
Abstract
Norberto, Matheus S., João Victor G. Torini, Matheus S. Firmino, and Marcelo Papoti. Validation of air storage system for hypoxia exposure during exercise. High Alt Med Biol. 00:000–000, 2024.—Considering the importance of optimizing normobaric hypoxia exposure (i.e., higher delivery capacity), the current study aims to validate a hypoxic air storage system. The study has a cross-over, one-blind randomized design. The air storage is composed of a piping system that directs hypoxic air from a hypoxia generator into nylon bags. Sixteen men (age, 25.4 ± 4.8 years; height, 174.9 ± 9.4 cm; weight, 77.1 ± 17.2 kg) performed three incremental treadmill tests until exhaustion on different days. For test–retest, the subjects repeated two tests in similar hypoxia conditions (H1 and H2; fraction of inspired O2 [FIO2] = ∼0.13; reliability analysis), and one time in normoxia (FIO2 = ∼0.20; condition comparison). Subjects’ performance, blood lactate concentration ([La−]), arterial oxygen saturation (SpO2), oxygen consumption (VO2), heart rate (HR), and several respiratory–derived variables were evaluated. A comparison was made between the rest, moderate intensity, and exhaustion stages. All variables were compared using the Friedman test with Durbin–Conover post hoc (p < 0.05). The hypoxia test–retest showed no statistical differences for any variable. Time analysis showed similar behavior for SpO2, HR, and cardiorespiratory variables (p < 0.01) for both conditions. The mean FIO2 at rest and during the incremental treadmill test was higher for normoxia (20.6 ± 0.2%) than for H1 (13.8 ± 0.8%) and H2 (13.7 ± 0.3%) (p < 0.001). The VO2 response was higher in normoxia than during hypoxia exposure at moderate intensity (Normoxia = 43.1 ± 8.1; H1 = 38.7 ± 5.7; H2 = 35.8 ± 8.8 ml.kg−1.min−1) and at the exhaustion stage (Normoxia = 52.7 ± 12.5; H1 = 41.9 ± 8.8; H2 = 40.5 ± 8.9 ml.kg−1.min−1) (p < 0.01). SpO2 and HR showed excellent intraclass correlation coefficient (ICC) during all moments, whereas VO2, SpO2, ratio between ventilation and CO2 production (VE/VCO2), ratio between oxygen consumption and ventilation (VE/VO2), and HR showed moderate or good ICC and coefficient of variation <9% during hypoxia test–retest exercises. Thus, the air storage system showed validity for its application and reliability in the measurements associated.
Introduction
The field of exercise physiology has significantly advanced in investigating the effects of altitude training as a physiological ergogenic approach (Marriott, 1994). Several models of altitude training equipment have become popular and have been incorporated into athletes’ exercise training routines aiming to improve performance (Christoulas et al., 2011; Millet et al., 2010; Sinex and Chapman, 2015).
Nonetheless, studies have shown that the normobaric hypoxia condition produced by hypoxia generators has become a “good option” for promoting similar physiological adaptations as hypobaric hypoxia (Coppel et al., 2015). Equipment such as hypoxia generators Colorado Altitude Training (CAT, USA) and Hypoxico Tent System (Hypoxico Altitude Training Systems, Germany), as well as techniques for adding nitrogen into the breathing air, have gained market share worldwide (Wilber, 2001).
However, there are some concerns regarding the normobaric hypoxia equipment. For instance, when exercising athypoxia conditions using hypoxic tents, the hypoxia generators (∼90 l/min) do not meet the demands of sedentary or active subjects during moderate exercise (ventilation >90 l/min), and also tents equipment may take up much space (Herdy and Uhlendorf, 2011), which is another important consideration.
Therefore, there is an emergence of new training models that need to be developed, such as inter-effort recovery hypoxia (de Carvalho et al., 2023; Papoti et al., 2023; Roels et al., 2005), which includes a system for quickly switching from normoxia to hypoxia air. We propose a new air storage system made up of “bags” containing a new air concentration that is connected to a system of pipes, to efficiently and compactly deliver hypoxia air to the subject at rest or during exercise. Thus, considering the low air rate production of hypoxia generators, the present study aims to validate a hypoxic air storage system for users engaging in exercise. It is expected that the air storage system will generate a hypoxic condition for the volunteers of the study at rest and during exercise.
Materials and Methods
Participants
Sixteen men (age, 25.4 ± 4.8 years; height, 174.9 ± 9.4 cm; and weight, 77.1 ± 17.2 kg) were recruited to participate in the study. The participants were physically active and engaged in different sports (i.e., weight training, ballet, soccer, running, handball, swimming, volleyball, soccer, and futsal) at least twice a week for 1 hour. All participants confirmed their participation in the research by reading and signing the informed consent form. This study was conducted in accordance with the Declaration of Helsinki (CAAE: 65263922.4.0000.5659).
Experimental design
The subjects were instructed to eat lightly in the last hour before the test. They completed a total of three visits. During one visit, subjects performed the incremental exercise test breathing normoxia air (FIO2: ∼0.20), while during the other two visits, they breathed air with identical hypoxia air concentration (FIO2: ∼0.13). The hypoxia condition was induced by the air provided by the hypoxia generator connected to the air storage system, which filled the bags only with hypoxia air. To provide normoxia air, a series of valves were shifted to allow the airflow, previously from the bags (hypoxia), to come from the environment (normoxia) (Fig.1). For the incremental exercise tests, participants wore a gas mask (Air Safety, Air San COD 524799, Brazil) connected to the air supply hose (Roseflex, 50 mm, Brazil).

An evaluation setup utilizing a hypoxia generator provided an air storage system. The participants underwent incremental tests on three different days. The tests were conducted twice in hypoxia and once in normoxia. The condition assignments were determined in a one-blind random experimentation.
The heart rate (HR), rate of perceived exertion (RPE), oxygen consumption (VO2), arterial saturation (SpO2), blood lactate concentration ([La−]), and respiratory-related variables such as ventilation (VE), ratio between ventilation and CO2 production (VE/VCO2), ratio between ventilation and O2 production (VE/VO2), respiratory quotient (RQ), end-tidal pressure of CO2 (PetCO2), and fraction of inspired O2 (FIO2) were monitored throughout the experiment. During 5 minutes of rest, all variables were collected to establish baseline values. At the beginning of the test, the participants performed the first stage at 7 km/h for 5 minutes as a warmup. At the end of the warmup period, the speed was increased by 1km/h for every 3 minutes of the tests. There were no cases of exhaustion with incomplete stages.
Air storage system
The air storage system composed of a 50 mm piping system that directs hypoxic air from a Colorado Altitude Training hypoxia generator (CAT-9 Air Unit-Everest Summit IITM) into four “bags” of 188 l made of very high oxygen holding material (i.e., Nylon resin fabric). The hypoxia generator airflow was ∼90 l/min. Each bag has two flanges at its extremity, an air inlet, and an air outlet. Fixed to the outlet flange, the piping system is also used to unify the airflow into a single outlet that passes through a valve system. The valve system was vertically disposed, the first valve controls the airflow from the environment to the supply hose (open/close the normoxia), the second valve controls the airflow from the bags to the supply hose (open/close the hypoxia), and the third valve controls the airflow fromthe bags to the environment (when in normoxia, this valve lets the bags airflow out, avoiding system overcapacity) (Fig. 2).
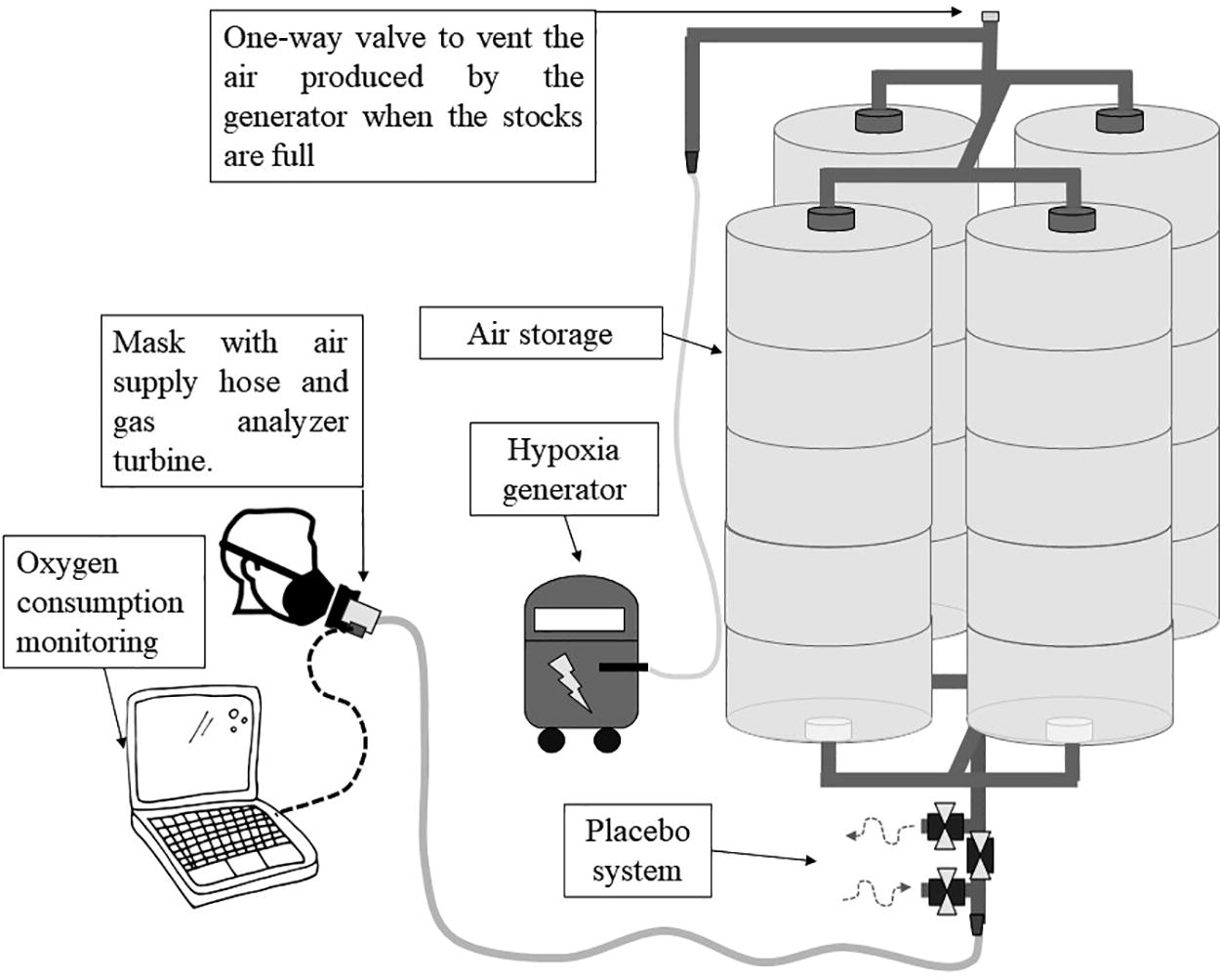
The experimental design used in this study consisted of a hypoxia generator connected to a piping system with four bags. The air outlet of the bags was unified into a single outlet that undergoes a system of three valves (placebo system). The valves can provide hypoxia or normoxia air (ambient air) to the subject’s supply hose. In normoxia, the valves block the air from storage and release excess air into the environment. In hypoxia, the air is directed from the bags to the supply hose. The subject’s mask was attached to the air supply hose and a turbine for gas analysis.
Oxygen consumption, blood lactate, and arterial blood saturation
To analyze the participants’ oxygen consumption, the supplied air flowed through a two-way nonrebreathing valve (Hans Rudolph), which directed the inspired air from the hose and the expired air to the environment. The gas analyzer turbine (Quark, Cosmed, Italy) was positioned between the adapter and the participants’ mask.
Blood samples (25 μL) were collected from the earlobe to determine blood lactate concentration ([La−]) before the first and after each stage. [La−] was determined using a blood analyzer YSI-2300 (Yellow Springs Instruments®, Ohio, USA). The SpO2 was monitored by a pulse oximeter (G-Tech Portable-Oled); the equipment was positioned on the distal phalanx of the participants.
Statistical analysis
A nonparametric Friedman test was used for group difference analysis with Durbin–Conover post hoc (p < 0.05) test. The analysis included variables at rest, at moderate intensity (5-point on RPE scale), and exhaustion stage (last completed stage). The reliability tests proposed by Hopkins (2000) and Weir (2005) used in these data included intraclass correlation coefficient (ICC), typical error (TE), coefficient of variation (CV%), standard error of the measure (SEM), and minimal difference needed to be considered real (MD). ICC was considered poor (<0.5), moderate (0.5–0.75), good (0.75–0.9), or excellent (>0.9) (Koo and Li, 2016).
Results
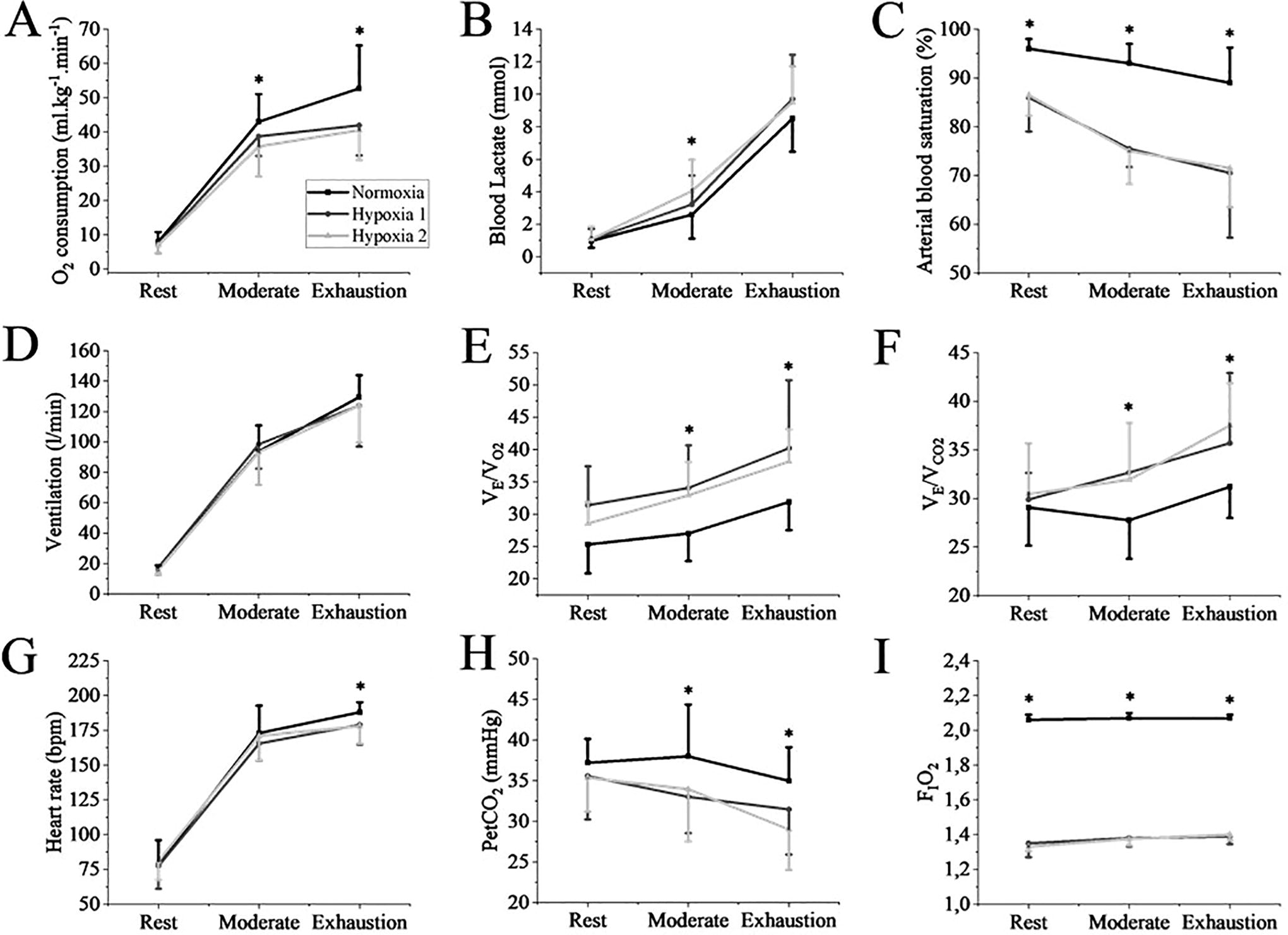
All three incremental exercise tests performed presented a continuous increase in VO2, VE, and HR during moderate intensity and exhaustion stages (p < 0.001). The SpO2 showed a slight reduction at moderate intensity (p < 0.001) at normoxia, which was maintained until exhaustion, and at hypoxia conditions, SpO2 showed a continuous decrease until the end of the test (p < 0.001). The [La−] and VE/VCO2 responses showed a continuous increase in all conditions (p < 0.01). VE/VO2 and PetCO2 (p < 0.01) showed similar reduction responses.
Both hypoxia incremental tests (test–retest hypoxia) showed no difference for any variable between them. VO2 was lower for both hypoxia conditions than for normoxia in moderate intensity (p = 0.002) and exhaustion stage (p < 0.001). Both hypoxia tests showed higher [La−] than normoxia at moderate intensity (p < 0.01). Both hypoxia tests showed lower SpO2 than normoxia in rest, moderate intensity, and exhaustion stage (p < 0.001). Both hypoxia tests exhibited higher VE/VO2 than normoxia at moderate intensity and exhaustion stage (p < 0.05). Both hypoxia tests demonstrated higher VE/VCO2 than normoxia at moderate intensity and exhaustion stage (p < 0.001). HR was lower for hypoxia tests than for normoxia at the exhaustion stage (p = 0.002). Both hypoxia tests showed lower PetCO2 than normoxia at moderate intensity (p = 0.025) and exhaustion stage (p = 0.012). FIO2 was lower for both hypoxia tests during rest, moderate intensity, and exhaustion stage compared with normoxia (p < 0.001).
The reliability tests applied on the test–retest hypoxia incremental exercise indicated moderate ICC for saturation (0.74) and HR (0.70) at rest. During moderate intensity, VO2, SpO2, VE, VE/VO2, and HR showed moderate ICC, and VE/VCO2 showed good ICC (0.80). In the exhaustion stage, VO2, VE/VO2, and HR showed moderate ICC, VE/VCO2 showed good ICC (0.79), and SpO2 showed excellent ICC (0.92). [La−] showed higher CV% in rest (21.1%), moderate intensity (19.2%), and in the exhaustion stage (15.2%). All the cardiorespiratory variables showed low CV% (<12%) at rest and moderate intensity. Although PetCO2 showed a higher CV% (20.2%), the cardiorespiratory variables showed low CV% in the exhaustion stage (<10%) (Table 2).
Discussion
The results of the present study indicated good validity for the air storage system, as it was accompanied by the expected reduction in FIO2, simulating hypoxia. In addition, good levels of reproducibility in several cardiorespiratory variables were also verified, indicating reliability regarding the use of the construct.
The present study found an expected behavior in the incremental exercise for the monitored variables, such as increased HR (Machado et al., 2013) and changes in ventilatory variables (Di Michele et al., 2009). However, it should be noted that some variables such as performance, VO2, HR, and SpO2 are affected differently when exercise is performed during hypoxia and normoxia conditions (Friedmann et al., 2004; Friedmann et al., 2005). The incremental exercise test performed under hypoxia condition drastically reduces SpO2 (Osawa et al., 2011), increases the [La−] at submaximal intensities with similar levels at high intensity (Lundby et al., 2000), and reduces the maximal VO2 reached (Ofner et al., 2014). Although it is known that reducing FIO2 directly affects SpO2 (Favier et al., 2015), the decrease in VO2 may be associated with reduced muscle oxygen delivery (Osawa et al., 2011), and the increased metabolic acidosis known as “lactate paradox” might be a compensatory response to respiratory alkalosis resulting from hypoxia (Cerretelli and Samaja, 2003).
PetCO2 and VE/VCO2, important variables in the medical field, when associated with an incremental exercise test, have the potential for monitoring the clinical condition of patients with pulmonary hypertension (Ross, 2003) and prevention of systemic sclerosis (Dumitrescu et al., 2010). Besides, the stabilization of PetCO2 during moderate intensity and its decrease during the exhaustion stage were similar in hypoxia and normoxia conditions (Table 1). This study also showed a difference in the absolute PetCO2 between the conditions (Fig. 3). Corroborating our findings, Subudhi et al. (2008) also found similar PetCO2 and VE/VCO2 behaviors associated with cerebral blood flow and reduced brain oxygenation. The authors suggest that the changes in these variables during high-intensity exercise may occur because of hypocapnic vasoconstriction associated with a respiratory compensation demand (increase in VE) that consequently reduces cerebral blood flow (Dalsgaard, 2006).
Difference between the three visits for VO2
Differences Between Rest, Moderate Intensity, and Exhaustion Stage for Cardiorespiratory and Physiologic Variables
FIO2, oxygen fraction inspired; HR, heart rate; PetCO2, end-tidal pressure of CO2; RQ, respiratory quotient; SpO2, arterial oxygen saturation; VE/VCO2, ratio between ventilation and carbon dioxide production; VE/VO2, ratio between oxygen consumption and ventilation; VO2, oxygen consumption.
Difference between moderate and exhaustion intensity (p < 0.01).
Difference for exhaustion intensity (p < 0.01).
Reliability Analysis of the Physiological and Cardiorespiratory Variables During Hypoxia Test–Retest
CV%, coefficient of variation; FIO2, oxygen fraction inspired; HR, heart rate; ICC, intraclass coefficient correlation; MD, minimal difference needed to be true; PetCO2, end-tidal pressure of CO2; RQ, respiratory quotient; SEM, stand error of measurement; SpO2, arterial oxygen saturation; TE, typical error; VE/VCO2, ratio between ventilation and carbon dioxide production; VE/VO2, ratio between oxygen consumption and ventilation; VO2, oxygen consumption.
Moderate index.
Good index.
Excellent index.
Although there were no statistical differences for ventilation, participants exhibited mean ventilation of ∼100 l/min at moderate intensity and ∼125 l/min at high exercise intensity during the incremental exercise test. This oxygen consumption level would not be adequately met without the addition of an air storage system, considering the airflow of the hypoxia generator (90 l/min). The prototype presented here includes four bags with a capacity to store 188 l of oxygen, totaling 752 l. Despite all subjects completing the incremental exercise tests without emptying the air storage system in this format, there is the possibility of including more air bags. Adding more bags to the system would ensure that subjects can perform longer training sessions.
Despite a hypoxia storage/delivery system recently utilized on patients with spinal injury (Tan et al., 2020), the present study was the first, to the best of our knowledge, to present the validity and reliability of a hypoxic air storage system. The SpO2 and FIO2 were variables that showed statistical differences when comparing normoxia and hypoxia conditions. This result confirms the effectiveness of the hypoxic air storage system in delivering hypoxia air to the subjects. Furthermore, the air storage system showed good reliability for most variables investigated, highlighting SpO2 and HR, often used for medical evaluation, cardiovascular tests, and training monitoring.
It is also important to consider that the hypoxic condition is not the only factor that impacts performance during exercise. The participants’ status on the test day (i.e., stress, feeding, sleep) may alter physiological (Halson, 2008) and hormonal responses (Kim et al., 2015), directly impacting the CV%, which, despite being near 6% for several variables, remained high for [La−] and PetCO2 in all moments. Similar to the present study, Sirotic and Coutts (2008) also evidenced VO2 and HR with high ICC and low CV%, whereas [La−] showed moderate ICC values with high CV%.
Although ICC and CV% provide a relative reproducibility index, SEM and TE provide an absolute index, quantifying the accuracy of the individual score in the tests, without being affected by within-subjects variability (Hopkins, 2000; Weir, 2005). In this sense, our SEM and TE analyses highlighted the lower variations in the hypoxia air storage system. It is also important to notice that, even with the highest CV% and ICC of PetCO2 and [La−], they showed a good absolute index of reliability since SEM and TE are presented in the same unit as the variables (Weir, 2005). Considering the importance of detecting real differences and noise, our study also presented the MD as representing an additional absolute index for detecting “true” modifications (Weir, 2005).
We concluded that the hypoxia air storage system is suitable for storing hypoxic air, enabling the simulation of hypoxic environments. Furthermore, several variables presented acceptable ICC, TE, SEM, and CV when associated with exercise.
Footnotes
Acknowledgment
The authors are grateful to the aquatic activities’ lab, partners, and volunteers. The authors would also like to thank Mrs. Margarida and Mr. Edson who were responsible for building the construct.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the São Paulo Research Foundation under Grant no. 2021/02403-1.
IRB Approval
All experiments were previously approved by the local Ethics Committee (Process number: 79144017.7.0000.5659) and conducted following the Declaration of Helsinki.