
Abstract
van Veelen, Michiel J., Giulia Roveri, Ivo B. Regli, Tomas Dal Cappello, Anna Vögele, Michela Masè, Marika Falla, and Giacomo Strapazzon. Personal protective equipment protocols lead to a delayed initiation of patient assessment in mountain rescue operations. High Alt Med Biol. 24:127–131, 2023.
Introduction:
Mountain rescue operations can be challenging in austere environmental conditions and remote settings. Airborne infection prevention measures include donning of personal protective equipment (PPE), potentially delaying the approach to a patient. We aimed to investigate the time delay caused by these prevention measures.
Methods:
This randomized crossover trial consisted of 24 rescue simulation trials intended to be as realistic as possible, performed by mountain rescue teams in difficult terrain. We analyzed the time needed to perform an airborne infection prevention protocol during the approach to a patient. Time delays in scenarios involving patients already wearing versus not wearing face masks and gloves were compared using a linear mixed model
Results:
The airborne infection prevention measures (i.e., screening questionnaire, hand antisepsis, and donning of PPE) resulted in a time delay of 98 ± 48 (26–214) seconds on initiation of patient assessment. There was a trend to a shorter time to perform infection prevention measures if the simulated patient was already wearing PPE consisting of face mask and gloves (p = 0.052).
Conclusion:
Airborne infection prevention measures may delay initiation of patient assessment in mountain rescue operations and could impair clinical outcomes in time-sensitive conditions.
Trial registration number 0105095-BZ Ethics Committee review board of Bolzano.
Introduction
Accidents in wilderness areas, such as national parks, create challenges for rescuers not found in urban areas. Weather conditions, altitude, challenging terrain, limited rescue personnel availability, and transport options may delay medical response and patient evacuation (Sumann et al., 2020). Despite these challenges, the goal remains to provide the best care as rapidly as possible. Rescue operations in wilderness environments can involve prolonged close interactions between rescuers and patients, necessitating measures to protect rescuers from airborne viruses such as COVID-19 (Massullo et al., 2021).
The Italian mountain rescue service, Corpo Nazionale Soccorso Alpino e Speleologico (CNSAS), has developed an internal airborne infection prevention protocol for patient care during the COVID-19 pandemic, consisting of a verbal risk assessment and the appropriate sequence of donning and doffing of personal protective equipment (PPE), such as a face mask, protective eyewear, gloves, and an optional protective suit (Massullo et al. 2021; Ortega et al., 2020).
Recently, the International Commission for Alpine Rescue has published more extensive infection prevention recommendations (Roy et al., 2021). Adherence to infection prevention protocols may lead to a time delay, which could be crucial for severely injured or ill patients in a hostile mountain environment when the outcome is time dependent (Rauch et al., 2018).
The actual time needed for completing the entire sequence of airborne infection prevention measures in the field has scarcely been investigated. The primary aim of this trial was to investigate the time delay associated with the protocol application during simulated mountain rescue operations in the field. The secondary aim was to determine whether there was a reduced delay if the patient was already wearing face mask and gloves at the time of rescue team arrival.
Materials and Methods
The study was designed as a randomized crossover trial involving simulation scenarios. The ethics committee review board of Bolzano, Italy, approved the study (protocol no. 0105095-BZ). The study was conducted under the principles of the Declaration of Helsinki.
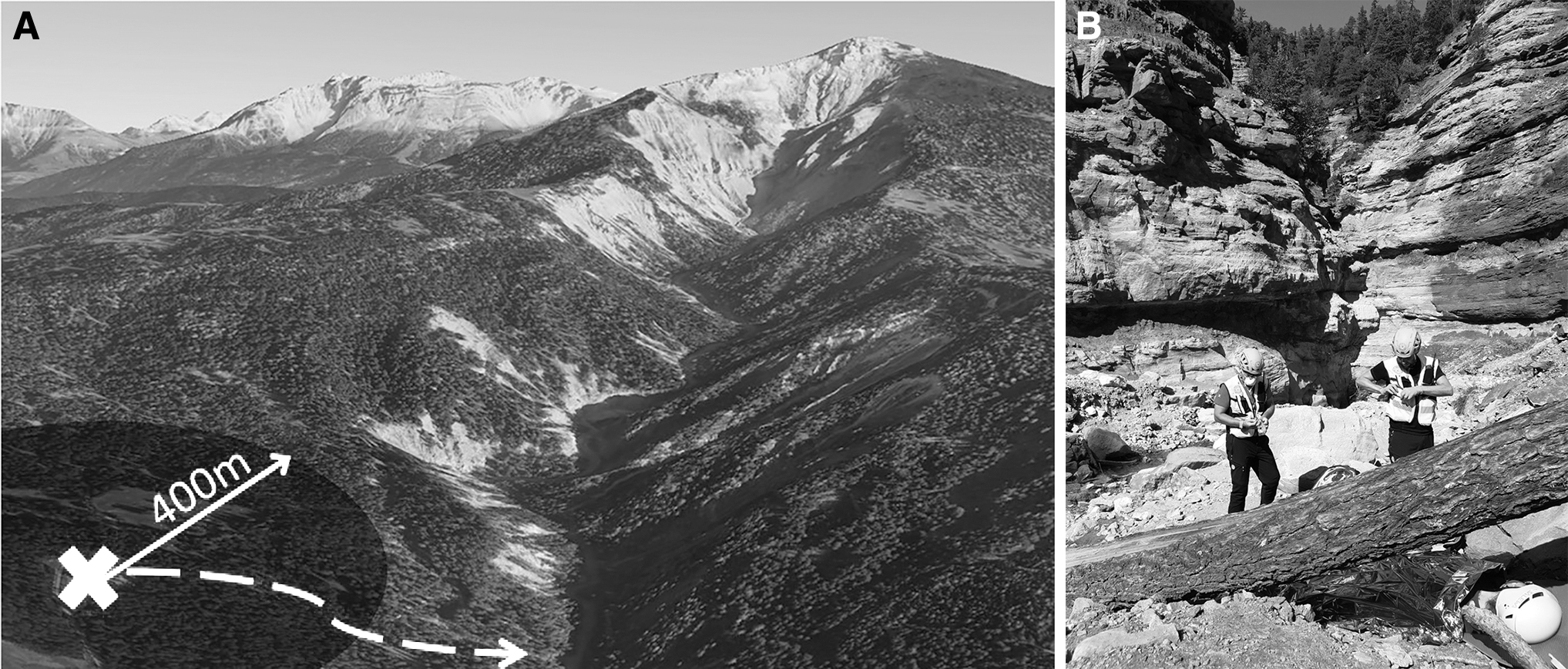
Twenty-four members of the Italian mountain rescue service CNSAS were included in the study. Age younger than 18 years old was an exclusion criterion. Rescuers were excluded if they had COVID-19 symptoms, a positive test for SARS-CoV2, or unprotected contact with COVID-19 patients in the previous 4 weeks. Written informed consent for the study was obtained. Study participants were divided into six teams. Every team consisted of one team leader and three rescuers. Study investigators simulated the patient. We simulated 24 search and rescue trials in the gorge of the GEOPARC Bletterbach, Italy (Fig. 1).
Before reaching the patient, each mission included a search phase on foot in the designated area with a distance covered of ∼2–4 km in rough terrain, including descending and scrambling on the canyon floor, which required a high physical effort for ∼15–20 minutes, depending on the exact location of the scenario. Scenarios were standardized and consisted of patients with minor injuries. During the simulated approach, the rescuers followed the CNSAS protocol and completed the preventive measures to avoid the transmission of infection (Fig. 2). The participants were trained in the protocol and accustomed to use it in daily practice.

Approach protocol of the Italian mountain rescue service during the COVID-19 pandemic (modified from Masullo et al., 2021).
The sequence of measures included (1) verbal screening questionnaire to stratify the patient as low or high risk; (2) use of hand sanitizer; (3) donning of adequate PPE, including filtering facepiece 2 mask (similar to an N95 respirator) and a pair of disposable gloves for both rescuer and patient. Rescuers did not use a protective suit. All patients were instructed to answer positively to one of the screening questions. The rescuers could decide when to initiate the infection prevention protocol (e.g., unpacking masks and gloves before contact with the patient), but the donning took place at the side of the patient.
The team requested that the simulated patient wears a mask and gloves, if the patient was not already wearing them. Time was taken by an observer using a stopwatch. After these measures, the team performed a standardized medical procedure consisting of an extremity splinting procedure and the application of a rescue foil. Each team performed four simulated trials: two trials in which the patient was already wearing a mask and gloves at the arrival of the rescue team, and two trials in which the patient was not wearing any PPE at the arrival of the rescue team. The teams conducted the trials in random order.
We analyzed the time needed to perform the infection prevention measures and the delay to initiate assessment. We used a linear mixed model (LMM) to evaluate the effect of patients already wearing PPE on infection prevention measures time. We inserted the consecutive mission number of each team in the LMM to consider a training effect. We chose the LMM to take the four repeated measures of each rescue team into account and to insert the team as a random effect. We used SPSS version 27 (IBM Corp., Armonk, NY). We considered p < 0.05 (two-sided) statistically significant. Values are reported as mean ± standard deviation (range).
Results
Twenty-four search and rescue trials were completed and included in the analysis. The overall time needed by the teams to perform the sequence of airborne infection preventive measures (i.e., screening questionnaire, hand antisepsis, and donning PPE) was 98 ± 48 (26–214) seconds (Table 1). After the ground team arrived at the patient, the time needed to perform the standard medical procedure in the scenario was 302 ± 100 (119–505) seconds.
Time Needed to Perform the Sequence of Preventive Measures to Avoid the Transmission of Airborne Infections
Twelve trials were conducted with the simulated patient already wearing face mask and gloves on the arrival of the rescue team, and 12 trials were conducted with the patient not wearing face mask and gloves on the arrival of the rescue team.
PPE, personal protective equipment; SD, standard deviation.
The time needed to perform infection prevention measures for a simulated patient who was not already wearing mask and gloves at the arrival of the rescue team was longer than the time it took for a patient already wearing mask and gloves [117 ± 55 (44–214) seconds vs. 79 ± 32 (26–115) seconds]. This was not statistically significant (p = 0.052). No training effect on the time to perform the infection prevention protocol was detected (p = 0.416).
Discussion
The time needed to perform the airborne infection prevention measures led to a delay in initiation of treatment. This delay in treatment initiation may be of limited clinical relevance in a patient with a minor injury or in a long search and rescue operation. However, such a delay may have a significant clinical impact in critically injured or ill patients, such as cardiac arrest or trauma patients with massive hemorrhage or impaired airway.
Local and international COVID-19 prevention guidelines provided recommendations for rescuers approaching a patient (Massullo et al., 2021; Roy et al., 2021). The actual time needed for completing the entire sequence of airborne infection prevention measures in the field has been scarcely investigated. The delays we found are consistent with a previously conducted in-hospital study on the time taken by health care personnel for donning PPE without administering a screening questionnaire before initiating a simulated tourniquet application, where the delay was 84 seconds (Kragh et al., 2020). Patients did not put on any PPE in the study.
A retrospective cohort study comparing prehospital response times of emergency medical services found no statistical difference in the overall response time for trauma patients, but actual time required for donning PPE was not recorded (Jarvis et al., 2021). Other studies including populations with acute medical conditions found increased on-scene times (Eskol et al., 2022). In addition to causing a time delay, wearing PPE might impair the quality of care by limiting freedom of movement in difficult terrain, compromising thermal regulation, especially during exertion, and impairing the quality of communication (van Veelen et al., 2021).
Wearing PPE in extreme environmental conditions involving heavy precipitation, strong winds, or crossing open water or snow during technical operations might limit the ability of rescuers to operate effectively and the effectiveness of the PPE itself (van Veelen et al., 2021).
A patient already wearing a face mask and gloves can be approached more rapidly, thus reducing the time needed for the assessment and initiation of the treatment. Because of local regulations requiring people to wear face masks, even outdoors, at some times during the COVID-19 pandemic, people may have had masks. It was less likely they would have had gloves (Badillo-Goicoechea et al., 2021). Patients and bystanders can be advised by telephone to wear masks and gloves, if they have them, as the rescuers are approaching. PPE might also be delivered by drones as part of a medical kit (van Veelen et al., 2020).
The limited amount of time saved would be clinically important only in a few cases requiring time-dependent critical care. Lack of protection has been described as a barrier to bystander care, including cardiopulmonary resuscitation (Scquizzato et al., 2020). Early availability of masks and gloves with instructions about how to don them might help persuade bystanders to assist. Another option to reduce the time delay could be to eliminate the screening for infectious diseases history from the procedure and consider all patients as potentially at high risk and apply universal precautions.
Risk stratification could be done later during transport to the hospital. In this trial, patients were routinely instructed to put on gloves. This is not a high-yield intervention given that COVID-19 is mainly spread by airborne transmission (Lewis, 2020), but it did add time to the rescue.
Although rescuer safety should be the main consideration, the potential benefits of decreasing the time delay caused by PPE application should be weighed against the estimated risk of infection (Hsu et al., 2021). This risk is dynamic and would depend on local infectious disease (variant) incidence and morbidity, advancing insight into transmission routes, and acquired immunity through vaccination or past infection prevalence, and its perceived effectiveness at different outbreak stages (Hsu et al., 2021; van Veelen et al., 2021).
This balanced decision could be influenced by the possible perspective of a future transition to an endemic state of a (novel) infectious disease, such as COVID-19. To increase the effectiveness of donning PPE, education and training in the protocols should occur under realistic conditions.
Limitations
There were only 24 trials. Results in the scenarios might differ from those in real rescues. None of the patients in the scenarios would have required time-critical intervention. The protocol of the Italian mountain rescue service was the only protocol used. There was no control group of rescuers not using PPE. The proportion of time taken to perform the questionnaire versus the actual donning was not recorded.
Conclusions
Measures to prevent transmission of airborne viruses may delay the assessment of patients in mountain rescue operations, potentially worsening clinical outcomes of patients with time-critical conditions. Delays in assessment are unlikely to be detrimental in the vast majority of mountain rescue missions not involving patients with critical conditions and long-duration operations. Use of universal precautions without prehospital risk stratification would likely be safe while limiting the time needed for the assessment.
Footnotes
Acknowledgments
We thank Tamara Herbst and all other members of the Italian mountain rescue service CNSAS who participated in this trial. We thank Christian Weber and his colleagues of the GEOPARC Bletterbach for their hospitality and support.
Authors' Contributions
Conception of the study was by G.S. Contribution to the design of the trial, data collection and/or analysis, and drafting the article, including critical revision for important intellectual content, and approving the final version to be published were carried out by all authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The research leading to these results has received funding from the European Regional Development Fund under the Cooperation Programme Interreg V-A Italia Austria 2014-2020, ITAT3023, Smart Test for Alpine Rescue Technology (START). The project consisted of seven partners from Italy and Austria and ran from 2017 to 2021.