
Abstract
Song Zhen, Anxin Zhang, Jie Luo, Guanghai Xiong, Haibo Peng, Rang Zhou, Yuanfeng Li, Hongqiang Xu, Zhen Li, Wei Zhao, and Haoxiang Zhang. Prevalence of high-altitude polycythemia and hyperuricemia and risk factors for hyperuricemia in high-altitude immigrants. High Alt Med Biol. 24:132–138, 2023.
Background:
Few studies have investigated the epidemiology of chronic mountain sickness (CMS) in high-altitude immigrants. This study evaluated the prevalence of polycythemia and hyperuricemia (HUA) and risk factors for HUA in high-altitude immigrants.
Methods:
A cross-sectional study was conducted with 7,070 immigrants 15–45 years of age living on the Tibetan Plateau between January and December 2021. Information from routine physical examinations was obtained from each participant. Binary logistic regression analysis was performed to determine the correlation of several risk factors for HUA.
Results:
The prevalence of high-altitude polycythemia (HAPC) and HUA was 25.8% (28.7% in males and 9.4% in females) and 54.2% (59.9% in males and 22.5% in females), respectively. The highest prevalence of HAPC in males and females was observed in participants 26–30 and 21–25 years of age, respectively. The highest prevalence of HUA in both males and females was observed in participants 26–30 years of age. Binary logistic regression analysis showed that age, sex, and hemoglobin (Hb) concentration were risk factors for HUA, among which age was a negative factor and male sex and Hb concentration were positive factors.
Conclusions:
Immigrants are more susceptible to HAPC and HUA. The high prevalence of CMS of immigrants may be associated with Hb concentration, age, and sex.
Background
High-altitude polycythemia (HAPC) is a common chronic mountain sickness (CMS) in high-altitude populations. It is defined as excessive erythrocytosis, which is induced by chronic exposure to hypobaric hypoxia environments at high altitude (Samuels, 2004). HAPC is clinically diagnosed based on a hemoglobin (Hb) concentration ≥165.0 g/l in females and 185.0 g/l in males, respectively (Wadleigh and Tefferi, 2010).
HAPC can lead to various symptoms such as headache, fatigue, dizziness, and sleep disturbance, and even result in secondary body injuries such as blood viscosity and kidney injury (Arestegui et al., 2011; Guan et al., 2015; Palubiski et al., 2020; Wang et al., 2022). It has been reported that the incidence of HAPC in the Qinghai-Tibet Plateau is ∼5.0%–18.0% (Leon-Velarde et al., 2005). The red blood cell (RBC) count and incidence of HAPC among immigrants are obviously higher than those in original high-altitude inhabitants with their genetic adaptation to hypobaric hypoxia environment (Fan et al., 2018; Jiang et al., 2014; Wu, 2005).
Hyperuricemia (HUA), characterized by rising serum uric acid (SUA) levels (>360.0 μmol/l in females and >420.0 μmol/l in males) (Multidisciplinary Expert Task Force on Hyperuricemia and Related Diseases, 2017), is not only a leading cause of gout but is also related to other diseases such as obesity, hypertension, stroke, chronic kidney disease, and even heart disease (Bonino et al., 2020; Brucato et al., 2020; Feig et al., 2008; Zhu et al., 2011). The prevalence of HUA varies worldwide, ranging from 12.0% to 25.8% (Liu et al., 2015; Trifiro et al., 2013; Uaratanawong et al., 2011; Zhu et al., 2011), owing to many differences in the environment, lifestyle, and underlying genetic factors.
A nationwide survey in China showed that the overall prevalence rate of HUA in adults was 13.0%, of which 8.0% and 18.5% were among females and males, respectively (Wu et al., 2017). Particularly, in local Tibetan Plateau inhabitants, the incidence of HUA ranges from 29.1% to 45.6% (Chen et al., 2011). When people migrate from low altitude to high altitude, their SUA levels significantly increase because of high-altitude hypoxemia (Peng et al., 2018).
More than 400,000 immigrants live at a high altitude in Tibet, of them mainly are Han ethnic (Statistics, 2021). Unlike with local Tibetan Plateau populations, immigrants should adjust their bodies to compensate for the anoxia induced by changes in the environment (Pei et al., 2012). Chronic exposure to high-altitude hypoxemia causes increased generation of RBC as well as rising SUA levels, which directly result in HAPC and HUA at the same time (Qiu et al., 2013; Wang et al., 2022). Many immigrants suffer from various types of CMS, including HAPC, HUA, and other serious secondary diseases (Pei et al., 2012).
The mechanism of high-altitude HUA is different from that in low altitude, which is closely correlated with high-altitude hypoxemia, lactic acid accumulation resulting from hypoxemia, and HAPC (Gonzales and Tapia, 2013; Li et al., 2018; Siques et al., 2009). Therefore, the risk factors for high-altitude HUA in immigrants are not the same as those in other populations. However, few studies have investigated the incidence and risk factors of HAPC and HUA in high-altitude immigrants. Therefore, it is important to carry out research on the prevalence and risk factors of HAPC and HUA to deeply understand the high-altitude acclimatization of immigrants.
Previous epidemiological studies on CMS have mainly focused on the general population at high altitude (Gao et al., 2021; Shen et al., 2019; Shen et al., 2017; Zhang et al., 2018), while studies on the epidemiology of CMS in immigrants have been limited. As differences in CMS exist among different ethnic subgroups (Supplementary Material S1), this study aimed to estimate the current levels of Hb and SUA and the prevalence of HAPC and HUA among immigrants at high altitudes to fill the void. In addition, this study investigated several risk factors to deeply understand the mechanism of HUA in immigrants.
Methods
Study design and subjects
A cross-sectional survey using cluster sampling was conducted between January 2019 and December 2021 to obtain a representative sample of immigrants. All participants underwent routine physical examinations at the 954th Army Hospital in Shannan, Tibet Autonomous Region, between January and December 2021. Shannan is located in the southern part of the Tibetan Plateau at an average altitude of 3,650 m above sea level. Participants were 15–45 years of age, who had been living for at least 2 years in Shannan, and the altitude distribution of the living environment of participants ranged from 3,600 to 3,700 m.
According to medical records or self-reported diagnoses, pregnant females, and patients with mental health diseases, malignant tumors, and/or severe hepatic, heart, or renal failure were excluded from the study. Data on age, sex, complete blood count (CBC), and SUA levels were obtained. A total of 7,070 immigrants were selected from healthy subjects and invited to participate in this survey, including 6,000 male and 1,070 female participants. Male and female participants were divided into six age groups, including 15–20, 21–25, 26–30, 31–35, 36–40, and 41–45 years, respectively.
All subjects gave informed consent for inclusion before their participation in the study. The study was conducted according to the Declaration of Helsinki, and the project was approved by the Ethics Committee of General Hospital of Tibet Military Region.
Laboratory measurements and definitions
After overnight fasting for at least 6 hours, venous blood samples were collected. CBC was tested using an XE-2100 automated hematology analyzer (SYSMEX, Kobe, Japan) using whole blood samples. SUA levels in serum samples were evaluated using a TBA-40 biochemical analyzer (TOSHIBA, Tokyo, Japan). HAPC was defined as Hb ≥165.0 g/l in females and ≥185.0 g/l in males (Wadleigh and Tefferi, 2010). HUA was defined as SUA levels ≥360.0 μmol/l in females and ≥420.0 μmol/l in males (Multidisciplinary Expert Task Force on Hyperuricemia and Related Diseases, 2017).
Statistical analysis
Continuous variables are presented as mean ± standard deviation and categorical variables are presented as cases (n) and percentages (%). Between-group differences were analyzed using Student's t-test for normally distributed variables. χ2-test and Fisher's exact test were used for categorical data. The mean levels of RBC, Hb, and SUA and the prevalence of HAPC and HUA were estimated for all subjects and for different age subgroups. Binary logistic regression analysis was performed to determine risk factors for HUA level among parameters performing significance in correlation analysis. The associations were quantified by odds ratios (ORs) and 95% confidence intervals (CIs). Data were analyzed with SPSS software, version 26.0 (IBM, Armonk, NY), and p-value <0.05 was identified as statistical significance.
Results
Baseline characteristics
The baseline features are presented in Table 1, including age, RBC count, Hb, SUA, and prevalence of HAPC and HUA. Totally, 7,070 participants were included in this study, comprising 6,000 (84.9%) males and 1,070 (15.1%) females. Significant differences were observed in RBC count, Hb, and SUA between males and females (p < 0.0001). Besides, prevalence of HAPC and HUA in males was much higher than in females (p < 0.0001).
Characteristics of Study Participants
Data are presented as either percentage (%) or mean ± SD. The p values compare the male group (n = 6,000) with the female group (n = 1,070) using either the Student's t-test or the chi-square test, as appropriate.
HAPC, high-altitude polycythemia; Hb, hemoglobin; HUA, hyperuricemia; RBC, red blood cell; SD, standard deviation; SUA, serum uric acid.
Hb and SUA distribution
The distributions of Hb and SUA with age are shown in Figure 1. For males, Hb reached its highest level between the age of 26 and 30 years, showing a significant difference (p < 0.05) compared to other age groups (Fig. 1a). For females, Hb reached its highest level between the age of 36 and 40 years, and also showed a significant difference compared with the 15–20 (p = 0.0007) age group (Fig. 1b). SUA in males reached the highest level between the age of 31 and 35 years, showing significant differences compared to other age groups (Fig. 1c). Moreover, SUA of females reached its highest level between the age of 21 and 25 years, showing significant differences compared to other age groups (Fig. 1d). The incidence of HUA between people with HAPC and non-HAPC showed a significant difference except for females (Supplementary Material S2).
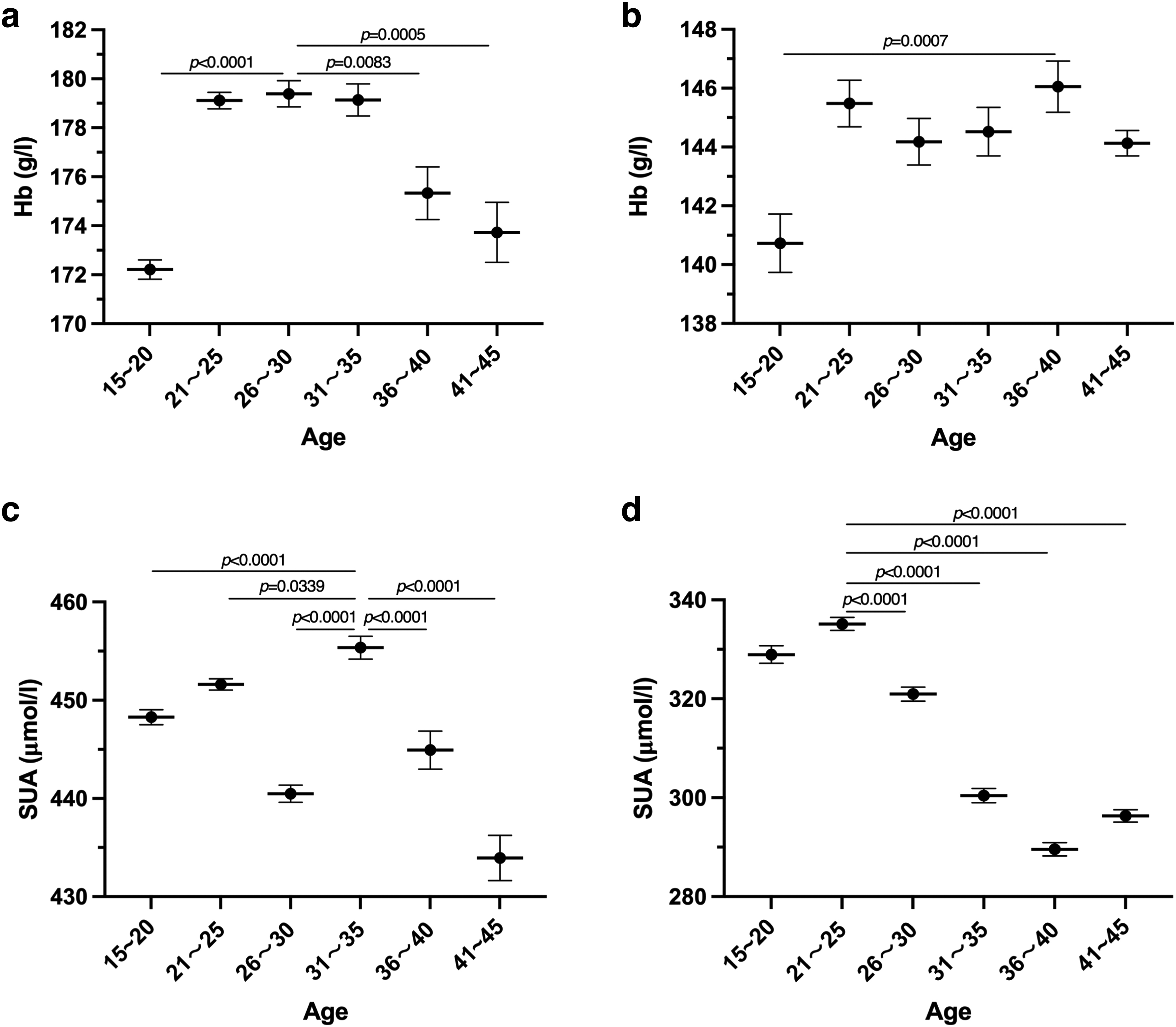
Hb and SUA distributions with age. The p values compare the different age groups using the Student's t-test.
Frequency of HAPC and HUA with age
The Hb levels in different age groups and the corresponding prevalence of HAPC are presented in Table 2. For males, Hb levels (F = 40.3, p < 0.0001) and the prevalence of HAPC (χ2 = 128.30, p < 0.0001) between different age groups showed significant differences, respectively. Besides, the age group of 26–30 with the highest prevalence of HAPC also had the highest Hb level. For females, Hb level between different age groups showed significant difference (F = 3.9, p = 0.0016), but the prevalence of HAPC of females among age groups showed no significant difference (χ2 = 1.3, p = 0.9404).
Hemoglobin Level and Prevalence of High-Altitude Polycythemia
Data are presented as either percentage (%) or mean ± SD. The p values compare the different age groups in males and females using either the one-way ANOVA or the chi-square test, as appropriate.
p < 0.05, contrasting to 26–30 years in males.
p < 0.05, contrasting to 36–40 years in females.
SUA levels in different age groups and HUA prevalence are shown in Table 3. For males, SUA level (F = 40.3, p < 0.0001) and the prevalence of HUA (χ2 = 17.1, p = 0.0043) between different age groups showed significant differences, respectively. For females, SUA level (F = 110.8, p < 0.0001) and the prevalence of HUA (χ2 = 24.0, p = 0.0002) between different age groups also showed significant difference, respectively. Meanwhile, the age group of 21–25 years with the highest prevalence of HUA also showed the highest SUA as well as Hb.
Serum Uric Acid Level and Prevalence of Hyperuricemia
Data are presented as either percentage (%) or mean ± SD. The p values compare the different age groups in males and females using either the one-way ANOVA or the chi-square test, as appropriate.
p < 0.05, contrasting to 31–35 years in males.
p < 0.05, contrasting to 21–25 years in females.
Risk factors for HUA
Age, sex, and Hb were selected to evaluate risk factors for HUA using binary logistic regression analysis. As shown in Table 4, age (B = −0.012, OR 0.988, CI 0.982–0.995), sex (B = 0.655, OR 0.514, CI 0.421–0.628, male as positive predictor), and Hb (B = 0.027, OR 1.028, CI 1.025–1.031) significantly affected the prevalence of HUA. Among the risk factors, age played a negative role in the HUA detection rate, whereas sex and RBC count positively affected the prevalence of HUA. Besides, univariate linear regression analysis showed that SUA had a linear relation with HUA (Supplementary Material S3).
Risk Factors Associated with Hyperuricemia
Binary logistic analysis of risk factors for HUA: B value and OR (95% CI) value represent the OR value of the corresponding variable and its 95% CI.
CI, confidence interval; OR, odds ratio.
Discussion
Tibet is a vast land with a hypobaric hypoxia environment, in which CMS is a common, but serious disease among high-altitude residents, causing severe damage to their health (Leon-Velarde et al., 2005). A large number of immigrants live in Tibet, and the number of immigrants from low altitude has increased constantly every year (Wu and Kayser, 2006). Genetic differences in high-altitude adaptation exist between immigrants and Tibetans, as has been proven in previous studies (Li et al., 2018). Immigrants are more susceptible to CMS than Tibetans, and much greater harm is caused to this population by CMS, such as HAPC and HUA. Thus, in this study, we investigated the prevalence of HAPC and HUA and evaluated several risk factors for HUA.
Both RBC count and Hb of males were much higher than females, which were in accordance with the previous study of Bai individuals (5.6 ± 0.5 × 1012/l and 173.6 ± 13.2 g/l in males and 4.9 ± 0.4 × 1012/l and 146.0 ± 13.6 g/l in females) at an altitude of 2,300 m (Gao et al., 2021). This study found that the prevalence of HAPC among immigrants was higher than that reported in a previous study of populations (5%–18%) (Luks et al., 2017). This difference was reasonable considering that the genetic factors and population characteristics of immigrants in this study were different from those in the previous study. Therefore, HAPC is a common CMS among immigrants, which cannot be neglected, and further studies on its mechanism and damage should be carried out.
In this study, overall SUA level was reported to be much higher than clinical diagnosis standard of HUA, especially in males. A cross-sectional study in Western China reported that the mean SUA level of employees was 357.9 μmol/l (382.5 and 294.4 μmol/l in males and females, respectively) (Shen et al., 2019), which was lower than results in this study. It is well known that HUA is a common disease, but the prevalence of HUA varies by region in China (Wu et al., 2017).
This study found that the prevalence of HUA in immigrants was much higher than 8.4%–13.3% reported by previous studies for the general Chinese population (Liu et al., 2015; Liu et al., 2014). The prevalence of HUA in employees working in Qinghai Tibet Plateau was reported to be 27.9% (Shen et al., 2019), and another cross-sectional study reported an HUA prevalence of 21.0% in the Yi ethnic group (Liu et al., 2018), and a study aiming to Tibetan herdsmen/farmers reported an HUA prevalence as low as 2.1% (Zhang et al., 2020). The HUA prevalence previously reported is much lower than results in this study, indicating that immigrants are more vulnerable to HUA in the process of adaptation to high altitude.
In this study, the highest prevalence of HAPC in males and females occurred in those 26–30 and 21–25 years of age, respectively, and of HUA in both males and females occurred in those 21–25 years of age. The trend of HUA prevalence in males was not correlated with HAPC, but that in females was correlated with HAPC, which was consistent with the findings of previous studies (Cheserek et al., 2018; Wu et al., 2017). In a previous study, the prevalence of HUA in males decreased with age, whereas it increased in females with age (Shen et al., 2019).
However, in our study, this trend of HUA was not significant in males or females, indicating that HUA of immigrants was not only simply influenced by sex or age but also by many other factors. This hypothesis is consistent with a previous study that found kidney damage and decreased SUA excretion induced by chronic exposure to high-altitude environments may cause HUA (Jefferson et al., 2002).
The risk factors for HUA were estimated using binary logistic regression analysis, which showed that age, sex, and Hb significantly affected the prevalence of HUA. Overall, age had a negative correlation with HUA, which may be due to the fuller adaptation to high altitude resulting from the longer exposure time of the elderly. Similar to previous studies (Liu et al., 2013; Qiu et al., 2013), males were observed to be much more susceptible to HUA than females in this study.
Hb was observed to be a risk factor for HUA, and we wondered whether HAPC was an indicator of HUA. Thus, participants were divided into two groups based on whether they had HAPC or not, and the prevalence of HUA was evaluated. A significant difference was observed in males, and the prevalence of HUA was much higher in participants with HAPC than in those without HAPC. Therefore, HAPC played an important role in the detection rate of HUA, which was similar to that observed in the Bai ethnic group (Wu et al., 2017).
HAPC leads to various damages to the microcirculatory and immune system, such as sleep disorders, vascular thrombosis, and even extensive organ damage (Guan et al., 2015; Jiang et al., 2012). HUA also causes serious damage to many organs, such as the heart and kidneys. CMS seriously threatens the health of immigrants, but few studies have focused on this special population. Thus, this study first evaluated the prevalence of HAPC and HUA in immigrants to help improve their health status.
This study had several limitations. First, as a retrospective study, altitude was not included in the study; however, altitude was considered a risk factor for CMS. Altitude was controlled at the same level for all participants. Second, this study was based on data from a single center of Tibetan immigrants in China. A multicenter study on the numbers of immigrants living in other high-altitude regions worldwide is needed to confirm our results. Third, this study lacks an intensive exploration of pathogenetic mechanisms of HAPC and HUA in immigrants. We will conduct multicenter sample studies and increase the evaluation factors of the study in future studies. The pathogenesis of CMS in immigrants requires further study.
In summary, CMS, especially HUA, is a prevalent disease among immigrants. In the process of adaptation to high-altitude environments, immigrants are more susceptible to HAPC and HUA, especially males. The prevalence of HUA was influenced by age, sex, and Hb, and the detection rate of HUA was also affected by HAPC. The findings of this study may help design further studies on the adaptation of immigrants and improve health care strategies in this population. However, multicenter studies are required to comprehensively explore the pathogenetic mechanisms.
Footnotes
Acknowledgments
We thank the medical staff at the 954th Army Hospital for their support with this study.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article.
Ethical Compliance
All participants were given informed consent for inclusion before they participated in the study. All procedures performed in this study involving human participants were in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study protocol was approved by the Ethics Committee of the General Hospital of the Tibetan Military Region (20220317).
Authors' Contributions
Study conception and design (Z.S. and H.Z.); data acquisition (A.Z., J.L., G.X., R.Z., Y.L., and H.X.); data analysis (Z.S. and A.Z.); article drafting (Z.S.); article critical revision (Z.S., A.Z., H.P., W.Z., Z.L., and H.Z.), and final article approval (Z.S., A.Z., J.L., G.X., H.P., R.Z., Y.L., H.X., W.Z., Z.L., and H.Z.).
Author Disclosure Statement
The authors declare that they have no affiliation with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this article.
Funding Information
This study was supported by a project of the Institute of Radiation Medicine, Academy of Military Medicine, Chinese PLA Academy of Military Sciences (Science and Technology Commission of the CMC National Defense Innovation Special Zone: 18-163-15-ZT-001-007-22).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.