
Abstract
Radiation-induced lung injury (RILI) is a major clinical complication for radiotherapy in thoracic tumors. An immediate effect of lung irradiation is the generation of reactive oxygen that can produce oxidative damage to DNA, lipids, and proteins resulting in lung cell injury or death. Currently, the medical management of RILI remains supportive. Therefore, there is an urgent need for the development of countermeasures. The present study aimed to evaluate the protective effect of manganese superoxide dismutase (MnSOD) gene–modified mesenchymal stem cells (MSCs) to facilitate the improved recovery of RILI. Here, nonobese diabetic/severe combined immunodeficiency mice received a 13 Gy dose of whole-thorax irradiation, and were then transfused intravenously with MnSOD-MSCs and monitored for 30 days. Lung histopathologic analysis, plasma levels of inflammatory cytokines (interleukin [IL]-1, IL-6, IL-10, and tumor necrosis factor-α), profibrotic factor transforming growth factor-β1, and the oxidative stress factor (hydroxyproline) were evaluated after MnSOD-MSC transplant. Apoptotic rates were evaluated by terminal deoxynucleotidyl transferase-mediated nick-end labeling immunohistochemical method. Colonization and differentiation of MnSOD-MSCs in the irradiated lung were analyzed by immunofluorescence staining. Consequently, systemic administration of MnSOD-MSCs significantly attenuated lung inflammation, ameliorated lung damage, and protected the lung cells from apoptosis. MnSOD-MSCs could differentiate into epithelial-like cells in vivo. MnSOD-MSCs were effective in modulating RILI in mice and had great potential for accelerating from bench to bedside.
Introduction
R
To this end, stem cell–based therapies have raised the possibility of improving lung repair. Mesenchymal stem cells (MSCs) derived from bone marrow have been attractive cell therapy vehicles for the delivery of agents due to their convenient isolation and expansion, regenerative and multiple differentiation abilities, low immunogenicity, and potent immunosuppressive effects. 8 –13 Several studies have demonstrated that the MSCs have beneficial effects in reducing lung injury in experimental models, indicating the potential for repair of injured lung. 14 –16 Moreover, MSC antifibrotic functions have been described in various organs. 17–18 Accordingly, stem cell therapy using genetically modified MSCs would be an attractive candidate for RILI.
Manganese superoxide dismutase (MnSOD) is the major antioxidant enzyme localized in the mitochondria catalyzing the dismutation of O2 into oxygen and hydrogen peroxide and protecting mitochondria against ROS. 19–20 Recently, we have reported that overexpression of MnSOD in MSCs appears protect against tert-butyl hydroperoxide induced apoptosis in vitro 21 and ameliorate radiation-induced intestinal syndrome in vivo. 22 In the present study, we sought to determine whether administration of MnSOD-MSCs could attenuate RILI.
Materials and Methods
Establishment and characterization of transgenic human MSCs that overexpress MnSOD
Human bone marrow–derived MSCs that stably express MnSOD were established as previously described. 22 Briefly, MnSOD cDNA was cloned from human fetal liver tissue using RT-PCR. Then the amplified human MnSOD fragments were ligated into a Pgc-lV lentiviral vector plasmid containing enhanced green fluorescent protein (eGFP). 21 The lentiviruses were assembled in 293-FT cells lines (Invitrogen). Human MSCs were seeded at 2.0 × 104 cells/cm2 one day before transduction. The medium was replaced with virus-containing supernatant supplemented with 4 mg/mL polybrene (Sigma-Aldrich), and incubated for 48 h. After 48 h of transfection, the eGFP-positive MSCs that constitutively expressed MnSOD were sorted by fluorescence-activated cell sorting.
Experimental animals
Six-week-old male nonobese diabetic/severe combined immunodeficiency mice were purchased from Beijing Vital-River Lab Animal Technology Co. Ltd (SCXK JING 2012-0001). All mice were bred and maintained under specific pathogen-free conditions in the experimental animal unit with a 12 h light–dark cycle. All animal handling and experimental procedures were performed in accordance with the guidelines of the Institutional Animal Care and Use Committee of the General Hospital of the Chinese People's Liberation Army (Beijing, China).
Local radiation and cell administration
Radiation was performed on anesthetized mice (intraperitoneal pentobarbital sodium 50 mg/kg). Mice were placed in specifically designed, well-ventilated plastic box and given 13-Gy gamma radiation from a cobalt-60 source to the whole thorax at a dose rate of 1 Gy/min. Then each recipient mouse was given a tail vein injection of 200 μ
Lung wet/dry weight ratio
The left lung was removed immediately after euthanasia, weighed to obtain the wet weight, and then placed in an oven at 60°C for 72 h for measurement of the dry weight. The ratio of wet weight to dry weight was calculated to assess the tissue edema.
Lipid peroxidation assay
Malondialdehyde (MDA) content in lung homogenate was measured using commercialized chemical assay kits according to the manufacturer's protocol (Nanjing Jiancheng Bioenginneering Institute, Nanjing, China). Thiobarbituric acid reacts with MDA in the acidic medium at 95°C for 30 min to form phenobarbitone acid–reactive product, and the absorbance of the resultant pink product were measured at 534 nm.
Broncho alveolar lavage fluid analysis
For broncho alveolar lavage fluid (BALF) analysis, the mice were sacrificed, an open tracheotomy was performed, and a small plastic tube was inserted into the trachea. The BALF was extracted three times with 2 mL physiological saline and centrifuged (400 g, 15 min) in mL modified Hank's balanced salt solution. Total nucleated cell and neutrophils counts were performed on cellular monolayers prepared by cytocentrifugation at 800 rpm for 10 min, followed by Giemsa-Wright's staining.
Lung histopathology analysis
For histological examination, the lung tissue samples in each group at each time were fixed in 4% paraformaldehyde for 24 h, dehydrated in a graded ethanol series, embedded in paraffin, and sectioned at an average thickness of 5 μm. The tissue sections were stained with hematoxylin-eosin. The severity of lung pathology was evaluated blindly by light microscopy depending on the following criteria: alveolar congestion, hemorrhage, interstitial edema, inflammatory cell infiltration, alveolar wall thickening, and small airway epithelial injury. 23 Collagen deposition was detected by Masson staining.
Enzyme-linked immunosorbent assay
Plasma from the peripheral blood was harvested by centrifugation. Interleukin (IL)-1β, IL-6, tumor necrosis factor (TNF)-α, IL-10, and transforming growth factor (TGF)-β1 levels were measured by enzyme-linked immunosorbent assay kits (all kits from R&D Systems Inc., Minneapolis) according to the manufactures' instructions. For hydroxyproline analysis, the lung tissues were homogenized and assayed by use of hydroxyproline enzyme-linked immunosorbent assay kits (Nanjing Jiancheng Bioengineering Institute, Nanjing, China) according to the manufacturer's protocol.
Apoptosis assay
Identification of apoptosis was confirmed using terminal deoxynucleotidyl transferase-mediated nick-end labeling immunohistochemical staining (ApopTag Peroxidase In Situ Apoptosis Detection Kit). Identification of apoptosis was confirmed according to the manufacturer's instructions. Terminal deoxynucleotidyl transferase-mediated nick-end labeling–positive cells were quantified by morphological criteria in five random images per group.
Immunofluorescence staining
Lung tissues were removed, frozen in optimum cutting temperature medium, and sectioned at 7 μm. The sections were fixed in ice cold acetone, permeabilized with 1% Triton X-100 in PBS for 15 min, and incubated in blocking buffer containing 10% goat serum for 30 min. For double-immunofluorescence staining, the sections were incubated with mouse antibodies against vimentin (Santa Cruz, 1:200) or E-cadherin (Santa Cruz, 1:100) and rabbit antibody against GFP (Proteintech Group, 1:500) overnight at 4°C, followed by incubation with secondary antibodies for 1 h at room temperature. Nuclei were visualized by 4′,6-diamino-2-phenylindole (Sigma). Fluorescence images were analyzed by inverted light microscopy (IX70, Olympus Optical Co.). Confocal images were collected on a LSM 510 META confocal system (Zeiss, Carl Zeiss Micro Imaging).
Statistical methods
All data were expressed as means ± of standard deviation and analyzed using SPSS 16.0 software (SPSS, Chicago, IL). For comparisons between multiple groups, repeated measures analysis of variance tests were applied. Kaplan-Meier survival curve was used for survival analysis. A probability value of less than 0.05 or 0.01 was considered statistically significant.
Results
MnSOD-MSCs improved survival and lung histopathology injury
Of the mice receiving radiation, 48.6% survived to 30 days (the period of observation). The survival rates at 30 days after radiation in mice receiving GFP-MSCs and MnSOD-MSCs were 63.5% and 81.8% respectively. As shown, the MnSOD-MSCs group appeared to be superior to the GFP-MSCs group (Fig. 1B).
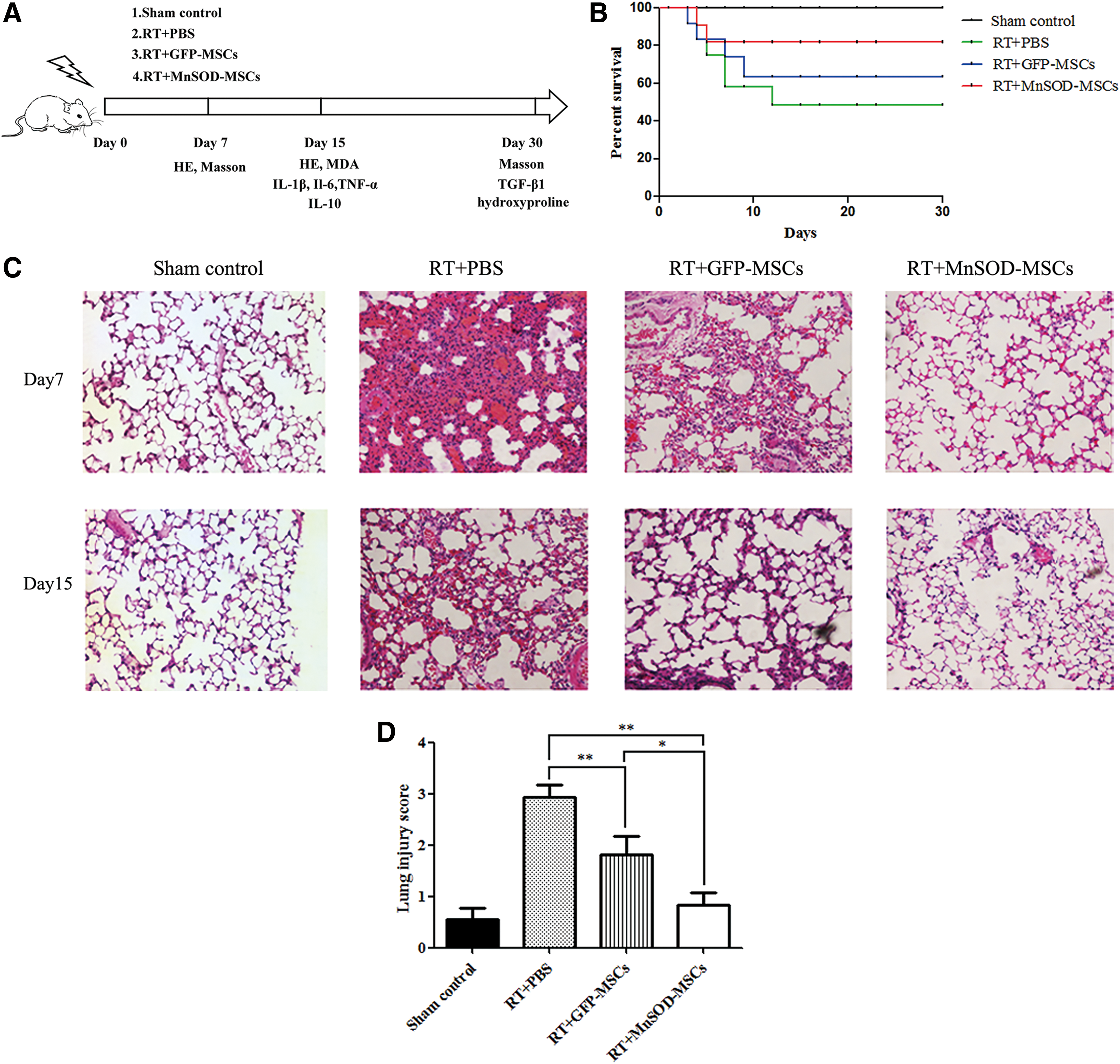
Protective effects of MnSOD-MSCs on histological changes after radiation.
Representative lung histological sections from each group are presented in Fig. 1. Lung tissue from animals without radiation showed lung architecture, respiratory bronchiole, alveolar duct, alveolar sac, and alveoli appearing histologically normal. In contrast, radiation significantly damaged lung architecture, with the remarkable hemorrhage, alveoli collapse, and inflammatory cell infiltrates. GFP-MSCs group showed relatively normal alveolar spaces in some areas. MnSOD-MSCs treatment attenuated alveolar wall thickening and minimal interstitial edema. And there seemed no significant difference compared with the sham control group. The evaluation of the lung histopathology injury was approved by lung score on day 15 after radiation. The lung score was highest in the PBS group. In contrast, the histological changes and the lung injury score were alleviated in GFP-MSCs group. The results suggested that MnSOD-MSCs alleviated the injuries and regenerated the lung structure and integrity.
MnSOD-MSCs treatment alleviated inflammation after RILI
Radiation exhibited a progressive increase in wet/dry ratio. GFP-MSCs administration showed significantly less increase in wet/dry ratio. Treatment with MnSOD-MSCs reduced the wet/dry ratio, which is an index of pulmonary edema, compared with the PBS group and GFP-MSCs group (Fig. 2A). In addition, the numbers of total cells and neutrophils in BALF was measured. The total cell counts and neutrophils counts of the BALF were increased significantly in RT group. In the GFP-MSCs group and MnSOD-MSCs group, the numbers of total cells and neutrophils in the BALF were significantly reduced, and MnSOD-MSCs group appeared to be superior to GFP-MSCs (Supplementary Fig. S1; Supplementary Data are available online at
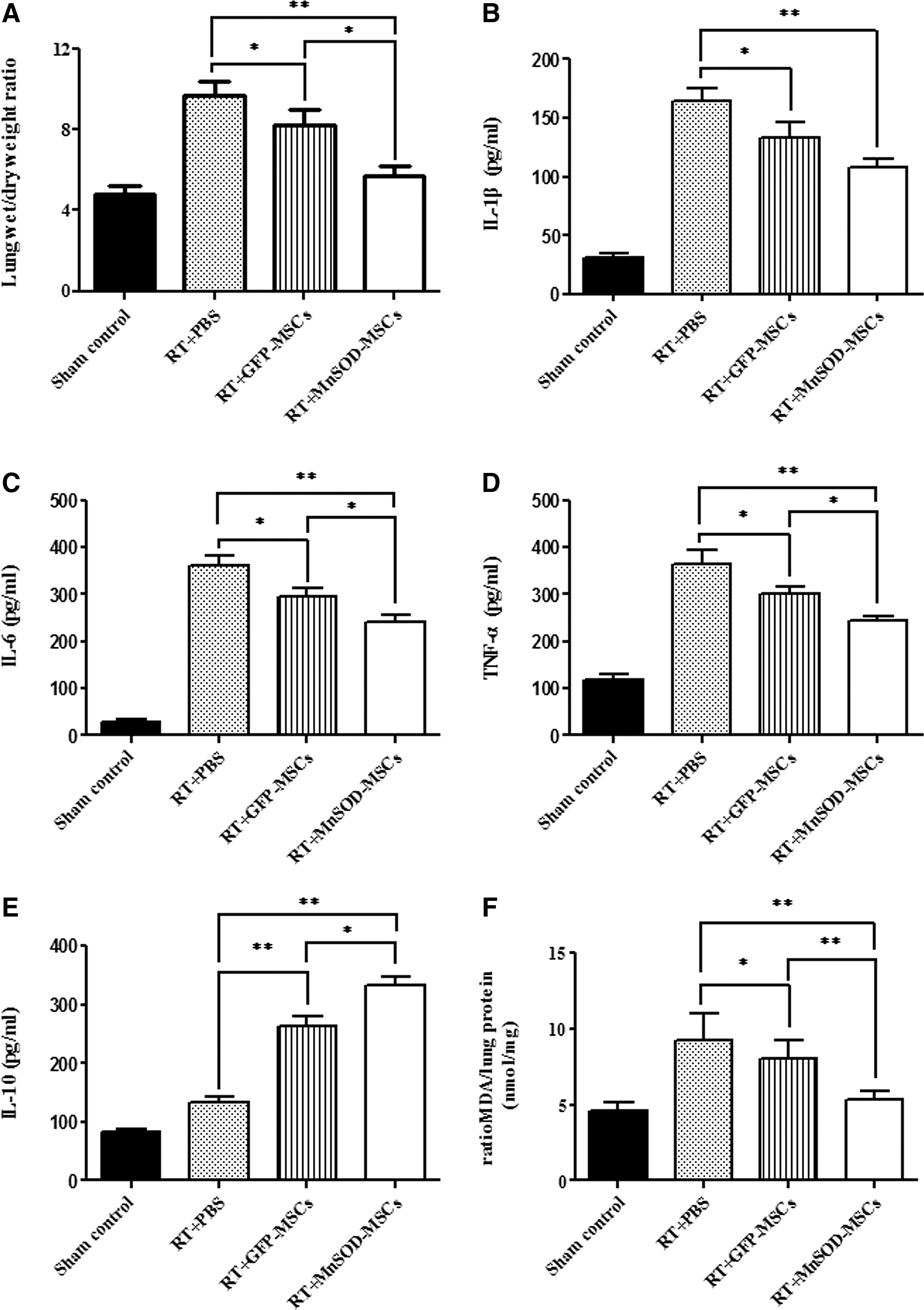
Anti-inflammatory effects of MnSOD-MSCs on RILI.
A number of cytokines and chemokines have been involved in radiation-induced lung pathology. 24 Radiation induced obvious increases in pro-inflammatory cytokines in plasma levels, including interleukin-1β (IL-1β), IL-6, and TNF-α. Treatment with either GFP-MSCs or MnSOD-MSCs decreased plasma concentrations of these cytokines (Fig. 2B–D), indicating that the treatments attenuate the radiation-induced acute inflammatory response. Meanwhile, IL-10 is a highly anti-inflammatory cytokine that inhibits macrophage production. 21 The level of the anti-inflammatory cytokine IL-10 in MnSOD-MSCs group was higher than the RT and GFP-MSCs group (Fig. 2E).
MDA is a marker of lipid peroxidation. 25 Compared with the PBS group, GFP-MSC and MnSOD-MSC administration decreased MDA concentrations in the lung tissues (Fig. 2F). Our data indicated that MnSOD-MSCs treatment might promote the recovery of the balance between pro-inflammatory and anti-inflammatory cytokines, which suggesting that MnSOD-MSCs have an anti-inflammation effect in RILI.
MnSOD-MSCs exert an antifibrotic effect on RILI
Fibrosis in lung tissues was assessed by Masson staining and hydroxyproline detection. Radiation caused marked collagen deposition in the lung interstitium as well as around blood vessels and bronchi. Such changes were attenuated by GFP-MSCs treatment and significantly alleviated by MnSOD-MSCs treatment (Fig. 3A).
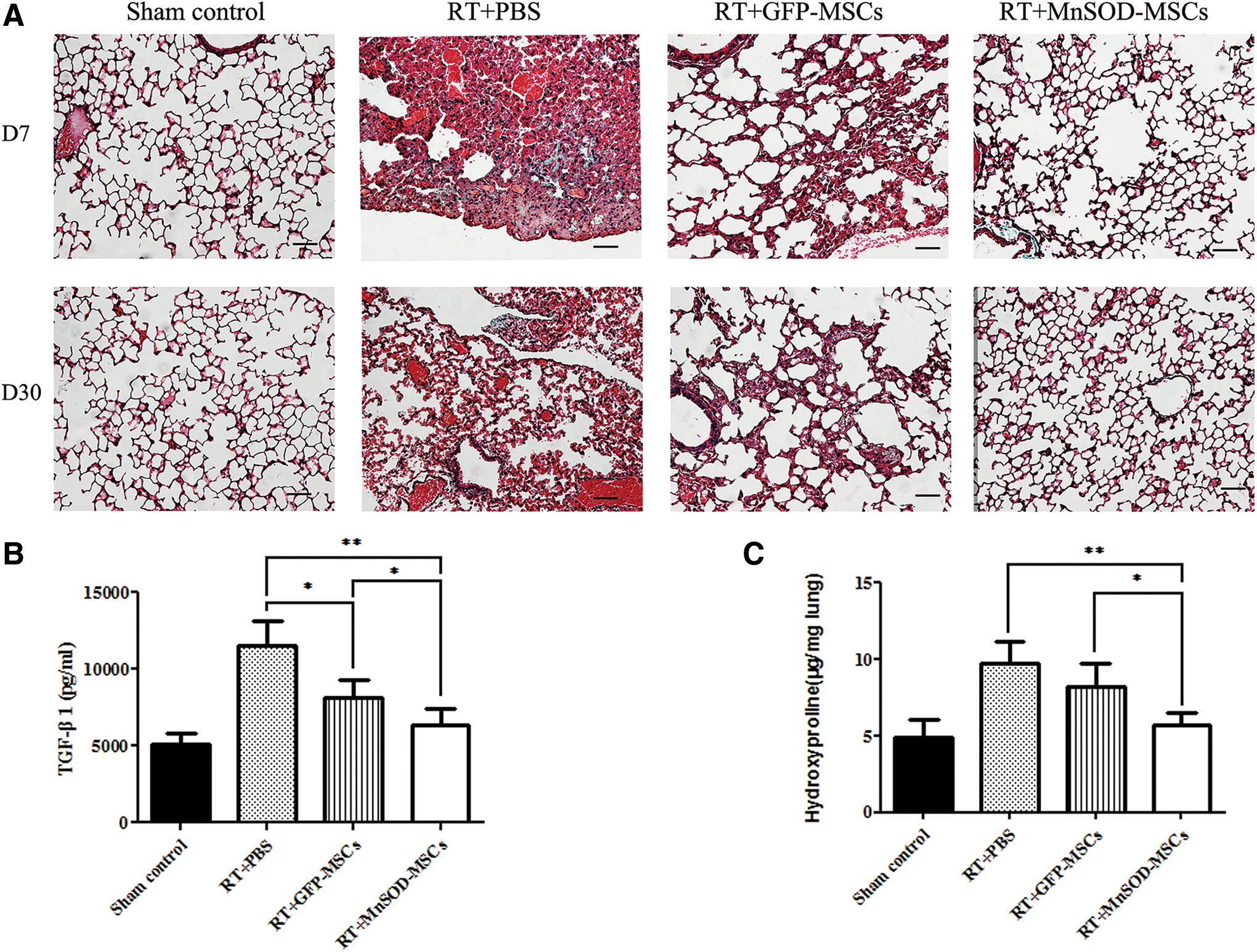
Improvements of lung fibrosis by MnSOD-MSCs administration.
TGF-β1 contributes to the maintenances of tissue architecture by influencing the production of extracellular matrix components. TGF-β1 is proposed to be a potent inducer in the lung tissues fibrosis. The level of TGF-β1 in plasma was compared with that of normal mice, with 5 mice at day 30 after radiation. As shown in Fig. 3B, the expression of TGF-β1 in the plasma of the PBS group and GFP-MSCs group significantly increased compared with sham-exposed mice. MnSOD-MSC treatment significantly reduced TGF-β1 level compared with the PBS group and GFP-MSCs group, although they were still higher than those in the sham control group. Apoptotic cells were studied on histological slides of lung tissue by TUNEL assay (Fig. 4A). We also analyzed the percentage of TUNEL-positive cells (Fig. 4B). At day 7 and day 15, a large number of apoptotic cells were observed in the lung tissue of irradiated mice and GFP-MSCs transplanted mice. In contrast, only a small number of apoptotic cells were observed in the lung tissue of MnSOD-MSCs transplanted mice.
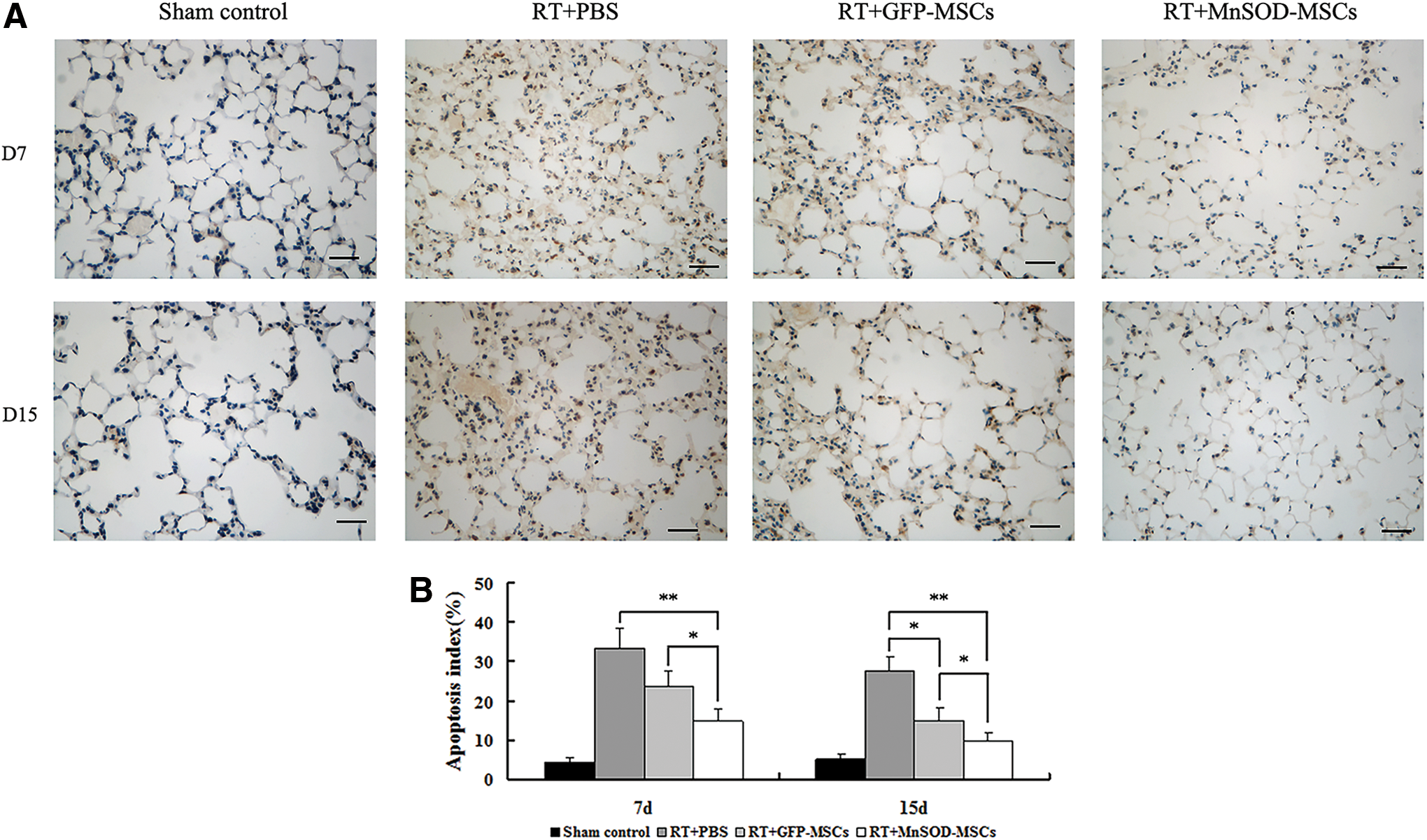
MnSOD-MSCs protected lung tissue cells from apoptosis after radiation.
Location and differentiation of MnSOD-MSCs in vivo
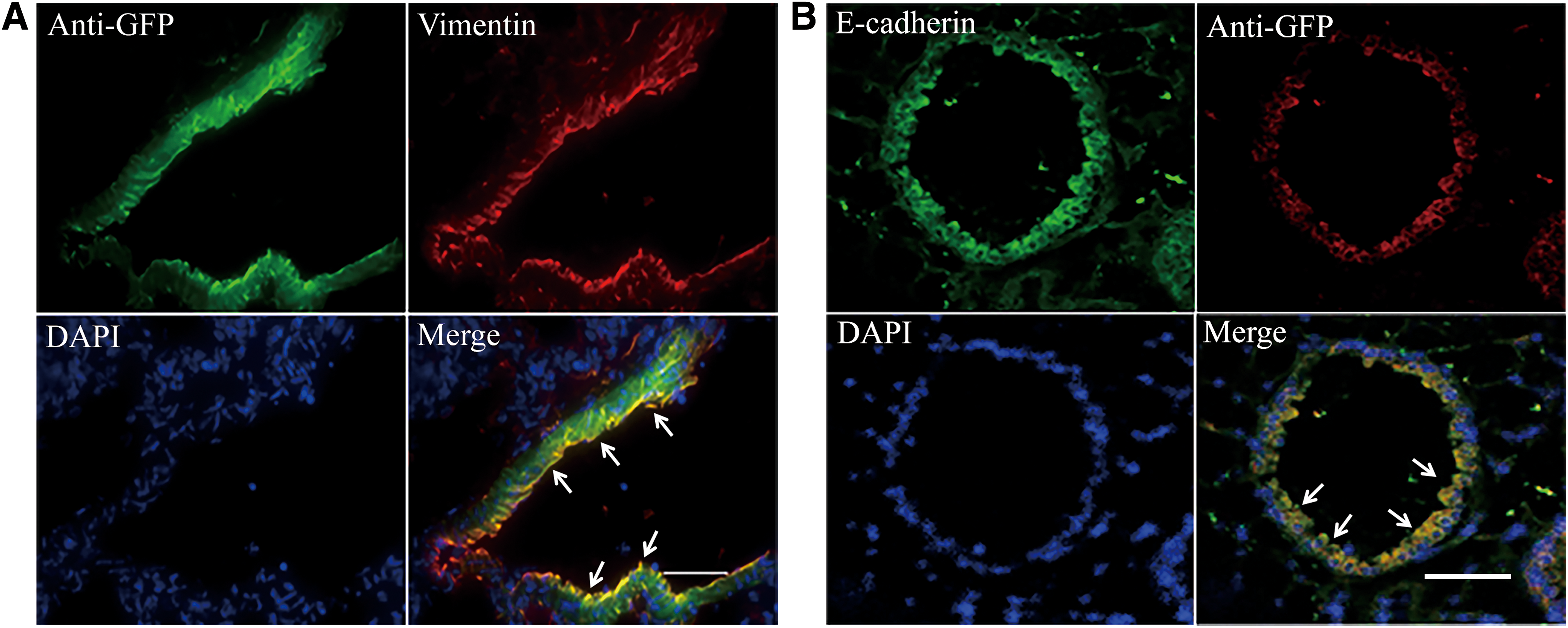
We first evaluated the engraftment of MnSOD-MSCs in the lungs. Immunofluorescence assay revealed that the GFP positive cells were mostly located around the epithelia of bronchiole/small airway (Fig. 5). And only few MnSOD-MSCs were detected in the lung tissues (data not shown). We observed the mesenchymal cell marker and epithelial marker, including vimentin and E-cadherin expression. The results showed that most of the engrafted MnSOD-MSCs and their offspring were positive for vimentin (Fig. 6A), and a small proportion of infused MnSOD-MSCs showed E-cadherin expression (Fig. 6B). These data suggested that the infused MnSOD-MSCs could differentiate into epithelial-like cells in vivo.
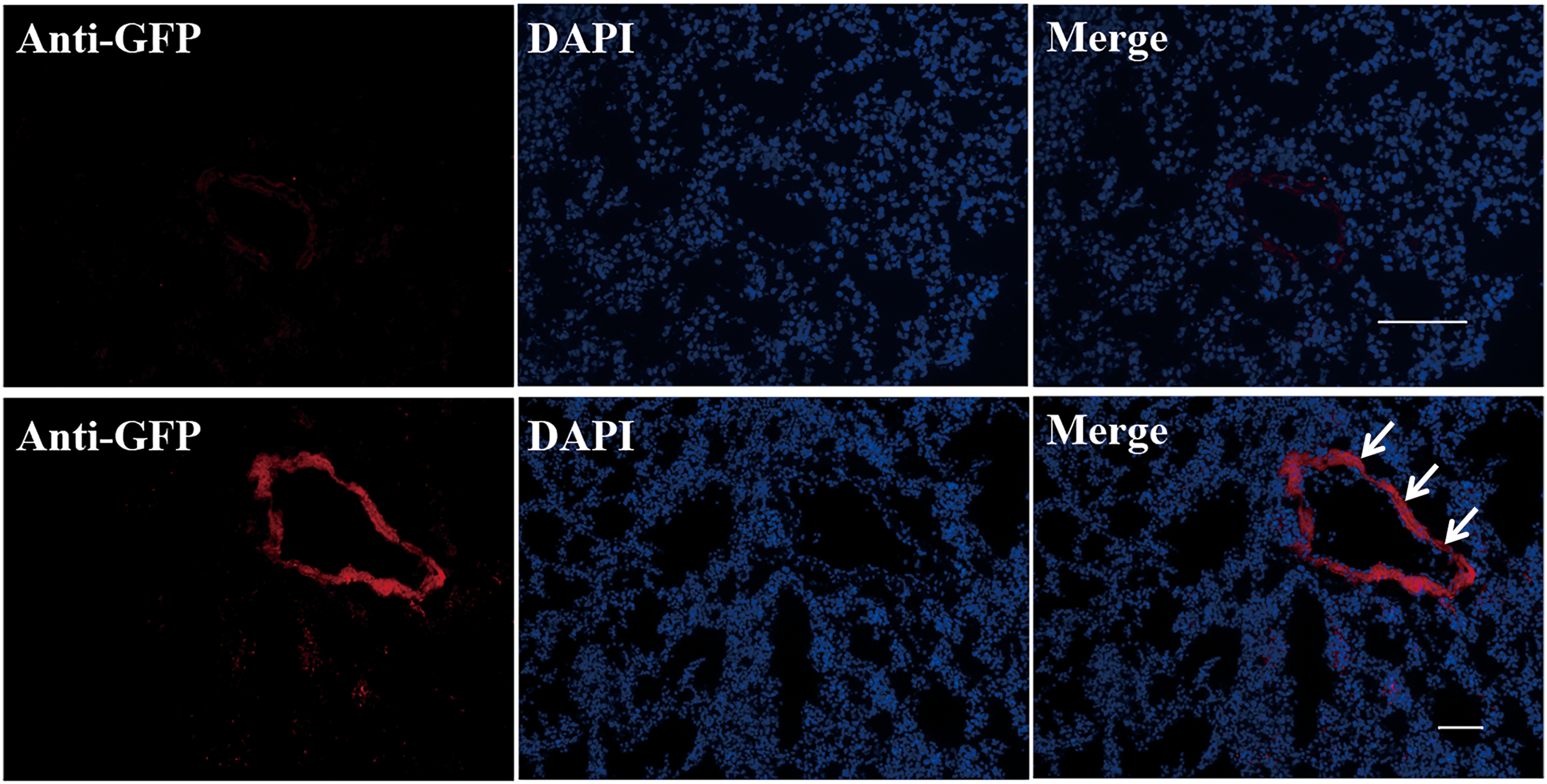
Chemotactic homing of MnSOD-MSCs. MnSOD-MSCs were located in the areas of alveolar duct and alveoli septa, and only a few MnSOD-MSCs were detected. Nuclei were stained with DAPI. Scale bar represents 100 μm. DAPI, 4′,6-diamino-2-phenylindole. Color images available online at
MnSOD-MSCs enhance repair of RILI.
Discussion
Radiation-induced pulmonary injury is part of the major dose-limiting factors of radiotherapy for thoracic malignancies such as lung and breast cancers. 26–27 Ionizing radiation–induced cellular and tissue damage includes mediated radiochemical reactions and oxidative stress. RILI develop through a complex pathological process involving an acute inflammation, increased collagen production, and ultimately pathological fibrosis. 28–29
MnSOD, one of the subtypes of natural superoxide dismutases, acts by catalyzing the dismutation of superoxide radicals into oxygen and hydrogen peroxide to protect cells against ROS. 30 Use of human MnSOD plasmid liposomes has provided significant protection against RILI in mice. 31
Furthermore, stem cell–based gene delivery using MSCs are promising for the development of future therapy. MSCs possess potent lineages differentiation capacity, and anti oxidative stress properties. 32 –35 Available data also suggested that MSCs suppressed the excessive immune responses from T cells, B cells, dendritic cells, macrophages, and natural killer cells. 36 Various investigations have evaluated the therapeutic effect of MSCs in preclinical animal models. 37 –40 Our group has previously demonstrated that overexpression of MnSOD gene in MSCs appears to protect against ionizing radiation–induced apoptosis in vitro. In addition, intravenous MnSOD-MSC therapy enhances the recovery of radiation-induced intestinal injury. 22 We wish to determine the therapeutic efficacy of MnSOD-MSCs on RILI. Inflammatory cytokines play a critical role in mediating, amplifying, and maintaining the RILI process. The radiation induced obvious increases in representative proinflammatory and profibrotic cytokines in plasma, including IL-1β, TNF-α, and IL-6. Our results demonstrate that MnSOD-MSCs markedly decreased plasma concentrations of these cytokines. Moreover, it inhibited the secretion of pro-inflammatory cytokines, such as IL-1β, IL-6, and TNF-α, and strengthened the production of anti-inflammatory cytokine, IL-10. Therefore, MnSOD-MSCs play a major role in the regulation of excessive inflammatory responses in RILI.
Lung irradiation–induced fibrosis is a complex process involving an activation of numerous profibrotic cytokines, which are produced by damaged alveolar epithelial cells, endothelial cells and activated interstitial cells. MSCs have been shown to alleviate fibrosis in various experimental models. Increased TGF-β1 expression leads to recruitment of macrophages and monocytes to the inflammatory site, which could enhance the maturation and activation of fibroblasts. 41 TGF-β1 has been recognized as the key cytokine in the development of lung fibrosis. 42–43 We investigated TGF-β1 level at day 30 after radiation. MnSOD-MSC treatment significantly reduced TGF-β1 level compared with the PBS and GFP-MSCs groups.
MSCs have a tendency to home to damaged tissue sites. The precise molecular mechanisms by which MSCs are able to migrate and home into sites of injury are not yet fully understood. 44 The chemokine stromal—derived factor 1 chemokine receptor 4 axis is a signaling pathway associated with active stem cell recruitment in MSC homing. 45 Systemically administered MSCs are found to migrate specifically to damaged tissue sites with inflammation. 22,46 In present study, we evaluated the engraftment of MnSOD-MSCs in the lungs. Immunofluorescence assay revealed that the GFP positive cells were mostly located around the epithelia of bronchiole/small airway. However, only a few MnSOD-MSCs were found in the injured lungs. The low rate of MnSOD-MSCs in injured lungs seemed insufficient to explain the therapeutic effects. We speculate that the therapeutic benefit of MSCs may be mediated by a paracrine action including MSC migration to the irradiation exposed sites, MSC production of vital growth factors and antioxidants. 47 In addition, MnSOD-MSCs could differentiate into fibroblasts and some could differentiate into epithelial-like cells in vivo.
In conclusion, this study showed that administration of MnSOD-MSCs and their secreted products strikingly reduced systemic and lung inflammation, ameliorated radiation-induced pulmonary fibrosis, improved the survival of irradiated mice, and protected the lung cells from apoptosis. The mechanism of MnSOD-MSCs repairing RILI is through secreting anti-inflammatory and reparative growth factors and also engraftment and differentiation. We speculate that MSCs overexpressing MnSOD gene represent a promising therapeutic option for RILI in patients who undergo radiotherapy of thoracic tumors.
Footnotes
Acknowledgments
The authors gratefully acknowledge financial support from the Natural Science Foundation of China (Nos. 31440039, 31600681, 81402345, 81673873, 81400274, 31570854, and 81670496), Beijing National Science Foundation of China (No. 5154035), and Beijing Nova Program of Science and Technology (xx2017103).
Author Disclosure
No competing financial interests exist. All authors declare that there are no conflicts of interest with regard to this study or in reporting the findings described in this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.