
Abstract
Kammerer, Tobias, Anna Walzl, Thomas Müller, Philipp Groene, Giulia Roveri, Rachel Turner, Johanna Roche, Hannes Gatterer, Christoph Siebenmann, and Simon T. Schäfer. Effects of hypobaric hypoxia on coagulation in healthy subjects exposed to 3,500 m altitude. High Alt Med Biol. 24:94–103, 2023.
Background:
Hypoxia is discussed as a trigger for prothrombotic changes both in intensive care and high altitude medicine. This research study aimed to evaluate the effect of isolated hypobaric hypoxia (HH) on coagulation in females in a highly standardized setting.
Methods:
Twelve healthy female subjects were studied under HH (equivalent to 3,500 m) and normoxia (NX) during two 4-day sojourns, in a strictly controlled crossover design. Nutrition, fluid intake, hormonal status (i.e., menstrual cycle variation), and physical stress were standardized. Functional coagulation and blood lysis were measured by viscoelastometry and compared between HH and NX. In addition, plasma-based coagulation tests (PBCTs), namely prothrombin time, activated partial thromboplastin time, fibrinogen, factor VIII coagulation activity (FVIII:C), von Willebrand factor antigen (vWF:Ag), and von Willebrand factor ristocetin cofactor activity (vWF:RCo) were measured.
Results:
Neither for Viscoelastic Haemostatic Assays nor for PBCTs significant changes were found for HH compared with NX (all p > 0.05). Specifically, the lysis ability, as well as clotting time, clot formation, clot amplitude, and maximum clot firmness unchanged were similar between HH and NX. This also applied to all other variables.
Conclusion:
We demonstrate that moderate HH per se has no influence on blood coagulation in healthy females.
Introduction
Hypoxia is considered as a possible trigger for prothrombotic changes in blood coagulation in mountaineers or on long-haul flights (Brill et al., 2013; Damodar et al., 2018; Jha et al., 2018; Ninivaggi et al., 2015; Rosendaal, 2002; Treml et al., 2022; Trunk et al., 2019; Wu et al., 2022). Two possible mechanisms could be responsible for prothrombotic changes under hypobaric hypoxia (HH): enhanced and temporally accelerated clot formation or inhibited fibrinolytic capacity. Although an increase in clot strength was indeed reported in hypobaric conditions (Rocke et al., 2018), only a few studies focused on fibrinolytic variables.
A recent study was the first to show that fibrinolytic capacity is lower in long-term high altitude residents in Tibet than in low altitude residents (Jiang et al., 2021). Furthermore, it is unclear whether procoagulatory changes in previous studies were a consequence of HH alone, or of other risk factors, such as venostasis, physical stress, environmental conditions, fluid balance, or hormone status, including menstrual cycle variations in women. This is not least due to the fact that confounders in field studies on mountaineers and air travelers cannot be adequately excluded due to the inadequate standardization.
All these factors could be an explanation for the sometimes controversial results of different studies (Bärtsch, 2006; Brill et al., 2013; Martin et al., 2012; Toff et al., 2006; Venemans-Jellema et al., 2014). To examine the isolated influence of hypoxia on blood coagulation, in vitro studies are, therefore, often carried out, but these can only be transferred to the in vivo situation to a limited extent. A better solution is to conduct studies in a hypoxic chamber, where environmental conditions and influencing factors can be standardized (Schaber et al., 2015).
The aim of this study was thus to use a hypobaric chamber to investigate the influence of HH (equivalent to 3,500 m) on coagulation, by performing Viscoelastic Haemostatic Assays (VHAs) and plasma-based coagulation tests (PBCTs). For this purpose, we have studied healthy women both under normoxia (NX) and HH in a highly standardized crossover setting controlling for major confounding factors, including menstrual cycle variation to test the hypothesis that HH has a procoagulatory influence on coagulation, either by increased clot formation or by inhibited fibrinolytic capacity.
Methods
The study was approved by the ethics committee of the Bolzano Hospital, Italy (No. 70-2019) and conducted in agreement with the Declaration of Helsinki.
Subjects
Twelve healthy female lowlanders gave written informed consent and participated in this experimental study (see Table 1). All participants lived close to sea level and had no history of acute mountain sickness (AMS) or high-altitude illness. Inclusion criteria were age between 20 and 30 years, body mass index between 20 and 25 kg/m2, and the use of either a combined oral third-generation estroprogestative contraceptive (n = 11) or intrauterin progestative contraception (n = 1) (see Table 1). Taking other medications, alcohol and nicotine abuse, high altitude ancestry, and regular endurance training were exclusion criteria. In addition, the subjects were not allowed to stay above 2,000 m from 4 weeks before and during the study. Since the study was conducted during the SARS-CoV-2 pandemic, all subjects were vaccinated/recovered, had documented antibodies, and were tested before (PCR) and after (rapid test) the chamber exposures.
Volunteers Characteristics
MW, molecular weight; SD, standard deviation.
Study protocol
The sojourns were carried out in a climate chamber (terraXcube; Eurac Research, Bolzano, Italy, 263 m), where the same environmental conditions were simulated under NX and HH.
The room temperature was kept constant at 22°C, with an average humidity of 30%. Under HH, the chamber was decompressed to a pressure of 657.7 mbar (493.5 mmHg), which corresponds to an altitude of 3,500 m.
The data described in this study were collected as part of a crossover controlled prospective study focused on plasma volume regulation (Roche et al., 2022). Subjects spent two 4-day sojourns in the chamber, one in NX and one in HH. For both sojourns, subjects entered the chamber at 6:00 in the morning and left the chamber in the morning of day 5. One group (N = 6) started under NX; after a 4-week break, the same group spent 4 nights under HH. The other group (N = 6) started under HH conditions and then completed the NX sojourn; also with a 4-week break in between. Group allocation was based on the contraception schedule of the subjects so that participation occurred during the active phase of pill consumption, and in the absence of menstruation for the progestin user.
Four days before and throughout the sojourns, the participants ate a standardized diet (1,900 kcal/day) consisting of three main meals and three snacks per day. This included a standard fluid intake of 2,000 ml divided into six portions. Each day of the sojourns the subjects reproduced their habitual step count (as evaluated by a pedometer throughout the three days preceding the first sojourn) by walking on a treadmill. No other endurance type exercise was allowed, but subjects were permitted light strength training and stretching. Symptoms of AMS were evaluated on the first evening at 19:00 and M2–M5 using the self-reported Lake Louise Score (LLS) (Roach et al., 1993). The complete details of the study protocol and environmental conditions were published previously (Roche et al., 2022).
Viscoelastic Haemostatic Assays
Functional coagulation analyzes were performed with a viscoelastometry system (ClotPro®; enicor GmbH, Munich, Germany). This system allows the assessment of clot activity, clot strength, and the fibrinolysis process. The results of this viscoelastometric system are comparable with rotational thromboelastometry (ROTEM®; TEM Innovations GmbH, Munich, Germany) and thromboelastography (TEG®; Haemonetics Corporation, Braintree, MA, USA) (Yoshii et al., 2022).
Venous blood was collected in the fasting state at 7.00 am on day 2 (M2) and day 4 (M4). Subsequently, different reagents were added to the blood by pipetting to activate the coagulation process. This simple handling of the reagents is known as “active tip technology.” In this study, the corresponding reagent is present in a sponge in the pipette tip and only dissolves through direct contact with whole blood.
We analyzed hemostasis using the IN, EX, FIB, and TPA tests. The IN or EX test gives an overview of the intrinsic or extrinsic pathway of blood coagulation (Calatzis et al., 2018). The samples are recalcified with calcium chloride, then the coagulation is activated with recombinant tissue factor in the EX test or ellagic acid in the IN test. For the examination of the fibrinogen level and fibrin polymerization by the FIB test, whole blood is again recalcified with calcium chloride and the extrinsic coagulation pathway is activated by tissue factor. Platelet activity and aggregation are inhibited with cytochalasin D and a GP2b3a antagonist. The TPA test allows the analysis of the fibrinolysis process induced with recombinant tissue plasminogen activator (Calatzis et al., 2018). The following components are included in the TPA test: tissue factor and t-PA as activators (650 ng/ml), polybrene as inhibitors and CaCl2 for recalcification.
Plasma-based coagulation tests
Venous blood sampling for analysis of PBCTs took place at 7.00 am on day 1 (M1) and day 5 (M5), also in the fasted state. Determination of prothrombin time (PT) was carried out with a high-sensitivity thromboplastin reagent based on recombinant human tissue factor (HemosIL® RecombiPlasTin 2G; Werfen, Munich Germany). For determination of activated partial thromboplastin time (aPTT) a synthetic phospholipid reagent (HemosIL® SynthASil; Werfen, Munich, Germany) was used. Determination of fibrinogen based on the Clauss method (HemosIL® Q.F.A. Thrombin (Bovine); Werfen, Munich, Germany).
Determination of factor VIII coagulation activity (FVIII:C) was done with a chromogenic method (FVIII:C chromogenic; COAMATIC® Factor VIII, Chromogeneix, Munich, Germany) and clotting method (FVIII:C clotting) using a one-stage aPTT-based clotting assay with FVIII-deficient plasma (HemosIL® SynthASil; Werfen). Determination of von Willebrand factor antigen (vWF:Ag) and von Willebrand factor ristocetin cofactor activity (vWF:RCo) were performed with latex enhanced immunoassays (HemosIL®, von Willebrand Factor Antigen, and HemosIL® von Willebrand Factor Ristocetin Cofactor Activity, respectively, Werfen, Munich, Germany).
Statistical analysis
The statistical analysis was carried out using GraphPad Prism 9.1.2 (GraphPad Software, San Diego, USA). The raw data were checked for normal distribution using the D'Agostino & Pearson test. Normally distributed data with repeated measures were analyzed using one-factor ANOVA with Greenhouse–Geisser correction and post hoc Bonferroni correction (p = 0.05/n) for adjustment of multiple testing. Non-normally distributed data were analyzed using Friedman test with Dunn's correction for adjustment of multiple testing. The statistical significance level was set at p < 0.05 and data are reported as means ± SD and median with interquartile range (25th/75th percentile), respectively.
Results
Owing to personal reasons, one subject left the study after the first sojourn. Her data were excluded from all statistical analyzes and figures.
The LLS under HH indicated mild AMS (LLS 3–4) in four subjects on the first evening and in one subject on M2 and M4. LLS ≥3 were also reported in NX, namely on the first evening in two subjects and on M2 in two subjects. However, the LLS did not differ between NX and HH at any time points (all p ≥ 0.44).
With respect to VHAs, there were no significant changes during the sojourns and between NX or HH. This was true for all test channels and variables examined. In detail, there was no change in fibrinolytic capacity in the TPA test under HH (see Fig. 4). Neither lysis onset time, clot lysis index after 30 minutes in percentage (CLI30%), lysis time, nor maximum lysis showed significant differences between M2 and M4 under NX and HH or between the individual measurement time points.
Similar results were seen for clot formation (clotting time [CT], clot formation time [CFT]), clot strength (MCF), and clot amplitude (A10) in the EX test, IN test, and FIB test channels (see Figs. 1–4). Again, there were no significant differences between M2 and M4 under either NX or HH. The same was true for the comparison of the individual measurement time points with each other. The complete results of the VHA variables can be found in Table 2A.
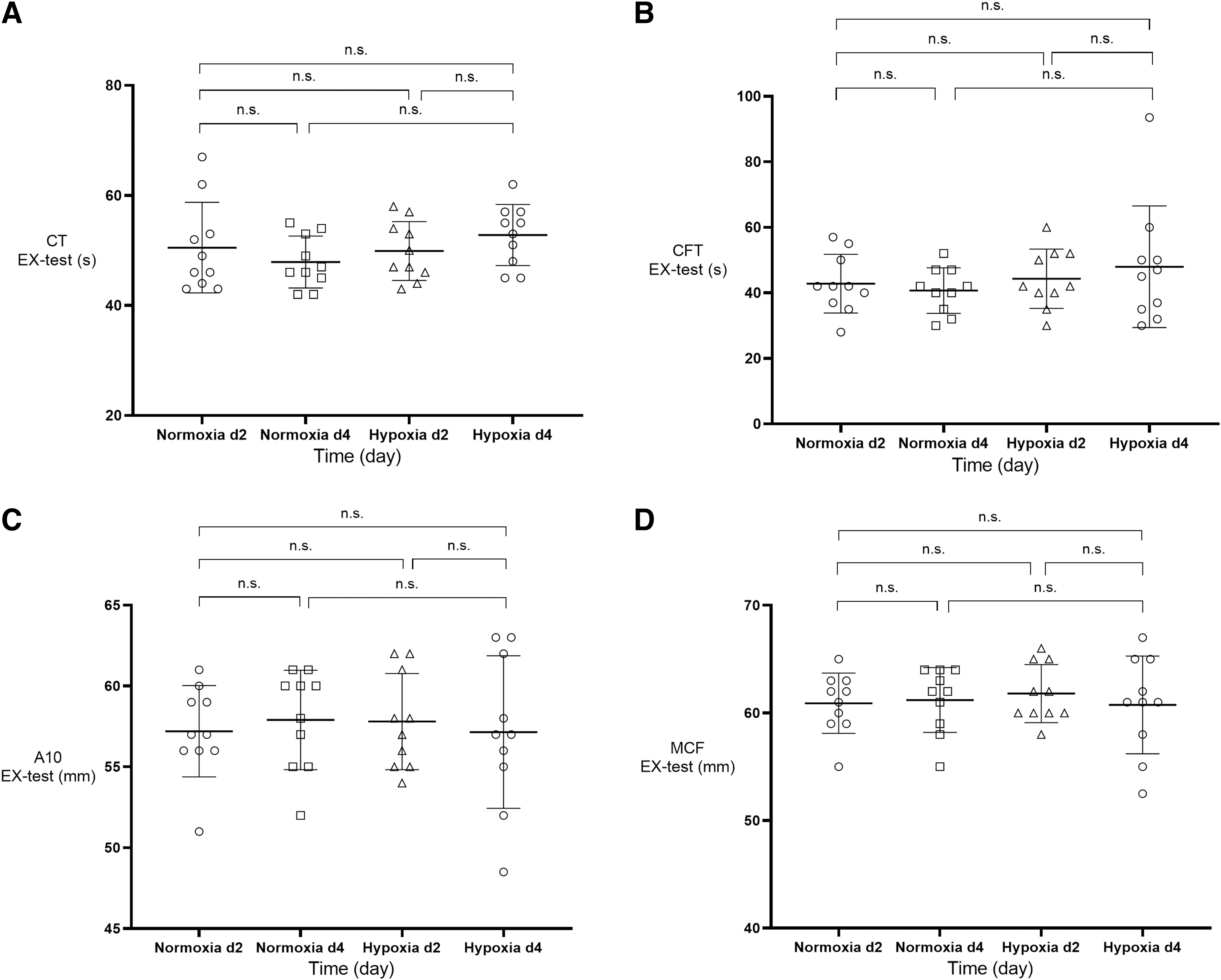
Change of thromboelastometric variables (mean+SD; n = 10) in EX test under NX and hypoxia on day 2 and 4 in whole blood.
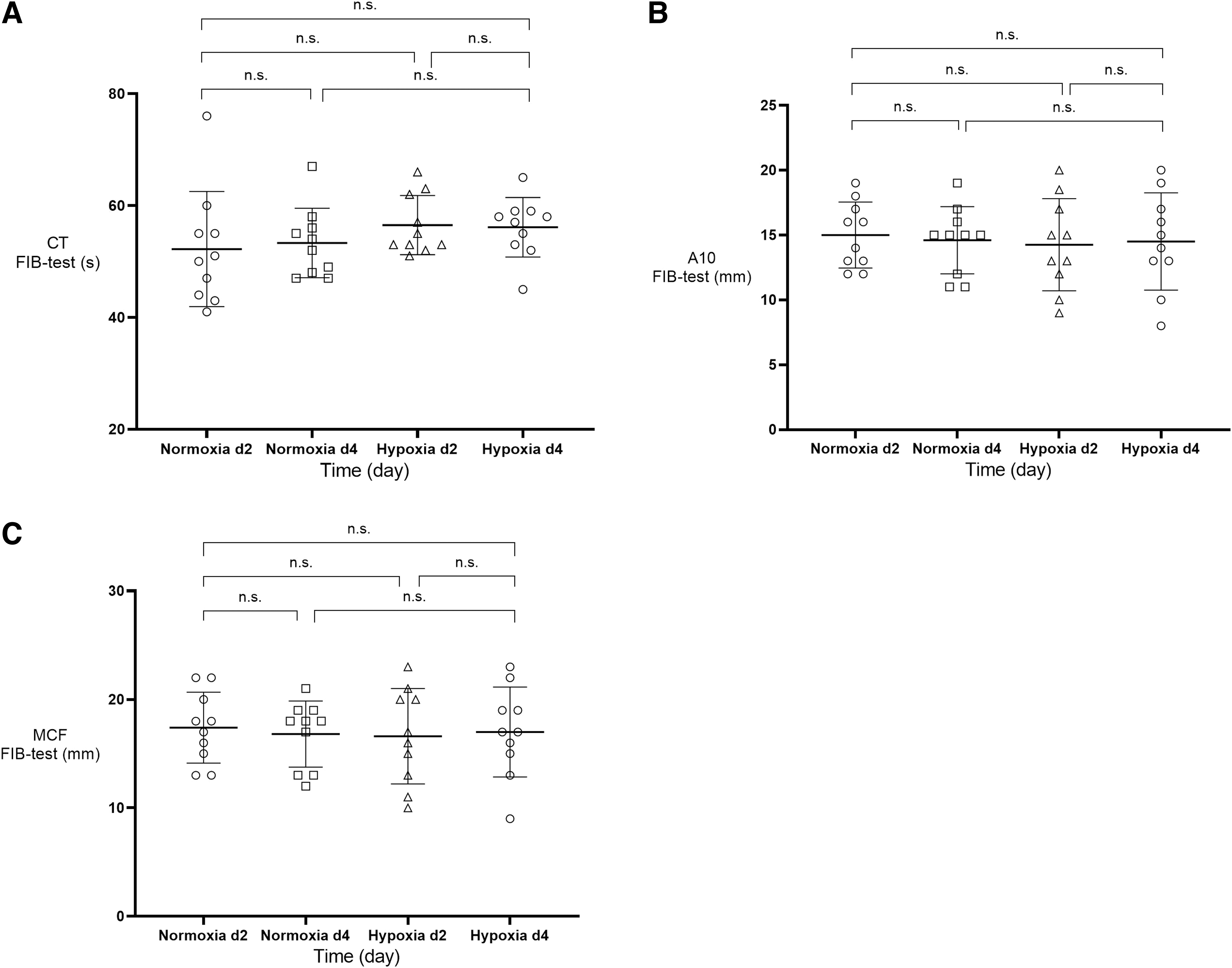
Change of thromboelastometric variables (mean+SD; n = 10) in FIB test under NX and hypoxia on day 2 and 4 in whole blood.
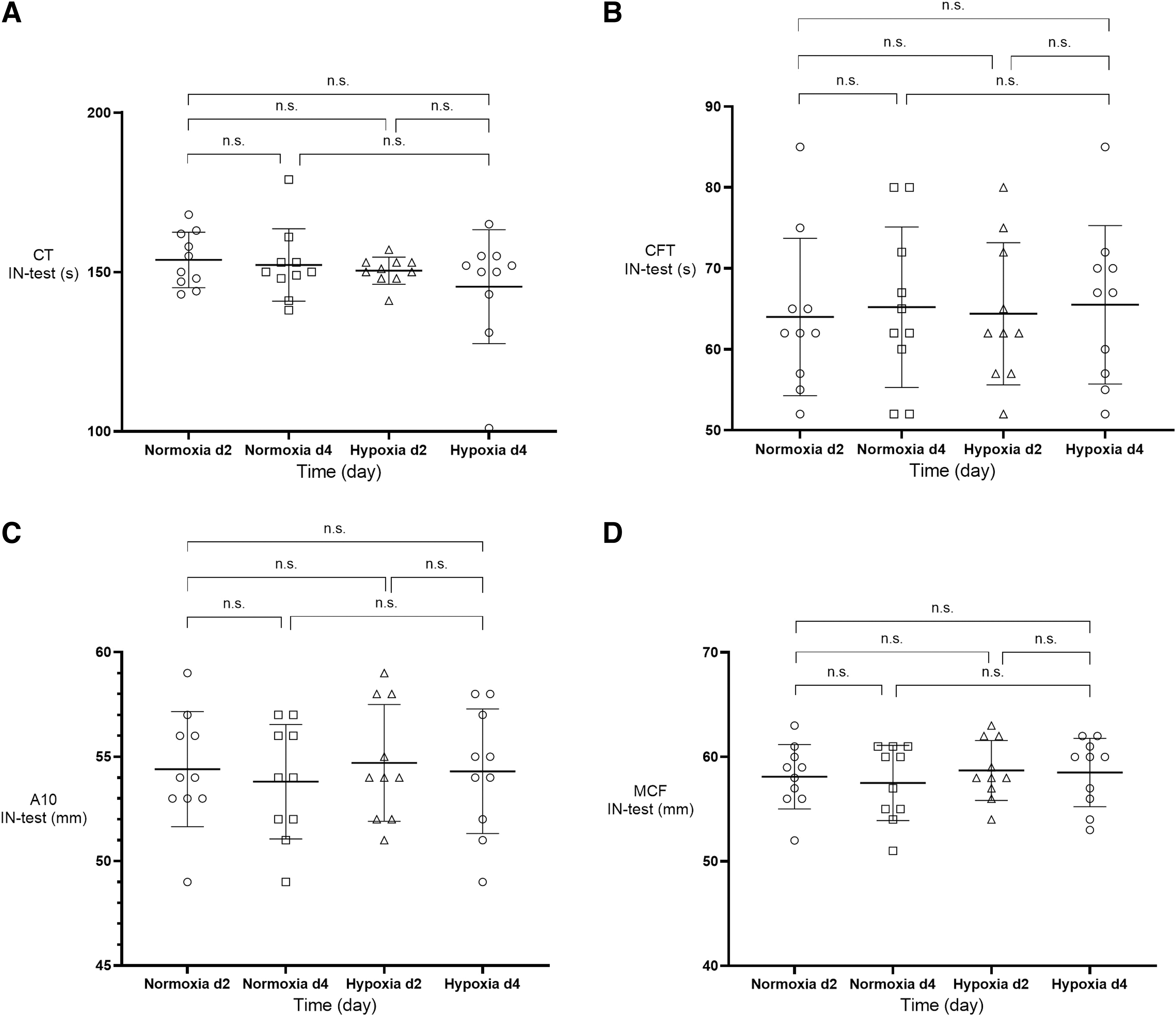
Change of thromboelastometric variables (mean + SD; n = 10) in IN test under NX and hypoxia on day 2 and 4 in whole blood.
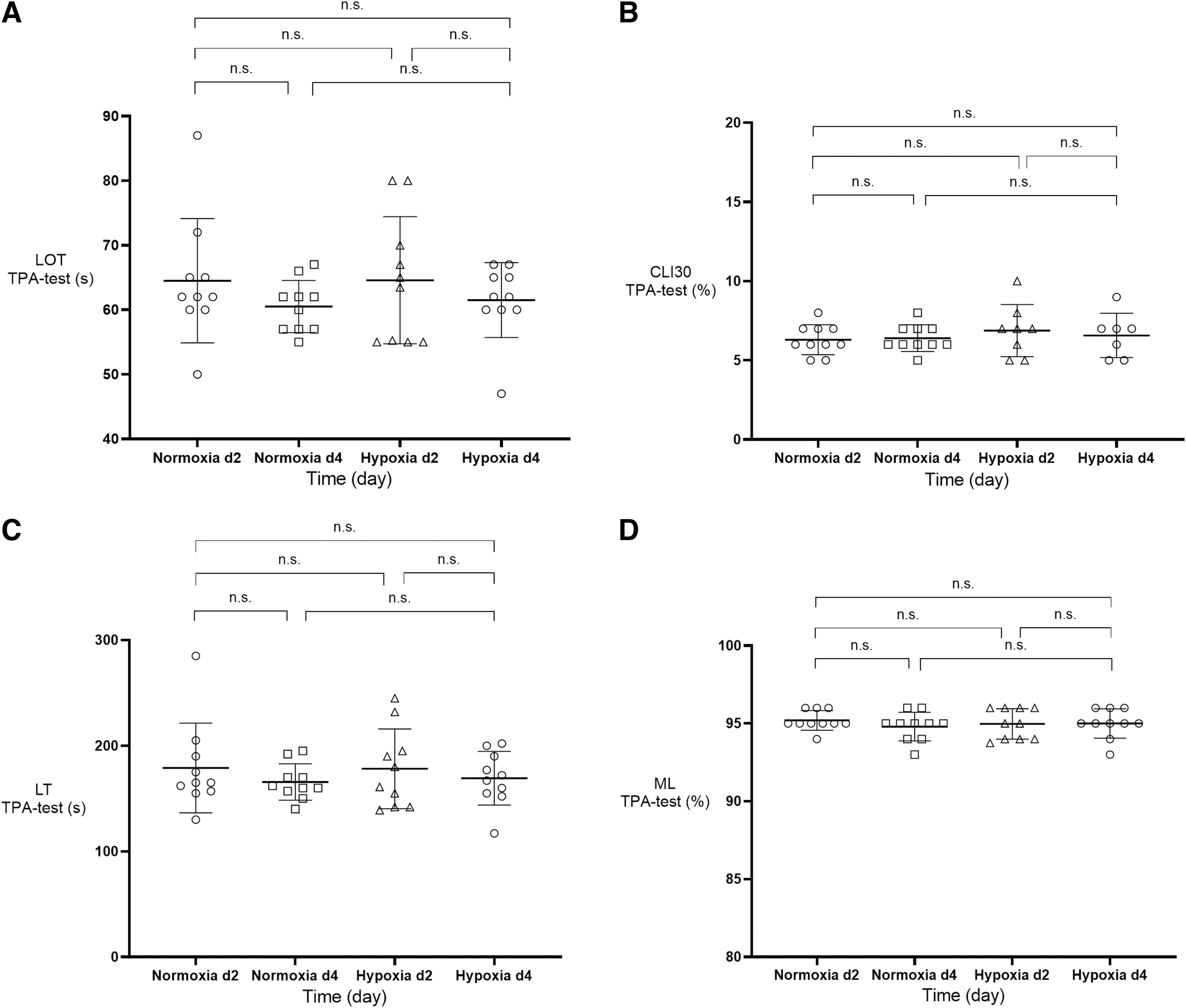
Change of lysis variables in thromboelastometric TPA test (mean + SD; n = 10) under NX and hypoxia on day 2 and 4 in whole blood.
(A) Variables of Viscoelastic Haemostatic Assays and (B) Plasmatic Coagulation Factors
CT, clotting time; CFT, clot formation time; MCF, maximum clot firmness; ML, maximum lysis; LOT, lysis onset time; LT, lysis time; CLI30, clot lysis index 30 min; PT, prothrombin time; aPTT, activated partial thromboplastin time; FVIII:C chromogenic, factor VIII coagulation activity (chromogenic assay); FVIII:C clot, factor VIII coagulation activity (clotting assay); vWF:Ag, von Willebrand factor antigen; vWF:RCo, von Willebrand factor ristocetin cofactor activity; M2/M4, second/fourth morning of sojourns; M1/M5, first/fifth morning of the sojourns.
The baseline values of PBCTs, namely aPTT, fibrinogen, FVIII:C chromogenic, FVIII:C clotting, vWF:Ag and vWF:RCo at M1 were within the normal range in all subjects and did not change from M1 to M5 in either NX or HH (see Table 2B). The only exception was PT, which slightly increased from M1 to M5 in HH (PT 1.04 ± 0.09 vs. 1.08 ± 0.09; p = 0.002).
Discussion
Studies on healthy volunteers and critically ill patients have suggested associations between hypoxia and a procoagulatory status (Anand et al., 2001; Damodar et al., 2018; Trunk et al., 2019; Wu et al., 2022). In most of these studies, however, environmental or disease-related confounders made it difficult to isolate the influence of hypoxia on coagulation. Using a strictly controlled setting, and using both well-known standard laboratory tests as well as new highly sensitive VHAs, we here demonstrate that HH per se has no influence on blood coagulation in young females during the active phase of pill consumption.
The pathophysiological mechanisms of hypoxia-induced coagulation activation have not only been a much discussed topic since the COVID-19 pandemic (Bikdeli et al., 2020; Kruse et al., 2020; Schulman et al., 2020; Spiezia et al., 2020). Also in high altitude and aviation medicine, associations between hypoxia and prothrombotic changes have been investigated in several in vitro and in vivo studies (Treml et al., 2022). Overall, the results are nowadays controversial even though the absolute altitude level and physical exertion have been identified as major influential factors (Treml et al., 2022). In agreement to this, studies that found an effect on coagulation in healthy participants have been performed at higher altitude or have been influenced by various confounding factors.
For instance, Ninivaggi et al. (2015) found an association between altitude exposure (i.e., 3,900 m) and thrombin generation in whole blood independently from physical activity, although with a high variability of the blood coagulation variables. They measured fibrinogen, FVIII:C, vWF:Ag, and plasma and whole blood thrombin generation, but no functional coagulation variables. They found an increase of thrombin generation in whole blood, but not in plasma and conclude that the cellular part of blood is involved in the prothrombotic phenotype induced by hypoxia. In contrast to this study, we used functional viscoelastometric variables that are highly sensitive and, in contrast to single coagulation factors (fibrinogen, FVIII:C), reflect the complex in vivo situation by measuring the clot formation and lysis.
In a combined bed-rest and field study, Venemans-Jellema et al. (2014) investigated the effects of immobilization and moderate HH on prothrombotic changes. The authors investigated 24 healthy female volunteers under 60-day bed-rest conditions and 25 healthy male volunteers at the Concordia Antarctic station under hypobaric conditions (equivalent to 4,000 m). They measured D-dimer, thrombin–antithrombin complexes (TAT), and prothrombin fragments as coagulation markers. The authors did not find any thrombotic changes in the vessels or an increase of coagulation parameters under HH. However, due to different conditions, this study can only be compared with our study to a very limited extent. In addition, the Antarctic is an extreme environment, so that immunological stress is a potential confounder (Strewe et al., 2019).
Another group evaluated the changes of coagulation during acclimatization in LaPaz, Bolivia, using TEG and platelet function (Rocke et al., 2018). Rocke and colleagues investigated 63 healthy male and female volunteers at sea level and up to 7 days at 5,200 m. The authors measured not only standard laboratory variables, but also functional viscoelastic values such as CT or CFT as well as platelet function parameters. They observed an increase in both clot strength and platelet activity under HH. However, the hypoxic stimulus (5,200 m) was presumably much stronger than in our study.
Different data concerning coagulation were found in the Everest study of Martin et al. (2012). The authors measured clot formation using TEG at sea level, 4,250 and 5,300 m, and found a prolongation of CT and, in contrast to Rocke et al., no increase of clot amplitude. The authors, therefore, report reduced coagulation at high altitude. In contrast to these studies and in agreement to our results, Schaber et al. (2015) found no significant or only minor changes in thrombelastometric values both over time and between nonacclimated healthy subjects with and without AMS during 12 hours 4,500 m altitude exposure (normobaric hypoxia chamber). They measured thrombelastometric variables (ROTEM), thrombin generation, and further hematological parameters during a 12 hour-exposure to normobaric hypoxia under controlled environmental conditions. The authors rejected their hypothesis of an acute activation of coagulation by hypoxia and thus support the results presented in this study.
Furthermore, two studies measured diverse aspects of coagulation at high attitude (4,559 m) in individuals with and without AMS (Bärtsch et al., 1989a; Bärtsch et al., 1989b; Lehmann et al., 2006).
Bärtsch et al. (1989a) investigated, among other variables, aPTT, vWF:Ag, fibrinopeptide A and fibrin fragment Bβ 15–42 in 25 mountaineers of whom 14 developed AMS and/or symptoms of HAPE, as well as bradykinin generated activation of blood coagulation by measuring factor XII, factor XI, plasma prekallikrein and high-molecular weight kininogen in 15 mountaineers over 5 days at 4,559 m (Bärtsch et al., 1989b). Lehmann et al. (2006) investigated prothrombin fragments 1 and 2 (PTF 1 + 2) and the thrombin–antithrombin complex (TAT) in 30 subjects with a history of HAPE and 10 healthy controls after an ascent to 4,559 m. The studies assessed contact activation of blood coagulation, in vivo thrombin formation and in vivo fibrin formation. As a result, the respective findings demonstrate that complete in vivo activation resulting in thrombin and fibrin formation does not occur in mountaineers with and without AMS.
One possible factor influencing prothrombotic changes is the use of oral contraceptives. Walter et al. (2006) showed in women that third-generation oral contraceptives in combination with exercise led to an increase in markers of thrombin and fibrin formation compared with women without oral contraceptives. Nine of the 11 participants in our study were using third-generation contraceptives. However, we did not use an exercise model, but evaluated the isolated effects of HH. Under these conditions, we found no evidence of increased coagulation under hypoxic conditions during the active phase of pill consumption.
Another potential mechanism for prothrombotic changes at high altitude that has been poorly studied is the influence of fibrinolytic capacity. In critically ill patients, it has been shown that prolonged fibrinolysis inhibition is associated with increased mortality and morbidity (Griemert et al., 2019; Moore et al., 2017). However, there are limited data in healthy subjects.
One of the few studies investigating this aspect was published recently. Jiang et al. (2021) were able to show that fibrinolysis parameters are altered by long-term exposure to HH. The authors found significantly higher plasma levels of fibrinogen, D-dimer, PAI-1, and plasminogen in healthy high-altitude subjects compared with low-altitude residents. They conclude that this phenomenon might be a physiologically compensatory response to high altitude–induced hypercoagulable state under HH and could play a potential role in adaptation to high altitude environments.
In our study under acute HH, no changes in fibrinolysis capacity were found. Although we did not examine the aforementioned parameters due to limited blood sampling, we were still able to visualize fibrinolysis using the novel TPA assay and did not find any significant changes. In detail, we found no evidence for an increased secondary fibrinolysis or inhibited fibrinolytic capacity.
A crucial factor for the development of a prothrombotic situation seems to be the combination of hypoxia and further pro-inflammatory conditions (Tyagi et al., 2014). For example, Gupta et al. (2017) demonstrated in rats that changes in the inflammasome can enhance venous thrombosis under HH. The significance of HH itself has been poorly elucidated. Our data provide first hints that the combination of hypoxia and other stressors is crucial for a procoagulatory status.
Limitations
Our study has some limitations. First, the study population was relatively small compared with other studies. However, the group was very homogeneous with comparable demographic data. Furthermore, we only examined female subjects. This was done to eliminate sex-specific effects that have been shown in previous studies on HH and coagulation (Huskens et al., 2016). Hence, our results cannot be extrapolated to male subjects. In addition, diet, fluid intake, physical exercise, hormonal status, and other factors were standardized. The best possible standardization of our study allowed us to isolate the effects of HH on blood coagulation.
However, this standardization is also a limitation of the study, as it complicates the transfer of the findings to real-world conditions, for example, at high altitude or in aviation. It is possibly the combination of several stressors that leads to coagulation activation in mountain expeditions, air travel, or even in critically ill patients. This issue could be clarified by further chamber studies in which the effects of cold, physical stress, or isolation are additionally investigated.
Moreover, we did not analyze platelet function and activation. The effects of HH on platelets, therefore, remain unclear. Nevertheless, there were no effects on functional coagulation, especially not on maximum clot firmness, which is significantly influenced by platelet count.
Conclusion
To the best of our knowledge, our study is the first focusing on the isolated effects of HH on functional coagulation in healthy women. We demonstrate that hypoxia per se has no impact on blood coagulation in vivo. This suggests that the clot activation under hypoxia described in previous studies occurs mainly in combination with other influencing factors such as strenuous exercise, dehydration, immobilization, isolation, or cold. Further standardized chamber studies, including such other influencing factors in a controlled manner, should investigate this issue.
Footnotes
Authors' Contributions
T.K. and S.T.S. conceived the project and wrote the article; A.W., G.R., R.T., J.R., H.G., and C.S. collected the data; T.K., A.W., T.M., G.R., R.T., J.R., H.G., and C.S analyzed the data.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was funded by a research grant from BEXMED (Deutsche Gesellschaft für Berg- und Expeditionsmedizin) to T.K. and S.T.S.