
Abstract
Yoder, Taylor L., Kreager A. Taber, Laurens E. Howle, and Richard E. Moon. Pushing scuba to new heights: approach, decompression, and logistical considerations for high-altitude diving. High Alt Med Biol. 26:109–117, 2025.—There is interest among technical, expedition, commercial, and military divers in expanding diving operations to high altitude. However, altitude diving presents unique challenges including acclimatization, increased decompression sickness (DCS) risk, and logistical and equipment considerations. Divers must plan altitude acclimatization strategies conservatively to reduce risk of acute mountain sickness and dehydration before diving. Several methods of augmenting sea level diving tables to be used at altitude have been theorized and tested both in simulated dives and high-altitude expeditions. With proper acclimatization, augmentation of standard diving tables, equipment, and safety planning, diving at high altitude may be performed in many contexts safely while minimizing risk of DCS or injury.
Introduction
Diving at altitude requires consideration of specialized equipment, logistical and safety plans, and decompression profiles different from those used at sea level. Jacques Cousteau’s 1968 exploration of Lake Titicaca (3,812 m) is credited as the first-known high-altitude diving expedition and it has quickly grown in popularity since, with many dive shops offering altitude diving courses for recreational divers (PADI, 2024) and individuals pushing the limits of altitude diving in pursuit of diving records (Kot et al., 2014). Expansion of diving operations into high-altitude lakes and reservoirs is also crucial for commercial divers for hydroelectric and construction operations (Zhong-Yuan, Xi-Wei and Yan-Meng, 2003). While it is recognized that decompression procedures at altitude need to be more conservative, there is no consensus among diving organizations as to what elevation is the threshold requiring such adjustments. Recommendations for the minimum elevation requiring altitude adjustments range from 0 m (with weather considerations) to 600 m above sea level, and “high-altitude dives” above 2,400 m require additional decompression precautions due to hypoxia risk (Egi, Pieri and Marroni, 2014).
Unique considerations with altitude diving include approach considerations to minimize risk of acute mountain sickness (AMS) and dehydration, greater nitrogen off-gassing due to the increased pressure ratio from depth to the surface (see below), and additional logistic and technical considerations that make development of decompression sickness (DCS) possible even with conservative dive profiles (Buzzacott, n.d.). This review summarizes current recommendations regarding approach and environmental considerations, acclimatization, safety concerns associated with decompression algorithms, and other concerns specific to high-altitude diving for recreational technical divers.
Effects of Altitude
Successful approach strategies for altitude divers have been reported along with outcomes of small-scale dive expeditions but altitude exposure still presents a risk to dive operations (Egi, Gürmen and Aydin, 2003; Kot et al., 2014; Le Pécho and Le Masson, 1994; Leach, McLean and Mee, 1994; Sahni et al., 1991). Altitude must be considered in terms of (1) effects on cognition, (Rex et al.) (2) altitude illnesses and acclimatization, and (3) adjustments that must be made to decompression procedures.
Altitude hypoxia can negatively impact cognition and physical performance (McMorris et al., 2017; Subudhi et al., 2014). The detrimental effects of altitude have been quantified as slowed reaction times (Dykiert et al., 2010; Virues-Ortega et al., 2004) impaired learning and memory (Kramer, Coyne and Strayer, 1993; Nation et al., 2017), and decreased mood and physical performance (Shukitt-Hale, Banderet and Lieberman, 1998), among other measures. During expeditions by Leach et al. (1994) and Sahni et al. (1991), divers were noted to exhibit decreased physical performance, impaired concentration, sleep and appetite changes, and fatigue during their initial ascents to altitude, and symptoms improved before dives were begun (Leach, McLean and Mee, 1994; Sahni et al., 1991). Although it is difficult to assess whether the predive cognitive effects of altitude exposure may contribute to intra-dive task performance, research by Shi et al. (2017) demonstrated intra-dive electroencephalogram (EEG) and acute mountain sickness (AMS) symptom evaluation improved to divers’ pre-altitude baselines. This suggests that in divers experiencing mild cognitive impairment as an effect of acute altitude exposure, their ability to perform and complete tasks during a dive is not impacted (Shi et al., 2017), undoubtedly due to normal or supranormal PO2. Furthermore, Shi et al. (2017) hypothesized that given resolution of divers’ self-reported AMS symptoms with exposure to hyperbaric conditions, their protocol of starting to dive 16 hours after arrival at 3,000 m may have even enhanced acclimatization due to the rise in PO2 during a dive, similar to the “stay high, sleep low” principle used for acclimatization.
AMS, defined as headache and other symptoms including dizziness, fatigue, loss of appetite, or insomnia, may develop after ascent to altitudes as low as 2,000 m in susceptible individuals (Honigman et al., 1993; Montgomery, Mills and Luce, 1989) and is a concern to altitude divers in the first days after arrival at altitude (Clark and Sheraton, 2024; Murdoch, 2010). AMS is common but variable among high-altitude trekkers with estimated incidence ranging from 36.7% to 75%, however, symptoms typically resolve within a few days and both prophylactic and treatment medications are available (Nafstad et al., 2016; Karinen, Peltonen and Tikkanen, 2008; Lawrence and Reid, 2016; Luks et al., 2024). Less common but more serious conditions such as high altitude pulmonary or cerebral edema (HAPE or HACE) would halt diving operations. In order to promote acclimatization with low risk of AMS the Wilderness Medical Society stresses that acclimatization rate varies among individuals but general recommendations include not increasing sleeping elevation by more than 500 m/day and including a rest day every 3–4 days at elevations above 3,000 m (Luks et al., 2024). Acclimatization improves arterial oxygenation, reduces AMS incidence, and results in recovery of cognitive function at altitude (Subudhi et al., 2014). Additionally, acetazolamide prophylaxis starting the night before ascent and continuing during ascent is recommended for AMS prophylaxis, particularly for travelers at medium/high AMS risk (Luks et al., 2024). Phospodiesterase-5 inhibitors (sildenafil and tadalafil) have been used to reduce pulmonary artery pressure at altitude and prevent HAPE (Luks and Swenson, 2008; Maggiorini et al., 2006; Poudel et al., 2024). However, a possible concern regarding these drugs related to diving is that rat studies indicate that doses analogous to those used in humans increase cerebral blood flow and accelerate the onset of central nervous system oxygen toxicity (Demchenko et al., 2009). Therefore, when using these medications, divers should not use a breathing gas in which the PO2 exceeds 1.0 atm. Conservative acclimatization strategies implemented in dive expeditions have broadly been successful in mitigating AMS development and mission-limiting effects of altitude including HACE and HAPE (Egi, Gürmen and Aydin, 2003; Leach, McLean and Mee, 1994; Sahni et al., 1991). Of note, one diver in Egi et al.’s (1997) expedition (Egi, Gürmen and Aydin, 2003) developed AMS symptoms including severe nausea/vomiting, fatigue, and lightheadedness despite a conservative ascent but the diver’s symptoms resolved quickly with bedrest.
DCS develops due to absorption of inert gas (most commonly nitrogen) into tissues with exposure to increased environmental pressure and subsequent bubble formation in the blood or tissue due to supersaturation caused by reduction in ambient pressure (Mitchell, Bennett and Moon, 2022). This may occur during dive ascents or rapid exposures to high altitude, for example during aviation or spaceflight. Symptoms of DCS include motor weakness, stroke-like symptoms, paresthesia, vertigo, musculoskeletal pain, constitutional manifestations such as fatigue, or cutaneous rash. Of particular interest in high-altitude diving conditions, risk of central venous gas emboli (VGE) and DCS is known to increase in cooler water compared with warmer conditions, even in mild temperatures such as 26.7°C compared with 36.1°C (Gerth, 2015). As many alpine lakes are far colder than these experimental conditions, these findings may not adequately quantify increases in DCS risk in the field. One study reported reduction of intravascular bubble detection with ultrasound during dives at sea level with predive intake of 700 ml water, although greater amounts increased bubble detection (Han et al., 2021). As ascent to altitude may predispose divers to dehydration, prevention of both AMS and DCS (Castellani et al., 2010; Han et al., 2021) may be facilitated by adequate hydration. This may be offset by use of acetazolamide to facilitate acclimatization, since it is a diuretic. Its use may therefore increase risk of dehydration (Clark and Sheraton, 2024) and conceivably DCS risk. In addition, a consequence of rapid ascent to altitude is lack of equilibration of tissue versus ambient inert gas partial pressure, which may take 24 hours.
Decompression Considerations
While at altitude, absolute pressure is decreased at depth compared to sea level due to the lower atmospheric pressure, however, the ratio of ambient pressure at any given depth to surface pressure is significantly increased at altitude, which for a given depth-time exposure increases the risk of DCS (NAVSEA, 2018c; NAVSEA, 2018d). This pressure gradient difference is especially distinct for the last 30–40 ft of the diver’s ascent (Fig. 1).
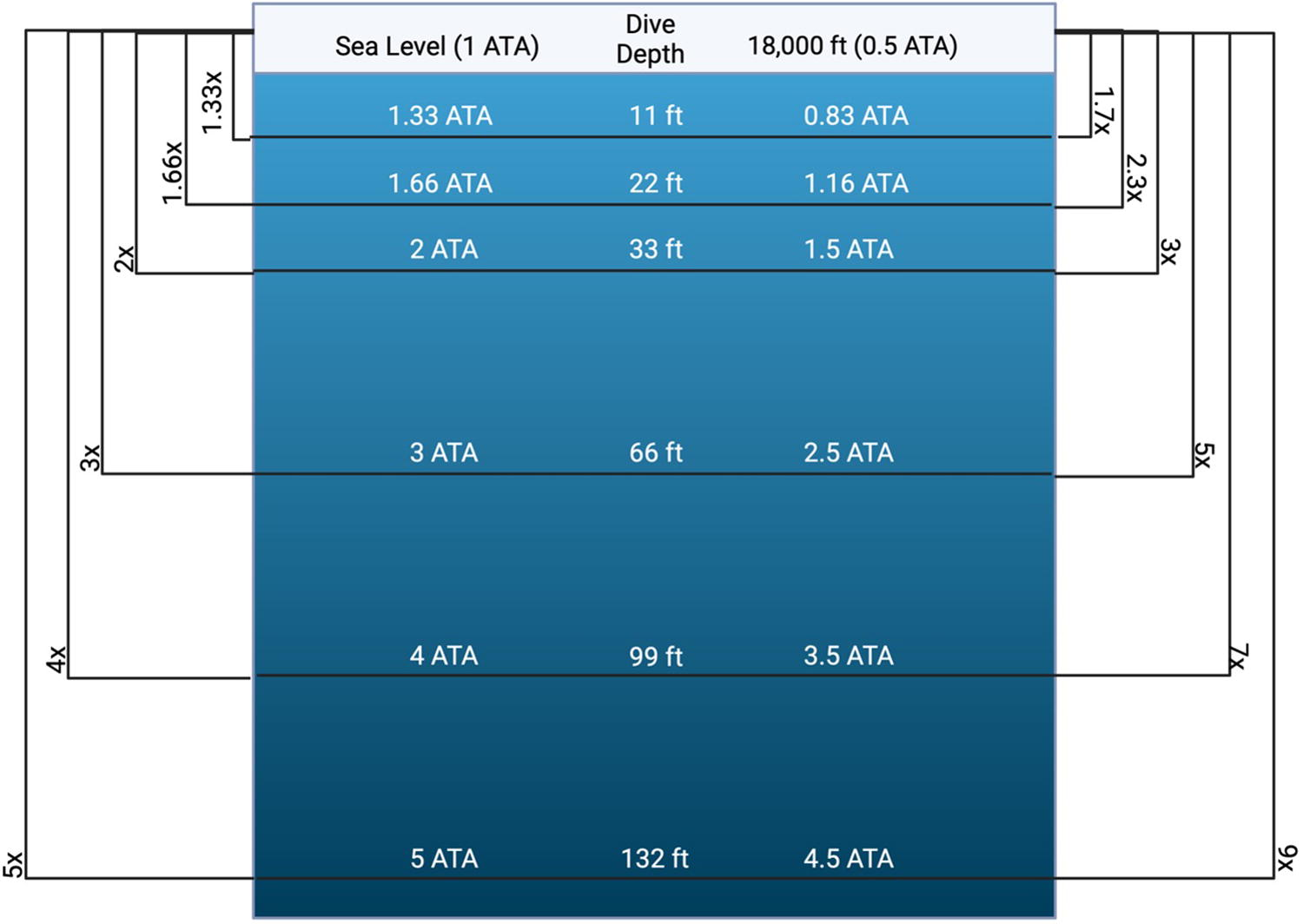
Ambient pressure changes while diving at altitude and relative depth to surface pressure ratios. Based on saltwater density—would vary with freshwater. Created with BioRender.com.
Along with the pressure gradient difference, growth of bubbles that may form during ascent from a dive is increased. Corrections must be performed to augment existing sea level decompression tables to allow safe altitude decompression (NAVSEA, 2018c; NAVSEA, 2018d).
Cross corrections (constant ratio translation)
One common method for decompression planning at altitude was first publicized by ER Cross in Skin Diver magazine in 1967 and once again in 1970 (Cross, 1967; Cross, 1970). This method, referred to as Cross corrections, calculates a “virtual” or “equivalent” depth for altitude dives that allows the use of standard sea level dive table for the new depth. Virtual depth is calculated by calculating the ratio of sea level atmosphere pressure to altitude atmospheric pressure (also referred to as a “Cross coefficient”) and then multiplying this ratio by the actual depth of the planned dive (Eq. 1). This results in a theoretical depth that can then be used with a sea level decompression table. This theoretical depth is deeper than the actual depth, therefore producing a more conservative decompression (Cross, 1967).
The depth of decompression stops must also be converted (Eq. 2). Unlike the theoretical dive depth, these theoretical stop depths are shallower.
Cross corrections allow for the use of the standard U.S. Navy (USN) tables while diving at altitude with simple mathematical conversions (NAVSEA, 2018d). Cross also endorsed using the method with repetitive dive tables, treatment tables, and for flying after diving, which increases the risk of DCS due to further decreased ambient pressure within the cabin of the plane (Cross, 1970). Cross corrections do assume acclimation to altitude by reaching a new steady state tissue inert gas partial pressure (roughly 24 hours after arrival) (Egi and Brubakk, 1995). The USN Diving Manual allows cross corrections for altitude dives up to 10,000 ft (3,048 m) (NAVSEA, 2018d). Note that most decompression tables are listed in feet of sea water (fsw), while most altitude diving is in fresh water, which is less dense and abbreviated as feet of fresh water (ffw): 1 ffw = 0.975 fsw.
Since its publication, this method has also been used in both real and simulated dives and shown to help mitigate DCS risk while diving at altitude. In 1994, British divers completed an expedition in the Nepali Himalayas with no-stop dives at 15,700 ft and 16,000 ft to 98 ffw. They used a similar method to Cross's theoretical depth by doubling their actual depth to use standard tables. Two enriched oxygen (“nitrox” N2/O2 60/40) dives were completed without any cases of DCS (Leach, McLean and Mee, 1994). Another expedition of four divers in the Himalayas in 2007 used Cross corrections to conduct six dives at Tilicho Lake at 16,138 ft to a maximum depth of 98 ffw while using nitrox: N2/O2 72/28. Divers breathed 100% oxygen during decompression from 10 mfw to the surface. There were no cases of DCS on this expedition but one diver did develop a high-grade doppler bubble score indicating significant decompression stress (Kot et al., 2014).
Zhong-Yuan et al. (2003) conducted a series of 85 simulated dry-air dives (with oxygen decompression for some) at 4,500 and 5,000 m. They used Cross coefficients to modify sea level decompression tables and no cases of DCS or bubbles were experienced by the divers (Zhong-Yuan, Xi-Wei and Yan-Meng, 2003). Cross corrections were supported again in a later study by Shi et al. (2017) when used to safely augment USN Heliox Tables (40% oxygen for 30 m dives and 26.7% oxygen for 50 m dives) at 5,200 m (Shi et al., 2017)
Two studies in recent years further showed efficacy of Cross corrections. Hess et al. performed simulated (hyperbaric chamber) air dives at 12,000 ft to 66 fsw using cross corrections (Hess et al., 2021). No cases of DCS were reported but VGE was measured (according to the Eftedal and Brubakk Scale) in 11 divers with a peak VGE grade 0 (no bubbles), 3 with VGE grade I (occasional bubbles), one with a VGE grade II (1+ bubble per four cardiac cycles), four with a VGE grade III (1+ bubble per cardiac cycle), and one with VGE grade IV (continuous bubbles) (Hess et al., 2021). While no DCS occurred, bubble formation did—further suggesting the importance of carefully balancing the rate of nitrogen off-gassing to the rate of bubble growth at altitude. Moon et al. studied the efficacy of cross corrections for dives performed in a hypobaric chamber after 12–48 hours of acclimatization at constant altitude to allow for AMS resolution. No-stop air dives to a depth of 60 fsw were performed at 8,000 (N = 12 divers) and 10,000 ft (N = 16 divers). Enriched oxygen (Nitrox—35% oxygen) no-stop dives were performed at 10,000 and 12,000 ft (N = 16 and 31 divers, respectively) to a depth of 100 fsw. Nitrox-specific dive tables were determined by first calculating the cross corrected dive depth followed by converting this to the equivalent air dive (EAD) as per the USN Diving Manual (Eq. 3) (Moon et al., 2023; NAVSEA, 2018a). In this equation, D (in fsw) is the converted dive depth and FO
2
is oxygen fraction of the nitrox gas. The calculated EAD is used when planning the exposure time for the dive. In this study, after returning to the surface, all divers were monitored for 12 hours with 2-D echocardiography and for symptoms of decompression illness. There were no cases of DCS and VGE were observed in relatively few individuals. This supports the safe usage of cross correction also for nitrox dives at altitude (Moon et al., 2023).
Cross corrections can convert USN Tables for use at altitude beyond the USN Tables recommended limit of 10,000 ft (NAVSEA, 2018d). However, Bell and Borgwardt argued that they may produce more conservative dive tables than what would be needed to be considered safe by other theories. While these may be acceptable for most recreational divers, this could waste time and resources for commercial or military divers and cause excessive environmental exposure (Bell and Borgwardt, 1976). Bell & Borgwardt (1976) argued that this strategy was best used as a “rule of thumb” since it fails in some scenarios (in some dives with decompression stops) but in a safe conservative direction, and its ease of use may outweigh any extra time or resources used (Bell and Borgwardt, 1976). Cross corrections have been successful both in simulated and real dives at preventing DCS at altitude including outside the originally mentioned limitations of 3,000 m up to 5,200 m (Böni et al., 1976; Shi et al., 2017), albeit with relatively small numbers. Based on current data, cross correction appears to be a valid, straightforward strategy for safe decompression at altitude.
Linear extrapolation of M-values
Another strategy for calculating decompression tables at altitude is through linear extrapolation of M-values (LEM). An M-value is the maximum nitrogen tissue pressure that can be tolerated by a theoretical tissue compartment before bubble formation (Bassett, 2007). M-values are dependent on the half-lives of inert gas exchange in a given compartment and depth (Egi and Gurmen, 2000). The critical supersaturation ratio, which represents the nitrogen pressure the compartments can tolerate relative to the total ambient pressure, is calculated by dividing the M-value by the absolute depth (depth + atmospheric pressure in fsw), which represents the pressure gradient driving bubble formation (Bassett, 2007).
While divers often are above the supersaturation ratio (tissue nitrogen pressure greater than ambient pressure), the critical supersaturation ratio must be surpassed for DCS to occur. Therefore, it is reasonable to base dive tables on keeping a diver under the critical supersaturation ratio for their given altitude (Egi and Brubakk, 1995). LEM uses M-values and tissue tension to build decompression tables based on this theory (Egi and Gurmen, 2000) and is considered to be more conservative than cross corrections (Bassett, 2007).
LEM has also been shown to be a safe decompression strategy at altitude. In Egi’s field trials in 2003, there were no cases of DCS while using linear extrapolation of USN M-values to calculate tables for dives no-stop dives at 3,500 m (Egi, Gürmen and Aydin, 2003).
Constant ratio extrapolation
Constant ratio extrapolation (CRE) is similar to Cross corrections and heavily based on decompression theory espoused by Haldane (Boycott, Damant and Haldane, 1908) but differs in how it calculates decompression stops. For no-stop dives, constant ratio translation (CRT) and CRE are the same. However, CRT is more conservative for dives requiring decompression stops (Bell and Borgwardt, 1976; Egi and Brubakk, 1995). This strategy was used by Böni et al. in 1976 to calculate tables for air dives up to an altitude of 3,200 m and tested up to an altitude of 2,000 m with a maximum depth of 50 m (Böni et al., 1976).
Standardized equivalent sea depth
Paulev & Zubieta-Calleja (2007) introduced another method for converting sea level tables for altitude diving (Paulev and Zubieta-Calleja, 2007). This strategy is based around standardized equivalent sea depth (SESD), which converts actual lake diving depth (ALDD) to its equivalent sea diving depth. This strategy considers the difference in density between fresh water and salt water. SESD is calculated (Eq. 4) by multiplying ALDD by the water density ratio (freshwater density/sea water density) and the nitrogen ratio (Eq. 5) (Paulev and Zubieta-Calleja, 2007).
The SESD factor is equal to the nitrogen ratio multiplied by the water density ratio (Eq. 6). This factor is used to calculate lake ascent rate by dividing the sea ascent rate by the SESD factor. Decompression stages are also recalculated by dividing by the SESD factor (Paulev and Zubieta-Calleja, 2007).
While other strategies may not account for ascent rate (Bell and Borgwardt, 1976), SESD slows the lake ascent rate and modifies the classical decompression stages.
Despite development of these methods, there has been little formal testing of decompression strategies and only limited experience in the field. Thus, precise risks associated with altitude diving are unknown and miscalculations may quickly lead to emergencies even in expeditions led by accomplished and seasoned divers. In a case publicized through National Geographic’s 2020 Documentary “Lost Temple of the Inca” (Aikman, 2020), a diver lost his life during an exploratory dive in Lake Sibinacocha, Peru at 16,000 ft, and due to loss of buoyancy control in the water his dive partner developed severe DCS. The dive was also complicated by a scooter battery failure, premature emptying of gas canisters, development of hypothermia, and other factors, as described by the surviving diver (Cockrell, 2018). The surviving diver was evacuated on horseback, then carried in an inflatable boat over a 17,000 ft mountain pass before definitive treatment could be applied in Cusco for his DCS (Cockrell, 2018). This tragic event emphasizes that planning must be meticulous for high-altitude dives, not only in terms of the approach and decompression procedures but also logistics for exposure and evacuation that may be less of a consideration for dives at sea level.
Logistical Considerations
In addition to acclimation and decompression, several logistical challenges are introduced with altitude dives including travel, exposure protection, and changes to gas maximum operating depths (MODs) and equipment efficacy, making detailed planning and careful attention to task loading mitigation crucial.
Despite available guidance online on flying with scuba gear (Michael, 2018), equipment may be broken or held by security, and last-minute equipment changes may result in use of unfamiliar gear. Exposure protection is necessary, as altitude diving may involve intense sun exposure predive and diving in snowmelt or low temperatures. Sun protection is needed to avoid burns (Leach, McLean and Mee, 1994), and adequate cold protection is important to prevent gear from freezing (Leach, McLean and Mee, 1994), preserve divers’ manual dexterity and cognitive abilities, and reduce DCS risk (Falla et al., 2021; Gerth, 2015). Drysuits are recommended for cold water exposures to decrease conductive heat loss but their use is not without risk (Lundquist, 2023; Partner, 2019). Air in drysuits may leak, and the bubbles maintaining buoyancy in drysuits and buoyancy control devices may be affected by altered pressure differentials at altitude, becoming more difficult to manage at shallow depths (Fig. 1) (NAVSEA, 2018c; NAVSEA, 2018d). This may result in difficulty controlling buoyancy in divers who are used to using their drysuits at sea level. In addition, the sealing pressures of wrist and neck seals may induce paresthesia or syncope in divers inexperienced with drysuit use (Covington et al., 2022). The feasibility of executing diving tables while prioritizing exposure protection must be considered: altitude diving can call for extended decompression times, which must be accounted for in the setting of potential hypothermia and gas management issues (Cross, 1970). Reassuringly, in cases where altitude divers have developed hypothermia, they have recovered with rewarming and able to quickly resume operations (Sahni et al., 1991).
Some diving organizations (such as the British Sub-Aqua Club) also recommend taking weather into account when converting tables for altitude as changes in weather or wind patterns may change ambient pressure further but there are insufficient data to support this (Egi, Pieri and Marroni, 2014). At sea level, there are less drastic variations in barometric pressure but locations at altitude are more susceptible to variation due to weather and seasons. High-altitude pressure variations are also greater in high-latitude regions compared with equatorial regions (West, 1996). From April 2023 to April 2024, Inca Manco Cápac International Airport (located 32 km from Lake Titicaca at 12,552 ft) recorded an atmospheric pressure high of 0.654 atm and a low of 0.641 atm (Wunderground, 2024). If the same variation were also present at Lake Titicaca, the Cross corrected theoretical depth for a dive of 100 ft would be ∼153 ft for the higher pressure and 156 ft for the lower pressure. The no-stop bottom time for both dives would be the same since they both fall within 150–160 fsw on USN Table 9-7 (NAVSEA, 2018b), therefore this would not affect the decompression profile. In most situations, atmospheric pressure variations would not augment decompression and may only realistically need to be considered during exceptionally extreme weather events or at areas of very high latitude.
At altitude, the somewhat decreased ambient pressure at depth leads to increased MODs for oxygen-enriched gas mixtures due to decreased PO2, decreasing risk of oxygen toxicity (NAVSEA, 2018d). Therefore, gases with higher percentages of oxygen can be used deeper at altitude than at sea level. For example, during a 100-ft sea dive at sea level (4 ata) a typical maximum safe oxygen percentage (1.3 atm) would be 32.5%, whereas at 10,000 ft altitude (0.688 ata), the ambient pressure during a 100-ft freshwater dive is 3.64 ata. Thus, the same breathing gas PO2 would be achieved with 35.7% oxygen. This can be important for reducing inert gas uptake and hence decompression stress (Hu et al., 2013; Shi et al., 2017) as well as conserving expensive gas components such as helium.
Many divers rely on dive computers to calculate their decompression. While computers may have altitude settings, these are often less conservative than manual calculation strategies (Buzzacott and Ruehle, 2009). Many of these computers are also restricted to altitudes of 3,000–4,500 m (Egi, Pieri and Marroni, 2014). Lastly, preparatory dives are recommended to develop fitness, resilience, and comfort with cold temperatures, dive routines, and equipment before expeditions (Egi, Gürmen and Aydin, 2003; Leach, McLean and Mee, 1994; Sahni et al., 1991). These also make protocol modifications possible in a safe environment. Physical fitness for the ascent to altitude and dive itself may be improved with respiratory muscle training protocols, which have been shown to increase arterial oxygen saturation during exposure to high altitude, decrease minute ventilation during exercise in both hypobaric and hyperbaric conditions, and increase swimming endurance in working divers at depth (Ray, Pendergast and Lundgren, 2008; Salazar-Martinez et al., 2017). Wheelock et al. (2021) investigated whether a protocol of resistance respiratory muscle training, including four weeks of 30-minute sessions three times weekly (12 sessions total), improved markers of respiratory fatigue in working divers at 55 fsw immediately after exposure to an altitude of 3,658 m. It was found that after completion of the respiratory muscle training protocol, exercising divers reported decreased relative perceived exertion in the final minutes of the dive, and had increased maximum inspiratory and expiratory pressures at depth (Wheelock et al., 2021). This suggests that loaded respiratory muscle training may improve symptoms of respiratory fatigue during dives at altitude and would be a valuable addition to pre-expedition preparation (Wheelock et al., 2021).
Rescue/Continuation of Decompression
When assessing symptoms occurring after altitude dives, it can be difficult to determine whether they are due to AMS, DCS, hypothermia, hypoxia, or other factors. A well-defined safety plan with buy-in from all divers and meticulous equipment planning are of paramount importance: as stated by Sahni et al (1991) prior to their record dive at 14,200 ft in Lake Pangong Tso, “planning was done in minute detail because the final dives would be in areas where no support, supplies, or spares could be expected” (Sahni et al., 1991). Divers must also be aware that additional decompression risk can occur with travel to higher altitudes after completion of a dive (Fig. 2). This risk has been well characterized in guidance for flying after dives, as Divers Alert Network recommends delaying commercial flight for 12–24 hours after recreational dives, though recommendations for military and scientific divers differ (Feldman and Cooper, 2024; RD, 2004). The austere setting of many altitude dive sites also complicates evacuation if divers experience severe DCS or other emergencies, and ground transport or transportation via horseback are likely the only options when accidents occur in locations where air rescue is impossible (Cockrell, 2018). Many recommendations for field management and evacuation of patients with decompression illness at sea level may apply to high altitude, including appropriate positioning during transport, oral or intravenous hydration when possible, and nonsteroidal anti-inflammatory drug administration in the absence of contraindications (Mitchell et al., 2018). In addition, 100% oxygen should be administered in the field, preferably from a rebreather device such as a diving rebreather or circle circuit device meant for first aid, until definitive hyperbaric oxygen treatment may be initiated (Blake et al., 2020). Portable Hyperbaric Units designed for treatment of AMS, HACE, and HAPE are able to inflate up to 2 psi and create a hyperbaric environment compared with the environmental pressure, making them theoretically helpful to facilitate stabilization and evacuation of patients with DCS (Taber, 1990). However, their use for DCS treatment has not been studied. Other possible treatments in the field, such as in-water recompression, have not been evaluated at altitude. Though the Professional Association of Diving Instructors and Divers Alert Network offer specific training and guidance for altitude diving (Soncini, 2020; Vann, 2011), accidents due to equipment failure (Cockrell, 2018; Lundquist, 2023) inexperience, or multifactorial failures (Pacher A, 2017) have been reported.
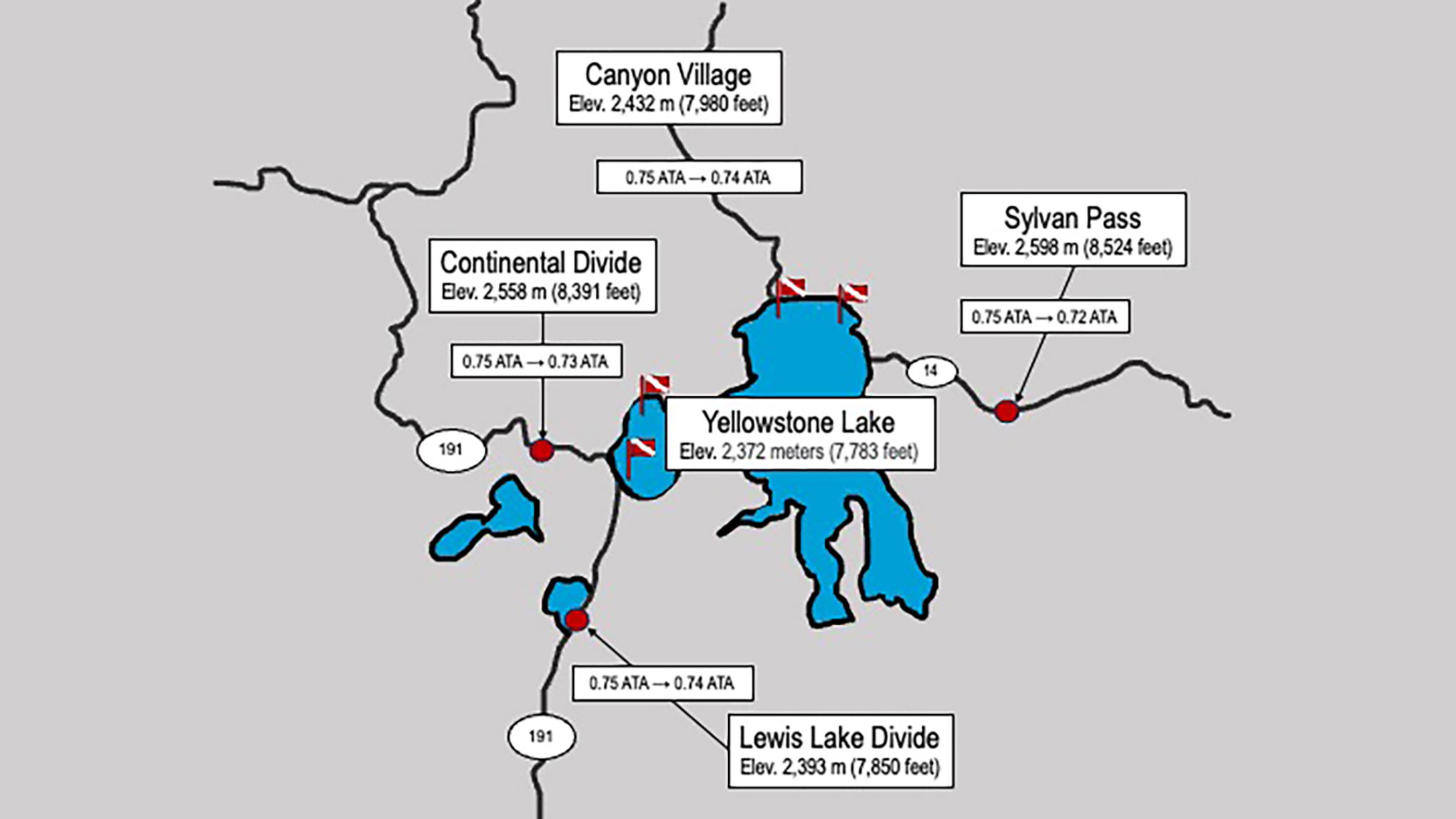
Theoretical paths for a diver after diving in Yellowstone Lake (Elevation 2,372 m). All major roads away from the dive site involve continued decompression and increasing elevation, potentially complicating the evacuation of a patient with DCS, arterial gas embolism, or other medical emergencies postdive. DCS, decompression sickness.
Conclusion
Advances in dive computers with altitude adjustments and publicly available information about equipment and decompression considerations have made altitude diving more feasible. There are several methods that can be used to design safe decompression profiles at altitude. With conservative acclimatization strategies, consideration of environmental challenges, and use of a well-tested decompression profile, the unique risks of altitude diving can be mitigated by recreational divers. However, more research and rigorous testing of these decompression profiles in the field and in a controlled laboratory environment are needed to determine the risks associated with each decompression strategy and to understand the mechanisms by which factors like hydration and acetazolamide use influence diving at altitude and DCS risk.
Footnotes
Acknowledgments
The authors are grateful to the staff of the Duke Center for Hyperbaric Medicine & Environmental Physiology.
Authors’ Contributions
T.L.Y.: Conceptualization, review and editing (equal). K.T.: Conceptualization, review and editing (equal). L.E.H.: Review and editing (equal). R.M.: Methodology (lead), writing—review and editing (equal).
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. Opinions expressed are those of the authors and do not necessarily represent the official views of nor are endorsed by the U.S. Government.
Funding Information
Funding was supplied in part by NAVSEA Contract # N00024-18-C-4318.