
Abstract
Ebert-Santos, Christine, and Ana Campos. Ileus at altitude. High Alt Med Biol. 25:342–344, 2024.–Autoimmune myasthenia gravis (MG) is a condition commonly caused by the production of antibodies that block acetylcholine receptors. Until recently, gastrointestinal (GI) symptoms were considered rare in myasthenia gravis, but are now being proposed as an early identification tool. Presented here is a case study that exemplifies GI symptoms in MG, exacerbated by low barometric pressure at altitude. This illustrates the need to identify GI symptoms earlier in MG patients, as well as the need for providers at high altitude to be aware of these manifestations of MG.
Case Narrative
Autoimmune myasthenia gravis (MG) is a condition commonly caused by the production of antibodies that block acetylcholine receptors. This blockade of neuromuscular signaling results in rapid muscular fatigue and weakness. Increased activity tends to worsen muscular issues, which usually resolve with rest. Prominent symptoms of MG include drooping eyelids, double vision—OMG (ocular myasthenia gravis)—difficulty swallowing, slurred speech, and shortness of breath. Muscles in the face and throat are the most impacted by myasthenia gravis. Myasthenia can affect any muscle group throughout the body (UK NHS, 2020). Gastrointestinal (GI) manifestations such as abdominal pain, vomiting, and constipation have been reported by individuals with MG. A case presented to the Summit Medical Center at 9,100 feet illustrating an unusually severe manifestation.
A 70-year-old woman came to the emergency department (ED) with severe abdominal and chest pain, concerned that she had a dissecting aortic aneurysm. She reported three previous episodes of severe pain in the 2 weeks leading up to the ED visit, all starting in the afternoon, increasing to prostration by 5 pm and resolving with bed rest. Past medical history was significant for myasthenia gravis treated with azathioprine 100 mg BID (twice daily). Two months previously she had a flare with ptosis and double vision, treated with prednisone 40 mg daily.
Vital signs: pulse 63; respiration rate 24; blood pressure 149/81; temperature 36.2°C; oxygen saturation 94. Laboratory results: complete blood count showing white blood cell count 7.4; hematocrit 43.4; mean crepuscular volume 100; red cell distribution width 57.2 (normal range 37.1–48.9); venous lactate 0.7; and aspartate aminotransferase 68. Troponin was 10 upon admission, and 9 upon discharge. Abnormalities in the comprehensive metabolic panel: alanine transaminase of 131 (49 two months later), lipase 165 (60 two months later). The electrocardiogram reading was normal. Medications administered in the ED included morphine (4 mg IV; 2 mg IV); GI cocktail (AL-MG-OH/Lidocaine-2:1 45 ml oral); and iohexol (omnipaque) 350 mg iodine/ml injection 100 ml IV.
Computed tomography scan (Figure 1): Marked gaseous distention of the colon with increased fecal material. Upstream nondependent gaseous distention of the small bowel. This could indicate the presence of an ileus. A focal region of bowel obstruction was not seen. Abdominal radiograph (Figure 2) also showed distended loops of bowel.
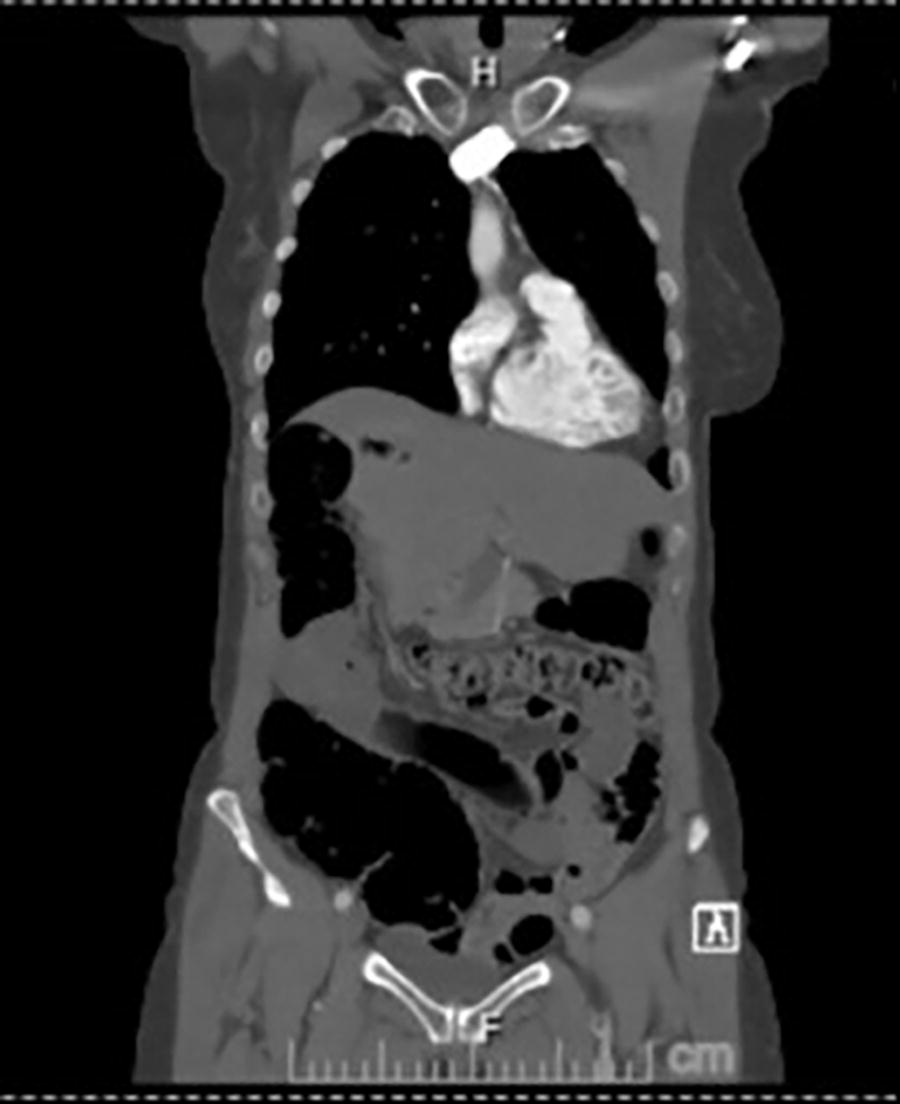
CT scan of patient with intestines diffusely distended with bowel gas.

X-ray of patient with intestines diffusely distended with bowel gas.
In summary, laboratory tests were normal except as noted above. Imaging showed distended loops of bowel consistent with ileus. She was treated with pain medication and the symptoms resolved. The patient continued to have episodes once or twice a month, including another ED visit, precipitated by treatment with Duoneb, containing ipratropium bromide, a tonic water drink, and guaifenesin, all antimuscarinic substances that interact with the cholinergic receptors in the viscera. Taking pyridostigmine 60 mg, a cholinesterase inhibitor, led to resolution within 2 hours, marked by “sparkly” sensations in her arms and legs and reactivation of bowel sounds with flatus. Subsequently she had several severe episodes of ileus requiring larger doses of pyridostigmine, up to 180 mg while using dulaglutide injections for weight loss.
Until recently, GI symptoms were considered rare in myasthenia gravis. In 2001, a case study demonstrated that gastric dysmotility was a common feature among individuals with myasthenia gravis (Vernino et al., 2001). Among all the motility dysfunction reported, gastroparesis was found to be a common autonomic feature in MG patients (Vernino et al., 2001). Gastroparesis is the slowing or stopping of movement in the GI tract resulting in delayed gastric emptying. Further research demonstrated that intestinal pseudo-obstruction was one of the most common GI manifestations of individuals with MG (Pande and Leis, 1999; Musthafa et al., 2006; Seretis et al., 2012).
In 2007, it was demonstrated that receptors in gut muscles were structurally like skeletal muscle receptors, indicating that GI motility could be impacted by the presence or lack of acetylcholine (Mandl and Kiss, 2007). Considering that antibody production in myasthenia gravis individuals can decrease acetylcholine binding to receptors, the presence of GI symptoms among other autonomic dysfunction symptoms suggests inadequate treatment (Auliya, 2021).
What was previously considered a rare symptom within a rare condition is now being proposed as an early identification tool. Considering receptor similarity, GI symptoms can be used as an early sign of myasthenia gravis, specifically gastrointestinal dysmotility (Alnajjar et al., 2023). The case study showed that MG developed less than a decade after the initial onset of GI dysmotility symptoms (Alnajjar et al., 2023). There is a clear need to identify GI symptoms earlier in MG individuals. This will allow for better treatment and improved long-term health outcomes for these individuals.
At altitude, the low barometric pressure causes gaseous distension in normal individuals producing increased flatus (Auerbach and Miller, 1981). Combined with MG, GI manifestations can be even more severe. Medical providers treating residents of high-altitude communities should consider MG in the differential of patients with abdominal complaints and treat recognized MG patients with anticholinesterase medications to control symptoms. None of this patient’s providers were aware of this manifestation of MG, including the neurologist who specializes in MG, the gastroenterologist who performed an upper endoscopy and colonoscopy, the ED staff, the radiologist, and the primary care provider. Patients with MG and their providers need to be aware of medications that interact with the cholinergic receptors in all parts of the body and screen for these as possible precipitators of symptoms outside the classic description of the disease.
Footnotes
Acknowledgments
The authors would like to thank Leah Gentner, B.A., for her help preparing this case report.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.