
Abstract
Szymczak, Robert K., Magdalena Sawicka, and Małgorzata Jelitto. Recurrent pulmonary embolism at high altitude in a mountaineer with hereditary thrombophilia. High Alt Med Biol. 25:345–347, 2024.—It is speculated that high-altitude travel is an independent risk factor for thrombosis. Mountaineering-specific factors, such as hypoxia, cold, and immobilization, may interact with patient-specific risk factors and contribute to thrombus formation. We present the case of a mountaineer with hereditary thrombophilia who experienced recurrent pulmonary embolism during high-altitude expeditions.
Case Presentation
A mountaineer developed pulmonary embolism (PE) during two expeditions. He had his first PE at the age of 35, after a 22-hour ascent of Cho Oyu (8,188 m) and two bivouacs >7,500 m. PE recurred 5 years later on Broad Peak (8,051 m), after a 2-week stay between 4,800 and 6,300 m and 2 days of diarrhea. In both cases, clinical features at 5,000 m were similar: dyspnea, dry cough, unilateral pleural pain, tachypnea (RR > 25), tachycardia (HR > 100), and SaO2 <60%. The first PE was diagnosed after returning from the expedition. The second PE was diagnosed by the expedition doctor, who started oxygen therapy, placed the mountaineer in a portable hyperbaric chamber, and administered low-molecular-weight heparin (Fig. 1). In both cases, it took 4 to 7 days from the onset of symptoms to hospital admission. The PEs were confirmed by CT angiography, which revealed embolic changes and pleural effusion (Fig. 2). Elevated D-dimer levels (>2.0 mg/l) and negative T waves in electrocardiogram lead III were observed. Echocardiography completed after the second PE showed right ventricular enlargement and mitral and tricuspid regurgitation.

Mountaineer taking a therapeutic dose of low-molecular-weight heparin subcutaneously.
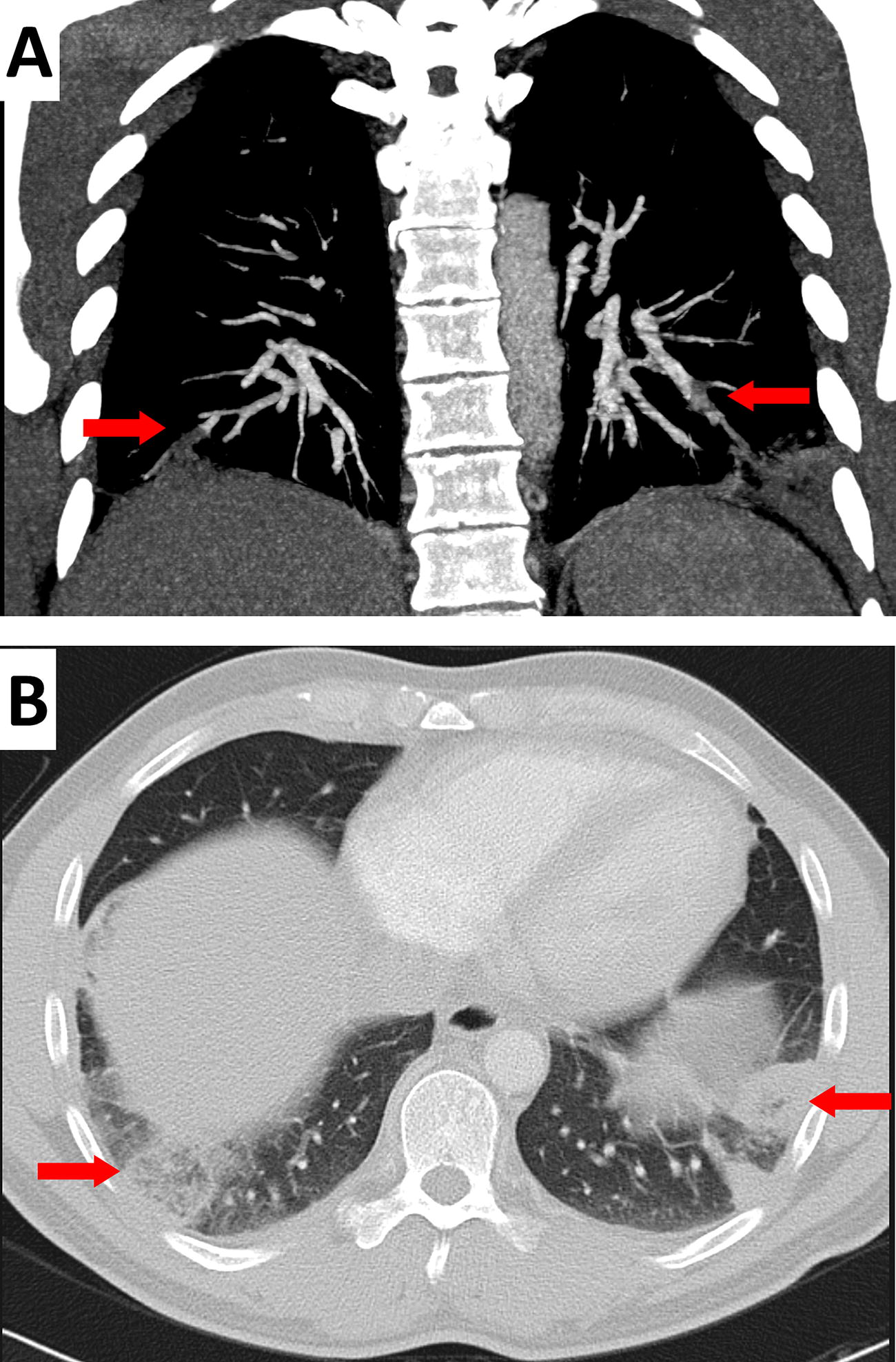
CT angiography images of a mountaineer upon second presentation of pulmonary embolism (PE), showing (arrows)
After the first PE, warfarin was recommended for 6 months. International normalized ratio was kept between 2 and 3. Within the 5 years between the two cases, the mountaineer participated in two expeditions; on both, he climbed to 7,000 m and had no venous thromboembolism (VTE). Genetic tests, performed after the second PE, revealed that the climber was heterozygous for factor V-Leiden mutation. Prolonged anticoagulation with dabigatran (150 mg b.i.d.) and withdrawal from high-altitude mountaineering were recommended. The climber limited his activity to trekking <5,500 m.
Discussion
High-altitude sojourn is speculated to be an independent risk factor for thrombosis (Trunk et al., 2019; Dutta et al., 2018). Specifically, the putative mechanisms of high-altitude VTE (HA-VTE) incorporate hypercoagulability owing to polycythemia, cold, and dehydration; hypoxia-induced upregulation of genes and proteins involved in platelet activation and thrombosis; and venous stasis caused by immobilization in tents (Trunk et al., 2019).
A risk stratification for HA-VTE includes altitude reached, length of stay, and mode of travel. Mountaineers seem to have the highest risk, therefore, as part of primary prophylaxis, they should avoid immobilization and dehydration and consider using graded compression stockings if tolerated.
There is high prevalence of some hereditary thrombophilias (HTs) and no pretravel screening is performed (Trunk et al., 2019). The analysis performed by Dutta et al. (2018) showed that HTs have a limited role in the etiology of PE at high attitude. On the contrary, there are case reports of HA-VTE in association with thrombophilias (Nair et al., 2008; Sandhu and Teves, 2018). As the impact of HT on the risk of HA-VTE is unclear, climbers with HT should not be disqualified from mountaineering. However, they should be aware of the potentially higher risk of HA-VTE, take nonpharmacological precautions, and follow general primary prophylaxis recommendations. Consideration should be given to equipping such mountaineers with direct-oral-anticoagulants (DOACs) to treat the acute phase of HA-VTE after on-site or online medical consultation.
The VTE recurrence rate for unprovoked VTE is 15.0% and 52.6% after 1 and 10 years, respectively (Prandoni et al., 2007). Although use of DOACs can reduce the VTE recurrence rate for unprovoked VTE to 2%, they increase the risk of major bleeding from 0.3% to 0.7% (Fernandes et al., 2019). However, as DOACs are superior than placebo for the combined outcome of fatal bleeding and fatal recurrence (Wu et al., 2015), extended prophylactic anticoagulation for all causes of VTE (except for surgical or trauma-related presentations) should be considered (Fernandes et al., 2019). DOACs at high altitude are recommended as a secondary prophylaxis for patients with the highest risk of HA-VTE, such as history of HA-VTE and HT, excluding those engaged in activities with a high risk of traumatic bleeding such as mountaineering (Trunk et al., 2019).
Taken together, this case and previous literature suggest that mountaineers with a history of high-altitude PE not taking prophylactic anticoagulants should avoid high-altitude mountaineering owing to the high risk of PE recurrence and the lack of medical help in remote areas. Those on DOACs should consider resigning from high-altitude mountaineering owing to a potential, although not scientifically proven, high risk of trauma-related bleeding.
The story of the described climber seems to indicate that he should have been advised to resign from mountaineering after his first high-altitude PE. However, scientific evidence is still insufficient to impose activity limitations on such mountaineers. It is certain that climbers with a history of HA-DVT or who are taking DOACs should be thoroughly informed by their consulting physicians about the risks of continuing high-altitude mountaineering. The combined effect of HT and high-altitude mountaineering on the risk of HA-VTE requires further research.
Patient Consent
The patient provided written consent for the publication of this report.
Footnotes
Authors’ Contributions
R.K.S. and M.S. equally contributed to acquisition of data and drafting of the article. M.J. contributed to interpretation and graphical presentation of radiological results.
Authors Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Medical University of Gdańsk (Excellence Initiative—Research University). The Medical University of Gdańsk financed the language correction.