
Abstract
Gardner, Laurel, Linda E. Keyes, Caleb Phillips, Elan Small, Tejaswi Adhikari, Nathan Barott, Ken Zafren, Rony Maharjan, and James Marvel. Women at altitude: Menstrual-cycle phase, menopause, and exogenous progesterone are not associated with acute mountain sickness. High Alt Med Biol. 00:000–000, 2024.
Background:
Elevated progesterone levels in women may protect against acute mountain sickness (AMS). The impact of hormonal contraception (HC) on AMS is unknown. We examined the effect of natural and exogenous progesterone on the occurrence of AMS.
Methods:
We conducted a prospective observational convenience study of female trekkers in Lobuche (4,940 m) and Manang (3,519 m). We collected data on last menstrual period, use of exogenous hormones, and development of AMS.
Results:
There were 1,161 trekkers who met inclusion criteria, of whom 307 (26%) had AMS. There was no significant difference in occurrence of AMS between women in the follicular (28%) and the luteal (25%) phases of menstruation (p = 0.48). The proportion of premenopausal (25%) versus postmenopausal women (30%) with AMS did not differ (p = 0.33). The use of HC did not influence the occurrence of AMS (HC 23% vs. no HC 26%, p = 0.47), nor did hormonal replacement therapy (HRT) (HRT 11% vs. no HRT 31%, p = 0.13).
Conclusion:
We found no relationship between menstrual-cycle phase, menopausal status, or use of exogenous progesterone and the occurrence of AMS in trekkers and conclude that hormonal status is not a risk factor for AMS. Furthermore, women should not be excluded from future AMS studies based on hormonal status.
Introduction
Women comprise nearly half of outdoor recreationists (Outdoor Foundation, 2002) and an increasing number of high-altitude athletes (Huey et al., 2020). With this rise in popularity, there has been a renewed focus on how female physiology might affect the risk of acute mountain sickness (AMS). Historically, women have largely been excluded from altitude research, at least partly because of the concern that progesterone might affect the occurrence of AMS and the challenge of controlling for fluctuating progesterone levels throughout the menstrual cycle. This has resulted in a significant inequity of research on women at altitude.
Progesterone is known as a respiratory stimulant (Skatrud et al., 1978) that can improve oxygen saturation at altitude by increasing the hypoxic ventilatory response (HVR) (Kryger et al., 1978). This observation has led to the hypothesis that higher levels of naturally circulating progesterone in women may provide an advantage in acclimatizing to altitude. Progesterone naturally spikes in the luteal phase of menstruation. Studies comparing cycle phases demonstrate that women in the luteal phase had increased hypoxic and hypercapnic ventilatory responses at altitude (Schoene et al., 1981; Takano, 1984; Regensteiner et al., 1990; Loeppky et al., 2001; Takase et al., 2002; Richalet et al., 2020) but did not find differences in the occurrence of AMS between cycle phases (Rock et al., 2001; Richalet et al., 2020). Supplemental progesterone also has physiological benefits in men, resulting in lower peripheral arterial carbon dioxide levels and higher peripheral oxygen saturation but, as in women, did not result in a reduction in occurrence of AMS (Wright et al., 2004).
Existing data on the effects of exogenous hormones in the form of hormonal contraception (HC) are inconclusive. Sandoval et al. (2001) found HC to have a protective effect in women at simulated altitude. Conversely, a small study of women traveling rapidly to altitude showed that those on HC were more susceptible to AMS and acetazolamide to be less effective at preventing AMS in that cohort (Harrison et al., 2013). A large database study of French women found that neither HC nor hormonal replacement therapy (HRT) affected the occurrence of AMS (Richalet et al., 2020).
We sought to determine whether menstrual-cycle phase, menopause, or the use of exogenous hormones affects the occurrence of AMS in women trekking at high altitude in Nepal.
Materials and Methods
Study design
This was a survey-based prospective observational convenience study designed to evaluate the relationship between female sex, hormones, and AMS as part of the Current Understanding and Relevant Trends in Altitude Illness in Nepal (CURTAIN) study. The Institutional Review Board’s approval was obtained through Stanford University and Nepal Health Research Council. Because of the remote location of the study, verbal consent was obtained. Participants completed a questionnaire on their first evening at altitude (Fig. 1), with data on demographics, ascent profile, last menstrual period (LMP), menopausal status, and the use of HC and HRT. Contraceptives were classified by delivery method and type of hormone. Subjects self-reported the 2018 Lake Louise Questionnaire (LLQ) for AMS on the evening of and the morning after arrival at the study site. We defined AMS as a score of ≥3 with at least one point for headache and moderate–severe AMS as a score of ≥6 with at least one point for headache (Roach et al., 2018). Participants were considered to have AMS if they scored positively at either time point. In premenopausal women not using HC, we used the difference between the date the survey was administered and the reported LMP to determine the menstrual-cycle phase of each participant. We considered women at 0–14 days after LMP to be in the follicular phase and 15–30 days after LMP to be in the luteal phase. We excluded women >30 days after their LMP as we were unable to define whether this was a natural cycle length or if the cycle was delayed.
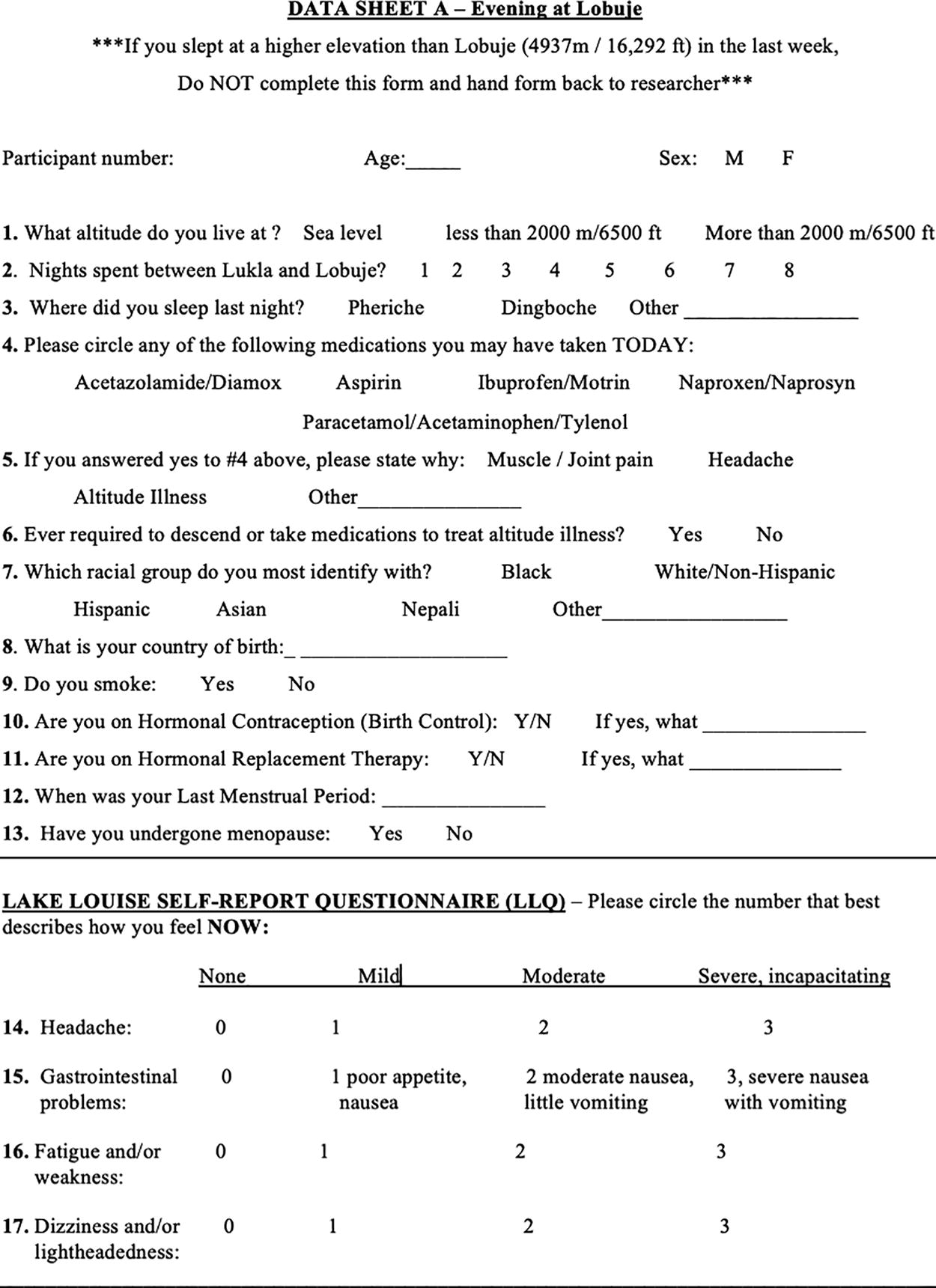
Data sheet filled out by participants in Lobuche. Participants in Manang used a similar survey.
Participants and data collection
We enrolled female trekkers traveling through Manang (3,519 m) on the Annapurna Circuit and Lobuche (4,940 m) on the Everest Base Camp Trek. Women were eligible for the study if they had not spent a night within the past week at a higher altitude to avoid potential confounding from previous acclimatization. Surveys were administered in English and Nepali. Participants who did not fill out both the evening and the morning LLQ sections were excluded from the final analysis. Women were excluded from the cycle-phase analysis if they reported HC use or if the cycle phase could not be clearly calculated (Fig. 2). We collected data on possible confounding variables including rate of ascent (defined as nights spent ascending to study altitude), smoking, acetazolamide use, and history of altitude illness.
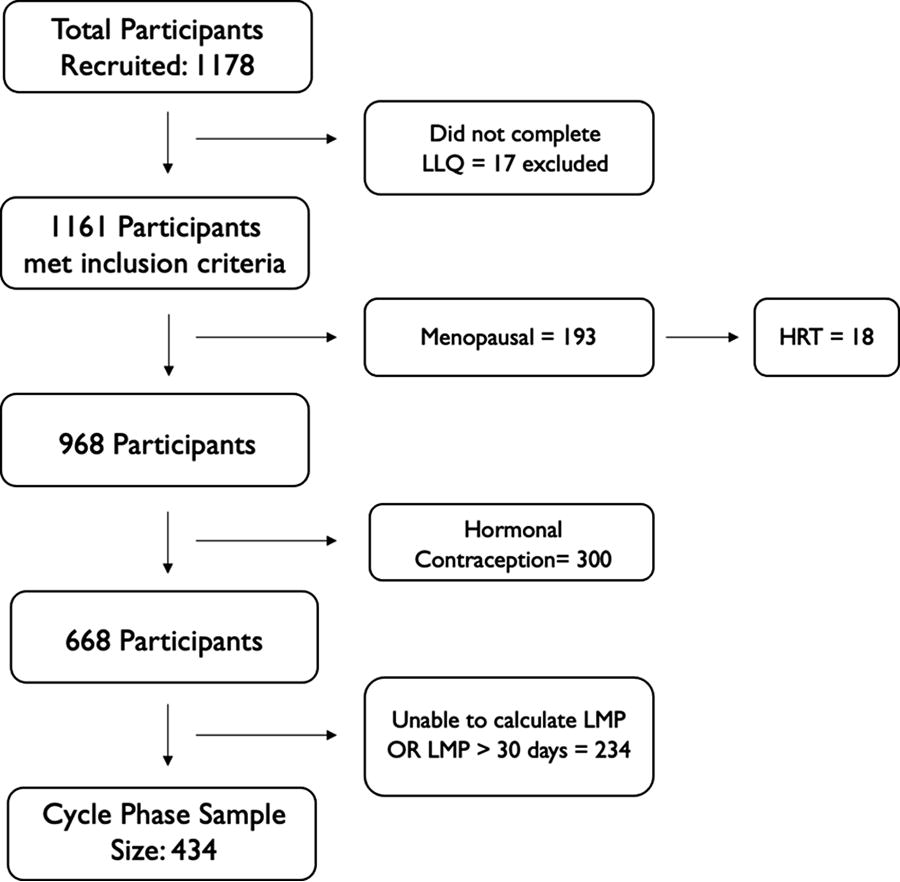
Flowchart describing participant inclusion and exclusion criteria for cycle phase, menopause, hormonal contraception, and hormonal replacement therapy analysis. LLQ, Lake Louise Questionnaire; LMP, last menstrual period.
Statistical analysis
We performed data analysis and postprocessing using the R environment for statistical computing version 4.1.1. We analyzed participants by survey location and within a combined cohort. We assessed differences in demographics between AMS+ and AMS− groups using the Welch two-sample t-test for continuous variables and Pearson’s chi-squared test for categorical data. We analyzed categorical variables with multiple responses as binary variables. We compared HC use and AMS using a two-sample test for equality of proportions. We calculated odds ratio using the median unbiased estimate with mid-p exact confidence intervals. We defined statistical significance as p < 0.05.
Results
We enrolled 1,178 female participants, 833 in Lobuche and 345 in Manang (Table 1). Exclusion of 17 of these enrollees was necessary because of incomplete data, leaving a total of 1,161 participants (Fig. 1). In total, 434 (37%) participants met criteria for inclusion in the cycle-phase analysis. Of these, 257 (59%) were in the follicular phase and 177 (41%) were in the luteal phase. Neither risk nor severity of AMS differed between menstrual-cycle phases (Table 2, Fig. 3). In total, 968 (83%) women were premenopausal and 193 (17%) were postmenopausal. There was no difference in the risk of AMS between menopausal and premenopausal women (Table 3, Fig. 3).

Distribution of LLQ score by hormonal status in all participants. Solid line represents score of 3. Dashed line represents score of 6. Data jittered for visualization, all scores ≥0. HC, hormonal contraception; HRT, hormonal replacement therapy; LLQ, Lake Louise Questionnaire.
Participant Demographics
Demographics for all women surveyed.
Median (IQR).
Median nights spent prior to arrival at study site (IQR).
AMS, acute mountain sickness; IQR, interquartile range; NR, no response.
Acute Mountain Sickness and Menstrual-Cycle Phase
AMS = LLQ ≥3, including at least one point for headache.
Moderate–severe AMS = LLQ ≥6, including at least one point for headache. There was no significant difference in occurrence of AMS between the follicular and the luteal phase for AMS (p = 0.48) or moderate–severe AMS (p = 1).
AMS, acute mountain sickness; LLQ, Lake Louise Questionnaire; OR, odds ratio.
Acute Mountain Sickness and Menopausal Status
AMS = LLQ ≥3, including at least one point for headache.
Moderate–severe AMS = LLQ ≥6, including at least one point for headache. There was no significant difference between pre- and postmenopausal women for AMS (p = 0.33) or moderate–severe AMS (p = 0.66).
AMS, acute mountain sickness; LLQ, Lake Louise Questionnaire; OR, odds ratio.
Of 968 premenopausal participants, 300 (31%) reported using a form of HC. There was no difference in risk or severity of AMS between women reporting HC use and those not using HC (Table 4, Fig. 3). There was no difference in occurrence of AMS between progesterone-only HC methods and combined oral contraceptives, nor for women on HRT (Table 4, Fig. 3).
Acute Mountain Sickness and Exogenous Progesterone
HC versus not on HC comparison considered only the premenopausal cohort. HRT versus no HRT comparison considered only our postmenopausal cohort.
AMS = LLQ ≥3, including at least one point for headache.
Moderate–severe AMS = LLQ ≥6, including at least one point for headache.
Unable to calculate odds ratio because of inadequate sample size. No significant difference between groups.
AMS, acute mountain sickness; HC, hormonal contraception; HRT, hormonal replacement therapy; OCP, oral contraceptive pill; OR, odds ratio.
We collected data on multiple possible confounding variables including acetazolamide use, ascent profile, smoking, and history of AMS (Table 5). A multivariate analysis revealed that acetazolamide use, smoking, or prior history of altitude illness did not influence the occurrence of AMS. There was no difference in ascent profile between women with AMS and those without AMS in Manang. However, in Lobuche, women reporting moderate–severe AMS ascended at a statistically faster rate (6.1 vs. 6.4 days, p = 0.04).
Potential Confounding Variables
AMS = LLQ ≥3, including at least one point for headache.
Moderate–severe AMS = LLQ ≥6, including at least one point for headache.
Median nights spent ascending to study site altitude (IQR). Comparison shown for cycle-phase cohort (premenopausal women not on HC).
AMS, acute mountain sickness; HC, hormonal contraception; IQR, interquartile range; LLQ, Lake Louise Questionnaire.
Discussion
Our results suggest that variations in progesterone levels between the follicular and the luteal phases are too weak to affect the risk of AMS. This lack of hormonal effect on AMS is further supported by our finding that the occurrence of AMS is similar between pre- and postmenopausal women. In studies that demonstrate the physiological benefit of progesterone in the luteal phase, the increased HVR in the luteal phase was equivalent to the HVR in male controls (Loeppky et al., 2001). It is likely that increased HVR associated with higher progesterone levels is less important than the increased HVR associated with ascent to high altitude. There is no evidence to support excluding women from studies based on their levels of natural progesterone.
Several small studies of exogenous progesterone in the form of HC have found mixed results with some showing decreased incidence of AMS (Sandoval et al., 2001), others with increased incidence of AMS (Harrison et al., 2013), and others finding no effect (Richalet et al., 2020). These findings were limited by inadequate sample size and retrospective or noncontemporaneous assessment of AMS. The large size of our prospective study strengthened our ability to examine the relationship between exogenous progesterone and AMS. Our results demonstrate that HC does not affect the risk of AMS. This finding holds true for the progesterone-only contraceptive methods and for combined oral contraceptives, the most commonly used method in our study. There was too much variability in progesterone dosage among reported methods to evaluate for differences between high- and low-dose methods. Although the number of participants using HRT was small, the negative result strengthens the argument that synthetic progesterone does not affect the risk of developing AMS in postmenopausal women.
Limitations
The LLQ is a validated tool to evaluate AMS but relies on self-reported subjective symptoms. Differences in perception of symptoms might introduce bias. As this was an observational study, we based the assessment of cycle phase on traditionally accepted cycle-phase ranges rather than controlling for each participant’s cycle length. Travel to high altitude can disrupt menstrual cycles, with women reporting alterations in the timing of their period (Miller, 1999). Surveys were administered in English and Nepali, limiting participation by individuals who did not read either language. We likely missed enrolling some participants who developed moderate–severe AMS but had descended before reaching the study sites or were too ill to participate in our survey. This may have introduced bias and limited our overall sample size. We assumed biological sex and did not include trans or nonbinary options or people taking sex hormones for these reasons.
Conclusion
The CURTAIN study provided us with one of the largest populations to date to evaluate the relationship between progesterone and AMS. Our data provide strong evidence that, whether in its natural or synthetic form, progesterone does not affect the occurrence of AMS in women. This was true for menstrual-cycle phase, menopause, and the use of exogenous progesterone in the form of HC and HRT. These findings can start to provide a basis to tailor more individualized recommendations for women at altitude. There is no need for women to alter ascent profiles based on cycle phase or menopausal status. Women can safely continue to use whatever HC or HRT method they prefer. Ultimately, these results are empowering for women, allowing them to control their cycle and take or avoid hormones at altitude however they like, without affecting their risk of AMS.
Footnotes
Acknowledgments
We thank all the participants. We thank the lodge owners in Lobuche and Manang for welcoming the research teams into their communities and for making our work possible. We also thank Garrett Madison of Madison Mountaineering for his gracious assistance in helping to resupply study materials. In addition, we would also like to thank the CURTAIN research team for assistance with study logistics and survey administration.
Authors’ Contributions
L.G.: Conceptualization, methodology, investigation, data curation, data interpretation, visualization, writing—original draft, writing—reviewing and editing, project administration; C.P.: Software, formal analysis, validation, data curation, visualization, writing—reviewing and editing; L.E.K.: Conceptualization, data interpretation, writing—reviewing and editing; E.S.: Investigation, data curation, project administration, writing—reviewing and editing; T.A. and N.B.: Investigation, writing—original draft, reviewing and editing; K.Z.: Visualization, writing—reviewing and editing; R.M. and J.M.: Conceptualization, methodology, supervision, resources, writing—reviewing and editing, project administration.
Author Disclosure Statement
The authors have no financial disclosures or conflicts of interest.
Funding Information
This project did not receive outside funding.