
Abstract
Developing effective anticancer treatments is a particular challenge, as agents must contend with not only the target cellular biology, but also with the complex tumor microenvironment. Here we discuss various in vitro strategies that have sought to address this issue, with a particular focus on new methodologies that utilize clinical samples in basic research and their application in gene therapy and virotherapy.
Introduction to the Disease
C
The disparity between the preclinical success of novel cancer therapeutics and high failure rates in the clinic suggests that the models by which we test such therapeutics need improvement. 5 Given the heterogeneity of cancer cells in vivo and the complexity of the tumor microenvironment, it is perhaps understandable that current models—such as in vitro studies in cell lines, mouse models, or xenotransplantation—are often too reductionist and fail to accurately predict the utility of a given therapeutic. It is imperative that increased focus on developing better therapeutics must be complemented by development of more accurate and predictive preclinical models.
Here we review in vitro preclinical human tumor model systems and how they can be refined for better predictive value in the context of cancer gene therapy. In particular, we highlight the growing use of systems based on ex vivo culture of primary human tumor biopsies obtained from patients undergoing biopsy or surgical resections. These culture systems can accurately recapitulate the multicellular architecture of human tumors, including the matrix and both the malignant and normal cellular compartments. However, logistical difficulties in obtaining, maintaining, and working with primary samples can make such experimentation difficult. We assess whether the scientific and predictive benefits outweigh the procedural challenges in using this type of preclinical assay.
Translational Studies Using Monolayer Cell Culture
Cancer cell lines derived from human tumors have been adopted as one of the most fundamental tools in cancer research. 6 They can be easily maintained, stored, and shared between different laboratories, and many well-characterized cell lines are now available. The NCI 60 cell platform, a collection of 60 cells representative of 9 prevalent cancer types, 7 has been used to screen over 100,000 8 potential anticancer compounds to date and has led to several important insights into cancer biology, including the discovery of P-glycoprotein expression in cancer cell lines, elucidating a major mechanism of drug resistance. 9,10
Unfortunately, the efficacy of anticancer agents on tumor cell lines in vitro shows little correlation with success in the clinics. 5 There could be many reasons for this, including phenotypic drift of tumor cells during extensive in vitro passaging and a fundamentally different tumor microenvironment in vivo. For example, the proportion of cells that are typically proliferating in vitro is higher than is normally seen in solid tumors in the clinic, 11 correlating with increased sensitivity of cancer cell lines to antiproliferative agents. 12 –14 Factors such as cell cycle discrepancies may be particularly important for cancer gene therapy, 15 where agents are often designed to exploit specific tumor-associated molecular changes that might be more prevalent in defined cell lines than in clinical disease. Similarly, the bourgeoning field of oncolytic vaccines depends on microenvironmental components that are not represented in simple cell line culture. 16
One approach to address this has been to provide more microenvironmental context by growing tumor cell lines with fibroblasts, often in a raft configuration. 17 Such systems show greater differentiation and three-dimensional (3D) structure, although the use of tumor cell lines would still be prone to in vitro adaptation. In other studies this has been addressed by the development of early passage cultures of primary tumor tissue, 18 including production of cell lines from disaggregated tissue samples. 19,20 Such approaches have the advantage of minimizing phenotypic drift, although there is still a loss of microenvironment and a natural selection of the most rapidly proliferating cells. 21,22
Although in vitro cell culture allows the precise study of clonal cancer cells in isolation, it is difficult to recapitulate the 3D nature of cancers and the heterogeneity of surrounding cells. Within solid tumors, nontransformed cells such as fibroblasts and immune cells provide a complex microenvironment, including substantial extracellular matrix, that generally supports tumor growth. 23 Such nontransformed cells can dramatically alter tumor biology and thereby influence the efficacy of therapeutic intervention. 24 For example, extensive hypoxic cores hinder access of chemotherapy 25 ; thick extracellular matrices protect tumors from radiotherapy 26 ; and localized immunosuppressive networks subvert effective antitumor immune responses. 23 These factors cannot be studied in cultures of isolated primary tumor cells and cell lines, and for better modeling of the human tumor there is a need to generate more representative in vitro/ex vivo model systems. Numerous strategies have been employed to try and achieve this, and they will be discussed below.
The Use of Cell Spheroids as Preclinical Models
In recent years research has highlighted the discrepancies in cancer cells studied in 2D versus 3D systems. 27 Considerable differences have been observed in migration potential, alongside receptor, and gene expression of tumor cells grown under these two conditions (reviewed in Pampaloni et al. 28 ), with the difference in gene expression alone estimated to be as high as 30%. 29 Consequently, the influence of the 3D microenvironment on the biology of tumors deserves careful consideration when evaluating a therapeutic intervention, particularly a gene therapy that is designed to target a specific phenotype. The spheroid model has emerged as an important technology to study the 3D nature of tumors and now represents an attractive model system in which to screen drugs and experimental gene and cell therapies. 30,31
Providing 3D interactions and architecture
Growth of spheroids of different sizes can replicate distinct physiological conditions that are found in tumors; small spheroids (200–500 μm in diameter) recapitulate some of the cell–cell interactions found in 3D tumor microenvironments and develop oxygen and nutrient gradients, while larger spheroids (>500 μm in diameter) can acquire secondary necrosis. 32 These differential gradients of oxygen become of particular interest for evaluating therapeutics that can be influenced by regions of hypoxia such as radiotherapy or replicating viruses. 33,34 Similarly, 3D spheroids generate regions of tumors with different proliferative indexes, which can be used to evaluate therapies that solely target highly proliferating cells. 35,36
Spheroids containing multiple cell types that recreate tumor microenvironments
Stromal cells are increasingly recognized for their central roles in tumor biology and can be easily incorporated into growing spheroids. Multicellular spheroids were used effectively by Muthana et al. to evaluate an oncolytic adenovirus controlled by a hypoxia promoter. 37 The authors used the multicellular spheroid model to demonstrate that macrophages could act as vectors for adenovirus, with macrophages migrating into the hypoxic regions generated by tumor spheroids and allowing hypoxia-driven replication of adenovirus. Similarly, by incorporating immune cells into the methodology, spheroid cultures are emerging as tools for evaluating immune-based therapeutics. 38
Although this approach provides a more relevant microenvironmental context, the use of extensively passaged cancer cell lines as the cancer component of spheroids may still foster unwanted clonal dominance and in vitro phenotypic adaptations. One intriguing approach to address this has been to use primary multicell-type “organotypic” spheroids. 39,40 This approach has arguably much greater clinical relevance and has been of particular use in assessing the replication and spread of oncolytic viruses.
Tumor Slice Technology for Ex Vivo Culture of Human Tumor Biopsies
Tumor slice models represent an approach that, in principle, captures all cell types in the tumor and maintains their 3D architecture. By generating fine slices or discs of primary tumor samples (typically ∼5 mm in diameter by ∼0.3 mm width), this approach allows freshly resected clinical samples to be maintained ex vivo for several days, within an adequately oxygenated environment. Additionally, using thin slices maximizes the number of samples that can be generated from a single tumor specimen. Given that human tumor collection is a complex process, requiring considerable coordination and cooperation between regulatory, medical, and scientific groups, maximizing the number of studies that can be performed from a single human tumor sample becomes important.
The tissue slice model is by no means a new technology. Indeed, the great potential of this model was illustrated early in the 19th century by Otto Warburg and later by Hans Krebs, where the usage of ex vivo liver slices facilitated fundamental research into cellular metabolism. 41 Since this early work, the tissue slice method has been used extensively in the study of liver metabolism, proving to be a key tool in drug testing and predicting liver toxicology from new drugs. 42 Refined protocols have allowed tissue slices to emerge as a means to assess efficacy and potential toxicity of new therapies in other areas of research. 43 Ex vivo slice protocols have been established for short-term cultures of tumors 44 and have been utilized effectively in a wide range of cancer types, including lung, 45,46 breast, 44,47 colon, ovarian, 48 and head and neck. 49
Preserving the 3D tumor architecture
By maintaining tissue architecture, slice methodology can allow the study of interactions that require a 3D and multicell-type environment. It also provides a more realistic assessment of therapeutic agents that are limited by barriers found within the tumor microenvironment. Dong et al. used the slice technology as a means to assess the efficacy of a nanoparticle treatment for nonsmall cell lung carcinoma. 46 Having previously demonstrated inhibition of telomerase activity through nanoparticle delivery of antisense oligonucleotides in a cell culture model, 50 tissue slices were used to successfully validate pharmacological activity in a 3D context where they reported significant reductions in telomerase activity.
A recent study by Dean et al. used thin slice technology to study a monoclonal antibody antagonistic to EMMPRIN—the extracellular matrix metalloproteinase inducer. EMMPRIN has been implicated in tumor–stromal interaction and could have key functions overlooked in traditional cell culture or immune-compromised mouse models. In their ex vivo study of head and neck squamous cell carcinoma, Dean et al. showed a significant effect in 58% of patient samples versus only a 33% response rate exhibited by Cetuximab, highlighting the promise for this new therapeutic. 49
The role of fibroblasts in the tumor microenvironment
Thin slice technology aims to preserve tumor stroma and capture the real tumor microenvironment. By doing so, this method would seem well suited for studying the associated stromal constituents. Tumor-associated fibroblasts can facilitate tumor progression through production of growth factors and pro-angiogenic agents such as VEGF 51,52 and, as such, can influence the efficacy of cancer therapeutics. 53 In a recent article by Sonnenberg et al., significant differences in drug sensitivity were shown between fibroblasts isolated from lung and breast cancer tissue and studied in isolation, compared with the same cancer-associated fibroblasts tested in the 3D microenvironment of the ex vivo tumor slice. 54 In short-term exposure to paclitaxel, it was shown that while purified cultures of fibroblasts appeared chemotherapy resistant, fibroblasts in the microenvironment of the tissue slice from the same patient were killed in a pattern similar to that of the tumor cells. The same experiments performed in lung cancer samples confirmed the discrepancies between cultured fibroblasts and those in the tumor microenvironment. Here, the isolated fibroblasts in culture revealed a population of highly proliferative cells compared with the low proliferation of fibroblasts in the tumor microenvironment: a difference reflected in sensitivity to cisplatin. Such examples demonstrate the influence of the cancer cells on the surrounding stromal cells, once again emphasizing the importance of using models that accurately recapitulate the tumor microenvironment to better test anticancer therapeutics.
The impact of tumor-associated immune cells
The slice method can also facilitate the study of immune cells within the tumor microenvironment. It is now accepted that the tumor microenvironment is generally immunosuppressive and protumorigenic. 23 Immune cells that may mediate antitumor immunity are often subverted to produce pro-proliferative and angiogenic mediators such as TGF-β, IL-10, and VEGF. Additionally, tumors actively recruit and promote proliferation of suppressive cells such as regulatory T cells, myeloid-derived suppressor cells, and tumor-associated macrophages that secrete inhibitory cytokines to suppress antitumor immune responses and even promote resistance to therapy. 55 One such inhibitory cytokine is TGF-β, which has been studied extensively for its ability to attenuate antitumor immune responses. 56 In a recent study by Joffroy et al., the action of TGF-β was shown to be an important consideration for anti-estrogen treatments in breast cancer. 47 Using the ex vivo slice model, they demonstrated that anti-estrogen therapy can increase FoxP3 expression and subsequent TGF-β production. This TGF-β was proposed to decrease cytotoxic effector function, thereby elucidating a potential immunosuppressive mechanism that would augment resistance to treatments such as Tamoxifen.
The use of the slice method for the study of the immune system has inherent limitations. With no blood flow or active lymphatic system, tissue slices do not facilitate studies of cells that require real-time education in the thymus or antigen-presentation in draining lymph nodes. Nevertheless, thoughtful use of the technique can allow for informative studies. Utilizing the preserved 3D architecture, Salmon et al. recently documented the localization of CD8 effector T cells within tumor tissue. 57 Tumor-infiltrating lymphocytes incubated with tumor slices were shown to have attenuated migration to tumor cells, instead being localized principally to stromal compartments as a result of the matrix architecture surrounding the tumor.
While the study of immune cells using the slice method is still in its early stages and will most likely be quite restricted in scope, it could provide an excellent technique for investigation for populations of tissue-resident immune cells. Of particular interest could be the myeloid populations such as tumor-associated macrophages, mast cells, and myeloid-derived suppressor cells, which should be very amenable for short-term ex vivo culture.
A tool for personalized medicine
Differential response to anticancer therapeutics between patients can be explained in part by the vast heterogeneity that exists between cancers, even within the same tumor type. Such heterogeneity was illustrated well by van der Kuip et al., who used the tissue slice approach to evaluate the effect of Taxol on slices of tumor tissue resected from 22 patients with breast cancer. 44 Taxols represent an important cancer therapeutic, constituting a first-line treatment for different types of cancer, including breast cancer; however, the authors report significant variability in the efficacy of the drug in these patient tissues, with only 60% of samples exhibiting a significant effect. In another study, the level of COX-2 was measured in tissue slices from patients with liver cancer. 58 Significantly elevated COX-2 levels were observed in many tissue slices and the levels intensified during culture, prompting treatment of slices with the selective COX-2 inhibitor Meloxicam. Comparison with normal liver tissue showed selective activity in the malignant tissue only, where Meloxicam was able to induce apoptosis in all patient samples. Such results illustrate the need for therapeutics that more effectively target a larger proportion of patients with cancer.
Slice technology is an ideal tool for personalized medicine. A key advantage of this technique is its economical use of tissue: a small tumor biopsy or resection can provide multiple tissue sections for experimentation. In an idealized situation, tumor specimens from patients could be tested for key oncogenes and signaling molecules, with a range of therapeutics against these targets tested in slice culture to discover the best drug for the patient. Such an approach was envisaged by Vaira et al., who evaluated key oncogenic signaling pathways in samples from colon, lung, and prostate tumors. 45 Focusing on the PI3K/Akt signaling status within these samples, Akt was shown to be in a constant activation state and, as such, treatment was administered in the form of a PI3K inhibitor. By tailoring the therapeutic based on functional evidence of aberrant signaling within the samples, tumors in culture exhibited reduced phosphorylation of Akt and, accordingly, reduced proliferation and tissue viability.
A preclinical model for testing oncolytic virotherapy
Thin slice technology is a relatively new tool for cancer research, and few groups have so far utilized this method to explore the activity of conventional anticancer treatments. In contrast, virological research has been quick to exploit the many advantages of this ex vivo system, which holds much promise for the field of oncolytic virotherapy—an exciting approach to cancer therapy using viruses that selectively replicate within tumor cells. 3 Adenoviruses are an attractive choice for this because they cause only mild disease, can be produced in high titer, are genetically stable because of a high fidelity proof-reading polymerase, and are amenable to genetic engineering. However, in developing oncolytic adenovirus strategies, species selectivity of adenovirus replication has led to difficulties in studying oncolytic human adenoviruses in classical mouse tumor models. This largely restricts in vivo study to human tumor xenografts in immune-deficient mice. 59 Here, the tumor slice method has proven itself to be ideal with defined assays existing for virus testing in slice cultures (Fig. 1), 60,61 and a number of tumor tissues being shown to be permissive to adenoviral replication, including breast, 62,63 glioma, 64 ovarian, 60 and pancreas. 65

Manual tissue slice methodology.
A major objective within oncolytic virotherapy is ensuring specificity of viral replication, limiting activity to target tumor cells in order to improve efficacy and reduce unwanted toxicity. 66 Akin to the original usage of slice culture for evaluating liver toxicology, the ex vivo slice method using liver metastases provides the ideal format to assess the specificity of oncolytic virus and demonstrate a “tumor on/liver off” expression profile. 60,61 In one such study, an adenovirus serotype 5 (Ad5)-based oncolytic virus was created by placing control of viral transcription under the COX-2 promoter; comparison of infection with normal liver and cancerous tissue revealed restriction of replication to cancerous tissue. 60 A similar study extended such work to a preclinical setting wherein a selection of adenoviruses under a range of cancer-associated promoters could be tested in ex vivo slices from patients, paving the way toward individualized medicine. 62 In a small preclinical study, Stoff-Khalili and colleagues showed that, while most of their breast cancer patients showed efficient and tumor-selective replication under the CXCR4 promoter, one in eight experienced better replication using the EGF-2 promoter. 62 In a similar study, Zimmerman et al. tested measles virus strains in tissue slices generated from a number of patients for their ability to infect cancerous tissue, highlighting the variation of infection observed across different virus strains in different patients. 67 Such studies illustrate that the ex vivo system is well suited to assess the utility and safety of oncolytic virotherapy in patients and further can facilitate a pretreatment screen for selection of the best therapeutic for the individual (Fig. 2).
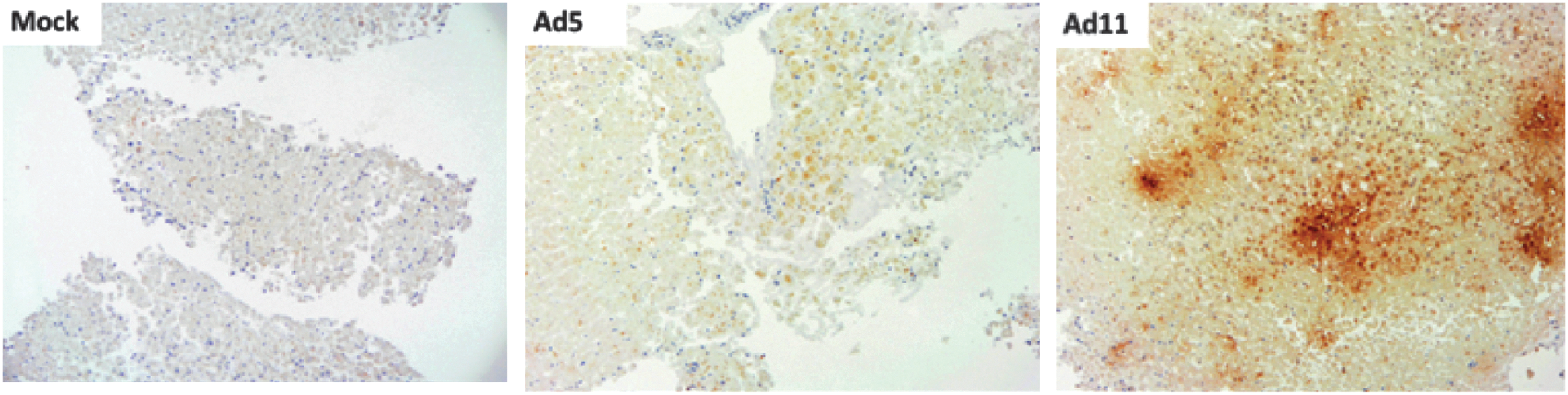
Infection of human colorectal tumor slices using wild-type adenovirus serotype 5 (Ad5) and 11p (Ad11). Virus infection and replication was assessed by staining with antihexon antibody to indicate synthesis of late viral protein.
The conditional replication attributed to oncolytic adenovirus relies on the selective infection and replication within tumor cells. For Ad5-based vectors, efficacy of infection can be influenced by the expression of the major uptake receptor, coxsackie and adenovirus receptor (CAR) on tumor cells. Such is the importance of CAR that evidence of decreased receptor expression on certain tumor cells correlates with poor infection. To circumvent this issue, Ad5-based vectors have been engineered with altered tropism to enable infection mediated through other prominent receptors expressed on tumor cells. One such strategy was used by van Geer et al.: retargeting adenovirus to infect via epherin-A2 to counteract low CAR expression in pancreatic tumor samples. The authors demonstrated successful infection of pancreatic tumor slices via epherin-A2 even in patient tumors with low CAR expression. 68 In a similar study by Pennington et al., a chimeric fiber protein was generated with an Ad3 knob domain, redirecting infection of breast cancer tissue slices from CAR to CD46. 69
The tumor microenvironment is thought to contain physical barriers to the spread of virotherapy. A complex extracellular matrix surrounding the tumor microenvironment can restrict viral spread and thereby reduce efficacy. 70 To overcome the issue, strategies are now being explored to encode soluble mediators such as relaxin within oncolytic viruses to enhance viral spread through controlled degradation of the extracellular matrix. 71 As such, encompassing a 3D model that maintains the restrictive environment of the tumor provides a far more stringent test of viral efficacy and the effects of enhanced tissue penetration. By using a GFP adenovirus, Rots et al. directly visualized the extent of penetration of their virus by looking at cross sections of the tumor slices. 61 In a novel approach, Mühlebach et al. sought to utilize the tumor microenvironment to generate a conditionally replicating oncolytic virus that is dependent upon the milieu of enzymes and cytokines present within solid tumors. A protein central to measles virus fusion, the F-protein, was engineered to become activated by the increased levels of matrix metalloproteinases found within tumors. By utilizing the preserved tumor microenvironment of tissue slices, the group demonstrated tumor-selective virus infection in samples of primary and secondary liver cancer. 72
It is becoming increasingly popular to “arm” oncolytic viruses, encoding genes for additional antitumor activity such as GM-CSF or TNF-related apoptosis-inducing ligand (TRAIL) 73 for immunomodulation. Again, the intact stromal cell component within the tumor microenvironment of the tissue slice can facilitate preclinical studies on the efficacy of such armed oncolytic viruses. A recent study by Liu et al. assessed the ability of an adenovirus expressing the TRAIL to induce apoptosis in a range of previously apoptosis-resistant glioma cell lines, and then strengthened their findings using an ex vivo slice culture of freshly resected glioma. 64
Conclusions
The use of tumor biopsies and resected samples has now extended to more than just basic diagnosis. Where microscopy using paraffin-embedded samples was once the only form of laboratory support, advances in high-throughput screening and microarray technologies (to name but a few) have expanded the potential of biopsies far beyond histopathology. Now, tumor samples resemble tools that further our understanding of basic tumor biology, demystify resistance to conventional cancer therapeutics, and aid progression toward personalized therapeutics.
The tissue slice methodology has several attractive features: most importantly, it maintains the complex microenvironmental architecture of the tumor. This allows direct study of therapeutic agents within clinically relevant tumor structures, including potential for short-term study of stromal cells, including resident immune cells. All models that aim to recapitulate the human immune system have their limitations and ex vivo slices are no exception (Fig. 3). Their main advantage, however, is that these are human tissues, preserving intact stromal cells with authentic extracellular matrix. While a lack of vascular and lymphatic flow will prevent infiltration of new immune cells and might prove deleterious for the culture of many short-lived cells, this technique should prove invaluable for the study of more tissue-resident immune cells.
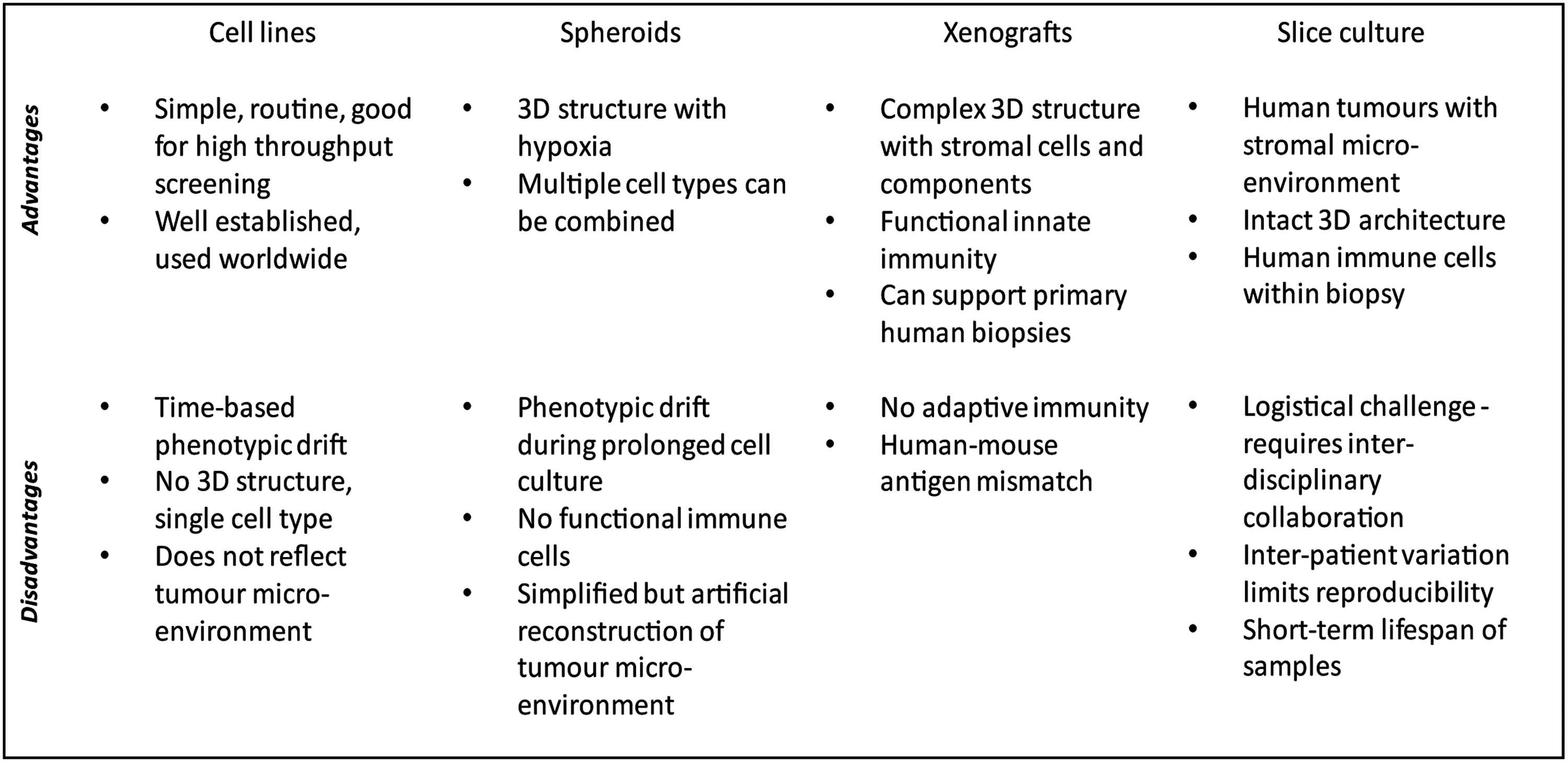
Strengths and weaknesses of some of the main preclinical model systems for the study of human cancer.
Primary tumor samples vary, their availability can be sporadic, and their usage requires significant assay optimization. In contrast, the convenience and reproducibility of using cancer cell lines makes them attractive to work with. In particular, they provide superb insights into the functioning of the cancer cell phenotype. However, by omitting the complex multicellular effects that influence all types of treatment, simple cell lines often provide poor predictors of clinical activity. This is particularly true for biological agents, currently undergoing a resurgence with demonstrable clinical progress of several gene- and immunotherapy-based approaches. We believe that the optimal approach to preclinical development of new agents requires a systematic combination of reductionist cell-based approaches and clinically relevant biopsy-based approaches. Increased opportunities for immunological and personalized interventions will surely make the use of human samples an imperative for the successful future of cancer research.
Footnotes
Author Disclosure Statement
No competing financial interests exist.