
Abstract
Adams, Edmund and Tamlyn Peel. Chronic mountain sickness: A comprehensive review of current management and proposals for novel therapies. High Alt Med Biol. 26:318–327, 2025.—Chronic mountain sickness (CMS) is an acquired condition affecting 5%–10% of high-altitude residents. Lifelong exposure to chronic hypoxia triggers excessive erythrocytosis, resulting in an expanded hematocrit. Patients present with symptoms such as dyspnea, fatigue, and palpitations. Complications such as pulmonary hypertension and heart failure are often fatal. Relocation to sea level remains the only definitive management of CMS but poses an unacceptable personal burden. Long-term oxygen therapy provides symptomatic relief, but dependency issues remain a concern. Phlebotomy reduces hematocrit and offers short-term symptom relief. However, side effects and cultural conflicts continue to pose challenges. Acetazolamide, enalapril, and medroxyprogesterone have lowered hematocrit and alleviated symptoms in human trials. Further research into systemic side effects, application in women, and long-term use is required. Methylxanthines, adrenergic blockers, almitrine, and dopamine antagonists showed promise in murine and/or short-term human trials, highlighting the need for further long-term human trials. Inhibition of hypoxia-inducible factor and Janus Kinase-signal transducer and activator of transcription pathways is currently used to suppress hematocrit in polycythemia vera, demonstrating potential application in CMS. Topiramate may stimulate ventilation via acid-base modulation, thus providing therapeutic value. Similarly, the effect of aspirin and caffeine on ventilation may provide a low-cost, accessible intervention.
Introduction
Chronic mountain sickness (CMS) is a progressive condition unique to long-term high altitude (HA) residents. CMS arises from maladaptive responses to prolonged hypoxia and is characterized by excessive erythrocytosis (EE) (females, hemoglobin (Hb) ≥19 g/dl; males, Hb ≥21 g/dl) (León-Velarde et al., 2005b). Patients present with symptoms such as fatigue, sleep disorders, and muscle weakness (Villafuerte and Corante, 2016). Without appropriate management complications such as pulmonary hypertension and cor pulmonale may prove fatal. There are no current data describing mortality rates in patients with CMS.
There is a lack of acceptable and definitive treatments for CMS. Although relocation to low altitude restores normal physiology, it imposes a huge socioeconomic burden. Phlebotomy offers temporary symptomatic relief, but there is insufficient literature supporting long-term safety and efficacy. Clinical trials of pharmacological options over the past four decades have posed a more hopeful solution. However, many medications lack long-term human trials. Identification of novel therapies is required to advance CMS management.
This article first examines the epidemiology of CMS. Next, it explores the pathophysiology, demonstrating pathways for therapeutic targets. Current management options and their supporting evidence are then reported. Finally, by examining pathophysiological targets and analyzing management of similar conditions, novel therapies are suggested. The article draws from primary research and reviews written over the past century since the first report of CMS by Carlos Monge (1928). The mainstay of current research originates from Peru, Bolivia, and Southwest China.
Epidemiology and Prevalence
As of the latest global estimate in 2021, 81.6 million people live at HA (>2,500 m) (Tremblay and Ainslie, 2021). Five to ten percent of HA residents may develop CMS (León-Velarde et al., 2005). Ethiopia has the largest absolute population living at HA, while Bolivia has the highest percentage. Due to increased migration, the number of maladapted HA residents is increasing, driving the prevalence of CMS.
Altitude is directly associated with CMS prevalence. Wu et al. (1998) reported CMS prevalence across three Tibetan settlements: 1.05% at 2,261–2,980 m; 3.75% at 3,128–3,980 m; and 11.83% at 4,000–5,226 m. The same trend is reported across settlements in the Andes: 5.2% at 3,600 m (La Paz); 6% at 3,800 m (Puno); and 15.4% at 4,330 m in men aged 30–39 years (Cerro de Pasco) (De Ferrari et al., 2014; Monge et al., 1989; Spielvogel et al., 1981). These findings suggest a positive correlation between altitude and CMS. Variables including health care access and diet may confound these results.
Genetic adaptation is associated with reduced CMS prevalence. Populations with ancient HA ancestry, such as Tibetans and Ethiopians, have lower CMS prevalence when compared with relative HA newcomers, such as Andean highlanders and those in Leadville, Colorado (Moore, 2001). In Qinghai, China (4,000 m), CMS prevalence is 1.21% in Tibetans versus 5.6% in recent Han immigrants, showing the protective effect of long-term habitation (Wu et al., 1998). Tibetans and Ethiopians exhibit phenotypes such as suppressed erythropoiesis and lower hematocrit, resulting in low CMS rates (Beall, 2002; Beall et al., 2004). In contrast, U.S. and Peruvian HA populations present with accentuated erythropoiesis, demonstrating maladaptation (Groves et al., 1993; Kryger et al., 1978b ; Vogel et al., 1962).
Pathophysiology
Moderate changes to cardiopulmonary physiology such as pulmonary hypertension, smooth muscle cell hypertrophy, and right ventricular hypertrophy are observed in healthy highlanders (Peñaloza et al., 1960; Qi et al., 2015). In excess, these adaptations become pathological.
Cascade of physiological changes
Primary CMS is associated with idiopathic, centrally orchestrated alveolar hypoventilation; of which etiology is poorly understood. Secondary CMS arises from hypoxia caused by an underlying condition (Villafuerte and Corante, 2016). The resulting reduction in arterial oxygen pressure (Pao2), caused by both primary and secondary CMS, may stimulate EE leading to polycythemia. Conversely, some studies suggest that polycythemia may be the primary driver of CMS, with hypoventilation presenting secondary to this. Genetic factors involving the SNEP1 gene may drive this phenomenon (Ronen et al., 2014; Villafuerte, 2015).
Individuals with CMS do not consistently exhibit raised levels of erythropoietin (EPO), the primary hormone regulating erythropoiesis. This may suggest that polycythemia arises from increased sensitivity to altitude-normal EPO levels or via EPO-independent EE pathways (Villafuerte et al, 2014). However, EPO production is typically suppressed in polycythemia. Thus, the absence of consistently elevated EPO levels may instead reflect inappropriately normal EPO in patients with EPO-dependent polycythemia.
Blood viscosity is significantly increased in patients with CMS compared with those without CMS, which is thought to be at least partly attributed to polycythemia (Stauffer et al., 2020; Tremblay et al., 2019). The symptomatology of CMS may result from inadequate organ perfusion secondary to raised viscosity (Rivera-Ch et al., 2007).
Sex hormones
Pathological androgen levels may trigger upregulation of EPO synthesis and suppression of the intrinsic apoptosis pathway, resulting in raised hematocrit (Gonzales and Chaupis, 2015; Ma et al., 2019). Estrogen may reduce EE by upregulating apoptosis in erythroid progenitor cells and attenuate hypoxia by stimulating ventilation (Azad et al., 2021). Alongside the phlebotomizing effect of menstruation in premenopausal women, sex hormones may contribute to the reduced prevalence of CMS in this demographic (Leon-Velarde et al., 1997).
Ventilation
The hypoxic ventilatory response (HVR) is a reflex responsible for ventilatory stimulation under hypoxic conditions. Desensitization of peripheral chemoreceptors in susceptible people may blunt this reflex, causing chronic hypoxia, thus exacerbating CMS progression (Gamboa et al., 2003a); (León-Velarde et al., 2003a). Murine studies show that increased dopaminergic activity within the carotid body is associated with blunting of the HVR, offering a potential therapeutic target (Pequignot et al., 1987).
An attenuated hypercapnic response may also promote CMS progression. (Fatemian et al., 2003) studied ventilatory responses to hypercapnia under hypoxic and euoxic conditions in three groups: healthy HA natives, sea level (SL) natives, and participants with CMS. They reported a heightened peripheral CO2 sensitivity in the HA group relative to the CMS and SL groups. In addition, hypoxia caused a greater increase in total CO2 sensitivity in the SL group relative to the HA and CMS groups. Reduced peripheral CO2 sensitivity in the CMS group, coupled with a blunted increase in hypercapnic sensitivity during hypoxia, may allude to altered physiology underlying CMS pathogenesis.
Cardiopulmonary complications
Increased blood viscosity contributes to increased pulmonary arterial pressure (PAP), resulting in smooth muscle cell hypertrophy (Cakmak et al., 2013). Over time, this leads to remodeling of the distal pulmonary arterioles (Naeije and Vanderpool, 2013). This impairs efficient gas transfer, accentuating hypoxia and accelerating disease progression in a vicious cycle. Raised PAP increases right ventricular workload, causing hypertrophy and, eventually, congestive heart failure. High altitude pulmonary hypertension (HAPH) and CMS are separate pathologies and can occur independently (Antezana et al., 1998).
Autonomic control of blood flow
Abnormal autonomic control of cerebral and systemic blood flow has been demonstrated in participants with CMS and may cause headaches and dizziness (Hainsworth et al., 2007). Healthy highlanders and acclimatized lowlanders demonstrate raised basal sympathetic drive and muscle sympathetic nerve activity (MSNA) (Lundby et al., 2018). This may compensate for the hypoxic effects of HA. In comparison, patients with mild CMS have reduced basal sympathetic drive, demonstrated by lower MSNA (Simpson et al., 2021). This may be a homeostatic mechanism aimed to balance the negative hemodynamic effects of EE. Alternatively, this phenomenon may occur secondary to reduced baroreceptor sensitivity in participants with CMS, as described by Moore et al. (2006).
Peripheral vascular resistance and vasoconstriction are augmented in participants with CMS during moderate-intensity exercise (Hansen et al., 2021). This coincides with a reduction in stroke volume and a heightened blood pressure response. Mediation of these changes was shown to be independent of sympathetic outflow, suggesting an alternative cause. Despite the altered hemodynamic response, global oxygen delivery is maintained in patients with CMS when compared with those without CMS (Hansen et al., 2021).
Sleep disturbance
Numerous studies report increased rates of sleep disordered breathing and nocturnal hypoxia in patients with CMS (Heinrich et al., 2020; Rexhaj et al., 2016; Young et al., 2024). Reduced hypoxic and hypercapnic sensitivity may be responsible for the highly variable and reduced nocturnal Spo2 (Fatemian et al., 2003). Furthermore, transient nocturnal right-to-left shunt in the setting of patent foramen ovale may exacerbate hypoxia, highlighting the need for increased caution in this demographic.
Management
Management of CMS is divided into preventative, nonpharmacological, and pharmacological treatments.
Preventative
Prevention of CMS can be achieved through the reduction of modifiable risk factors and the transition to a cardiopulmonary protective lifestyle. Changes can be made both at the individual level and at the population level. Epidemiological data indicate that HA communities in the Andes experience the greatest disease burden and thus should be a focus of public health incentives.
The current literature demonstrates that light exercise lowers the risk of CMS development and reduces symptoms. Cornolo et al. (2005) reported that HA athletes have a lower Hb than healthy HA nonathletes. Likewise, Macarlupú et al. (2021) reported a reduction in EE and CMS symptoms following 8 weeks of exercise training (N = 8). However, excessive exercise may exacerbate HAPH, increase pulmonary interstitial fluid accumulation, and exacerbate hypoxia (Stuber et al., 2010; Pratali et al., 2012). Exercise prescription may offer a cost-effective strategy to reduce CMS burden. A retrospective study comparing CMS prevalence with activity level is yet to be conducted.
For centuries, mining has been a major industry in the HA settlements of the Andes. Research has suggested that residing in a mining city may be a risk factor for increased hematocrit (Rivera-Ch et al., 2007). A study by Jefferson et al. (2002) suggested that mining metals, including nickel and cobalt, may stimulate EPO production. Toxic serum cobalt levels were measured in 11 of 21 participants with CMS in Cerro de Pasco but were undetectable in controls at both HA and SL. During this study, the highest ever hematocrit level of 91% was recorded. These exceptionally elevated hematocrit levels were not recorded in 2017 following a governmental clean-up initiative (Sharma et al., 2017). Mining may also predispose to secondary CMS by increasing the risk of conditions such as scoliosis and pneumoconiosis (Vearrier and Greenberg, 2011). Management of this hazard falls to governmental health policy change and clean-up efforts in mining towns.
Other modifiable risk factors for CMS include smoking, indoor fires, obesity, and malnutrition (Penaloza and Arias-Stella, 2007; Pal et al., 2020).
Nonpharmacological
Relocation
The only definitive, long-term management for CMS is relocation to SL. This move must be permanent in severe, life-threatening cases. For moderate cases, periodic travel to SL can sufficiently control hematocrit (Villafuerte and Corante, 2016). Tropical and humid locations increase the risk of recurrent respiratory disease. Relocation causes immediate resolution of breathlessness and poor sleep quality and reduction in alveolar hypoxia. Over 18–23 days, hematocrit returns to normal (Zubieta-Calleja et al., 2007). Pulmonary hypertension persists for 1–2 years after relocation to SL, Sime et al., 1975). On return to HA, symptoms return.
Despite offering an effective treatment option, the socioeconomic burden of leaving behind one’s social network, occupation, and culture poses a major obstacle (Villafuerte and Corante, 2016). As a result, relocation is often considerd unfavourable in many cases of CMS.
Oxygen therapy
Long-term oxygen therapy (LTOT) is commonly used for symptom control in CMS, despite the lack of supportive research. Its use is thus purely based on clinical observation. The aims are to alleviate hypoxia and attenuate polycythemia, thus relieving symptoms. However, patients may become dependent on high oxygen levels, and in the case of therapy cessation, this may result in acute severe episodes of hypoxia (Pal et al., 2020). A retrospective study examining symptomatology, quality of life, and physiological parameters in patients with CMS on LTOT would benefit the literature base.
There is evidence to suggest that intermittent oxygen therapy (IOT) may alleviate symptoms in patients with and at high risk of CMS. A randomized control study at 3,658 m analyzed 263 participants with and without CMS and their responses to IOT over a 30-day window (Feng et al., 2016). They found that IOT seven times a week may be beneficial in participants with severe symptoms. Nocturnal oxygen therapy may attenuate nocturnal suppression of Spo2 and reduce erythropoietic drive, thus improving daytime symptoms. In addition, it would reduce the occupational burden associated with daytime oxygen supplementation. A study investigating intermittent nocturnal oxygen therapy is thus warranted. LTOT and IOT have been associated with social isolation and depression (Koczulla et al., 2018).
Phlebotomy
Phlebotomy is a technique used to treat iron overload and polycythemia. Isovolumic hemodilution (IVHD) aims to reduce Hb and red cell mass while preserving total blood volume. It is the treatment of choice for many HA natives and is widely used to suppress Hb levels (Rivera-Ch et al., 2007). Several studies report that IVHD causes short-term improvement of sleep, cognition, ventilation, cardiac output, and arterial and venous Po2 (Cruz et al., 1979; Klein, 1983; Winslow et al.). In addition, peak oxygen intake was found to be preserved after IVHD in 14 male participants (six with and eight without EE) (Anza-Ramírez et al., 2023).
Sanchez-Azofra et al. (2022) investigated the short-term (48 hours) negative effects of IVHD in six participants with CMS. They reported an increase in oxyhemoglobin desaturation index (p = 0.008) and an increase in sleep time spent with Spo2 < 80% (p = 0.012) but no effect on sleep arousal or efficacy. Clinical observations report concern of rebound Hb levels, exceeding prephlebotomy values (Villafuerte and Corante, 2016). However, these concerns are yet to be reproduced in clinical trials. Other undesirable attributes include iron deficiency anemia, the invasive nature of the procedure, and a cultural aversion to blood removal in a limited number of communities (Smith et al., 2009). Research into the long-term effects of IVHD on hematological and cardiopulmonary parameters, sleep quality, and quality of life would help establish its effectiveness and clarify the safety of the therapy.
Pharmacological
Pharmacological targets for CMS can be categorized into acid-base modulators, direct ventilatory stimulators, hypoxic ventilation response modulators, and EPO inhibitors. Figure 1 demonstrates the chain of events leading to CMS progression and the pharmacological targets of current and novel therapies. Pharmacological management does not require specific equipment or paid medical personnel. Accordingly, the financial burden may be lower than some nonpharmacological options.
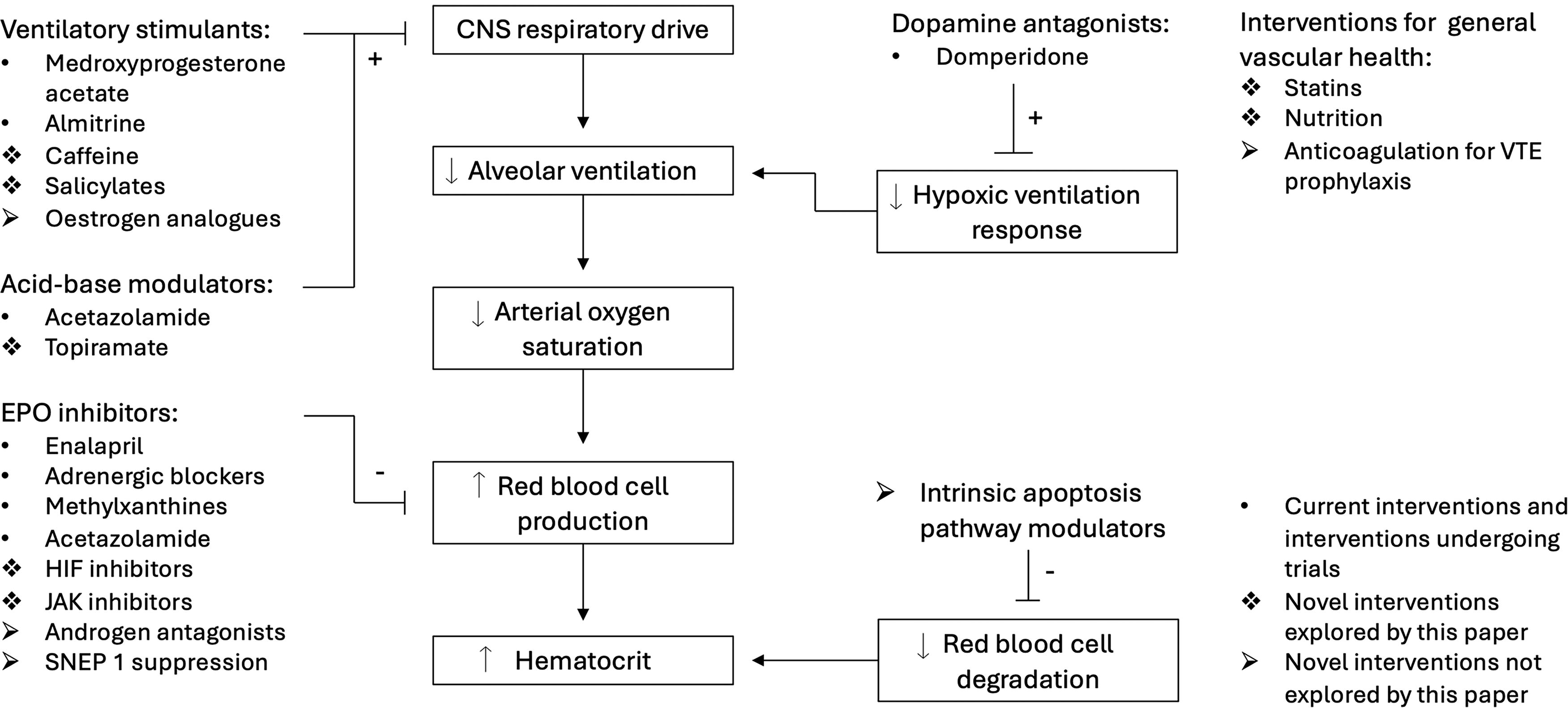
The boxes in this figure depict the cascade of changes leading to chronic mountain sickness progression. Each step in this chain presents a target for therapy. Current medications can be differentiated from novel medications using the key in the bottom right corner. Further candidates for novel therapies not explored by this article are included for completeness.
Acid-base modulation
Acetazolamide
Acetazolamide is widely used in CMS management and supported by a substantial literature base (Richalet et al., 2005, 2008; Champigneulle et al., 2025). It inhibits the enzyme carbonic anhydrase, preventing carbonic acid breakdown and inducing a metabolic acidosis (Farzam and Abdullah, 2024). The resulting pH shift is detected by chemoreceptors, stimulating respiration, raising Spo2, and reducing erythropoietic drive. In addition, acetazolamide may directly inhibit EPO production in peritubular interstitial cells (Rivera-Ch et al., 2007). Other effects include lowering blood pressure via diuresis and reducing intracranial pressure by decreasing cerebrospinal fluid production (Farzam and Abdullah, 2024).
Multiple double-blinded, randomized controlled trials over the past 20 years highlight its efficacy. The first trial (N = 30) compared different doses of acetazolamide with placebo, finding 250 mg/day to be most effective for reducing CMS symptoms over 3 weeks (Richalet et al., 2005). The second study examined 250 mg/day versus placebo over 6 months, reporting fewer polycythemic subjects (p = 0.02), a decrease in hematocrit from 69% to 64% (p < 0.001), and improved pulmonary circulation, with no adverse effects (Richalet et al., 2008). After a 4-week washout, hematocrit returned to baseline.
Sharma et al. (2017) studied the effects of 250 mg acetazolamide (N = 15) when compared with placebo (N = 17), N-acetylcysteine (N = 16), and combination of N-acetylcysteine and acetazolamide (N = 18) groups. They found a 6.7% relative reduction of hematocrit in participants treated with 250 mg acetazolamide, in contrast to a 2.7% reduction in the placebo group (p = 0.048). The combination group yielded no additional therapeutic effect over the acetazolamide group. Monotherapy with N-acetylcysteine did not produce a statistically significant reduction in hematocrit compared with placebo.
The final study assessed acetazolamide for CMS at extreme altitudes (>5,000 m) (Champigneulle et al., 2025). Twenty-seven patients with CMS living at La Rinconada (5,100–5,300 m) were randomized to receive either 250 mg/day (N = 13) or placebo (N = 14) for 9 months. In the treated group, Pao2 increased by 13.4% (95% confidence interval [CI]: 4.3%–22.5%) and hematocrit dropped by 5.4% (95% CI: 8.3%–2.2%). These results demonstrate acetazolamide’s therapeutic effects at extreme altitudes over 9 months. Due to COVID-19 restrictions, the study could not assess long-term use or adverse effects of systemic carbonic anhydrase inhibition.
There is limited research on acetazolamide in women. Initial studies focused on men due to the higher prevalence of CMS in males. Now that the mechanisms and potential benefits are better understood, future research should include women to assess adverse effects in this population and avoid overgeneralizing male-centric data.
CA inhibition affects various systems, including gluconeogenesis, lipogenesis, and ocular pressure, as well as influencing tumorigenicity and virulence (Rahman et al., 2019). Long-term inhibition may thus have adverse effects, which may be elucidated by retrospective studies.
Ventilatory stimulation
Medroxyprogesterone acetate
Medroxyprogesterone acetate is widely used for contraception, amenorrhea, and abnormal uterine bleeding (Abha and Valerie, 2022). Its stimulatory effect on ventilation positions it as a candidate for managing respiratory conditions such as CMS. A controlled interventional study (N = 17) investigated the effects of 10 weeks of medroxyprogesterone acetate (60 mg) on 17 EE patients living at 3,100 m (Kryger et al., 1978a). Mean participant hematocrit reduced from 60.1% (±1.6%) to 52.1 (±1.5%) (p < 0.001), and mean resting ventilation increased from 9.7 to 11.7 l/min (p < 0.001). Furthermore, Pao2 increased and Paco2 reduced. Long-term management over 16 months demonstrated a consistent reduction in hematocrit in 16 of the 17 participants. Despite promising therapeutic outcomes, the potent side effect of diminished libido in men prevented this treatment from gaining popularity. The side effect of reduced libido is less prevalent in the female population, where the medication is commonly used as a contraceptive (Abha and Valerie, 2022). This suggests that the drug may still have application in women of childbearing age who are not planning on becoming pregnant and in postmenopausal women.
Almitrine
Almitrine is a ventilatory stimulant that acts at aortic and carotid chemoreceptors. Its potential to reverse alveolar hypoventilation suggests therapeutic value in the treatment of CMS. To test this hypothesis, a double-blinded, placebo-controlled study was performed in two parts (Villena et al., 1985). The first part investigated the acute effects of almitrine (3 mg/kg) (N = 20) on blood gases, when compared with placebo controls (N = 20). It was reported that 3 hours after administration, there was a significant rise in Pao2 and a reduction in Paco2 in the treated group, with no such change recorded in the control group. The second part (N = 12) investigated the chronic effects of almitrine. Following 4 weeks of almitrine administration (1.5 mg/kg/day), there was a significant reduction in hematocrit (3.5%) alongside unchanged Pao2, Paco2, and PH. Unchanged daytime blood gases alongside reduced hematocrit indicated that chronic almitrine use may induce nocturnal ventilatory stimulation as opposed to daytime stimulation. However, this hypothesis requires further investigation with nocturnal blood gas measurements.
Despite promising results, there is a lack of sufficient follow-up research regarding almitrine. A serious complication of this medication is peripheral neuropathy. This has resulted in the lack of approval of the medication in many nations (Bouche et al., 1989). Future studies investigating chronic usage may be beneficial but must be weighed against the risk of adverse effects.
Hypoxic ventilation response modulation
Dopamine antagonists
Murine studies have demonstrated increased levels of dopamine within the carotid body during chronic hypoxia (Pequignot et al., 1987). This is thought to be associated with attenuation of the hypoxic ventilation response at HA, causing reduced responsiveness to alveolar hypoventilation. Therefore, blockade of dopaminergic receptors in the carotid body, using antagonists such as domperidone, may restore HVR, thus increasing ventilation. This hypothesis is supported by an animal study which reported that domperidone increased hypoxic ventilation and reduced Hb concentration in 18 chronically hypoxic rats (Gamboa et al., 2003b). A human study reported increased hypoxic ventilation responses 1 hour post a 40 mg dose in five patients with CMS at HA, five healthy participants at HA, and five sea-level participants (Leon-Velarde et al., 2003a).
There have been no further human studies, despite positive acute effects on the hypoxic ventilation response. Future long-term studies investigating chronic domperidone use in patients with CMS may determine the longevity of therapeutic response, adverse effects, and symptom control.
Erythropoiesis inhibitors
Enalapril
Angiotensin converting enzyme inhibitors (ACE-Is) were first noted to reduce hematocrit following posttransplant EE, later proving to be effective in treatment (Gaston et al., 1994). ACE-Is act on the renin-angiotensin-aldosterone system, reducing EPO via two pathways. First, suppression of angiotensin II reduces direct EPO production in peritubular renal cells (Pratt et al., 1992). Second, vasodilation enhances renal perfusion, opposing renal hypoxia, thus reducing renal EPO production (Izaguirre et al., 1994).
Murine models conducted in hypobaric hypoxia demonstrate that enalapril suppresses hematocrit (Gamboa et al., 1997). A randomized control study compared a treated group against a placebo group over two years (N = 26) (La Paz, Bolivia, 3,600 m) (Plata et al., 2002). The treated group demonstrated a significant reduction in packed cell volume, Hb concentration, and proteinuria following the 2 years of treatment. Future studies investigating the effects of higher doses may be beneficial.
Methylxanthines
Methylxanthines, also used for posttransplant EE, inhibit adenosine 2 receptors, thus modulating hypoxia-dependent EPO release (Bakris et al., 1990; Fisher, 1988). Through reducing EPO, these drugs limit EE in adults, thus presenting a potential role in CMS management (Fang et al., 1998).
Murine models conducted under hypobaric hypoxia demonstrate that prophylactic pentoxifylline significantly reduces hematocrit (Gamboa et al., 1997). If given following the development of polycythemia, the same response is not elicited. This study may indicate a prophylactic function, but its use in treating developed CMS is unclear. It is plausible that repeat studies using higher doses may yield improved results. This medication class is known for adverse effects, including cardiac arrhythmias, treatment-resistant convulsions, and gastrointestinal upsets (Donegani et al., 2016). There have been no human trials investigating its use for CMS. Thus, future human trials, with careful analysis of adverse effects, may demonstrate therapeutic application.
Adrenergic blockers
The sympathetic nervous system facilitates hypoxic renal EPO release via noradrenergic stimulation of alpha- and beta-adrenergic receptors. Blockade of this pathway with adrenergic blockers may reduce hematocrit in CMS. Murine models conducted under hypobaric hypoxia investigated the use of prazosin over 28 days (Izaguirre et al., 1994). Treated mice demonstrated reduced erythropoiesis and hematocrit from day 3 when compared with controls. It is possible that by decreasing peripheral vascular resistance, prazosin increases renal perfusion, thus countering renal hypoxia and restoring normal renal EPO production. To date, there are no human studies investigating the use of prazosin in CMS.
Studies on the effects of beta blockade on polycythemia are limited to one noncontrolled study including 11 unacclimatized men at HA (4,300 m) (Grover et al., 1998). They concluded that propranolol does not affect the polycythemic response over a 3-week period. There have been no studies on the effects of propranolol on highland patients with CMS.
Novel Therapies
Hypoxia-inducible factor inhibitors
Hypoxia-inducible factor (HIF) is a transcription factor that when stimulated by hypoxia triggers upregulation of multiple target genes. This includes genes associated with EPO, angiogenesis, and metabolism (Masoud and Li, 2015). HIF inhibitors may thus reduce erythropoiesis. A recent study investigated the use of MK-6482, a second-generation allosteric HIF-2α inhibitor, in the treatment of three mice with induced polycythemia and pulmonary hypertension (Ghosh et al., 2021). They reported that treatment with MK-6482 reduces EPO expression, hematocrit, right ventricular pressure, and pulmonary hypertension in all three mouse models. This indicates possible applications for CMS and HAPH. No animal or human studies to date have investigated HIF inhibition in CMS. Future research may take the form of a randomized control study with primary parameters including hematocrit and symptom control and secondary parameters including adverse effects. Downregulation of HIF target genes may cause a reduced rate of wound healing, anemia, and metabolic disturbances (Masoud and Li, 2015).
JAK inhibitors
The JAK/STAT pathway stimulates erythropoietic drive by enhancing the survival and differentiation of erythroid progenitor cells and accelerating hypoxic stress erythropoiesis (Zivot et al., 2018). Inhibiting this pathway may provide a useful target for reducing hematocrit in patients with CMS. The JAK1/2 inhibitor ruxolitinib has been licensed for the management of polycythemia vera and myelofibrosis; conditions characterized by EE (Hatalova et al., 2018; Cakmak and Harrison, 2023). Future research may use murine studies under hypobaric hypoxia to determine efficacy.
Topiramate
Topiramate is currently used in the prophylaxis of migraine and the treatment of convulsions (Mirza et al., 2009). Like acetazolamide, topiramate acts as a carbonic anhydrase inhibitor, inducing a metabolic acidosis by preventing the breakdown of carbonic acid. Thus, it may be hypothesized that topiramate will provide similar therapeutic effects as acetazolamide. There has been no research to date investigating the use of this agent in CMS or polycythemia. Future research may investigate therapeutic potential and compare efficacy against acetazolamide.
Salicylates
Salicylates such as aspirin have known properties of ventilatory stimulation mediated via the medulla. In addition, they are known to increase respiratory center sensitivity to CO2. Thus, it is reasonable to consider its application in the setting of CMS to directly address alveolar hypoventilation. The authors could find no prior mention of salicylate use in CMS regarding ventilation stimulation. This medication would be especially beneficial, due to its low cost and accessibility.
Caffeine
Caffeine is derived from xanthine, the same precursor as methylxanthines. Xanthine has a stimulatory effect on the central nervous system, increasing ventilation (Donegani et al., 2016). It can be hypothesized that due to the chemical proximity between caffeine and xanthine, caffeine may share therapeutic traits such as increasing ventilation and reducing hematocrit. This would make it a possible treatment option for CMS. A study investigating the effects of caffeine on EPO in premature infants demonstrated that caffeine is less potent than theophylline in reducing EPO-dependent erythropoiesis (Fang et al., 1998). However, as caffeine is cheaper, more tolerable, and more easily accessible, it could provide a convenient management option for mild cases of CMS. As little is known about the erythropoietic effects of caffeine, this requires future research. A retrospective cohort study comparing CMS prevalence in daily coffee drinkers compared with noncoffee drinkers would present a cost-effective means to investigate such a relationship. Outcomes would include the ideal doses of caffeine to exert therapeutic effects without negative side effects and whether coffee drinking alone is sufficient to elicit a response.
Limitations
This literature review has investigated potential novel therapies for future research. The array of possible targets and pharmacological agents is extensive, and thus, not all possible options were thoroughly explored. Examples of novel therapies not investigated by this article include estrogen analogs, androgen antagonists, gene therapy targeting the SNEP 1 gene, medications targeting the intrinsic apoptosis pathway, statins, venous thromboembolism prophylaxis, and nutrition (Young et al., 2003; Zhou et al., 2013; Gonzales and Chaupis, 2015; Ma et al., 2019; Bailey et al., 2022). These medications and their respective pathological targets are depicted in Figure 1.
Conclusions
CMS poses an ongoing burden to a significant population of HA natives worldwide. Previous nonpharmacological interventions for this condition, such as IVHD, LTOT, and relocation, pose challenges concerning cultural, economic, and practical considerations. Accordingly, there is a need for cost-effective and accessible pharmacological interventions.
Over the past four decades, research has analyzed the efficacy of several medications through murine and human studies.
This article reviewed the current pharmacological management of CMS to provide a guide for future research. While commending the quality of the research to date, the quantity of studies and pace of progression have been limited. This may be a product of the geographic isolation and minority status of the target populations. Research has frequently failed to progress to human trials following encouraging results from murine studies, as was the case following research on methylxanthines and adrenergic blockers. Accordingly, randomized control trials assessing the effects of these medications against placebo in patients with CMS are needed. Short-term human studies have reported promising effects of almitrine (over 4 weeks) and dopamine antagonists (within 1 hour) on ventilation. Long-term human studies are required to validate findings and explore adverse effects. To date, acetazolamide and enalapril represent the most promising interventions, with long-term human trials reporting reduced hematocrit and improved symptoms. Large-scale retrospective studies investigating adverse effects and patient well-being would be beneficial. Medroxyprogesterone acetate demonstrated promising application, but research was discontinued due to adverse effects on libido. Females experience this side effect to a lesser extent, suggesting possible application in this population.
It is worth noting that nearly all prior studies consist of male-only cohorts. Justifications include the intent to reduce confounders and the increased prevalence of CMS in males. However, there is a need to safely treat the female population, and data obtained from a male-only cohort cannot be accurately generalized to describe the female population. Future phase 3 and 4 clinical trials should include female participants to address this caveat.
Research into novel therapies is required to drive improvement of CMS management. The manipulation of HIF and JAK has emerged as an exciting revelation in the field of HA medicine and polycythemia. Murine studies have demonstrated the antierythropoietic effects of HIF inhibitors, while human studies have shown similar effects with JAK inhibitors, both in the management of polycythemia vera. Subsequently, investigation into the use of these agents in CMS is warranted and may take the form of a randomized control trial. Alternate methods of acid-base manipulation with topiramate may provide therapeutic relief through similar mechanisms to acetazolamide. Murine models using polycythemic mice under hypobaric hypoxia may elicit this. Due to the low economic burden and easy accessibility, ventilatory stimulation with salicylates and caffeine may provide practical forms of therapy. A large cohort retrospective study comparing coffee drinkers with noncoffee drinkers should be used to determine the effects of caffeine in a cost-effective manner. Murine studies should be used to investigate the erythrosuppressive effects of salicylates.
CMS remains a significant challenge to HA communities worldwide. Enhancing current pharmacological management and advancing novel therapies is imperative to improving quality of life and mitigating mortality rates. Moreover, research on occupational risk factors is essential to form the groundwork to inform health policy interventions and preventative measures at the level of the individual and community. This review has identified promising candidates for future pharmacological management and offers specific suggestions to guide the trajectory of research.
Footnotes
Authors’ Contributions
E.A.: Literature review, origional draft writing, revision. T.P.: Supervisor, critical review, editing of the manuscript.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.