
Abstract
Wang, Bowen, Mengjia Peng,, Liheng Jiang,, Fei Fang,, Juan Wang,, Yan Li,, Ruichen Zhao,, and Yuliang Wang,. A Rare Case of High-Altitude Polycythemia Complicated by Spontaneous Splenic Rupture. High Alt Med Biol. 25:247–250, 2024.—High-altitude polycythemia, a condition characterized by an increase in red blood cellRBC mass, can occur after prolonged exposure to high altitudes. While several studies have explored the complications associated with high-altitude polycythemia, there is currently no literature available on spontaneous spleen rupture caused by high-altitude polycythemia. Here, we reported a case of acute abdominal pain and hemodynamic instability in a 36-year-old male who had been residing at high altitude for 6 years, without any recent history of trauma. Computed tomography imaging revealed significant fluid accumulation in the abdomen, and a tear of the splenic capsule was identified during the following laparotomy. Subsequent evaluations confirmed the presence of polycythemia secondary to prolonged high-altitude exposure as the underlying etiology. This case served as an important reminder that high-altitude polycythemia could lead to serious complications, such as spontaneous spleen rupture. Clinicians should be aware of this potential complication and consider it in the differential diagnosis of patients presenting with abdominal pain and hemodynamic instability in this population.
Introduction
High-altitude polycythemia is a common physiological response to low oxygen availability at high altitudes. It is characterized by an increase in red blood cell (RBC) mass, hemoglobin concentration, and hemoconcentration (Wang et al., 2022). Although increased RBC could partially compensate for the hypoxia caused by long-term exposure to high altitude, excessive accumulation of RBC might affect blood flow, increase blood viscosity, and cause other serious complications (Wang et al., 2023). However, no evidence of spontaneous spleen rupture caused by high-altitude polycythemia has been found.
We present the case of a 36-year-old male who developed high-altitude polycythemia complicated by spontaneous spleen rupture. This case highlighted the importance of recognizing and managing this rare but potentially life-threatening complication of high-altitude polycythemia.
Case Presentation
A 36-year-old male patient presented to our hospital with a 6-day history of abdominal pain and bloating. One day before, he suddenly developed an altered mental status and was found with a blood pressure of 40/20 mmHg. After fluid resuscitation, he was transferred to our hospital for further treatment.
On physical examination, the patient had a temperature of 36.7°C, a heart rate of 152 beats per minute, a respiratory rate of 28 breaths per minute, and a blood pressure of 70/30 mmHg. Both tenderness in the upper abdomen and positive shifting dullness were observed. Diagnostic paracentesis yielded dark red intraperitoneal fluid. Laboratory data showed a RBC count of 4.1 × 1012/l, hemoglobin level (Hb) of 126 g/l, hematocrit level of 39%, creatinine level of 61.3 μmol/l, Alanine aminotransferase (ALT) level of 15 U/l, Aspartate transaminase (AST) level of 18 U/l, prothrombin time of 72.0 seconds, and the activated partial thromboplastin time or thrombin time did not coagulate. Abdominal enhanced computed tomography showed an enlarged spleen and massive intraperitoneal fluid (Fig. 1A).
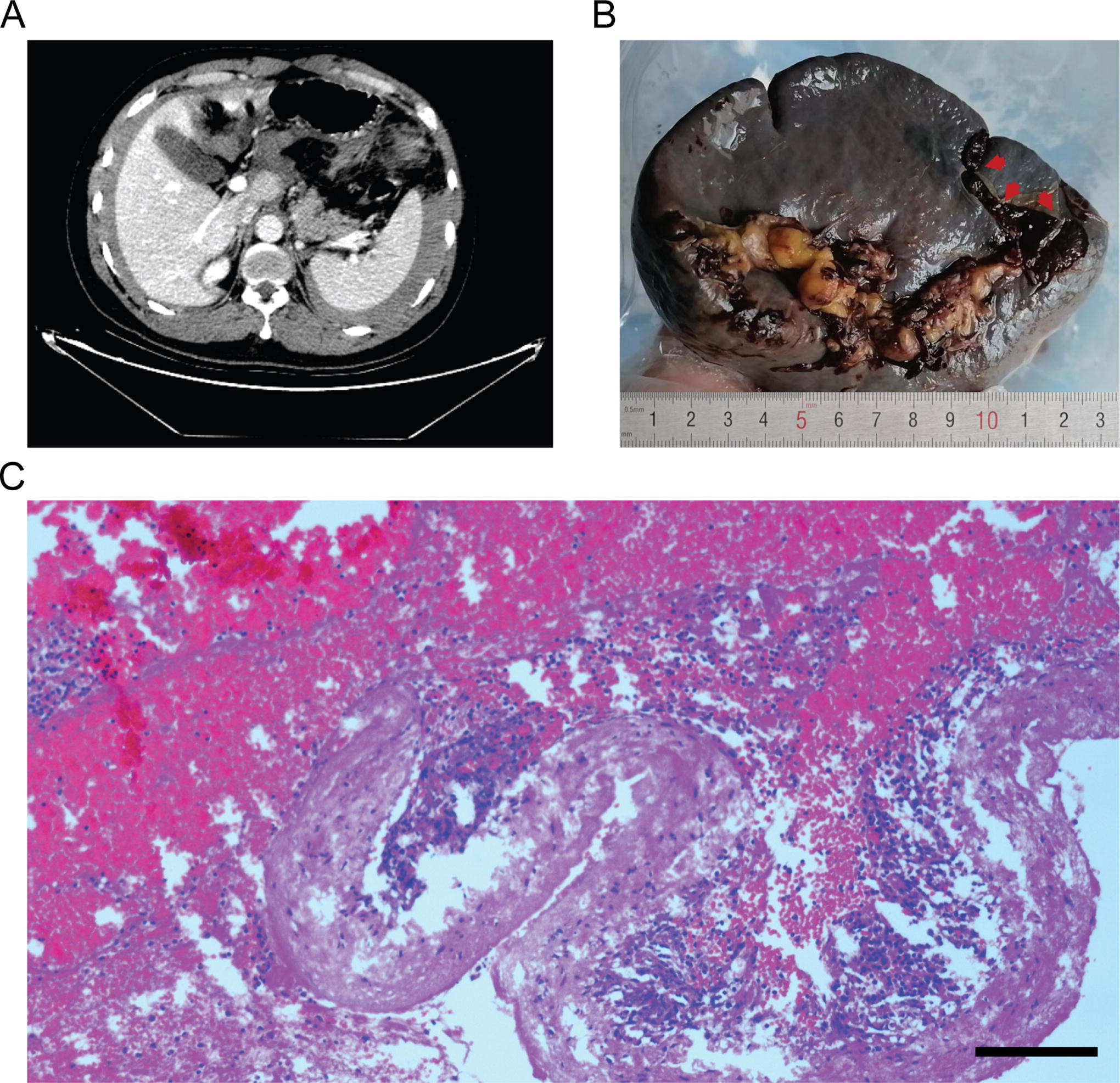
Imaging, macroscopic, and pathological manifestations of ruptured spleen.
An immediate exploratory laparotomy was performed, revealing approximately 4,000 ml of dark red, non-coagulated blood in the peritoneal cavity. A 4.0 cm × 0.5 cm irregular laceration with local active bleeding was observed in the lower pole of the enlarged spleen (12.5 cm × 10.5 cm × 4.2 cm) (Fig. 1B). Splenectomy was performed, and pathology suggested normal spleen tissue and hemorrhage (Fig. 1C). The patient received a blood transfusion and fluid resuscitation and was discharged later.
The patient’s medical history denied recent abdominal trauma. Six years ago, he had migrated from a low-altitude area to Tibet, China (altitude 3,700 m). Annual routine physical examinations were performed, showing high-altitude polycythemia and hyperuricemia (Fig. 2). However, the patient did not show any obvious symptoms. Upon returning to the low-altitude area, the patient’s RBC count and uric acid level returned to normal (Fig. 2).
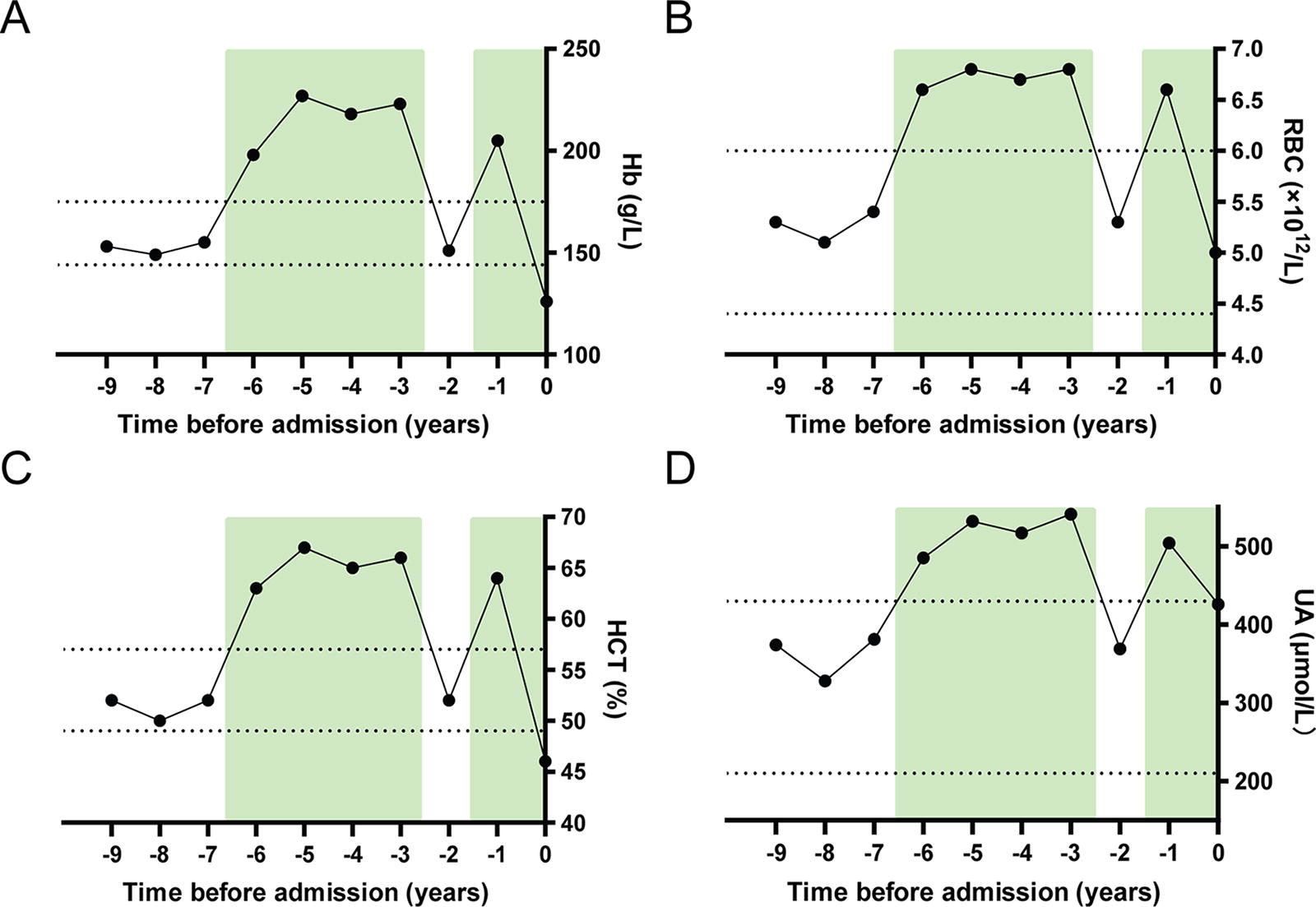
Laboratory results of patient’s the annual routine physical examinations before admission. Figures showed the results of physical examinations of Hb
Discussion
A moderate increase in RBC count has been shown to facilitate acclimatization in high-altitude populations (West, 2012). Nevertheless, excessive accumulation of RBC in high-altitude polycythemia would not improve their oxygen-carrying capacity. Instead, it increases blood viscosity and congestion, leading to splenomegaly (Holmstrom et al., 2020; Lv et al., 2016). In this case, the patient’s medical history of high-altitude polycythemia and the enlarged spleen also further supported the hypothesis that a combination of increased blood viscosity, a congested spleen, and mechanical stress on the splenic capsule contributed to the occurrence of spontaneous spleen rupture.
Many studies have tried to explain the pathogenesis of high-altitude polycythemia. Researchers have investigated various factors leading to high-altitude polycythemia and its complications, including oxidative stress, hypoxic response, erythropoietin production, and genetic susceptibility (Villafuerte et al., 2022). Hypoxia-inducible factors (HIFs), particularly HIF-1α, are key regulators of erythropoiesis and were involved in the pathogenesis of high-altitude polycythemia. Under hypoxic conditions, HIF-1α promote the production of erythropoietin and stimulate erythroid progenitor cells in the bone marrow (Shaharuddin et al., 2023). This leads to an increase in red blood cell production and contributes to the development of polycythemia. Oxidative stress is an important factor in high-altitude polycythemia pathogenesis. Exposure to high-altitude hypoxia results in increased production of reactive oxygen species (ROS). The imbalance between ROS production and antioxidant defenses contributes to the damage of target organs (Li and He, 2019).
We note that both high-altitude polycythemia and polycythemia vera (PV) are characterized by an increase in RBC. However, cases of spontaneous spleen rupture caused by PV have been previously reported (Hardy et al., 2016), while spontaneous spleen rupture associated with high-altitude polycythemia are relatively rare. This difference could partly be attributed to variations in platelet status and quantity between the two diseases. PV often presents with leukocytosis and elevated dysfunctional platelets (Huang and Li, 2022), whereas high altitude-polycythemia is typically accompanied by reduced platelet levels due to prolonged high-altitude exposure (Wang et al., 2022). Under normal circumstances, the spleen plays a role in clearing aging, abnormal, and damaged platelets and red blood cells. In fact, the spleen might have to deal with a heavier load if platelets are destroyed too quickly or excessively. (Ebbo et al., 2017). Thus, an increased platelet count in PV could be a contributing factor to the pathogenesis of spontaneous spleen rupture.
Notably, not all individuals with high-altitude polycythemia develop splenic rupture. In this particular case, we noted that the patient’s multiple trips between high-altitude and low-altitude areas led to fluctuating levels of Hb and RBCs. This might be one of the triggering factors for the occurrence of spontaneous spleen rupture. Besides, the high workload and irregular lifestyle of this young patient may have been potential factors resulting in his splenomegaly. However, these factors did not seem to fully explain the etiology of high-altitude polycythemia with spontaneous spleen rupture in this patient. Thus, additional studies, including genetic testing and more pathological splenic testing, are desperately needed to examine his distinct features and offer new insights.
In conclusion, our case provided a rare case of high-altitude polycythemia complicated by spontaneous spleen rupture. Clinicians should be aware of this potential complication when evaluating patients who reside in or travel to high-altitude areas. Further research is needed to better understand the underlying mechanisms leading to splenic rupture in high-altitude polycythemia and to develop targeted preventive strategies for this rare complication.
Footnotes
Acknowledgments
The authors are grateful to the many medical staff and pathologists for their dedication of the patient.
Authors’ Contributions
B.W. and Y.L. were responsible for the study concept, designed the study, and took responsibility for the integrity of the data and the accuracy of the data analysis. B.W., M.J., and L.H. collected the data. B.W., M.J., F.F., J.W., and Y.L. drafted the article and did the statistics analysis. R.C. and Y.L. revised the article and gave final approval for the version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors contributed to the article and approved the submitted version.
Author Disclosure Statement
All authors declare no competing interests.
Data Availability Statement
The raw data of this article will be made available by the authors, if it is necessary. Participates involved in this study has agreed with an informed consent for the publication of this case report.
Ethics Statement
Ethical approval for this study (Ethical Committee GHTM 2023-07-018) was provided by the Ethical Committee of General Hospital, Lhasa, China on 24th July, 2023.
Funding Information
This work was supported by the Natural Science Fund of Tibet Autonomous Region (ZRKX2024000383).