
Abstract
Stauffer, Emeric, François Caton, Raphael Marlu, Aurélien Pichon, Landry Seyve, Michael Furian, Aymeric Paillisser, Florence Berquet, Jeremy De Abreu, Blandine Deschamps, Benoit Polack, Philippe Connes, Paul Robach, Stéphane Doutreleau, Julien V. Brugniaux, Samuel Verges, and Benoit Champigneulle. Acclimatized lowlanders exhibit a hypocoagulable profile after a passive ascent at high altitude. High Alt Med Biol. 26:209–214, 2025.
Background:
Discordant results have been previously reported regarding the impact of high-altitude (HA) exposure on coagulation. We aimed to investigate changes in coagulation parameters in lowlanders exposed to HA for 14 days using a combination of dynamic coagulation assays and conventional in vitro tests.
Material and Methods:
We assessed coagulation in 10 lowlanders using whole-blood rotational thromboelastometry (ROTEM), thrombin generation assay (TGA) on poor-platelet plasma, and conventional coagulation tests. Tests were performed at low altitude (LA, 210 m) and at the end of a 14-day sojourn at HA, including passive ascents to 3,800 m for 6 days and then to 5,100 m for 8 days.
Results:
Conventional tests revealed significant changes in coagulation factors and inhibitors after HA exposure, although these changes remained within normal ranges. ROTEM assays demonstrated a delayed clot initiation in EXTEM/FIBTEM, without any alteration in clot firmness, in HA versus LA (p < 0.01). TGA changes showed an increase in time to peak (p < 0.01), a decrease in endogenous thrombin potential (p < 0.05), and a decrease in thrombin peak (p < 0.001).
Conclusions:
We found no evidence of hypercoagulability in lowlanders after a 14-day sojourn at HA. In contrast, dynamic coagulation assays (ROTEM and TGA) revealed a hypocoagulable pattern.
Introduction
Every year, millions of lowlanders travel to high-altitude (HA) areas for professional or leisure activities and are thus acutely exposed to a hypobaric hypoxic environment whose intensity is proportional to the reached altitude (Gatterer et al., 2024). Therefore, understanding the physiological effects induced by this environment on human homeostasis is crucial to prevent acute hypoxia-related diseases such as acute mountain sickness (AMS) or disease exacerbations induced by hypoxic exposure. Based on several reports, a common belief is that HA exposure is associated with an increased risk of thrombotic events (Gupta and Ashraf, 2012; Trunk et al., 2019). However, despite many studies reporting significant changes in hemostasis testing in this context, evidence is lacking regarding a potential procoagulant effect of HA exposure by itself, as emphasized by a recent review (Treml et al., 2022); indeed, HA field studies are subject to potential confounders, such as strenuous physical exercise, that may have by themselves a direct procoagulant effect. Besides, most of the previously published studies have focused on specific steps of the hemostasis process and did not provide an overview of the overall coagulation process (Treml et al., 2022). In the particular HA environment, using global dynamic tests such as viscoelastic hemostatic assays (VHA) that assess the whole-blood dynamic clotting process or thrombin generation assays (TGA) may be informative for detecting changes in the hemostatic balance. Both VHA and TGA have been previously used, most often separately, to assess hemostasis changes during a HA sojourn in lowlanders. Studies using TGA performed after an acute ascent at ∼3,900 m by the same group concluded to a prothrombotic pattern associated with HA exposure (Kicken et al., 2018; Ninivaggi et al., 2015). Two additional studies using VHA at comparable altitudes (5,200 and 5,300 m) yielded conflicting results: one identified a prothrombotic phenotype after a 7-day exposure (Rocke et al., 2018), while the other concluded to a delayed coagulation after a more prolonged HA sojourn (15–17 days) (Martin et al., 2017). Only one study previously used both TGA and VHA to investigate the effect of hypoxic exposure on coagulation, but only over a brief 12-hour period in a normobaric hypoxic chamber and failed to highlight any relevant changes (Schaber et al., 2015). Therefore, in order to better understand the potential coagulation changes induced by a HA sojourn in lowlanders, this study aimed to assess changes in VHA and TGA, as well as in conventional hemostatic parameters, following a 2-week sojourn at HA.
Methods
Study protocol and participants
This study was approved by the ethics committee of the Universidad Peruana Cayetano Heredia (Lima, Peru, IRB number: 00003251) and was conducted in accordance with the Declaration of Helsinki. A complete hemostasis testing panel, including on-the-field rotational thromboelastometry (ROTEM) and TGA, was performed in 10 lowlanders at low altitude (LA, 210 m, Grenoble, France) 1 week before travelling to HA, and then after 14 days of HA exposure, including 6 days at 3,800 m (Puno, Peru) followed by 8 days at 5,100 m (La Rinconada, Peru), where the HA evaluations were performed. This study was a part of a global project (Expedition5300) aiming to investigate the physiological effects of permanent residency at HA (Champigneulle et al., 2023); therefore, part of the data presented here were previously published, as the participants of the present study served as a “sea-level control group” for another study (Champigneulle et al., 2024). Nevertheless, the rationale and HA tests and analyses presented in this study are original and have not been previously published. All participants were researchers involved in the Expedition5300 program, without any HA exposure in the months prior to the study. None had notable medical history (including known prothrombotic disease or bleeding diathesis), and they did not take any regular medications (except low-dose combined estrogen–progestin oral contraceptive for one female). No participants experienced AMS during the HA stay; a few reported only isolated symptoms, such as mild headache, in the initial days of HA exposure. Therefore, subjects were considered acclimatized when the HA evaluations were performed on day 14. None of the participants consumed any medications, except low doses of acetazolamide (for eight of them) in order to prevent AMS. All travel and ascent were passive (plane, then by car), and the subjects, assigned to full-time research activities, did not engage in significant physical activity during the HA sojourn.
Measurements
Hemostasis assays were first performed at LA (210 m, Grenoble, France), then at HA (5,100 m, La Rinconada, Peru), and have been described in detail elsewhere (Champigneulle et al., 2024). Whole-blood ROTEM tests (ROTEM delta, Werfen, Le-Pré-Saint-Gervais, France) were conducted at both altitudes using citrated blood venous samples, following the manufacturer’s instructions; standard assays were used to examine the extrinsic pathway (EXTEM), the intrinsic pathway (INTEM), and the contribution of the fibrinogen to the clot (FIBTEM, by platelet inhibition with cytochalasin D) (Volod et al., 2022). For each ROTEM assay, the two key parameters extracted from the TEMogram (Fig. 1A) were the clotting time (CT, in seconds, indicating the interval from coagulation activation to the detection of a 2-mm-amplitude clot) and the clot amplitude at 20 minutes (in millimeters, signifying clot firmness) (Champigneulle et al., 2024; Volod et al., 2022). At both altitudes, hemoglobin (Hb) concentration and hematocrit (Hct) were determined on-site using a co-oximeter (ABL-80, Radiometer, Copenhagen, Denmark) and the microcentrifuge method, respectively. Platelet count was obtained from a complete blood count at both altitudes. Complementary hemostasis assays were conducted on deep-frozen poor-platelet plasma samples using a STA-R Max 3 coagulometer (Stago, Asnières, France), including prothrombin time (PT), activated partial thromboplastin time (aPTT), fibrinogen activity (Clauss method), and coagulation factors/inhibitors activities (Champigneulle et al., 2024). Thrombin generation assay was performed for nine participants (one missing due to technical failure) on poor-platelet plasma, using a calibrated automated thrombogram assay (Thrombinoscope BV, Maastricht, Netherlands), as previously described (Champigneulle et al., 2024). Lag time (time to start of thrombin generation, in minutes), time to peak (in minutes), peak height (nanomolar), and endogenous thrombin potential (nanomolar per minute) were recorded. Details regarding used reagents for hemostasis and thrombin generation assays are available in our previous publication (Champigneulle et al., 2024).
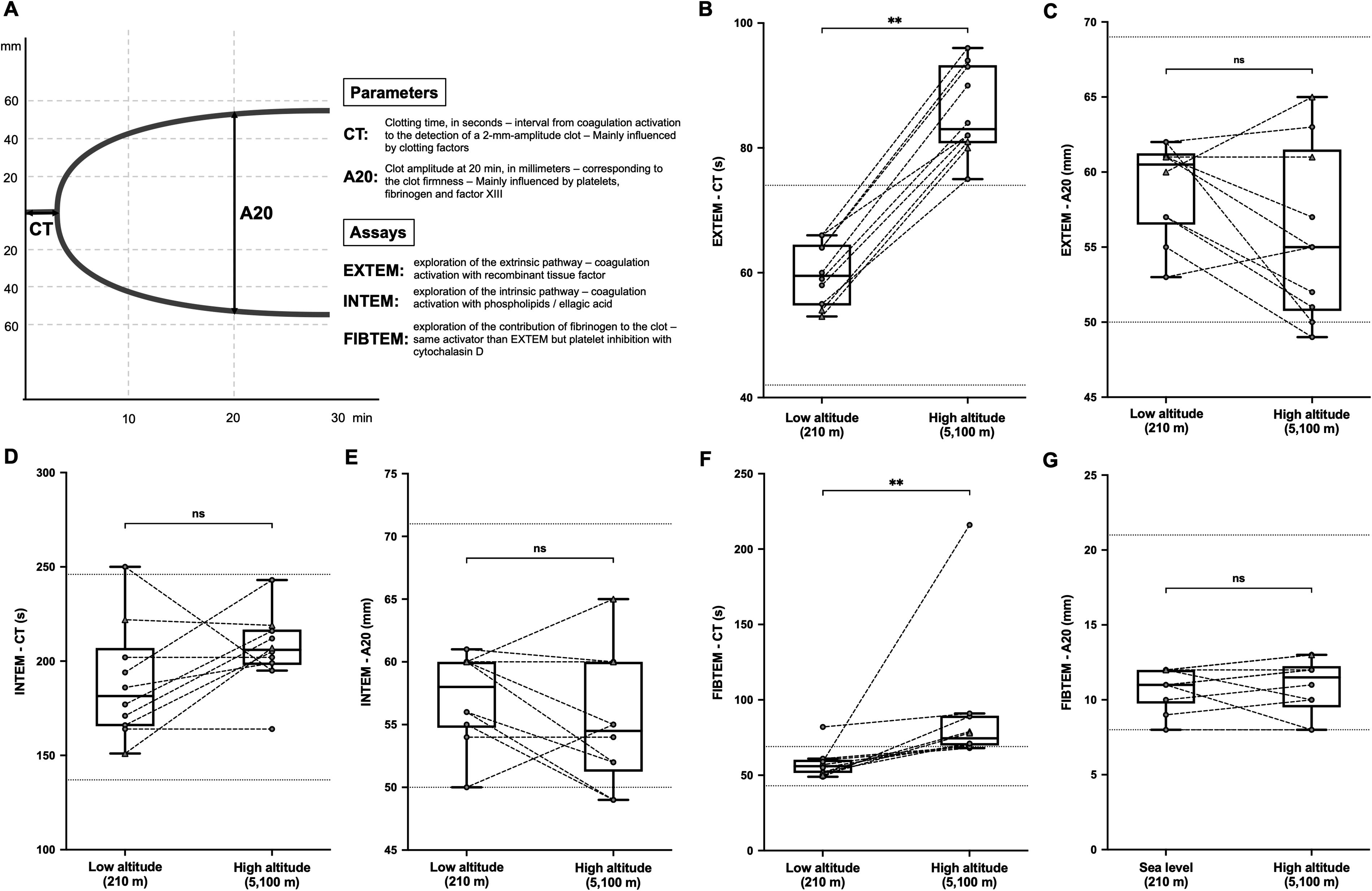
Changes in ROTEM parameters in 10 lowlanders, after a 14-day sojourn at high altitude, in the different ROTEM assays.
At each altitude, special attention was given to the pre-analytical phases, especially regarding the venous blood sampling (Champigneulle et al., 2024). As no participant exhibited a Hct value >55%, no adaptation of citrate volume was required (Kitchen et al., 2021).
Statistical analysis
Categorical data were expressed as absolute count and percentage (%). Continuous data were expressed as mean ± standard deviation or median (25th–75th percentiles), depending on data distribution (assessed using the Shapiro–Wilk test). Changes in continuous variables between LA and HA were assessed using paired Student’s t-tests or Wilcoxon signed-rank tests, as appropriate. All tests were two-sided, and a p value <0.05 was considered statistically significant. All statistical analyses were performed using R software (version 4.4.1) and GraphPad Prism (version 10.2.3).
Results
Table 1 presents the general characteristics of the 10 lowlanders. HA exposure predictably led to elevated (Hb) and Hct levels and decreased oxygen saturation. After 14 days at HA, participants showed a significant increase in PT and aPTT, as well as a slight, albeit significant, increase in fibrinogen level. Clotting factor and inhibitor dosages revealed a slight but significant decrease in factor V, protein C, and free protein S, balanced with a slight significant increase in factor IX and XI (Table 2), although individual values mostly remained within the laboratory limits at both altitudes (individual data not shown). Results from the different ROTEM assays (Fig. 1) highlighted a delayed clot initiation in EXTEM/FIBTEM assays at HA (Figs. 1B and 1F), with no change in clot firmness at 20 minutes (A20, Figs. 1C and 1G) and similar INTEM values at both altitudes (Figs. 1D and 1E). The results of the TGA are presented in Figure 2. After the 14-day sojourn at HA, lowlanders exhibited a hypocoagulable TGA pattern compared with the LA evaluation (Fig. 2A), including a longer time to peak (Fig. 2C) and a decrease in thrombin peak and endogenous thrombin potential (Fig. 2D and 2E), without any delayed lag time (Fig. 2B).

Changes in thrombin generation assay pattern and parameters in 10 lowlanders after a 14-day sojourn at high altitude.
Demographic, Hematological Characteristics and Conventional Coagulation Tests at Low Altitude and after a 14-Day Sojourn at High Altitude
Continuous data are reported in mean ± SD or median (25th–75th percentiles). Categorial data are reported in absolute count and percentage (%).
LA, low altitude; HA, high altitude; SpO2, transcutaneous oxygen saturation; (Hb), hemoglobin concentration; Hct, hematocrit; PT, prothrombin time; aPTT, partial thromboplastin time.
Plasma Levels of Clotting Factors and Inhibitors Measured at Low Altitude and at High Altitude after a 14-Day Sojourn at High Altitude
Data are reported in mean ± SD.
LA, low altitude; HA, high altitude.
Discussion
In this brief report, we found no evidence of a procoagulant pattern in a group of 10 lowlanders following a passive exposure to HA for 14 days. Conversely, dynamic tests performed in the field in whole blood (ROTEM) or later from frozen poor-platelet plasma (TGA) indicated a potential hypocoagulant profile in comparison to the baseline LA tests. To the best of our knowledge, no previous field study reported such a large panel of coagulation testing in lowlanders exposed to such high altitude for several days (Treml et al., 2022). Studying the components of the hemostatic system, including the coagulation phase, remains a challenge in the HA environment, where VHA, which is easy to perform in the field, represents a useful test. Field studies are subject to external confounders such as cold, physical activity, or differences in terms of hypoxic dose (time and altitude), which may limit the comparison of our results with previous studies. Our results are (at least partially) concordant with some recent VHA studies performed in lowlanders under experimental laboratory conditions or in the field. In a strictly controlled study performed in 12 healthy female participants, Kammerer et al. (2023) did not highlight any change in VHA parameters during a 4-day exposure to a simulated altitude of 3,500 m. Consistent with our findings, Martin et al. (2017), using thromboelastography, reported a slowed coagulation (including a delayed clot initiation and an increased clot formation time without any change in maximum clot strength) in lowlanders exposed to a similar altitude for a similar duration. Conversely, Rocke et al. (2018), using ROTEM after a 7-day sojourn at 5,200 m, found a significant increase in clot firmness and concluded to a procoagulant pattern at HA, despite a paradoxical associated delayed CT. Finally, the difference in VHA patterns observed between these different studies conducted at ∼5,000 m could be explained by different exposure times and the possibility of an evolving coagulation pattern over time, as suggested by a recent experimental study conducted in rabbits (Zhong et al., 2022). Longitudinal studies aiming to assess changes in coagulation patterns over the exposure duration at a stable altitude are still lacking in order to confirm similar findings in humans.
Using TGA conducted in poor-platelet plasma, we also reported a clear hypocoagulant pattern in HA versus LA. Here again, comparing this finding with previously published data is challenging due to methodological differences. Previous reports on thrombin generation were conducted at lower altitudes with a shorter exposure time, investigated the combined effects of both altitude and exercise, or measured thrombin generation in whole blood or with different concentrations of activator (Kicken et al., 2019, 2018; Ninivaggi et al., 2024, 2015). Nevertheless, in these studies conducted between ∼3,400 and 3,900 m, TGA was almost unaffected by altitude exposure alone when performed in poor-platelet plasma or showed a hypercoagulable pattern, especially when conducted in whole blood samples (Kicken et al., 2018; Ninivaggi et al., 2015).
Our study had some limitations. Firstly, the investigations were conducted in a limited sample, and the unbalanced sex ratio did not allow the assessment of potential sex differences (Kammerer et al., 2023; Ninivaggi et al., 2024). Moreover, a potential confounding effect of acetazolamide uptake could not be totally excluded even if acetazolamide seems to have no effect on ROTEM parameters (Agbani et al., 2020). Last, we were not able to study the contribution of the platelets to the hemostasis process, as platelet reactivity has been shown to be divergently impacted by HA exposure (Kicken et al., 2019, 2018; Ninivaggi et al., 2024; Rocke et al., 2018).
Conclusions
The present study does not support a procoagulant pattern in lowlanders after a 14-day exposure to HA. Moreover, dynamic coagulation assays suggest hypocoagulant features compared to baseline. Further studies are needed, especially to assess the potential temporal changes in coagulation patterns over time during a HA sojourn.
Footnotes
Acknowledgments
The ROTEM® delta analyzer used for this study was kindly provided by Werfen (Werfen, Le-Pré-Saint-Gervais, France). The sponsor had no further involvement in any steps of the study (study design, collection, and analysis of the data or writing of the article). The authors would like to thank the study volunteers for their commitment and time invested in this study, and the medical students of the scientific association of medical students from the Altiplano University (Puno, Peru) who actively contributed to the research program implemented in La Rinconada.
Authors’ Contributions
E.S.: Conceptualization, methodology, investigation, and writing—original draft and supervision. F.C.: Conceptualization, methodology, resources, and writing—review and editing, funding acquisition. R.M.: Conceptualization, methodology, validation, resources, and writing—review and editing. A.P.: Conceptualization, investigation, and writing—review and editing, supervision. S.L.: Methodology, validation, resources, and writing—review and editing. M.F.: Conceptualization, investigation, and writing—review and editing. A.P.: Conceptualization, investigation, and writing—review and editing. F.B.: Conceptualization, investigation, and writing—review and editing. J.D.A.: Conceptualization, investigation, and writing—review and editing. B.D.: Conceptualization, investigation, and writing—review and editing. B.P.: Conceptualization, methodology, resource, and writing—review and editing, funding acquisition. P.C.: Conceptualization, methodology, and writing—review and editing, supervision. P.R.: Conceptualization, methodology, and writing—review and editing, supervision. S.D.: Conceptualization, methodology, and writing—review and editing, supervision. J.V.B.: Conceptualization, investigation, methodology, and writing—review and editing, supervision. S.V.: Conceptualization, methodology, investigation, and writing—review and editing, supervision, project administration, funding acquisition. B.C.: Conceptualization, methodology, formal analysis, investigation, visualization, and writing—original draft, supervision, and project administration. All authors gave final approval and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Grenoble Alpes University foundation, the “Fonds de dotation AGIR pour les maladies chroniques,” the Air Liquide Foundation and by the French National Research Agency (ANR-12-TECS-0010) in the framework of the “Investissements d’avenir” program (ANR-15-IDEX-02).