
Abstract
Foster, Katharine, James D. Anholm, Gary Foster, Suman Thapamagar, and Prajan Subedi. Effects of naltrexone on sleep quality and periodic breathing at high altitude. High Alt Med Biol. 26:13–19, 2025.
Objective:
This study examined the effects of naltrexone on breathing and sleep at high altitude. Mu-opioid receptor (MOR) agonists have a depressive effect on respiration. Naltrexone is known to block the MOR. We hypothesized that MOR blockade with naltrexone would result in higher nocturnal oxygen saturations, fewer apneas, and improved sleep at high altitude.
Methods:
This double-blind, placebo-controlled, crossover study included nine healthy volunteers (four females, five males) aged 27.9 (4.6) (mean [standard deviation]) years. Two overnight trips spaced at least 2 weeks apart took participants from Loma Linda, CA (355 m) to the Barcroft Laboratory, CA (3,810 m) for each arm. Participants ingested either 50 mg naltrexone or matching placebo at bedtime. Sleep metrics were recorded using an ambulatory physiological sleep monitor (APSM). Subjective data were measured with the Groningen Sleep Quality Scale, Stanford Sleepiness Scale, and the 2018 Lake Louise Score (LLS) for acute mountain sickness (AMS).
Results:
Mean overnight SpO2 was lower after taking naltrexone, 81% (6) versus 83% (4) (mean difference 1.9% [2.1, 95% confidence interval or CI = 0.1–3.6, p = 0.040]). The lowest overnight SpO2 (nadir) was lower on naltrexone 70% (6) versus 74% (4) (dif. 4.6% [4.3], CI = 1.0–8.2, p = 0.020). Total sleep time and total apnea–hypopnea index were unchanged. Subjective sleep quality was significantly worse on naltrexone measured via the Groningen Sleep Quality Scale (p = 0.033) and Stanford Sleepiness Scale (p = 0.038). AMS measured via LLS was significantly worse while taking naltrexone (p = 0.025).
Conclusion:
Contrary to our hypothesis, this study demonstrated a significant decrease in nocturnal oxygen saturation, worse sleep quality, and AMS scores. Further characterization of the MOR’s effects on sleep and AMS is needed to evaluate potential exacerbating mechanisms for AMS and poor sleep quality at altitude.
Introduction
Rapid ascent to high altitude produces a spectrum of pathologies including acute mountain sickness (AMS), high-altitude cerebral edema (HACE), and high-altitude pulmonary edema (HAPE) in unacclimatized, otherwise healthy individuals (Luks et al., 2021). The risk of developing altitude illness relates to the rapidity of ascent and the final altitude reached (Luks et al., 2021). Ventilatory response is one of many components contributing to acclimatization, and the lowest oxygen saturations for a trip to altitude are commonly recorded during sleep. Poor sleep quality at altitude is common, and most individuals ascending above 2,500–3,000 m report trouble sleeping (Reite et al., 1975; Zieliński et al., 2000). The causes are multifactorial and include the direct effect of hypoxia, central periodic breathing (PB), and frequent nocturnal arousals (Ainslie et al., 2013; Anholm et al., 1992; Khoo et al., 1996; Patrician et al., 2024).
The mechanisms underlying the control of breathing while awake and during sleep are complex with numerous neuronal interactions throughout the brain, brain stem, and chemoreceptors (both central and peripheral) (Dempsey and Forster 1982; Dempsey et al., 2010; Mahamed and Duffin 2001; Paula-Ribeiro and Rocha 2016; Robbins 2001; Smith et al., 2015). Opioid receptors are divided into four main classes: mu (μ), kappa (κ), dopamine (δ), and nociception/orphanin (Pattinson 2008).
High concentrations of opioid receptors are found in the respiratory center of the brain stem and cause respiratory depression in response to opioid receptor agonists. Naloxone and naltrexone are opioid receptor antagonists (ORAs) with high affinity for the mu receptor and are used in the reversal of opioid overdose and treatment of alcohol addiction. Both have a high affinity for the mu receptor and cause competitive inhibition of mu receptor agonists. Naloxone is formulated as an intravenous and intranasal solution, has a half-life of 30 minutes, and is used for overdose reversal (Jordan and Morrisonponce 2024). Naltrexone is available as an oral pill or intramuscular injection, and because of its longer half-life of ∼4–14 hours, it is used preventatively in the treatment of alcohol addiction (Sudakin 2016). The mu receptor is also bound by endogenous compounds, enkephalins, and beta-endorphins, which act as agonists. Naloxone and naltrexone block the natural analgesic effects of these endogenous compounds. Beta-endorphin binding to the mu receptor is associated with exercise-induced analgesia and the repression of substance P; however, the role of beta-endorphins in the modulation of respiration is not completely understood (Chen et al., 2018; Da Silva Santos and Galdino 2018; Trescot et al., 2008).
Sea level studies on the respiratory effects of beta-endorphins show conflicting results. In 1985, Chada, Birch, and Sackner concluded that hypoxia-induced PB was blunted by pretreatment with naloxone (Chadha et al., 1985). The same year, Steinbrook et al. concluded that plasma beta-endorphin levels were not significantly altered by naloxone (Steinbrook et al., 1985).
Earlier studies conducted on the effects of naloxone or naltrexone during either hypoxia or at high altitude have been assessed during periods of exercise (Koglin and Kayser 2013; Strassman et al., 1989). Studies on the effects of naltrexone on sleep quality and pulse oximetry are limited to low altitude and show significant differences in opiate-naive versus opiate-tolerant individuals (Ferber et al., 1993; Sramek et al., 2014; Staedt et al., 1996). The effect of mu-ORA on respiratory depression and sleep-disordered breathing in healthy participants at high altitude is unknown. The present study investigates the effect of ORA via naltrexone administration on sleep quality and oxygenation. We hypothesized that ORA would result in higher nocturnal oxygen saturations, fewer apneic periods, and unchanged subjective sleep quality.
Methods
Ethical approval
Ethical approval was obtained from the VA Loma Linda Healthcare System Institutional Review Board. The study conformed to the Declaration of Helsinki and was registered in Clinicaltrials.gov (NCT05037032). All volunteers signed a written informed consent document before any study procedures.
Participants
In this small pilot study, we aimed to recruit 10–15 individuals. Study volunteers were recruited through word of mouth in the local community. Only nonsmoking volunteers aged 18–35 years with body mass index (BMI) < 27 kg/m2 (average BMI was 20.7 [range 18.3–23.1]) with no history of sleep apnea, sleep-disordered breathing, or other cardiopulmonary disease were included. Other exclusion criteria were a history of alcohol abuse; use of any benzodiazepine or opioid substance (prescribed or otherwise) within 2 weeks of study enrollment; any medications that might, in the opinion of the investigators, interfere with or alter respiratory control (e.g., acetazolamide); and recent (within 3 weeks) exposure to altitudes ≥ 3,500 m. A total of 16 volunteers were recruited and signed the written informed consent; five of these volunteers did not meet inclusion criteria on further review because of medication use, and two additional volunteers only completed one trip to altitude before dropping out because of AMS symptoms. Nine healthy participants (mean age of 27.3[4.6] years, four females, five males) completed all arms of the study.
Study design
This study was designed as a randomized, double-blind, placebo-controlled crossover study conducted in three phases as illustrated in Figure 1. Low-altitude overnight baseline sleep studies were performed at ∼370 m altitude using APSM devices (WatchPAT® device, Itamar Medical Ltd.) to exclude volunteers with marked sleep-disordered breathing. The mean (standard deviation [SD]) baseline apnea–hypopnea index (AHI) was 2.37 (1.98) events per hour, ranging from 0.2 in one individual to 6.6 in another individual.
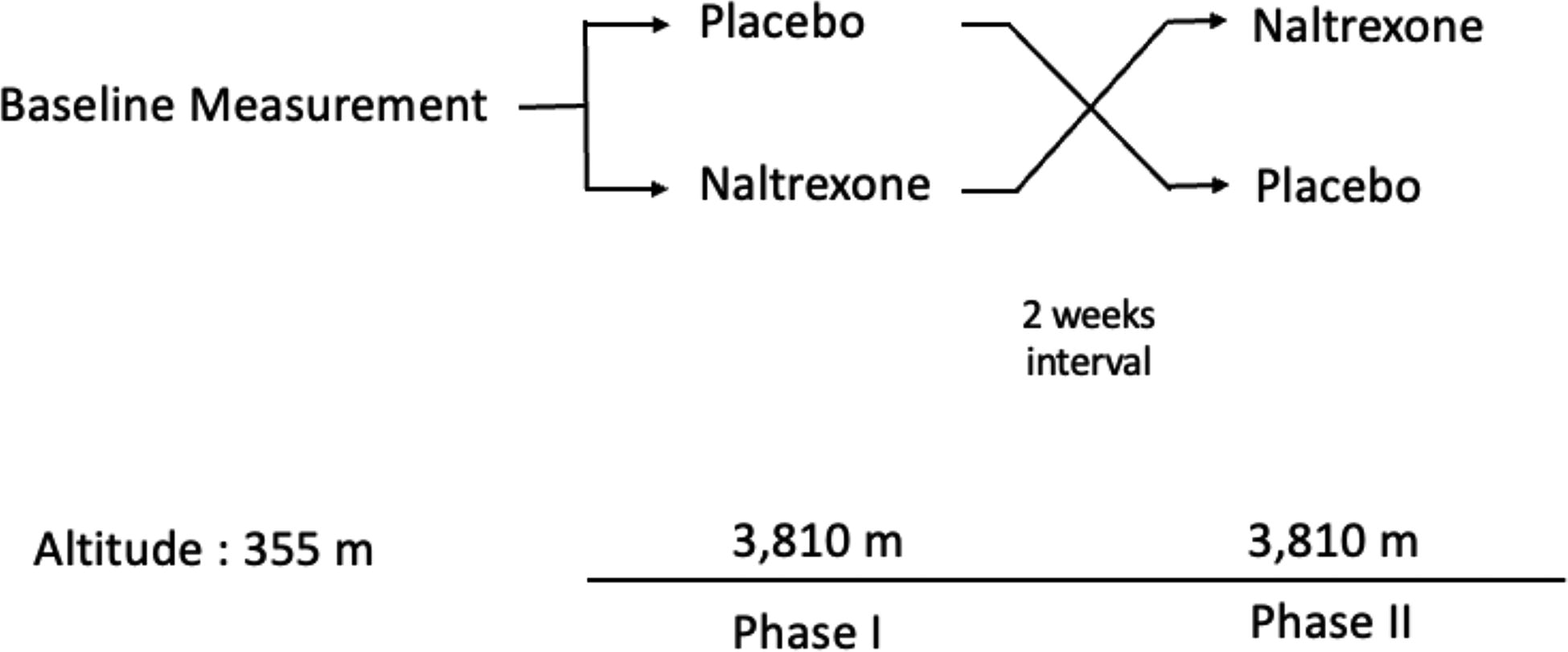
Study flow diagram showing both arms of the randomized crossover design.
Study volunteers were randomized to either naltrexone first or placebo first with the alternate medication/placebo given on the second trip to altitude. The groups were balanced with respect to the number of participants receiving naltrexone on their first or second trip. Study volunteers were driven from an estimated altitude of 370 m to the Barcroft/Nello Pace Laboratory, White Mountain Research Station, CA, at 3,810 m elevation. The drive took 5 hours with the majority of elevation gain occurring in the last 1 hour. Participants arrived between 7 and 8 pm on each trip. Two hours after arrival, study volunteers received their blinded pill and filled out the Stanford Sleepiness Scale (Hoddes et al., 1973) as well as the Groningen Sleep Quality Scale (Jafarian et al., 2008).
After completing the questionnaires, participants were instrumented with an APSM device and slept according to their normal sleep schedule. After natural awakening, morning oxygen saturation was measured by pulse oximetry (Masimo Rad-57®, Masimo Corp.), and the second set of the previously described questionnaires was completed along with the Lake Louise AMS score (Roach et al., 2018). After a washout period of a minimum of 2 weeks, study volunteers participated in another overnight sleep study at the Barcroft/Nello Pace Laboratory on the alternate medication (either placebo or naltrexone).
Intervention
Volunteers were randomized using a computer-generated block randomization schedule to receive either a 50 mg naltrexone pill or matching placebo (corn starch capsule). Fifty milligrams is the approved dose of naltrexone for alcohol addiction treatment and is the dose routinely used for both men and women without dose adjustments (Sudakin 2016). Participants received the alternate therapy on their second trip. The research pharmacist placed the doses in identical containers, and all doses were taken as a group at 10 pm on both trips.
Sleep data collection
Ambulatory physiological sleep monitoring devices were used to record nocturnal oxygen saturation and sleep variables. These devices were donned before each subject sleeping and were removed upon natural morning arousal. The APSM device monitors and measures variations in peripheral arterial tone (PAT) via an opto-pneumatic finger-mounted probe. These devices using PAT show strong agreement with full polysomnography (Van Pee et al., 2022). Additional recorded channels include pulse rate, oximetry, actigraphy, body position, chest motion, and snore sensor. Sleep/wake detection is based upon actigraphy data, and sleep staging is thereafter based upon variability in pulse rate, attenuation and variability of PAT amplitude, and inter-pulse period features. The PAT (AHI) and PAT respiratory disturbance index (RDI) are number of events per hour of sleep and are estimates of conventional AHI and RDI values produced by polysomnography. The AHI is calculated using the number of oxygen desaturation events ≥3% per hour of technically valid sleep time. Similarly, the oxygen desaturation index (ODI, 3%) is calculated using the number of ≥3% oxygen desaturations per hour of sleep time.
Self-reported data
Study volunteers completed questionnaires upon arrival to the Barcroft/Nello Pace Laboratory, before sleep, as well as in the morning upon waking. The evening questionnaires included the Lake Louise Score (LLS) for measuring AMS symptoms and the Stanford Sleepiness Scale. The morning questionnaires included the Groningen Sleep Quality Scale (Jafarian et al., 2008; Meijman et al., 1988), the Stanford Sleepiness Scale (Hoddes et al., 1973), and the LLS for measuring AMS symptoms. For the Groningen Sleep Quality Scale, scores range from 0 to 14, with higher scores indicating worse subjective sleep quality. The Stanford Sleepiness Scale is a self-reported score between 1 and 7 with higher numbers indicating increased sleepiness. AMS was scored using 2018 version of the LLS, which does not evaluate sleep. The LLS requires a score of at least 3, in the presence of headache score of at least 1, to indicate AMS. AMS score of 3–5 points was considered mild AMS, 6–9 points moderate AMS, and 10–12 points severe AMS (Roach et al., 2018).
Statistical analysis
Statistical analysis was performed using Microsoft Excel version 16.16.27 and R version 4.2.2. The Shapiro–Wilk test was performed to test for normality. Normally distributed data were analyzed by paired t-test and reported as mean (SD), and non-normal data were analyzed by Wilcoxon signed-rank test and reported as median and interquartile range. All comparisons were two-sided. A p value ≤0.05 was considered significant.
Results
At altitude, the mean overnight oxygen saturation was lower while taking naltrexone than on placebo (p = 0.040) (Table 1). The lowest overnight oxygen saturation was also significantly lower on naltrexone when compared with placebo (p = 0.020) (Table 1, Fig. 2). The mean saturation during desaturation nadirs on naltrexone was 77.9% (5.2) versus 80.1% (3.6) on placebo (mean difference 2.2% [2.1], 95% confidence interval or CI: 0.5–4.0, p = 0.018). No statistically significant difference was found in the total number of oxygen desaturations, the ODI, or the AHI (p = 0.846, 0.250, 0.134, respectively).
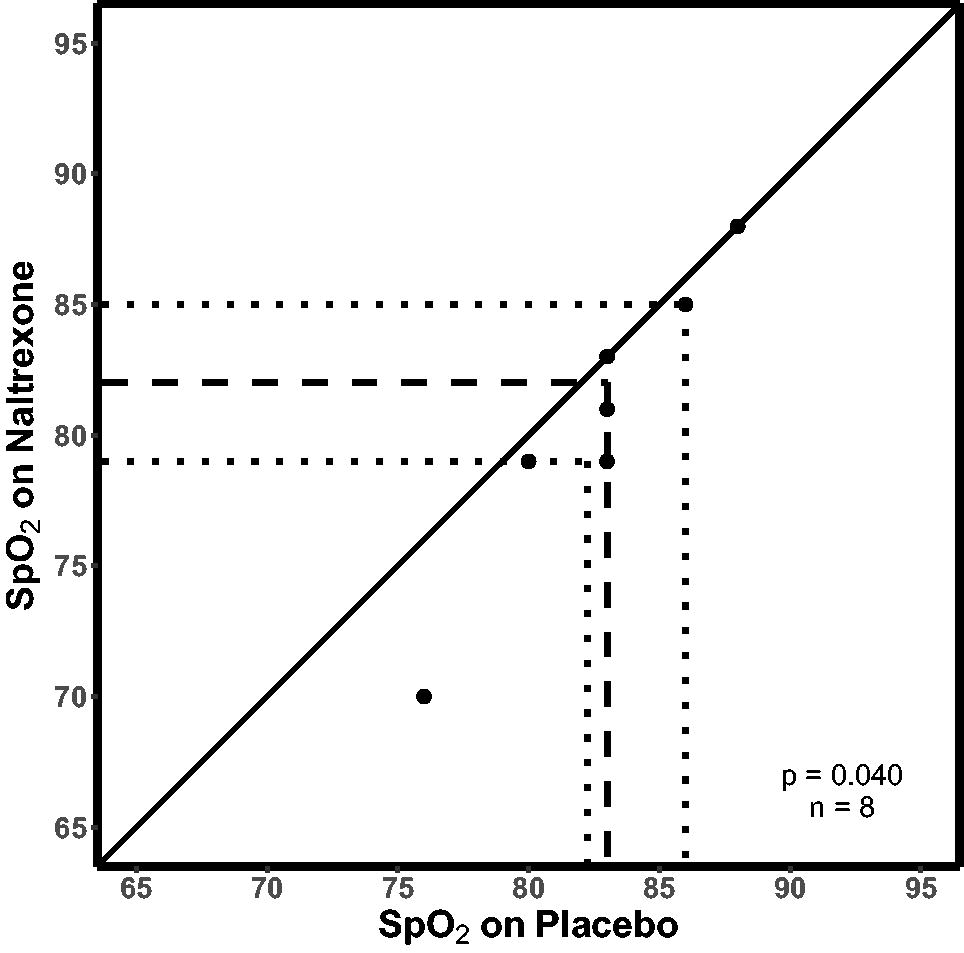
Mean nighttime SpO2 while taking naltrexone is plotted against values while taking placebo. The solid diagonal line is the line of identity. The dashed line shows the median value, whereas the dotted lines show the first and third quartiles. p-Value is from a two-sided paired t-test comparison.
Summary of Sleep and Subjective Results
Number of volunteers included in each paired comparison is shown in brackets. LLS for acute mountain sickness. Units for the Groningen, LLS, and Stanford Sleepiness Scales are arbitrary units. Paired t-tests were used unless noted otherwise, for example, “Wilcoxon” for Wilcoxon signed-rank test.
CI, confidence interval; IQR, interquartile range; LLS, Lake Louise Score; ODI, oxygen desaturation index; pAHI, apnea-hypopnea index based on PAT; pRDI, respiratory disturbance index based on PAT.
Bolded p-values indicate p-values less than 0.05.
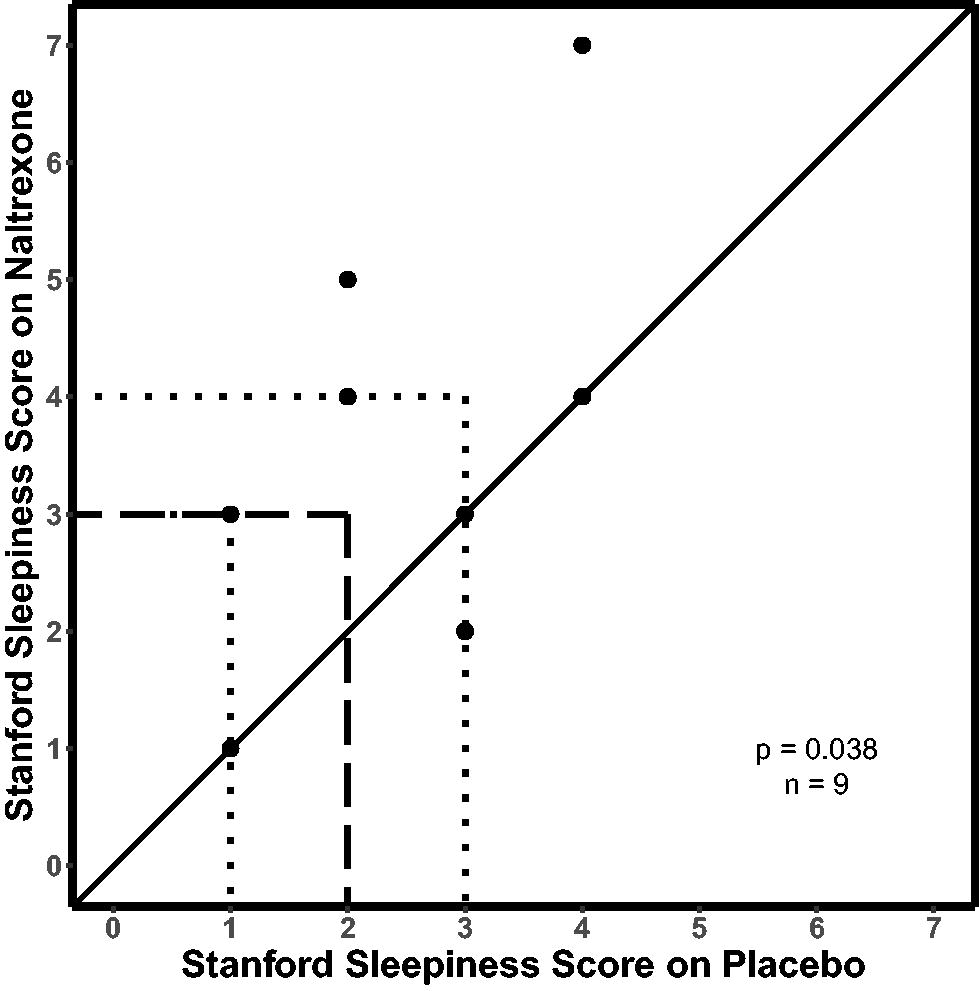
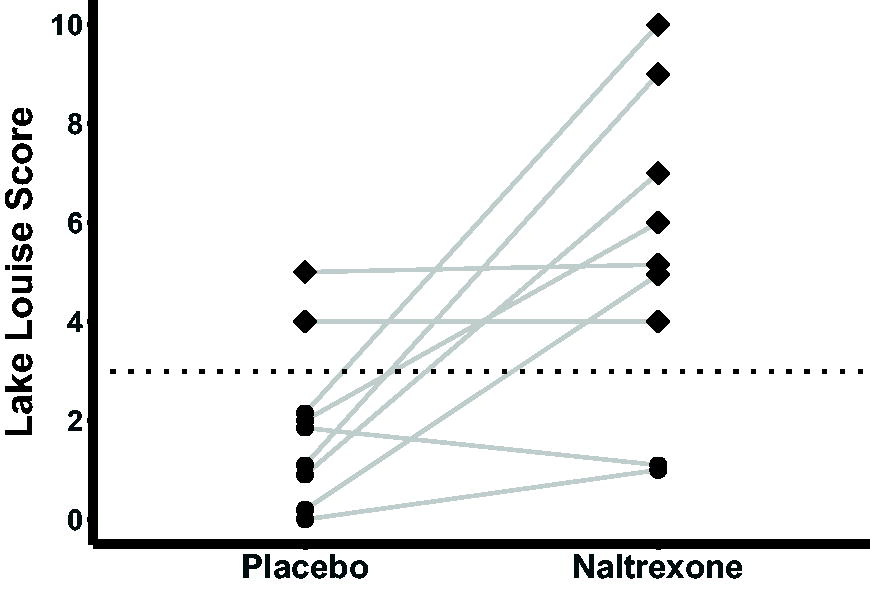
Subjective sleep quality was significantly worse on naltrexone measured via the Groningen Sleep Quality Scale (Fig. 3) and Stanford Sleepiness Scale (Fig. 4). The 2018 LLS, which does not consider sleep, was significantly worse on naltrexone (Fig. 5), with seven out of nine individuals reporting AMS while taking naltrexone. Only two of these same volunteers experienced AMS while taking placebo, with symptoms and scores consistent with mild AMS. While on naltrexone, AMS was mild in three volunteers, moderate in three, and severe in one individual (Fig. 5).
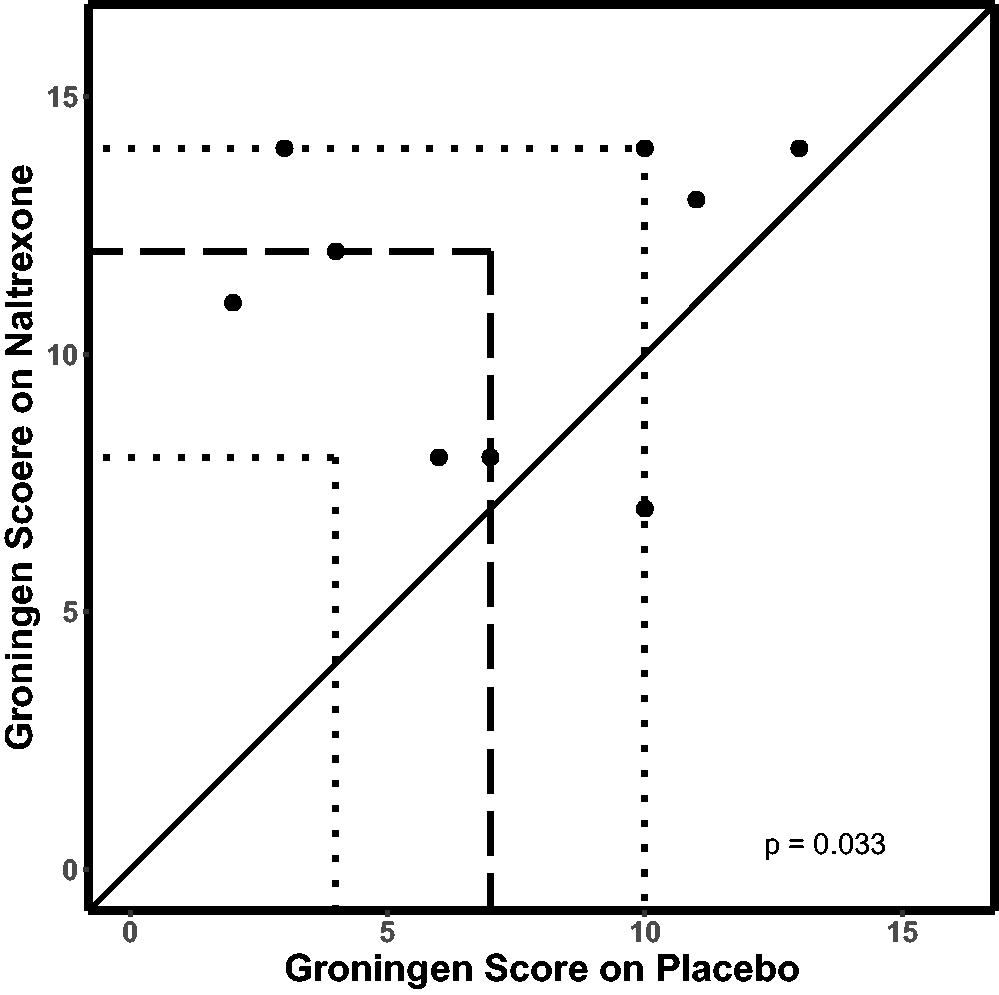
Groningen Sleep Quality Scale scores on naltrexone versus when taking placebo. The solid diagonal line shows the line of identity. The dashed line represents the median values, and the dotted lines show the first and third quartiles. Higher scores while taking naltrexone indicate worse subjective sleep quality by paired t-test (n = 9, p = 0.033).
Lake Louise AMS scores while taking a placebo and in the same individuals after taking naltrexone. The dotted line at a score of 3 when combined with headache score ≥1 is the cutoff for AMS versus no AMS. Filled circles show individuals without AMS, whereas diamonds represent individuals with AMS. AMS scores were significantly higher on naltrexone by Wilcoxon signed-rank test (p = 0.025). AMS, acute mountain sickness.
Stanford Sleepiness Scale while taking naltrexone versus while taking placebo. The solid diagonal line shows the line of identity. The dashed line represents the median values, and the dotted lines show the first and third quartiles. Higher scores indicate increased sleepiness (n = 9); however, two points lie on top of one another with naltrexone scores of 3 and placebo scores of 1. p = 0.038 by two-sided paired t-test.
Although limited by the sample size, we attempted to determine whether taking naltrexone on the first trip to altitude altered any findings compared with those who took placebo first. No effect was observed except in the percentage of deep sleep where naltrexone appeared to worsen deep sleep more in those taking naltrexone on their first trip (p = 0.045). Likewise, we attempted to evaluate the effects of gender on outcomes, but no significant effect was found.
Discussion
Contrary to our initial hypotheses, this study demonstrated three main findings: (1) significantly decreased mean overnight oxygen saturation after taking naltrexone, (2) worsened overnight subjective sleep quality with naltrexone compared with placebo at high altitude, and (3) significantly increased AMS scores while taking naltrexone. To our knowledge, this is the first study to test physiological effects of mu-receptor blockade on humans during sleep at high altitude and the subjective effect this has on sleep quality.
PB
PB consists of a series of three to six breaths with waxing and waning tidal volume followed by a short apneic period (Cheyne–Stokes breathing pattern). Mechanisms causing PB are complex. A loop gain phenomenon has been described (Khoo et al., 1982), in which increased respiratory gain coupled with relatively delayed chemoreceptor response sets up a cyclic pattern. Perturbations in the normal respiratory cycle such as a breath with larger than normal tidal volume or a change in sleep state can also induce PB. Changes in the hypoxic ventilatory response affect the amount of PB in different individual volunteers and different populations (Burgess et al., 2008; Lahiri et al., 1983; Lahiri et al., 1984). Changes in cerebral blood flow also influence the amount of PB in healthy individuals (Burgess et al., 2018).
Our study intended to evaluate the effect of mu-receptor antagonism in ventilatory response to altitude. Earlier studies on the effect of endogenous compounds that bind opioid receptors and their effect on ventilation have been inconclusive and methodologically confounding.
In a 1985 sea level experiment, Chada, Birch, and Sackner concluded that hypoxia-induced PB was blunted with naloxone (Chadha et al., 1985). The same year, Steinbrook et al. concluded that plasma beta-endorphin levels were not altered by naloxone administration (Steinbrook et al., 1985). In 1993, a study on individuals with obstructive sleep apnea found that naltrexone decreased the number of hypoxic and hypercapnic events and improved blood–gas patterns (Ferber et al., 1993). In our study, a clear relationship between PB and mu-receptor blockade was not observed. PB was recorded in all participants at high altitude. Response to naltrexone was split with approximately half of volunteers experiencing fewer total desaturations and half experiencing increased desaturations with naltrexone. The variation in number of desaturation events in study volunteers varied widely, ranging from 40 to 652 events on placebo and from 4 to 581 events on naltrexone. When standardized by hours of sleep, the range remained wide (5–61 and 4–107 events on placebo and naltrexone, respectively). This variation within our sample indicates significant heterogeneity in the ventilatory response to altitude in healthy individuals and would be better investigated by a larger sample size and subgroup analysis.
Oxygenation
We hypothesized that naltrexone use would be associated with higher mean oxygen saturations. In contrast, the opposite was found. Naltrexone use was associated with decreased mean and minimum overnight oxygen saturations as well as a lower mean saturation during desaturation nadirs (a lower average saturation during the lowest saturation periods). Although the reason for this finding is unclear, one possible mechanism may be found in an effect of naltrexone on vascular tone. To our knowledge, there have been no high-altitude studies on this interaction. In one feline model at sea level, naloxone inhibited morphine-induced pulmonary vasodilation (Kaye et al., 2008). Other studies discussed in the next section have shown additional vasoactive effects of naloxone and naltrexone. These actions have the potential to worsen existing pulmonary arteriolar hypertension, contributing to worsened respiratory status. However, these mechanisms are speculatory and would require further investigation into the effects of the mu receptor on pulmonary vascular reactivity.
AMS
AMS is notoriously difficult to quantify given the subjective and nonspecific nature of symptoms. Notably, the symptoms of AMS share similarities with the symptoms of precipitated opiate withdrawal. Both are characterized by headache, dizziness, nausea, and vomiting. Naltrexone typically only induces these symptoms in individuals who have opiates in their system and has minimal effect on individuals without current opiate intoxication. In our study, a significant increase in AMS symptoms was found in participants taking naltrexone. Seven out of nine participants experienced increased AMS symptoms while taking naltrexone. Four of these seven experienced moderate or severe AMS with headache, nausea, vomiting, and dizziness on naltrexone. These four participants received standard treatment for altitude illness (oxygen, acetazolamide, and/or dexamethasone). One was evacuated to a lower altitude with rapid recovery on descent. This response was particularly striking to researchers as similar sea level studies have shown no clinically significant side effects after naltrexone administration (Sramek et al., 2014), and this response to naltrexone has not been previously reported outside of precipitated withdrawal in opiate-addicted, intoxicated individuals. Although the etiology of this response is unclear, rapid resolution of symptoms in one subject with decent to lower elevation and a similar sea level study without any clinical findings after naltrexone administration make the mechanism less likely to be an isolated side effect of naltrexone (Sramek et al., 2014). The similarities between AMS and precipitated withdrawal not only complexify the interpretation of our observed findings but also raise the question of whether endogenous mu-receptor agonists may play a role in symptomatology of AMS.
The opioid receptor system has wide-reaching effects, including catecholamine regulation under stress, the regulation of cerebral blood flow, vasogenic edema, and cerebral glutamate release. Arterial epinephrine has been shown to be elevated in volunteers with AMS compared with individuals at the same altitude without AMS symptoms (Kamimori et al., 2009), whereas increased arterial epinephrine concentrations have been demonstrated in healthy volunteers on naltrexone in response to cold pressor test when compared with placebo (Kotlyar et al., 2008). Further studies on the catecholamine response to stress in individuals at altitude would be needed to investigate this speculation. Other conjectures include a potential role for the vasoactive effects of opioid receptors in the cerebral vasculature. Notably, morphine administration decreased vasogenic edema in rats through decreased release of nitric oxide and decreased glutamate release (Whiteside et al., 2005). Similarly, morphine and other opiates are known to have effects on intracranial pressure (Wiener et al., 2019), and alterations in the regulation of this homeostasis can result in symptomatology and could be responsible for the AMS findings in our study. Future studies investigating the role of opioid receptor regulation of catecholamines and intracranial pressure at altitude are needed.
Sleep quality
In our sample, participants reported significantly worse sleep on naltrexone measured via two separate scoring systems. The few studies assessing the effects of naltrexone on sleep at low altitudes show differing results depending on whether the volunteers were opiate naive or opiate addicts (Ferber et al., 1993; Sramek et al., 2014; Staedt et al., 1996). In healthy individuals not addicted to opiates, only subclinical sleep disturbances, predominantly rapid eye movement duration, were noted (Sramek et al., 2014). In our sample, lower oxygen saturation in the naltrexone group likely contributed to higher AMS symptoms and poor sleep quality. To our knowledge, this is the first sleep study to investigate the role of mu-receptor antagonism at altitude. Further study of individual sleep parameters with a larger sample size is needed to establish the mechanism and significance of our findings.
Limitations
Although the double-blind, crossover design of this study allowed each study subject to serve as their own control, it is still limited by its small sample size. Difficulties were encountered in recruiting study volunteers who met inclusion criteria without any centrally acting medication use (most significantly encountered were medications for the treatment of depression and attention deficit hyperactivity disorder), which significantly limited the sample size. This also highlights the difficulties in generalization of these findings given the extensive exclusion criteria and high population levels of substance or centrally acting medication use. The large variance in the number of apneic periods raises the question of whether individual factors in the function of the mu receptor may account for some of the difference. Participants with a history of prior opioid addiction or treatment using naltrexone were excluded from the study because of the documented differences in naltrexone response from individuals with a history of opioid addiction and opiate-naive individuals (Sramek et al., 2014); however, history of prescribed opiate use outside of diagnosed addiction was not used as exclusion criteria, which could explain some of the variance between individuals. Furthermore, a urine drug screen was not performed that further limits this analysis.
Owing to the small sample size, assessment for possible sex/gender effects is limited. Our analysis did not find any significant differences.
The data were analyzed for order effect, and while this analysis did not show any order effect (except for percentage of deep sleep), there remains the possibility of an order effect. Naltrexone and its metabolite 6β-naltrexol have a commonly cited terminal half-life of ∼4–14 hours, which is supported by recent studies and review articles (Krieter et al., 2019; Sudakin 2016; U.S. Food and Drug Administration 2013; Yancey-Wrona et al., 2011). However, one study from 1976 of four patients cites an estimated terminal half-life of 96 hours for naltrexone and 18 hours for 6β-naltrexol (Verebey et al., 1976). This discrepancy has not been discussed in further journal publications to our knowledge. As such, it is possible there may have been some remaining effects of naltrexone on those participants even 2 weeks later when they made their second trip to altitude.
Conclusion
This study demonstrated significant findings that did not support the hypothesis that mu-receptor blockade would result in higher nocturnal oxygen saturation, fewer apneic periods, and resultant improved subjective sleep quality. Conversely, naltrexone resulted in a significant decrease in overnight mean and minimum oxygen saturations, worse subjective sleep experience, and worse AMS scores. The mechanisms responsible for these findings are unclear. Further studies on the effects of naltrexone on intracranial pressure (ICP) and ventilatory response at low and high altitudes are warranted.
Footnotes
Acknowledgments
We would like to thank all the participants without whom we could not have completed the study. We also would like to thank Aimee D Rodriguez, RCP-RRT for administrative support and writing assistance and Lien Duong, PharmD for pharmacy support. Portions of this manuscript were presented at the International Hypoxia Symposium in Feb. 2023, Lake Louise, AB, Canada.
Portions of this manuscript were presented at the International Hypoxia Symposium in Feb. 2023, Lake Louise, AB, Canada.
Authors’ Contributions
Conception and design of the study: K.F., J.D.A., G.F., and P.S. Acquisition, analysis, or interpretation of the data: K.F., J.D.A., G.F., S.T., and P.S. Drafting the article and critical revision of the article: K.F., J.D.A., G.F., S.T., and P.S. In addition, all authors have approved the final version of the article, and all authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors qualify for authorship and all those who qualify for authorship are listed.
Author Disclosure Statement
The authors declare no conflicts of interest regarding the content of this article.
Funding Information
This material is the result of work supported with resources and the use of facilities at the VA Loma Linda Healthcare System. The contents of this article do not represent the views of the VA or the United States government.