
Abstract
Lankford, Harvey V., and Hannah Kimberley. Supplemental oxygen on the Annie Smith Peck Expedition of 1903 to 6,367 m (20,892 ft) Mount Sorata (Illampu). High Alt Med Biol. 26:227–235, 2025.—The 1903 expedition to 6,367 m (20,892 ft) Mount Sorata (Illampu) in Bolivia that was conceived, organized, and led by American mountaineer Annie Smith Peck appears to have been the first to take a supplemental oxygen apparatus to a great mountain. The expedition did not have heavy cylinders of compressed oxygen or closed-circuit rebreathers with chemically generated oxygen but took an apparatus to produce oxygen on the mountain apparently by a 19th century heated chlorate chemical method. Oxygen was to be manufactured in camp, stored in rubber bags, and used with an open-circuit breathing set while climbing. The equipment was taken, but once in Bolivia, a late change in plans resulted in a summit attempt on 6,427 m (21,086 ft) Ancohuma rather than Illampu on the twin-peaked Sorata massif. The summit attempt ended prematurely at 4,700 m (15,350 ft), and the oxygen system was not used. The present paper reviews some of the supplemental oxygen options that were available in 1903 and examines the Sorata expedition, a little-known part of the early history of mountaineering oxygen use.
Introduction
The 1903 Annie Smith Peck Mt. Sorata (Illampu) expedition in Bolivia is an unfamiliar part of the history of supplemental oxygen use for mountaineering. This story unfolded decades prior to the 1953 British Everest expedition that used compressed oxygen to reach the summit. The Sorata expedition did not have any of the systems of compressed oxygen in cylinders or closed-circuit rebreathers with chemically generated oxygen. Instead, the expedition took equipment to produce oxygen in camp very likely by the 19th century method of heating potassium chlorate and storing it in rubber bags for use while climbing. Early steps in the use of supplemental oxygen for climbing were sometimes limited, untested, unsuccessful, or unfulfilled. The expedition to 6,367 m (20,892 ft) Sorata (also known as Illampu) on the twin-peaked Sorata massif was changed once in Bolivia to an attempt on 6,427 m (21,086 ft) Ancohuma rather than Illampu. The attempt ended unexpectedly at 4,700 m (15,350 ft), but this paper will nonetheless explore this portion of the history of supplemental oxygen use in early 20th-century mountaineering.
Oxygen was discovered in the 1770s, but it was not until the next decade that French chemist Antoine Lavoisier (1743–1794) correctly interpreted its role in cellular respiration. In 1820, the Russian Joseph Hamel (1788–1862) may have been the first person to suggest the use of supplemental oxygen at high altitude. He intended to use compressed oxygen while attempting 4,804 m (15,774 ft) Mont Blanc, but the equipment was not suitable (Simons and Oelz, 2001). The modern era of understanding oxygen physiology is attributed to French physiologist Paul Bert (1833–1886), whose barometric chamber studies showed that low partial pressure of oxygen produced physiological impairment with alleviation by supplemental oxygen (Bert, 1878). During the late 1800s, advances were slowly made in breathing equipment for ballooning, mining, diving, and other irrespirable atmospheres. In the 20th century, mountaineers would learn about the benefits of supplemental oxygen on climbing rate, stamina, cognition, warmth, and more.
Annie Smith Peck and Mt. Sorata
Annie Smith Peck (1850–1935) of Providence, Rhode Island was an accomplished classics scholar. She was among the first female undergraduates at the University of Michigan, where she also earned her master’s degree. Peck became the first woman to attend the American School of Classical Studies in Athens, Greece. She taught Latin at Purdue University and was an author, suffragist, international lecturer, mountain climber, founding member of the American Alpine Club and adventurer. When asked where her home was, she replied, “Where my trunk is” (Peck, 1911). Her life and many achievements were exceptional although mountaineering is the emphasis of this paper.
Peck’s climbing résumé began in 1885 with modest peaks, followed by the Matterhorn and then higher ones in Mexico including Popocatépetl and the tallest, Pico de Orizaba 5,636 m (18,491 ft), in 1897. Like most in that era, she employed mountaineering guides. Soon after Orizaba, which no woman had climbed before, Peck’s ambition and start of plans were to climb the highest peak in South America, which had yet to see a first ascent by a man or a woman. She knew that 6,959 m (22,831 ft) Aconcagua had been climbed in 1897, and while it ultimately proved to be the tallest in South America, there was speculation of even higher peaks. In early 1898, Peck had already turned her attention to a Bolivian mountain range, but her “heart sank” when she read that it would be explored later in that same year by Sir W. Martin Conway (1856–1937) (Peck 1911; Peck 1906).
Peck was aware of Conway, but they sometimes confusingly used the names Sorata and Illampu interchangeably or with different interpretations. Conway was a British explorer of the Karakoram Himalaya and the Andes including an 1898 first ascent of 6,438 m (21,122 ft) Illimani on the southern end of the Cordillera Real. He next approached the northern end of the Cordillera Real and “Mt. Sorata,” describing it as “world-renowned.” For Conway, Sorata was not a mountain but a massif. Since the pre-Columbian era, two peaks on the Sorata massif were known by their indigenous names and legends. The northern peak is 6,367 m (20,892 ft) Illampu; the southern peak is 6,427 m (21,086 ft) Ancohuma (Janq’u Uma). Centuries before Conway, the approach town of Sorata (Surat’a in the Aymara language) northwest of nearby Illampu accounted for the Sorata name of the massif, or it may have been the converse. However, Conway also wrote that the Sorata massif was then popularly but incorrectly called by its northern peak, Illampu, and Peck sometimes used it that way, too. His chapter “First Attempt on Mount Sorata” was about attempting the higher Ancohuma, then known as the south peak of Illampu. From the town of Umapusa, he reached almost 6,100 m (20,000 ft) on Ancohuma but was stymied by crevasses and heavy snowfall. Conway visited Sorata town in the north, but because of inclement conditions, he could not attempt Illampu. A second effort on Ancohuma was also unsuccessful. To summarize, Conway called the whole massif Mt. Sorata (Conway, 1901; Conway, 1899). Today, still confusingly, the massif is known as Mt. Sorata, the Sorata massif, the Illampu-Ancohuma massif, or the Illampu-Janq’u Uma massif, while the north peak is known as Mt. Sorata or Mt. Illampu.
In Peck’s correspondence, interviews, newspaper reports, and publications about the 1903 expedition, Sorata initially and usually meant Illampu peak. In her “Climbing Mt. Sorata” paper about 1903 is a photo caption “Mt. Sorata from town of Sorata,” and she used “Sorata or Illampu” once in the text (Peck, 1906). The names in her later 1911 book are somewhat in line with Conway; for example, the chapter “Journey to Mt. Illampu” has a photo caption “Sorata, Mt. Illampu” (Peck 1911). She reached Sorata town intending to climb Illampu peak on the Sorata massif. However, guide Antoine Maquignaz insisted that they climb on the Sorata massif by attempting Ancohuma peak from the town of Umapusa because that was the way he tried on the Conway expedition. Peck only briefly mentioned this late change in towns and routes but not Ancohuma by name. Either route or peak was on the Sorata massif and would have been a first ascent. In our paper about 1903, we follow Peck’s original plan and preference of using the name Sorata for the 1903 expedition, its equipment, and the intended peak, Illampu. In the title and conclusion, we use “Sorata (Illampu),” even though ultimately it was Ancohuma on the Sorata massif that she attempted.
Peck began her first attempt on Sorata in 1903, reaching about 4,700 m (15,350 ft). The activity with oxygen on Sorata is examined later in this paper. In 1904, with a new team, she attempted the same peak on the Sorata massif again, this time reaching to within 250 m (800 ft) of the summit. In 1908 in Peru, on a sixth attempt, a guide and Peck completed the first ascent of Huascarán Norte 6,655 m (21,834 ft) (Kimberley, 2017; Peck, 1911; Peck, 1906). However, the focus of this paper is Peck’s 1903 first attempt on Sorata that reached 4,700 m (15,350 ft) with the intention of using supplemental oxygen higher up. The authors are unaware of how or why Peck considered an informal experiment with supplemental oxygen, but the expedition of 1903 was the first to take an apparatus to chemically generate oxygen on any great mountain expedition. In this case, it was in the Andes.
The 1903 Mt. Sorata Expedition Annie Peck and William Tight
Peck supplied the inspiration, planning, persistent fund-raising, and determined leadership for 5 years for the expedition to Sorata in 1903. She selected and paid for three people to leave New York with her for Bolivia. One of the two European mountain guides was Maguignaz. The third man was William G. Tight, PhD (1865–1910), president of the University of New Mexico (UNM) and a geomorphologist (Brooklyn Daily Eagle, 1903) (Fig. 1). New Englander Peck described Tight’s selection: “by correspondence to a gentleman of an hour’s acquaintance who, a few years earlier, had been recommended to me as an expert photographer and an all-around scientist, his specialty being geology” (Peck, 1911). Peck planned the expedition to have scientific validity; consequently, the team took meteorological, medical, and topographical instruments. For example, she had two mercurial and two aneroid barometers, each from a different source (Peck, 1911; Peck, 1906).

The Sorata team leaves New York on June 16, 1903 (Brooklyn Daily Eagle, 1903). Behind Annie Peck is the tall and bearded William Tight. They are accompanied by two European guides.
By 1903, balloonists had already reached heights considerably higher than Sorata with or without supplemental oxygen compressed in tanks or bags and delivered by a tube or pipe stem in the mouth (Featherstone and Ball, 2020). People had already climbed to heights slightly greater than Sorata without supplemental oxygen. Peck, having been to 5,636 m (18,491 ft) on Orizaba, was optimistic about the prospects of going higher and wrote this: “The region of the Andes has troubles peculiarly its own or shared only by the Himalayas. These difficulties, due to the extreme and unaccustomed altitude, though grave, are by no means insurmountable to one of strictly sound physique” (Peck, 1911). Nevertheless, she safeguarded her chances, stating more simply: “I propose… to experiment with bags of oxygen… I expect the oxygen to help much” (Las Vegas Daily Optic, 1903; Peck, 1906).
Peck described the Sorata oxygen system in a New York Times article two days before leaving for Bolivia: “Five oxygen tanks have been provided, one for each member of the party, and an extra one in case one of them gets out of order. The tanks are made of rubber and are made to be worn over the shoulder in the same way that soldiers carry blankets on forced marches. Each tank is of 10 gallons [38 l] capacity, and attached to each is a long rubber tube fitted with a patent inhaler, through which the gas can be taken whenever required. Dr. Tight will manufacture the oxygen and will have with him a complete manufacturing apparatus” (New York Times, 1903). However, geologist Tight was not in any strict sense an oxygen apparatus inventor or high-altitude pioneer in the mold of Scottish chemistry lecturer and Himalayan mountaineer Alexander Kellas (1868–1921). Peck wrote little about Tight’s role in her paper “Climbing Mount Sorata” (Peck, 1906). A few more details appeared in her later book: “We prepared to attempt the use of oxygen on the mountain… Accordingly, we planned to transport to our highest camp materials for its manufacture, with rubber bags to contain the gas. They were made by the Davidson Rubber Company of Charlestown, Mass., who assisted in their design” (Peck, 1911).
An analysis relies on these writings and our assumptions and deductions. A “complete manufacturing apparatus” will be considered later in this paper. The Boston location of Davidson implies that Peck arranged it, not the other team members who lived in New Mexico or Europe. Peck wrote “bags,” so oxygen compressed in metal cylinders can be excluded. Davidson being a supplier of medical products suggests that the Sorata delivery device was adapted from an ordinary medical oxygen apparatus rather than a more obscure mining or diving set. Their stock oval rubber bag volumes ranged up to 10 gallons (38 l), but Peck’s rubber “tanks” may have been the reinforced oblong ones available by dimension (Smithsonian Institution, 2024). These capacities were insufficient for hard-breathing climbers even if reinforced rubber bags were modestly pressurized with hand-cranked compressors. The small volumes and the phrase “gas can be taken whenever required” imply the intermittent use of oxygen prevalent at the time. The term “patent inhaler” suggests a commercial product with a reed or flapper valve in the mouthpiece for pinching to control flow. A “long rubber tube” without mentioning valves means that gas flowed in one direction without a loop; therefore, it was an open-circuit set. In summary, oxygen manufactured in camp would have been transferred via tubing to a large storage bag to carry it and from there distributed by a modified medical tube, small bag, and mouthpiece open-circuit set as had been done for many years in clinics, homes, and other sedentary settings. There is a rough sketch of a small medical oxygen set (Leigh, 1974) (Fig. 2).
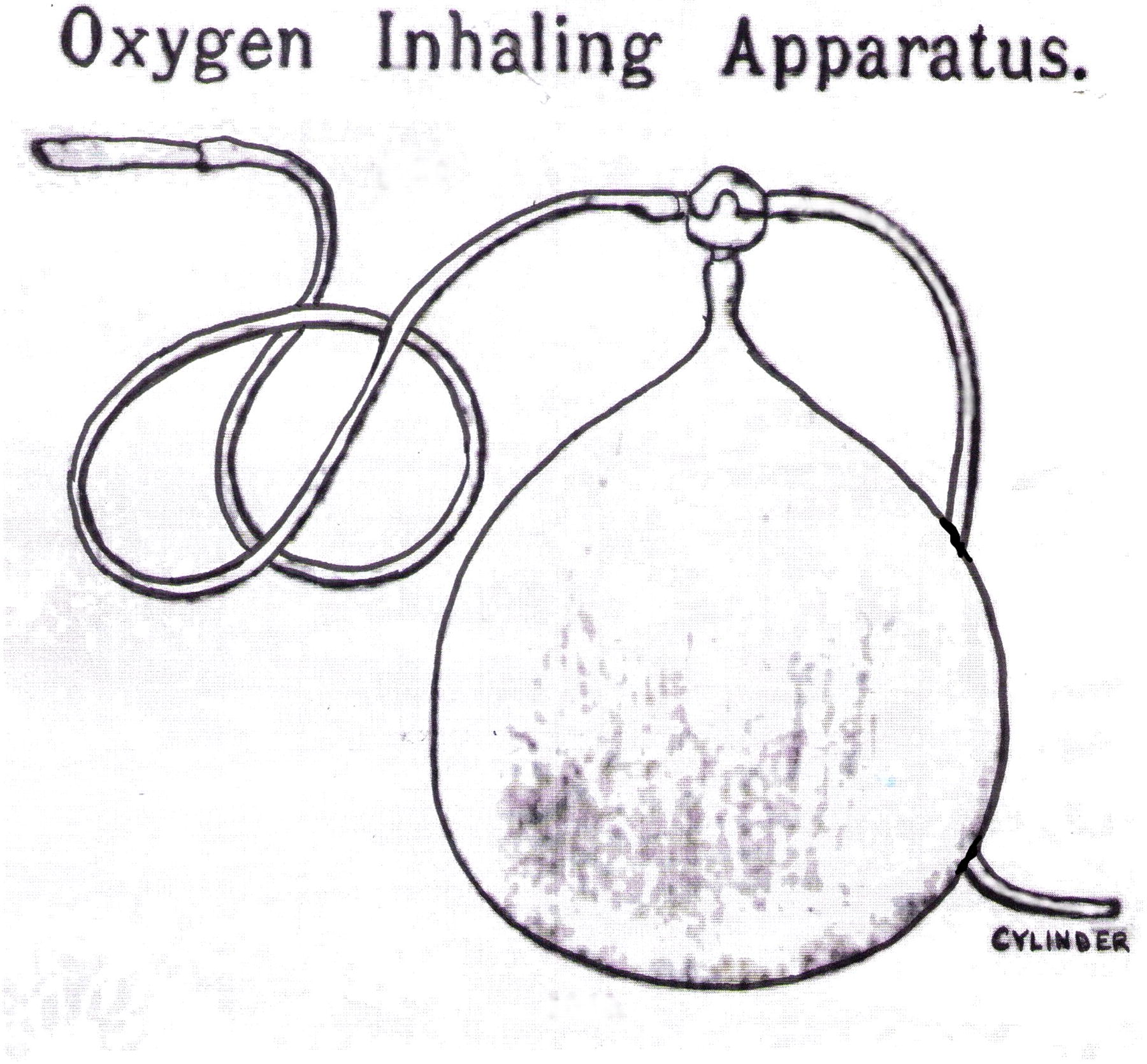
Sketch of a 1919 medical oxygen tube, bag, and mouthpiece open-circuit set similar to those used for over a century (Leigh, 1974). Chemically generated or compressed oxygen enters the device under pressure from the tube at bottom right. The rubber bag is an inflatable bladder that moderates pressure and volume during expiration when the mouthpiece valve is closed. Oxygen is inhaled through the tube at upper left and through a valved mouthpiece to the sedentary user.
Users needed to master the rhythm of biting the mouthpiece flow valve during nose expiration but not during mouth inspiration. Fortunately, two-valve mouthpieces became available, so respiration could be more normal (Leigh, 1974). The Sorata device needed to be a larger version to allow the heavy respirations of a climber. Lastly, Davidson “assisted in their design” is unknown. No details on this subject were found by the Peck biographer, author H.K. (Kimberley, 2017). A further search of Peck correspondence in the Brooklyn College archives by author H.L. in 2024 was also unrevealing.
Chemical production of oxygen in the 19th and into the 20th century
Throughout the 1800s, oxygen was produced by heating and thermal decomposition of various chemicals. Oxygen for small nonindustrial users since the 1860s was typically produced by heating potassium chlorate with manganese dioxide catalyst to about 400°C (Featherstone and Ball, 2021). It was usually not procured but was produced directly at the site of usage and often stored in rubber bags (Leigh, 1974). Physicians, oxygen “parlors,” and homes dispensed oxygen sometimes laced with nitrous oxide, other gases, or colorants for entertainment or as a panacea for real or imagined medical conditions and by routes under the skin or into the urethra, vagina, rectum, nose, or mouth. The usual delivery device was a tube from a rubber bag of gas. Rubber bag usage continued long after 1868, when stronger but heavier cast iron or steel cylinders supplanted copper cylinders for storage (Featherstone and Ball, 2021; Leigh, 1974). There were no guidelines for the use of oxygen anywhere, let alone on a mountain. Oxygen was typically used only intermittently, often for just minutes. Continuous therapy first began in 1890 for a pneumonia patient (Grainge, 2004; Leigh, 1974). John Scott Haldane (1860–1936) later helped bring medical oxygen therapy to a rational and scientific basis (Grainge, 2004; Haldane, 1917). His pithy remark was that the reluctance by medical professionals to administer oxygen continuously but rather only intermittently was” like bringing a drowning man to the surface of the water—occasionally” (Grainge, 2004). It was well into the 20th century that continuous oxygen became standard medical care (Grainge, 2004). In 1903, when Peck went to Sorata, it was not known how to use supplemental oxygen in the mountains either intermittently or continuously, at rest or while climbing, at what altitude, at what rate, for how long, by what delivery device, or to what benefit.
While the heated chemical method could provide oxygen to compress in cylinders, it was not feasible to use such a method inside a breathing apparatus. There was more progress in the development of inside devices for mining, diving, and rescue breathing with hydroxide chemicals to absorb carbon dioxide than with other chemicals to produce oxygen. For example, German physiologist Theodore Schwann (1810–1882) demonstrated a prototype closed-circuit device that relied on compressed oxygen with a soda lime carbon dioxide scrubber in Brussels in 1876 and Paris in 1878, but it never went into production. Contemporaneously, British diving engineer Henry Fleuss at Siebe Gorman Company in London patented and produced the first practical apparatus using compressed oxygen and a potassium hydroxide carbon dioxide scrubber (Davis, 1950; Foregger, 1966; Martin, 1913).
There were two possibilities for chemical production of oxygen on Sorata in 1903. The first involves a class of chemicals that react with water and carbon dioxide to release oxygen and simultaneously capture carbon dioxide. Several peroxides and superoxides have these remarkable chemical properties. French chemical engineer George Jaubert (1870–1959) recognized the properties of solid sodium peroxide and potassium peroxide in 1898 and studied their industrial and biological uses. (Gall, 1902). Oxylithe was the marketing name for the preparation that Jaubert formulated in or before 1902 and was produced at the Société d’Electrochimie. The chemical name is derived from two ancient Greek morphemes that signified oxygen and stone. Oxylithe was mostly or all sodium peroxide and agglomerated into pellets or small cubes and also larger blocks for industry. Jaubert tested Oxylithe in closed-circuit systems using guinea pigs and began applications for short-term use in humans in mining, diving, and underwater rescue (Crookes, 1902; Davis, 1950; Durand, 1902; Gall, 1902; Mitchell and Rodway, 2011; Rodway, 2004; Scientific American, 1902; West, 2003a).
The rights to the French product were acquired in 1904 by the English Siebe Gorman Company. Augustus Siebe (1788–1872) had moved from Germany to England and in 1819 created Siebe and Company. A variant of the use of Oxylithe was a large, heavy steel 1904 Siebe Gorman apparatus that used only the oxygen-producing qualities of the chemical and stored it inside a rubber bag to then be compressed into a tank. (Davis, 1950). The possibility that this unwieldy 1904 device was used on Sorata in 1903 can be excluded.
Breathing systems evolved through many versions using carbon dioxide scrubbers, compressed air, compressed oxygen, chemical production of oxygen inside the apparatus, and eventually, liquid oxygen. The Austro-Hungarian Nachfolger closed-circuit Pneumatogen systems using solid peroxides and superoxides were marketed in England by Siebe Gorman, along with the latter’s products, especially those developed under Director Sir Robert H. Davis (1870–1965). Siebe Gorman was also heavily involved with the compressed oxygen systems on all of the British Everest expeditions of the 1920s to 1953 (Bech, 2024; Davis, 1950; Grahn and Beeckmann, 1907; Martin, 1913; Singleton, 2018).
The aforementioned Pneumatogen refers to a device taken on a 1907 British expedition. It was written in 2003 that “The first use of supplementary oxygen in the Himalayas was apparently in 1907 when A. L. Mumm, Thomas Longstaff, and Charles Bruce went to the Garhwal [Himalaya] and made the first ascent of Trisul (7,127 m), [sic], which [presumably] remained the highest summit to be climbed for 21 years. Small oxygen generators were taken along on this expedition” (West, 2003b). The height of Trisul 1 is now considered to be 7,120 m (23,360 ft). It was not recognized until about 80 years later that Kellas broke the altitude record in 1911 on 7,125 m (23,375 ft) Pauhunri and without using supplemental oxygen (Mitchell and Rodway, 2011).
Mumm’s high point in 1907 was “Misery Camp” at about 6,100 m (20,000 ft). He wrote that, “I took out, as my special contribution to our outfit, some oxygen generators, or pneumatogen cartridges, manufactured [actually, marketed] by Siebe, Gorman, and Co. They are intended to be employed in mines where the air is foul, but I thought they might be useful at great heights.” (Mumm, 1909). Mumm may have had just a cartridge, as he stated, or an entire ingeniously named pneumatogen assembly of a generating cartridge, breathing chamber, bag, hose, and mouthpiece. The model is unknown, but it would likely have been a closed-circuit rebreather set with cartridges of potassium sodium superoxide whose chemical reactions with moisture and carbon dioxide in exhaled breath simultaneously generated oxygen and removed carbon dioxide. Some models also had small canisters of compressed oxygen to boost the initial flow of oxygen. The earliest Pneumatogen was the basic 1904 Type 1 (Stoek, 1908) (Fig. 3). More sophisticated models would follow (Bech, 2024; Grahn and Beeckmann, 1907; Stoek, 1908). The Peck expedition would not have had any of these in 1903.
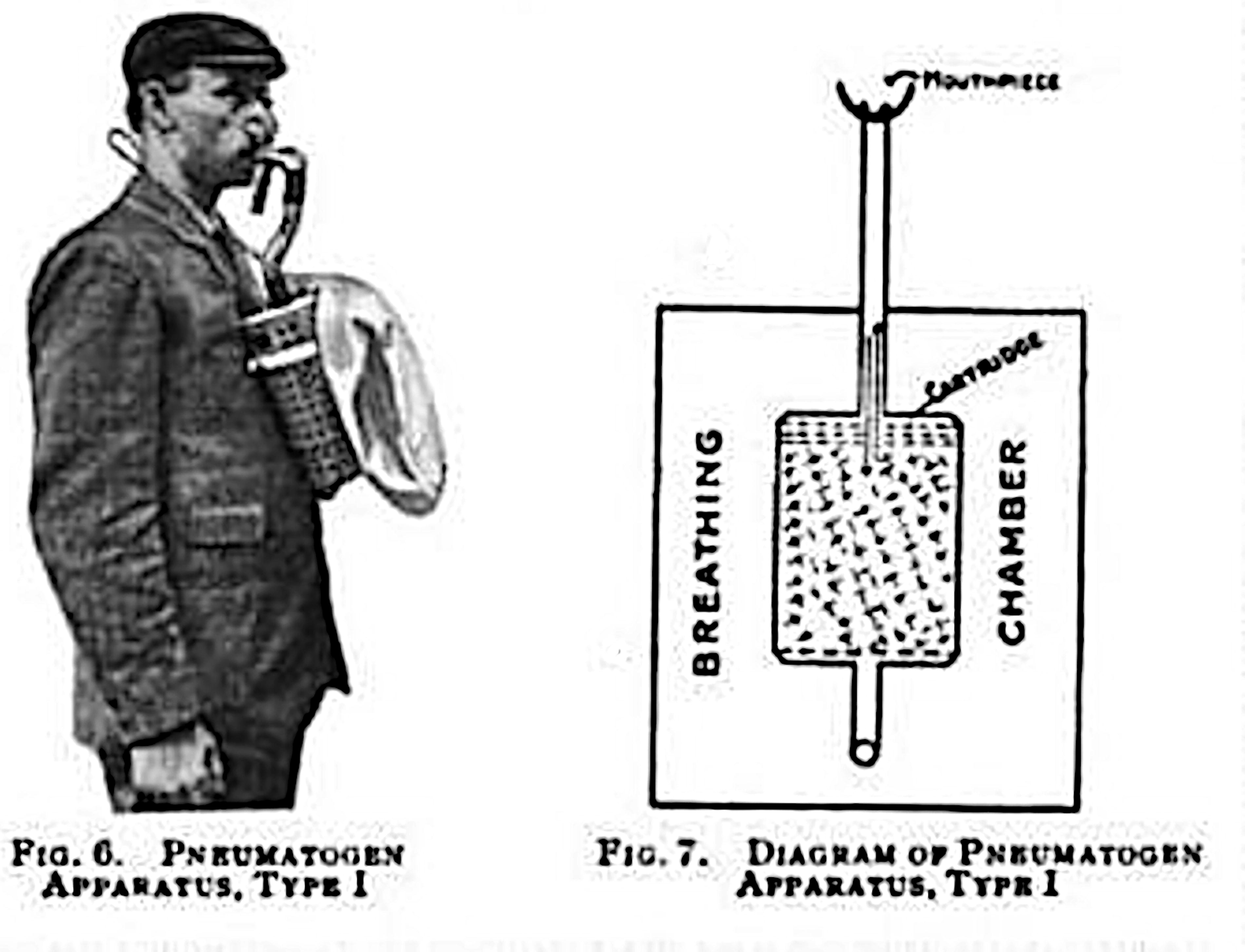
Pneumatogen Type 1 1904 (Stoek, 1908). Manufactured in Austria-Hungary by Nachfolger and marketed in England by Siebe Gorman, this basic closed-circuit rescue set had a single back and forth breathing tube, bag and regenerating cartridges of potassium sodium superoxide. The chemicals are represented by the stippled area in the center of the sketch. The device made oxygen and removed carbon dioxide but was limited by high respiratory effort and a 30-minute duration at a low walking speed (Bech, 2024; Grahn and Beeckmann, 1907; Stoek, 1908). Even if available for Peck in 1903, this 1904 first model would not have been suitable for mountaineering.
As West stated, the Mumm anecdote did not constitute a scientific attempt; however, in 1907, it was the only supplemental mountaineering oxygen information available until the use of compressed oxygen in heavy cylinders was compared with chemically generated oxygen in bags by Kellas in 1920 (Kellas, 1921; Mitchell and Rodway, 2011; Rodway, 2004; West, 2003b).
Other attempts at chemical production of oxygen on mountains were tried later. British physiologist Leonard Hill (1866–1952), who collaborated with Siebe Gorman, suggested that Kellas try Oxylithe in 60 l rubber bags on the 1920 Kamet expedition in the Himalaya.
The Hill/Kellas “bag method” was a simple closed-circuit system that generated oxygen and simultaneously removed (scrubbed) carbon dioxide by chemical reactions inside a large rubber bag carried under the arm while climbing (Kellas, 1921; Rodway, 2004). Hill probably advised the bag method because of its simplicity. Like the early 1904 Pneumatogen Type I, breathing simply flowed air back and forth between the user and the device through a short tube. It was a valveless closed-circuit set but not a one-way recirculating loop. Water and carbon dioxide in exhaled breath promoted a continuous chemical reaction with the Oxylithe in the bag. Kellas tested subjects over a short course on a peak near Kamet at about 5,486 m (18,000 ft) and found that breathing low-flow supplemental oxygen while carrying heavy cylinders of compressed oxygen slowed the climbing rate. However, breathing oxygen released from Oxylithe inside the lighter bags, and shaking to agitate it while carrying it awkwardly under an arm improved the climbing rate (Kellas, 1921; Mitchell and Rodway, 2011; Rodway, 2004; West, 2003a). Despite this experiment, the simple but limited-duration Hill bag method was not used again. Oxylithe was not taken on the 1921 British Everest expedition, where Kellas unfortunately died, and the compressed oxygen taken in cylinders was not used by the others. The possibility that the 1920 oxylithe bag method was used on Sorata in 1903 can be excluded.
There were attempts on Everest by the British in the 1920s, 1930s, and 1953. All these expeditions had open-circuit sets with compressed oxygen that simply expelled exhaled breath and unused oxygen. With modifications and newer materials, this continues today as the mountaineering standard. Closed-circuit sets were also tried, with hydroxides to scrub carbon dioxide and compressed oxygen instead of oxygen chemically generated inside the breathing sets. The closed-circuit design was taken on British attempts on Everest in 1936 and 1938, on Cho Oyu in 1952 with simulated closed-circuit sets, and very nearly successfully on Everest in 1953 (Windsor et al., 2005).
The Swiss Spring 1952 Everest oxygen system with potassium superoxide to generate oxygen and remove carbon dioxide was adapted from a Mine Safety Appliances, Pittsburgh, Pennsylvania, device. It was a closed-circuit rebreather but only tested beforehand in a hypobaric chamber by a sedentary user. Flow restriction in the tubing and mouthpiece limited its use to while at rest. It was not found to be effective at the high ventilatory rate and volume required for active climbing (West, 2003a; Wyss-Dunant, 1953).
There was only a remote chance on Sorata in 1903 of using an early closed-circuit rebreather mining apparatus. The first model potassium sodium superoxide Austro-Hungarian Pneumatogen was not until the 1904 Types 1. European models did not appear in mines in the United States until 1908, and none were made in the U.S. until later (Bech, 2024; Grahn and Beeckmann, 1907; Singleton, 2018; Stoek, 1908; Van Dolah, 1972). Even if it had just become available, the use of an unfamiliar and potentially dangerous system was improbable on Sorata in 1903. Peck’s date and description for Sorata in 1903 do not fit any of these possibilities, and it can be excluded.
Potassium chlorate
The second possibility for chemical production of oxygen on Sorata in 1903 was the long-established heated chlorate method. In the 1870s, potassium chlorate taken orally was used without a medical or chemical basis on at least 3 mountaineering expeditions in Central Asia and South America (Bellew, 1875; Henderson and Hume, 1873; Whymper, 1892). Instead, heating chlorate was the effective method of producing oxygen and is the main point of this paper.
Oxygen had been produced by battery-powered electrolysis since about 1800, but on Sorata heavy and cold batteries and the absence of electrical utilities made this impossible. Liquid oxygen had only recently been developed, but securing, storing, and transporting it was impractical for Sorata. The only realistic option was to chemically manufacture oxygen in camp by the traditional method of heating potassium chlorate. Today, some chemical oxygen generators still use sodium, potassium, or lithium chlorate or perchlorate for mining, diving, rescue, industrial, medical, austere setting, naval, aviation, and even spacecraft purposes. Chlorate “candles” (canisters), invented during the Second World War, are highly efficient per volume (Graf, 2017; Schechter et al., 1950).
Heating potassium chlorate with a manganese dioxide catalyst could be done simply in a flask over a burner or in larger amounts by a device for immediate use, storage in bags, or compression into metal tanks. For example, a contemporary tabletop 1902 Kamm apparatus heated the chemicals to release oxygen (Lancet, 1902). One Kamm retort made 113 l of oxygen; a twice-loaded retort could fill Peck’s five 38 l bags. Another example was the small suitcase-size New York Wallian device that could make up to 95 l per retort in 25 minutes (Aulde, 1890).
The outcome
In 1903, the Sorata team departed New York by ship, then by rail, and crossed Panama, where Tight complained of not knowing that they would be gone so long. The seeds of discontent were sown. They traveled along the Pacific coast by ship, then by rail rapidly ascended the western cordillera of Bolivia, where Tight developed a violent headache ostensibly attributed to acute mountain sickness, known there as soroche. Peck had a supply of the local remedy, coca leaves. After crossing Lake Titicaca, they reached La Paz before proceeding up the eastern cordillera to Sorata town with plans to produce oxygen for climbing at a camp above there. (Peck, 1911; Peck, 1906).
It is not known what appliance Tight intended to use, but he could manufacture oxygen using the traditional heated chlorate method and would have known its productivity and its danger. Ironically, Tight used these same chemicals at UNM 3 years later and suffered severe injuries and permanent scars from an explosion. (Bork, 2003; Davis, 2006). Disappointedly, many of his papers were lost during unrelated fires at Denison University in 1905 and UNM in 1910. Tight biographer Kennard Bork found no direct information on the Sorata subject (Bork, 2003; personal communication 4/3/2024). Investigation of the remaining Tight archives by Bork and author H.L. in 2024 revealed no additional details. Even in the absence of physical evidence, the history and 1903 date suggest a near certainty that the goal was to produce oxygen on Sorata by the method of heating chlorate.
Despite the noteworthy history of supplemental oxygen in this narrative, the story takes a downturn. In Bolivia, a debacle unfolded. Peck was perturbed when Tight geologized in a mine for a day rather than the team proceeding directly to the mountain, her raison d' être. Although she planned to climb Illampu on the twin-peaked Sorata massif, the goal once there was changed to Ancohuma. Reaching about 4700 m (15,350 ft), they were not on the glacier yet but were higher and colder than Tight’s experience. There were the difficulties of nights below −18°C, snow, poorly-outfitted porters, and Tight’s schedule. The next morning, thoroughly chilled and worried about time, Tight began to descend. Peck’s plan was to transport the gear “to our highest camp,” likely meaning at about 5500 m (18,000 ft) on the glacier. Peck offered to double the local laborers’ pay and lighten their loads, including the oxygen equipment, if only they would carry some gear higher. They refused. The two guides rejected the idea of offering themselves for triple load carries upward. On the Sorata and Huascarán expeditions, the porters and guides would respond only to a man rather than Peck because of the misogynistic attitudes of the era. They did not acknowledge a woman as the leader of the expedition, even though she organized it and paid their way. (Kimberley, 2017; Peck, 1911; Peck, 1906). The oxygen system was not used. Peck had no choice but to follow the others down without a summit bid.
Many publications initially but erroneously reported a successful ascent, but it was not. Peck was “dumbfounded” and publically blamed Tight (Newark Daily Advocate, 1903). In “Climbing Mount Sorata” and in A Search for Apex of America, Peck referred to Tight disparagingly only as “the scientist” or “The Professor,” never by his name (Peck, 1911; Peck, 1906). A magazine sponsor did not even open a box of Tight’s photographic plates because they declined to publish Peck’s account of an unsuccessful expedition (Abbott, 1903). The oxygen apparatus was only mentioned again to state that it was not taken on the following year’s Sorata attempt (Peck, 1911). Whether a trial of using the rudimentary 1903 Sorata oxygen apparatus would have improved the climbing rate and for how long is unknown. No one would know significantly more about any type of supplemental mountaineering oxygen until Kellas in 1920.
Conclusions
The Annie Smith Peck expedition of 1903 to 6,367 m (20,892 ft) Mount Sorata (Illampu) took the first chemical oxygen apparatus to a great mountain. This preceded Arnold Mumm in 1907, who took and informally used a different chemical oxygen generator the Pneumatogen system, for a few minutes on Mt. Trisul 1. The incompletely described Sorata chemical oxygen generator and rubber bag apparatus had limited potential and were unused at 4700 m (15,350 ft) on the 6,427 m (21,086 ft) Ancohuma of the twin-peaked Sorata massif, but the conclusions here are reasonable deductions. The equipment taken by Annie Peck and William Tight almost certainly would have generated oxygen by the traditional 19th century method of heating potassium chlorate, collecting the oxygen in a bag, and delivering it to the climbers using a modified medical tube and mouthpiece open-circuit set. This episode reveals a little-known part of the story of supplemental oxygen in the mountains.
Footnotes
Acknowledgments
The lead author would like to express his respect and appreciation for high altitude medicine historian George Rodway, co-author H.K. (biographer of Annie Peck), Kennard Bork (biographer of William Tight), Jan Willem Bech (certified safety manager and RAH occupational hygienist) at ![]() , the archives staff of Brooklyn College and the University of New Mexico, and Remi Sojka (adventures together in the Himalaya, on Orizaba and Aconcagua).
, the archives staff of Brooklyn College and the University of New Mexico, and Remi Sojka (adventures together in the Himalaya, on Orizaba and Aconcagua).
Ethics Statement
The authors declare that there were no ethical issues.
Authors’ Contributions
H.L.: Concept and first drafts. H.L. and H.K.: Research, revisions, and approval.
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Funding Information
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.