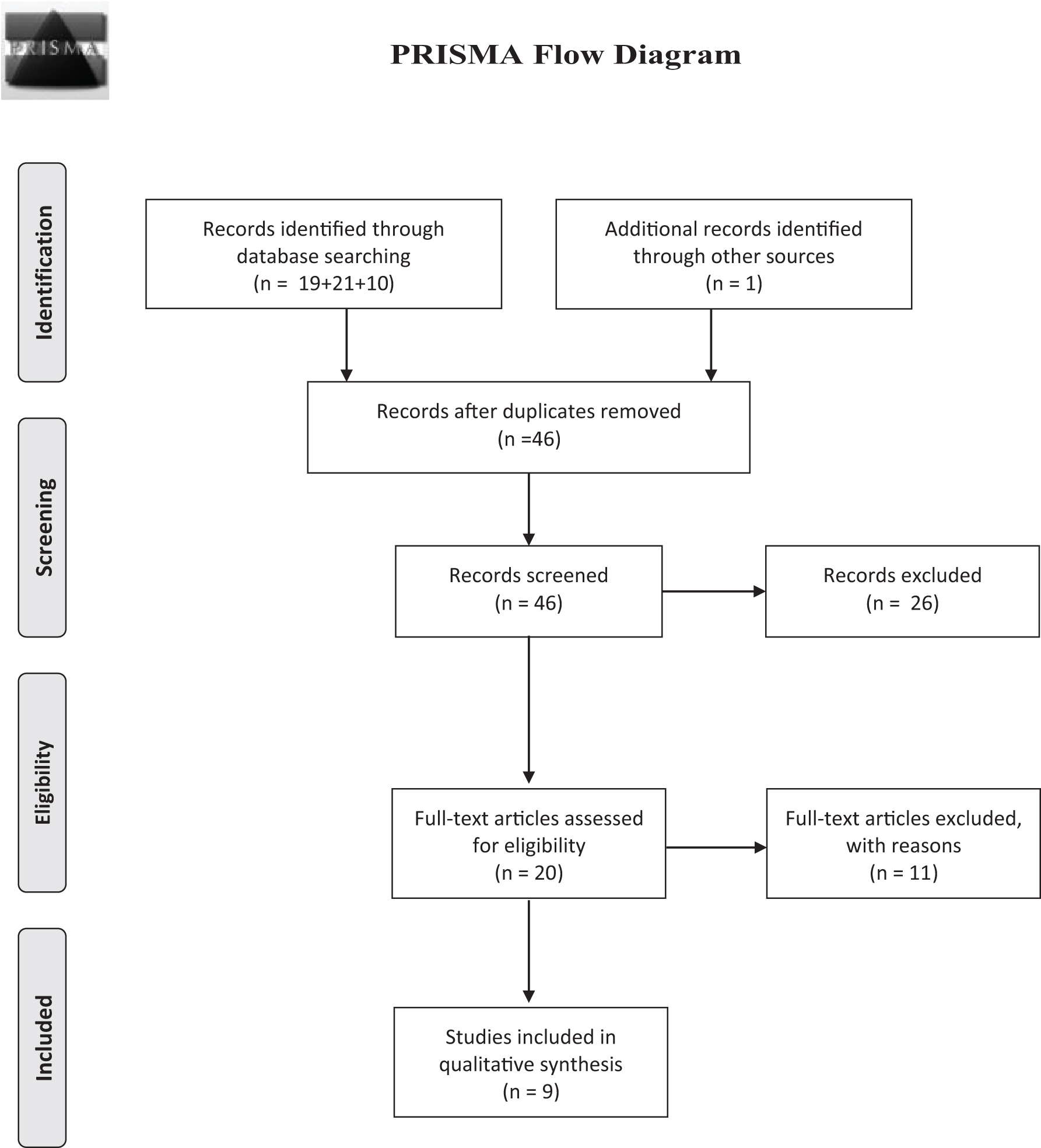
PRISMA flow diagram for selection of studies. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses. From Moher et al., 2009.
The characteristics of each included study discussed below are summarized in Table 1. The imaging characteristics are described in Table 2, while the treatment and prognosis portions are depicted in Table 3.
Characteristics of the Cerebral Venous Thrombosis Patients at High Altitude
CVT, cerebral venous thrombosis; GCS, Glasgow Coma Scale; NA, not available; NIHSS, NIH Stroke Scale; OCP, oral contraceptive pill.
Imaging Characteristics of Patients Diagnosed with Cerebral Venous Thrombosis
CTV, CT venography; IJV, internal jugular vein; MRV, magnetic resonance venography.
Treatment Received Along with Management of Cerebral Venous Thrombosis Patients
LMWH, low-molecular-weight heparin.
Study findings and characteristics
The included studies were published from 2016 to 2019. The systematic review included articles from 1983 to 2016 (Zavanone et al., 2017). Five articles were case reports (Khan, 2016; Khanal et al., 2016; Kim et al., 2017; Nair et al., 2016), two were retrospective studies (Hassan et al., 2019; Khattar et al., 2019), and only one was a case series (Paliwal et al., 2019). A total of 75 cases were found to be diagnosed with CVT at HAs, including 66 male and 9 female patients. All the cases had HA exposure ranging from an altitude of 3,000–8,848 m and the average duration of HA stay was >2 weeks in all except one case with an average of 107.8 days in the largest retrospective study of 28 CVT cases. One case was reported to have CVT on the 5th day of HA exposure.
One retrospective study used the NIH Stroke Scale (NIHSS) as an initial assessment technique with an average mean score of 5.3 (Hassan et al., 2019), while another retrospective study and two other case studies used the Glasgow Coma Scale (GCS), which ranged from 8 to 12 out of 15 (Khattar et al., 2019; Paliwal et al., 2019; Ye et al., 2017).
Clinical symptoms
The most common clinical symptom at the time of presentation with HA exposure was headache (22 cases), followed by seizures (8 cases), vomiting (6 cases), limb weakness (5 cases), dizziness (5 cases), unconsciousness (5 cases), difficulty in speech (5 cases), visual difficulty (3 cases), and altered sensorium (2 cases). Other various symptoms are tabulated in Table 1.
Risk factors
Smoking and drinking habits were the most reported predisposing risk factors. In addition, use of oral contraceptive pills (OCP) and trauma were other reported risk factors (Khattar et al., 2019).
Hypercoagulable states
Mean hemoglobin was higher than normal in a retrospective study with the highest number of cases (28) and all other cases that reported hemoglobin had also polycythemia with an exception of a single case. Secondary polycythemia, low C4 levels, elevated homocysteine level, an increased anticardiolipin antibody titer, protein C and protein S deficiency, and factor V Leiden mutation were the reported hypercoagulable states (Table 1).
Diagnostic assays
D-Dimer has a high negative predictive value for the diagnosis of cerebral sinus venous thrombosis, but a low positive predictive value that was reflected in this study with raised D-Dimer in 30 patients while it was reported normal in only one case report.
As described in Table 2, CTV/MRV findings showed the sites of the thrombus. Hassan et al. showed that 39.3% had normal MRI findings, while 25% showed signs of hemorrhage and 14.3% showed infarcts. The left parietotemporal area was the most commonly involved area (17.9%). On MRV, the left transverse sinus (25%) and superior sagittal sinus (22.5%) were the commonly involved sinuses (Hassan et al., 2019). In Khattar et al. (2019), CT in all cases had a hemorrhagic conversion, and only then a CT venography was done.
Paliwal et al. (2019) used noncontrast CT and CTV/MRV to diagnose and locate the lesions; right and left transverse sinus, superior sagittal, straight, and sigmoid sinuses were found to be involved. A case of Galen vein thrombosis was also found (Ye et al., 2017). Autopsy findings also helped in diagnosing CVT in a case (Khan, 2016). Superior sagittal, right and left transverse, and straight sinuses were the commonly involved sites in MRV/CTV in the systematic review by Zavanone et al (2017).
Management/treatment
As described in Table 3, anticoagulant therapy such as low-molecular-weight heparin (LMWH) (most commonly used), directly acting oral anticoagulants (DOACs) (rivaroxaban), and warfarin was used to manage the CVT. Decompressive craniotomy and intravenous mannitol were also used as treatment modalities (Khattar et al., 2019).
Outcomes/prognosis
Hassan et al. found that 53.6% of the patients had an mRS score of 0, and 7% were found to have an mRS score of 2 with the mortality of one patient on follow-up at 30 days (Hassan et al., 2019). Khattar et al. (2019) used the Glasgow Outcome Scale (GOS) at discharge. Twelve patients (57%) had mild or no neurological disability (GOS 5), while seven patients (33%) had outcomes ranging from vegetative state to severe disability (GOS 2–4) and two died (GOS = 1). One armed personnel also died during treatment among the three reported cases of CVT among army personnel (Paliwal et al., 2019). In the rest of the cases, one died, while the other five had good outcomes. Of the three patients who expired and had their imaging, two of them had intracerebral hemorrhage along with CVT.
Discussion
Our review is an updated systematic review, including a total of 75 cases of CVT diagnosed at HAs, providing a brief overview of clinical symptoms, risk factors, and underlying hypercoagulable states of CVT along with diagnostic modalities, treatments opted, and their outcomes and prognoses.
Vascular thrombosis in the form of DVT with or without pulmonary embolism, CVT, and arterial thrombosis has been frequently reported from HAs. Cerebral venous thrombosis is a common autopsy finding in patients who die at HAs, but due to its rarity and diagnostic dilemma with various other HA illnesses, the exact occurrence of CVT at HAs is yet to be determined (Dickinson et al., 1983; Song et al., 1986). However, it has been observed that CVT is the most common venous thromboembolic complication at HAs with a male predisposition. This is in stark contrast to the known increased risk of CVT in women at lower elevations (Bushnell and Saposnik, 2014; Choudry et al., 2021; Nair et al., 2022). The reason behind high male caseloads may be attributed to male dominance among soldiers and mountaineers, which made up most of the cases.
A recent study on Indian soldiers at HA (>15,000 ft) published in Lancet found a higher incidence of both arterial and venous thrombosis in healthy subjects at HA when compared with that reported in the literature at sea level. These index cases had increased coagulation, endothelial dysfunction, and inflammation marker with decreased levels of natural anticoagulants and dampened fibrinolysis compared with healthy subjects (Nair et al., 2022).
HA is known to have a significant impact on cerebral physiology, blood flow, and various hypoxia-induced factors that raise blood viscosity and hematocrit (Ainslie and Subudhi, 2014). Gupta et al. (2017) emphasized the presence of an active proinflammatory response to hypoxia using innate and adaptive immune cells resulting in aggravated venous thrombosis. This proinflammatory state develops in response to HA due to the action of hypoxia-induced factor 1-alpha (HIF-1a) on the NLR Family Pyrin Domain Containing 3 gene.
Polycythemia is suggested to be one of the primary causes of CVT at HAs, with reported Hb levels ranging as high as 19 mg/dl. Another study showed a statistically significant increase in Hb levels in soldiers posted in HA regions (Kotwal et al., 2007; Zavanone et al., 2017). An underlying prothrombotic state, such as congenital thrombophilia, appears to be the most common risk factor for developing CVT in an HA setting. A systematic review showed that 9 out of 14 reported cases had an underlying hypercoagulable state, with secondary polycythemia and factor V Leiden mutations being the most common (Zavanone et al., 2017). Heterozygous factor V Leiden mutation increases the risk of thromboembolism by sevenfold, whereas homozygous mutation increases the risk by eightfold (Segler, 2001).
Pichler Hefti et al. (2010) showed that ascent to HA resulted in hypercoagulability in the form of increased D-dimer levels, prothrombin time, and activated protein C resistance. Other possible mechanisms that predispose an individual to CVT include dehydration, hypoxia-induced hemostatic changes such as increased platelet activity, volume depletion, reduced mobility, inflammatory changes secondary to endothelial injury that accelerates the thrombotic process, hyperhomocysteinemia, exercise, and coagulation pattern triggered by hypothermia (Zavanone et al., 2017). In addition, genetic or acquired prothrombotic conditions, infections, malignancy, pregnancy, and use of oral contraceptives are some of the established risk factors of CVT (Ferro et al., 2004). Also, a strong correlation has been shown between smoking and thrombosis. In a study, 75% of evaluable cases in the thrombosis group were smokers compared with 22% in the control group (Choudry et al., 2021).
Recently, Sagoo et al. (2017) demonstrated that hypoxia (after 22 hours) can increase parenchymal whole-brain volume and also cause varying degrees of venocompression at the level of small and deep cerebral veins. This can restrict the venous outflow and thus theoretically predispose to the development of thrombosis along with other risk factors.
The diagnosis of CVT may be difficult, as some neurological disorders arising at HA can mimic CVT, including acute mountain sickness (AMS), HACE along with other neurological disorders such as ischemic stroke, and intracranial bleeding (Wilson et al., 2009). Noninvasive imaging using intravenous contrast agents significantly increases the sensitivity of diagnosis, with MRV as the most sensitive diagnostic imaging modality (Lafitte et al., 1997; Silvis et al., 2017). CT venography is a reasonable alternative to MRV for the diagnosis of CVT (Ferro et al., 2017). As stated earlier, the D-dimer levels have a high negative predictive value and are often utilized in the screening of venous thrombotic events; however, they cannot be reliably used to confirm CVT due to their poor positive predictive value (Dentali et al., 2012).
The first-line treatment of CVT is anticoagulation, using either subcutaneous body-weight-adjusted LMWH or dose-adjusted intravenous heparin, with at least doubled activated partial thromboplastin time. Concomitant intracerebral hemorrhage related to CVT is not a contraindication for heparin therapy (Einhäupl et al., 2010). Initial presentation with extensive hemorrhages associated with signs of elevated intracranial pressure (ICP), midline shift, or impending brain herniation warrants urgent surgical intervention with decompressive craniectomy (Zuurbier et al., 2015). Twenty-five percent of patients with CVT deteriorate despite adequate anticoagulation (Bushnaq et al., 2018). According to the International Study of Cerebral Vein and Dural Thrombosis (ISCVT), 13% had poor neurological outcomes, whereas 4.3% were recorded to have died during the acute phase.
Bushnaq et al. demonstrated that the most significant predictor of poor prognosis is an altered mental status. Other indicators for poor prognosis are seizures, papilledema, hyponatremia (<139 mEq/l), low platelet count (<225 × 109/l), and involvement of more than one sinus (Bushnaq et al., 2018). It should be kept in mind that unlike other HA illnesses such as HACE and AMS, the use of acetazolamide or steroids in acute CVT is discouraged (Ferro et al., 2017).
Oral anticoagulation, either warfarin or DOACs, is continued after the acute phase for 3–12 months to prevent the recurrence of CVT (Ferro et al., 2019; Ferro et al., 2017).
Careful history-taking and medical screening should be performed individually before going to high-altitude. There are no evidence-based guidelines to make firm recommendations; however, it should be considered to advise all travelers to HA to drink adequately (2–3 L of water/day) to avoid dehydration and hyperviscosity, avoid strenuous activity at the high summit, and those with known predisposing factors to thrombosis to avoid altitude sickness (e.g., HACE and the increased ICP, which further compromise the cerebral blood flow) considering all the helpful measures (e.g., acclimatization and specific treatment). In addition, women on oral contraceptives should consider the risk of being exposed to HA (Falla et al., 2021). OCP should be discontinued by females before embarking on an HA journey (Ferro et al., 2017).
Although screening for thrombophilia is not recommended for CVT at normal altitude (Ferro et al., 2017), studies showing a strong relationship between the two should prompt further research on whether thrombophilia screening should be incorporated into the diagnostic protocol for CVT cases presenting in an HA setting. Those set to experience hypobaric hypoxic conditions should also get routine blood counts to screen for polycythemia and thrombocytosis. Screening for vitamin B12 and folate levels can help detect a state of hyperhomocysteinemia (Syed et al., 2018).
Although the aim was to know the association of CVT occurrence with HA exposure, the paucity of data without the pertaining analysis in included studies made it difficult to get to a clear conclusion.
Conclusion
Our review concludes that HA exposure can predispose individuals to an increased risk of CVT owing to different risk factors such as underlying hypercoagulable states, smoking, drinking habits, and use of OCP. Moreover, a careful history and medical screening should be performed individually before going to altitude. Additionally, larger scale studies are required to further clarify the association.
Footnotes
Acknowledgment
We would like to thank Prof. Dr. Buddha Basnyat for his valuable suggestions.
Authors' Contributions
S.K.: Conceptualization, methodology, software, writing—original draft, and writing—review and editing. S.S.: Conceptualization, methodology, software, writing—original draft, and writing—review and editing. S.R.P.: Conceptualization, methodology, software, writing—original draft, and writing—review and editing. S.A.: Conceptualization, writing—original draft, and writing—review and editing. A.S., S.B., and S.S.B: Conceptualization, writing—original draft, writing—review and editing, and supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.