
Abstract
Horiuchi, Masahiro, and Samuel J. Oliver. Post-exercise hypotension after exercising in hypoxia with and without tart cherry supplementation. High Alt Med Biol. 26:63–69, 2025.
Background:
This study investigated the effects of hypoxic exercise with and without tart cherry (TC) supplementation on post-exercise hypotension (PEH).
Method:
In a randomized order, 12 healthy young adults (9 men and 3 women) completed cycle exercise to exhaustion (1) in normoxia without any supplementation (Norm), (2) in hypoxia (13% O2) with placebo (Hypo), and (3) in hypoxia with TC supplementation (Hypo + TC). Supplements were supplied for 5 days pre-trial (TC was 200 mg anthocyanin per day for 4 days and 100 mg on day 5).
Results:
Cycle exercise total energy expenditure was greater in Norm than Hypo and Hypo + TC (p < 0.001) with no difference between Hypo and Hypo + TC (p = 0.41). Mean arterial pressure (MAP) decreased during recovery in all trials (main effect of time, p < 0.001), with no difference in PEH between the trials (p > 0.05, change [Δ] in MAP from pre-exercise at 60 minutes recovery, mean difference, Norm Δ-4.4 mmHg, Hypo Δ-6.1 mmHg, and Hypo + TC Δ-5.2 mmHg). Cardiac baroreflex sensitivity decreased during recovery in all trials (p < 0.001) and was lower in Hypo than Norm and Hypo + TC (main effect of trial, p = 0.02).
Conclusion:
PEH was not increased after exercise in hypoxia, with or without TC supplementation, compared with exercise in normoxia.
Introduction
Arterial blood pressure (BP) is reduced for up to 24 hours following a single session of physical exercise; a phenomenon called post-exercise hypotension (PEH) (Halliwill et al., 2014). It is clinically important to investigate factors that enhance PEH as the magnitude of PEH after acute exercise relates to the beneficial BP-lowering effects of exercise training (Kleinnibbelink et al., 2020). While various factors such as exercise mode, intensity, duration, and environmental temperature may influence PEH, few studies have investigated the effect of hypoxia on PEH (Halliwill et al., 2014; Horiuchi and Oliver, 2023). PEH follows a decrease in peripheral vascular resistance (Brito et al., 2014), and as hypoxia enhances vasodilation (Joyner and Casey, 2014), greater PEH may be anticipated after exercising in hypoxia than normoxia, which has been confirmed in some (Horiuchi et al., 2018; Horiuchi et al., 2016a; Saito et al., 2019) but not all previous studies (Fornasiero et al., 2021; Horiuchi et al., 2022; Kleinnibbelink et al., 2020). BP may not be reduced after exercise in hypoxia due to an attenuation of baroreflex sensitivity (BRS) and a shift in cardiac autonomic function to sympathetic activity (Bourdillon et al., 2023; Halliwill et al., 2014).
Tart cherries, and other dark-colored berries, are rich in antioxidants and polyphenols including anthocyanins (Keane et al., 2016). In normoxic conditions, anthocyanin-rich supplements have been shown to increase peripheral artery diameter and blood flow (Barnes et al., 2020; Cook et al., 2023; Matsumoto et al., 2005), and reduce peripheral vascular resistance (Barnes et al., 2020), which precedes PEH (Halliwill et al., 2014). Moreover, a recent study in normoxia reported a larger decrease in post-exercise systolic blood pressure (SBP) but not diastolic or mean arterial pressure (MAP), following 7 days of an anthocyanin-rich supplement compared with a placebo (Shan and Cook, 2023). These vascular effects may be mediated by polyphenols and circulating metabolites’ improving nitric oxide bioavailability (Bell and Gochenaur, 2006; Xu et al., 2004) and reducing oxidative stress, which is elevated post-exercise and in hypoxic environments. PEH may also be expected to be greater after hypoxic exercise and anthocyanin-rich supplementation compared with normoxic or hypoxic exercise alone, as antioxidant supplementation has previously been shown to restore the imbalance of cardiac autonomic nervous activity, as assessed by heart rate variability (HRV) in humans (Weggen et al., 2021), and improve BRS in rats (Alves et al., 2015; Garcia et al., 2017).
Accordingly, this study investigated the effects of tart cherry (TC) supplementation on PEH after exercising in hypoxia. We hypothesized that the magnitude of PEH would be greater in hypoxia compared with normoxia, and PEH would be further accentuated with TC supplementation.
Methods
Participants
The present report presents additional recovery and normoxia data from previously published investigations that examined TC supplementation effects on hypoxic exercise performance (Horiuchi et al., 2023). This study was approved by the Ethical Committee of Mount Fuji Research Institute in Japan and was performed following the Declaration of Helsinki guidelines (No. 202001). Of the 13 participants in the previous study, 12 (9 men and 3 women) performed an additional normoxic exercise and recovery experimental trial. The participants’ age, height, and body mass were 21 ± 1 years, 169 ± 7 cm, and 62.1 ± 8.9 kg, respectively (values are mean ± standard deviation [SD]). All participants were non-smokers, had no history of cardiovascular disease, and had not been exposed to an altitude higher than 1,500 m in 6 months before the study.
Study design
This study consisted of three trials (Fig. 1): (1) normobaric normoxic exercise without any supplementation (Norm), (2) normobaric hypoxic exercise (13% O2) with a placebo (Hypo), and (3) normobaric hypoxic exercise (13% O2) with TC supplementation (Hypo + TC). In a double-blinded and randomized manner, each participant ingested a placebo or TC capsule (TC 1,200 mg containing 100 mg of anthocyanin; Nature’s Life, Orem, UT, USA) twice per day for 4 days before the experimental trial, and once on the day of the experimental trial 2 hours before beginning excise, which is consistent with studies reporting hemodynamic changes after single doses and 4–7 days of anthocyanin-rich supplementation (Matsumoto et al., 2005). Participants were provided a list of antioxidant-rich foods and instructed to avoid these while in the study.
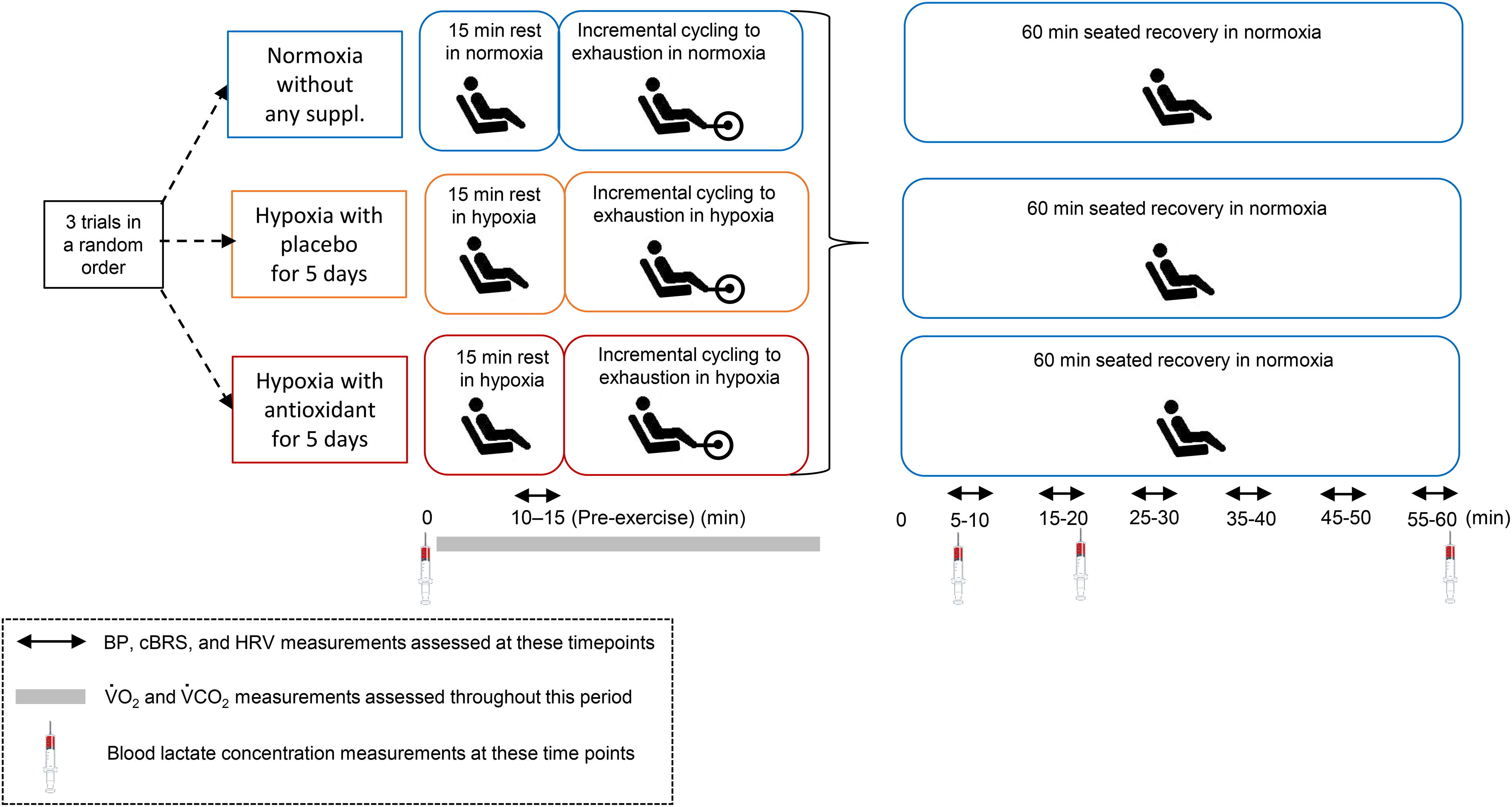
Experimental procedure. BP, blood pressure; cBRS, cardiac baroreflex sensitivity; HRV, heart rate variability; suppl., supplementation; VCO2, carbon dioxide output; VO2, oxygen uptake.
Experimental procedure
The exercise was performed on a cycle ergometer (COMBI232-C; COMBI, Japan) in an environmental chamber (24°C, 50% relative humidity; TBR-4, 5SA2GX; Tabai Espec Co. Ltd., Tokyo, Japan). After a 15-minute semi-recumbent rest, participants performed incremental leg cycling exercise to exhaustion, consisting of three 4-minutes incremental stages (40–80–120 Watts [W] for men, and 30–60–90 W for women, with each stage lasting 3 minutes), followed by an increase in the workload of 20 W (men) or 10 W (women) per min until exhaustion. The pedal cadence was set at 60 rpm using a metronome. After exhaustion, the participants sat semi-recumbent for 60 minutes in normoxia in all trials.
Measurements
At rest and during exercise, pulmonary oxygen uptake (VO2) and carbon dioxide output (VCO2) were measured by a metabolic cart (AE-310S; Minato Medical Science, Osaka, Japan) and beat-by-beat BP was measured using finger photoplethysmography at the middle or index finger (MUB-101; Medisens Inc., Tokyo, Japan) as the time-averaged from the beat-by-beat pressure wave (Horiuchi et al., 2016b). Beat-by-beat BP data were stored with a sampling frequency of 200 Hz by a field data recorder (es8; TEAC, Tokyo, Japan), and transferred to a laptop computer for further analysis. Based on a previous study (Horiuchi and Thijssen, 2020), heart rate (HR) was measured using a portable HR monitor (Check-My-Heart; TRYTECH Co., Ltd., Tokyo, Japan), and HRV was calculated by accompanying HRV analysis software. Participants were instructed to breathe normally throughout testing. Fingertip blood samples (0.3 µl) were taken to measure blood lactate concentration (Lactate Pro 2LT-1730; Arkray, Tokyo, Japan) pre-exercise, 5, 20, and 60 minutes of recovery. Total urine samples were collected pre-exercise and 1hour post-exercise and analyzed for urinary 8-hydro-2’-deoxyguanosine (8-OHdG), an index of oxidative DNA damage, as described previously (Horiuchi et al., 2023).
Data analysis
To calculate spontaneous cardiac BRS (cBRS), the beat-to-beat SBP time series and RR interval were analyzed for more than three consecutive beats, with increasing or falling direction from a 5-minute steady-state data segment at rest and during recovery (Carrington and White, 2001; Horiuchi and Oliver, 2023; Ogoh et al., 2005). Linear regression was applied to each baroreflex sequence, with only sequences with an R2 >0.85 accepted (Horiuchi and Oliver, 2023; Iellamo et al., 1994). The overall average slope of the SBP–RR interval was calculated as spontaneous cBRS. Time domain HRV was calculated by the SD of the normal-to-normal intervals (SDNN) and the root-mean-square of successive differences in R-R interval (RMSSD). In the frequency domain, the extent of very low-frequency (LF) oscillations (0.0033–0.04 Hz), LF oscillations (0.04–0.15 Hz), and high-frequency oscillations (HF: 0.15–0.4 Hz) were quantified using a fast Fourier transformation (Horiuchi and Thijssen, 2020). Total exercise energy expenditure (EE) was calculated using VO2 and VCO2 as follows: total EE (J/s) = (3.869 × VO2) + (1.195 × VCO2) × 4.168/60 × 1,000, where the unit of VO2 and VCO2 were liter per minute (Horiuchi et al., 2017).
Statistics
Data are presented as mean ± SD. Statistical analyses were performed using commercial software (Jamovi, 3.2.3). One-way repeated measures analysis of variance (ANOVA) compared the total EE across the three trials, and changes in urinary 8OHdG excretion. A two-way (time × trials) repeated ANOVA compared time course changes in all physiological variables (BPs, HR, HRV, and blood lactate). For further comparisons, Tukey’s post hoc test was used. The effect size was calculated as η2, defined as small (η2 = 0.01), medium (η2 = 0.06), and large (η2 = 0.14) (Lakens, 2013). Statistical significance was set at p < 0.05. The normality of the data was examined using the Bartlett and Levene test. If equal variance failed, logarithmic transformation data were used for further analysis (HF and LF/HF).
Results
Cycle exercise total EE was detected to be different between the trials (F = 34.5, p < 0.001, η2 = 0.21), where total exercise EE in Norm (846 ± 189 J/s) was greater than Hypo (672 ± 125 J/s) and Hypo + TC (692 ± 153 J/s) (p < 0.001, respectively), with no differences detected between Hypo and Hypo + TC (p = 0.41).
During the 60 minutes recovery, an interaction effect was found for MAP (F = 1.86, p = 0.045, η2 = 0.013) but not for SBP and diastolic BP (DBP) (Fig. 2). MAP decreased in all trials (main effect of time, F = 14.51, p < 0.001, η2 = 0.15), with no difference detected in PEH between trials (p > 0.05, change [Δ] in MAP from pre-exercise at 60 minutes recovery, mean difference [95% confidence interval], Norm Δ-4.4 [–6.0, –2.8] mmHg, Hypo Δ-6.0 [–8.5, –3.7] mmHg, and Hypo + TC Δ-5.2 [–8.8, –1.6] mmHg) (Fig. 2A).

cBRS was reduced during recovery compared with pre-exercise (main effect of time, F = 59.55, p < 0.001, η2 = 0.62). Moreover, a main effect of trial was detected (F = 4.45, p = 0.02, η2 = 0.02), where overall cBRS was lower in Hypo than Norm (p = 0.03) and Hypo + TC (p = 0.06), with no difference between Norm and Hypo + TC (p = 0.74) (Fig. 3A). No trial or time effects were detected for HR. An interaction was detected for HR due to higher resting HR on Hypo and Hypo + TC than Norm (F = 2.29, p = 0.01, η2 = 0.01) (Fig. 3B). There was no interaction or/and trial effects in blood lactate (Fig. 3C). For HRV metrics, no interactions or main effects of time were detected. However, regardless of the trial, cardiac parasympathetic activity indices (SDNN, RMSDD, log [HF]) were lower, and cardiac sympathetic activity index (log [LF/HF]) was higher during recovery compared with pre-exercise (Table 1). At 1 hour post-exercise, changes in urinary 8-OHdG excretion from pre-exercise were 5.2 ± 4.4 in Norm, 5.3 ± 3.1 in Hypo, and 3.4 ± 2.7 ng kg-1h-1 in Hypo + TC, with a trend for a smaller increase in 8-OHdG excretion on Hypo + TC than Hypo (p = 0.08).

Cardiac Autonomic Function During 60 Minutes Recovery After Exercise in Normoxia (Norm), Exercise in Hypoxia with Placebo (Hypo), and Exercise in Hypoxia with Tart cherry (Hypo+TC)
Values are mean ± standard deviation.
a.u., arbitrary unit; HF, high frequency; LF, low frequency; RMSSD, root-mean-square of successive differences in R-R interval; SDNN, standard deviation of the normal-to-normal intervals; TC, tart cherry.
Discussion
Our study showed that incremental leg cycling until exhaustion leads to reductions in MAP of 4–6 mmHg after exercise in untrained men, supporting the presence of PEH. These findings confirm the results of previous studies showing PEH after various exercise intensities, durations, and types (Jones et al., 2021; Marcal et al., 2021; Pimenta et al., 2019). In contrast to our hypothesis, PEH was not increased after exercise in hypoxia, with or without TC supplementation, compared with exercise in normoxia. One possible explanation is the exercise was performed until exhaustion, which resulted in greater exercise EE and absolute work in Norm than Hypo or Hypo + TC. This is consistent with a recent study that revealed the magnitude of PEH was not different between normoxia and hypoxia when the absolute work of exercise was matched (Fornasiero et al., 2021). These findings have good ecological validity as those exercising in hypoxic conditions normally reduce workload due to increased perception of effort (Rossetti et al., 2017).
TC supplementation before exercise in hypoxia did not further accentuate PEH compared with exercise in hypoxia alone. These unique findings build upon the limited research in normoxia to examine the effect of anthocyanin-rich supplementation on PEH (Shan and Cook, 2023). Consistent with this previous study, we reported no difference in MAP or DBP post-exercise after placebo and anthocyanin-rich supplementation. In contrast, we did not observe a larger decrease in post-exercise SBP, which may be explained by the different types (TC vs. New Zealand blackcurrant) and dose of anthocyanin-rich supplementation (7 vs. 4 days, and 210 vs. 100 mg anthocyanin on the final day).
In the present study, HRV indices during recovery indicated a shift in cardiac autonomic balance compared with pre-exercise, i.e., increased cardiac sympathetic activity and decreased cardiac parasympathetic activity; however, these indices were not influenced by hypoxia or TC supplementation. cBRS was lowest during recovery after exercise in Hypo, which is consistent with previous research indicating hypoxia lowers cBRS (Bourdillon et al., 2023). cBRS was similar during recovery in Hypo + TC to Norm, suggesting TC supplementation restored cBRS, lowered by exercise in hypoxia. One possible explanation is oxidative stress tended to be lower after hypoxic exercise with TC supplementation compared with a placebo. This explanation is supported by animal research reporting improvements in BRS after antioxidant supplementation (Alves et al., 2015; Garcia et al., 2017). Improvements in oxidative stress and cBRS sensitivity with TC supplementation at the same time as similar magnitude of PEH in all trials suggest a limited regulatory role of oral antioxidants and cBRS in PEH. Previous research has also shown the intravenous infusion of antioxidants did not influence PEH (Romero et al., 2015). Therefore, non-antioxidant mechanisms, like increased NO bioavailability, may explain the greater reductions in post-exercise BP observed after consuming anthocyanin-rich supplements (Shan and Cook, 2023).
Conclusion
PEH was not increased after exercise in hypoxia, with or without TC supplementation, compared with exercise in normoxia.
Footnotes
Acknowledgments
The authors appreciate the time and effort spent by their volunteer participants. They would like to thank Miss Misato Watanabe for her technical assistance.
Authors’ Contributions
The conception of the study design (M.H. and S.J.O.), performing the experiments (M.H.), analyzing the data and interpretation of the results (M.H. and S.J.O.), drafting of the first article (M.H.), revising the article (M.H. and S.J.O.), and approval of the final article (M.H. and S.J.O.).
Author Disclosure Statement
The authors declare no conflict of interest related with this study.
Funding Information
This study was supported in part by the Japan Society for the Promotion of Science (JSPS, KAKENHI, Numbers;