
Abstract
The present clinical trial assessed the effect of double-dose administration of replication-deficient adenovirus-thymidine kinase and ganciclovir (ADV-TK/GCV) in patients with advanced hepatocellular carcinoma (HCC) who underwent liver transplantation (LT). Eighty-six patients with single tumor diameters >5 cm or multiple tumors with diameters >3 cm each, regardless of vascular invasion, were examined over a follow-up period of 61 months. All patients underwent orthotopic LT; 43 received LT only, and 43 received LT plus double-dose ADV-TK/GCV gene therapy (LT + ADV-TK/GCV). Recurrence-free survival (RFS) and overall survival (OS) rates, as well as therapeutic safety, were assessed. The RFS and OS rates in LT + ADV-TK/GCV patients at 3 years (55.9% and 60.3%, respectively) were significantly higher than those in the LT-only group (13.5% and 19.3%, respectively; p < 0.001). LT + ADV-TK/GCV patients without vascular invasion showed significant improvement in RFS (73.7%) and OS (68.6%). LT + ADV-TK/GCV patients without extrahepatic vascular invasion experienced higher OS versus LT-only patients. Double-dose ADV-TK/GCV gene therapy combined with LT was safe and improved RFS and OS in advanced HCC patients without vascular invasion over the 5-year follow-up period. The potential to select patients with intrahepatic and extrahepatic vascular invasion for LT requires further confirmation.
Introduction
A
Liver transplantation (LT) has been validated as a highly effective HCC treatment, as it removes the tumor, prevents formation of metachronous lesions on underlying cirrhosis, and restores normal liver function. 5 In 1996, Mazzaferro et al. established the Milan criteria for HCC patients who are candidates for LT. 6 Although patients who meet these criteria and undergo LT have been shown to exhibit satisfactory long-term survival, application of these criteria excludes a large proportion of patients from LT, preventing them from the chance of becoming cancer free. 7
Several centers have attempted to expand the Milan criteria. 8 –10 Mazzaferro et al. 11 reported in 2009 that HCC patients meeting a more precise estimation of survival based on individual tumor characteristics and use of up to seven criteria could receive LT. Previously, the authors' group successfully expanded the criteria for LT by using adjuvant gene therapy. The research showed that HCC patients without vascular invasion could undergo LT followed by adjuvant adenovirus (ADV)-thymidine kinase (TK)/ganciclovir (GCV) therapy, regardless of tumor location, size, or diffuseness. 12
ADV-mediated delivery of herpes simplex virus TK into tumor cells is a well-studied approach for facilitating the eradication of tumors. TK converts the prodrug GCV into a toxic, phosphorylated form that gets incorporated into DNA during cell division, terminates DNA replication, and leads to tumor cell death. 13 –15 TK transduction effectively eradicates cancer cells via a bystander effect that acts not only on the targeted lesion but also on distant lesions. 16 The hepatotropic tendency of ADV-TK and possibly the immune evasion of ADV-TK reagents in host patients may improve the efficiency of gene transfer, resulting in stronger transgene expression in the target tissue. 17,18 The advantages of ADV-TK therapy highlight its potential as an adjuvant treatment for HCC patients after LT.
In the current clinical trial, which was motivated by the authors' previous studies, 12,19 ADV-TK/GCV therapy was delivered to patients twice in an attempt to enhance LT efficacy. These patients harbored advanced HCC beyond Milan and the authors' previous criteria, with some patients experiencing intrahepatic or extrahepatic portal branch involvement. The clinical effect of double-dose ADV-TK/GCV adjuvant therapy was assessed over 5 years, and the possibility of expanding HCC transplantation criteria was evaluated.
Materials and Methods
The present study was conducted in accordance with the Declaration of Helsinki. All patients provided written, informed consent. This study was also approved by the local ethics committee and was registered with
Eligibility criteria
Eighty-six patients in YouAn Hospital (Beijing, P.R. China) and Chaoyang Hospital (Beijing, P.R. China) participated between October 2006 and December 2011. All participants with advanced HCC were 18–70 years old and had not received radiotherapy, chemotherapy, targeted therapy, or other biological treatment within 4 weeks before LT. Tumors were evaluated via computed tomography (CT) or magnetic resonance imaging (MRI) and a complete liver function panel. Patients who had unresectable HCC with a single tumor >5 cm in diameter or multiple tumors each >3 cm in diameter and no metastases in the lungs and bones were eligible to participate. Vascular invasion of the intrahepatic or extrahepatic portal branches was not considered to be an exclusion criterion. However, cases that displayed 50% invasion of the main portal vein, as well as cases with lesions beyond the upper half of the main portal vein, were excluded. Vascular invasion was evaluated via ultrasonography prior to LT surgery or via pathology afterwards. Locoregional treatments, such as radiofrequency ablation, transcatheter arterial embolization, and hepatectomy, were used to control HCC progression before LT.
Study design and treatment
The aim of the present study was to evaluate and compare recurrence-free survival (RFS) and overall survival (OS) in each treatment group, as well as the safety of double-dose ADV-TK/GCV adjuvant therapy. Patients were randomly assigned (1:1) to LT-only or LT + ADV-TK/GCV groups via individual randomization numbers sealed within envelopes given to each patient according to the randomization table kept at YouAn Hospital. Participants and study investigators were not blinded to treatment allocation. LT-only patients received orthotopic LT and subsequent immunosuppression therapy. In the LT + ADV-TK/GCV group, ADV-TK/GCV therapy was administered in addition to any treatments received by the LT-only group (Fig. 1).
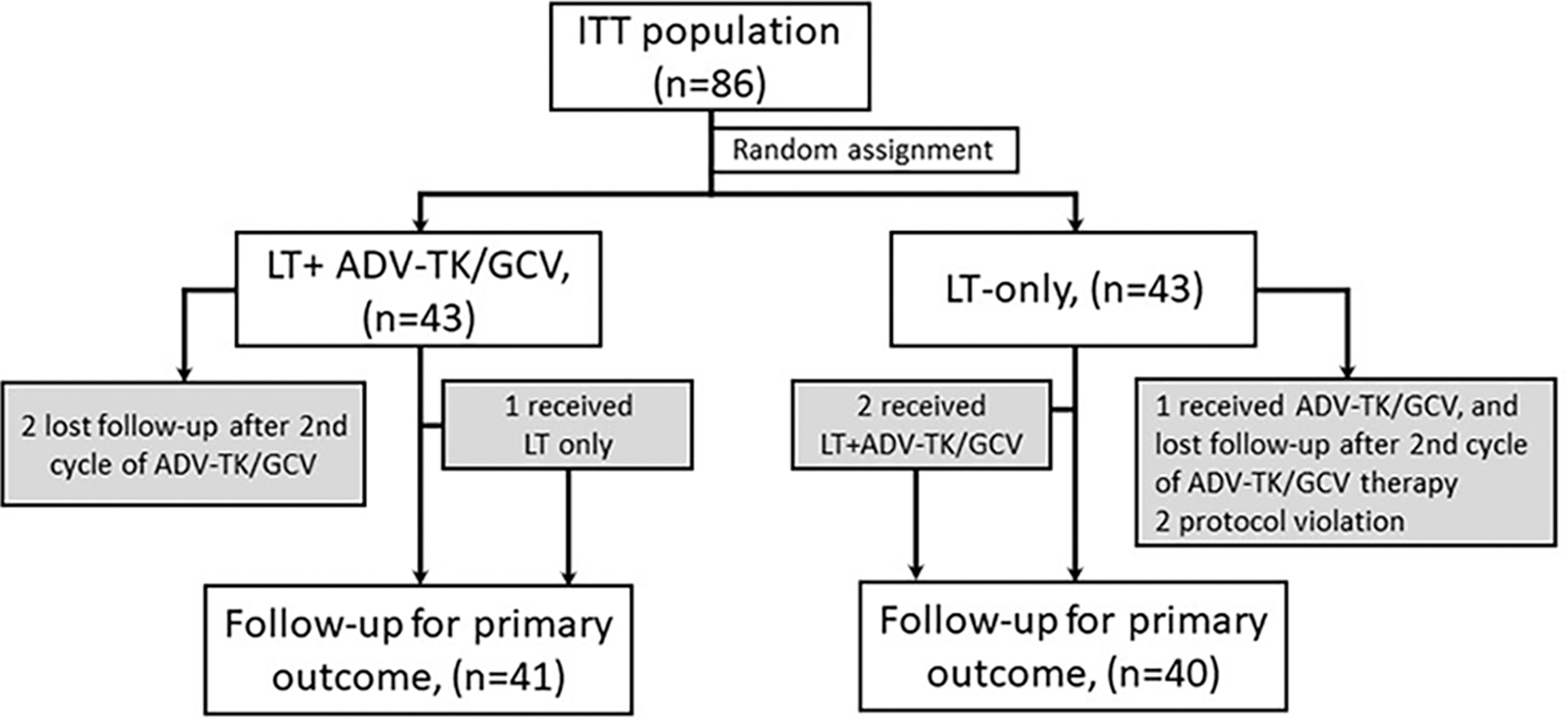
CONSORT diagram. Eighty-six advanced hepatocellular carcinoma patients in YouAn Hospital and Chaoyang Hospital were recruited to an intent-to-treat population. Three patients were lost to follow-up after receiving two cycles of adenovirus-thymidine kinase/ganciclovir (ADV-TK/GCV) therapy: two in the ADV-TK/GCV plus liver transplantation (LT) group, and one in the LT-only group. Two patients in the LT-only group were withdrawn from the study due to protocol violation. The patients in the shaded boxes were included in the final statistical analysis for recurrence-free survival (RFS) and overall survival (OS). The patients in the white boxes were withdrawn from the study.
Orthotopic LT and subsequent immunosuppression therapy were performed as previously described. 12 For patients who received double-dose ADV-TK/GCV (Tian Dakang Co.), the first ADV-TK dose was administered during LT surgery; 1.0 × 1012 viral particles of ADV-TK in 100 mL of 0.9% saline were injected into peritoneum tissues around the liver, including the lesser curvature of the stomach, side of the abdominal aorta, head of the pancreas, surface of the right kidney, area under the right diaphragm (60 mL for all preceding locations), and partial area of the gastroepiploic vein (40 mL). Most of the viral dose was administered into the middle of the peritoneum tissues in contact with the liver. The first intravenous dose of GCV (2.5 mg/kg; Hoffman–La Roche) was slowly administered 36 h after LT and twice daily thereafter for 14 days. The second ADV-TK dose was administered 30 days after LT; 1.0 × 1012 viral particles of ADV-TK in 100 mL of 0.9% saline were injected into the celiac (60 mL) and superior mesenteric (40 mL) arteries via femoral artery puncture. A second, identical GCV administration was also performed.
Patient follow-up always included CT or MRI to detect recurrence. Follow-up was performed monthly up to the third postoperative month, then once every 3 months up to the third postoperative year, and then at least once every 6 months thereafter. When possible, positron emission tomography was carried out to detect micrometastatic foci or early recurrence. Adverse effects were evaluated based on symptoms reported by the patients or observed by clinicians.
The primary endpoints were RFS and OS. RFS was measured from the day of randomization to objective recurrence or HCC-related death, whichever occurred first. OS was measured from the day of randomization to death. For patients remaining alive, survival was recorded at the time of the last follow-up.
Statistical analysis
The plan was to enroll 80 patients (40 patients per treatment group) in accordance with the outcome of a previous trial. 16 This estimate was based on 80% power and two-tailed significance of 5%, with 5% for treatment switch and withdrawal cases, assuming a 35% improvement in 3-year RFS after additional ADV-TK/GCV treatment (50%) versus LT alone (15%). All analyses were performed based on an intent-to-treat population (Fig. 1). Continuous variables were assessed for normality via the Kolmogorov–Smirnov test. Means between two groups were compared using a two-tailed, unpaired Student's t-test or analysis of variance. The Mann–Whitney test was used to test the medians of the treatment groups when continuous variables did not exhibit a normal distribution. Chi square or Fisher's exact tests were used for categorical variables where appropriate. RFS and OS were presented as Kaplan–Meier estimates and compared via log-rank tests. Treatment hazard ratios (HR) with 95% confidence intervals (CI) were calculated using the Cox regression model. For comparisons against the LT-only group, a HR <1 indicates a benefit with ADV-TK/GCV therapy. Hypotheses were tested in a two-sided fashion. p-Values <0.05 were considered to indicate statistical significance. Data were analyzed with IBN SPSS Statistics for Windows v22.0 (IBM Corp.).
Results
Patient characteristics
As of December 31, 2011, 86 advanced HCC patients at YouAn Hospital (Beijing, P.R. China) and Chaoyang Hospital (Beijing, P.R. China) were recruited to an intent-to-treat population. Demographics and baseline characteristics were similar between groups. Before LT, 33 patients received locoregional treatments; 17 achieved stable disease, and disease progression was observed in 16 patients. Although three patients showed progressive disease with new lesions, they still met the eligibility criteria (Table 1). Rejection episodes occurred in eight patients (four in each treatment group). Three patients received glucocorticoid pulse therapy. The immunosuppression regimen was adjusted in five patients in response to details of rejection episodes. Overall, 81 patients completed treatment (Fig. 1); the median follow-up time for these patients was 23 months (range 1–61 months).
Demographics and baseline characteristics of 86 HCC patients
LT-only group: three patients with hepatitis B and C, one patient with primary sclerotic cholangitis, one patient with hepatitis B and alcoholic cirrhosis; LT+ADV-TK/GCV group: two patients with hepatitis B and C, one patient with hepatitis C-associated cirrhosis, three patients with alcoholic cirrhosis.
LT-only group: Two patients received both hepatectomy and TAE; one patient received ligation of right portal vein branch 3 months before LT.
No significance between LT-only group and LT-ADV-TK/GCV group.
Compared with preoperative serum AFP level, p < 0.001.
HCC, hepatocellular carcinoma; LT, liver transplantation; ADV-TK, adenovirus-thymidine kinase; GCV, ganciclovir; HBV, hepatitis B virus; TNM, tumor node metastasis; BCLC, Barcelona clinic liver cancer; TAE, transcatheter arterial embolization; RFA, radiofrequency ablation; SD, stable disease; PD, progressive disease; AFP, alpha-fetoprotein.
Double-dose ADV-TK/GCV therapy improved RFS in HCC patients who underwent LT (LT + ADV-TK/GCV)
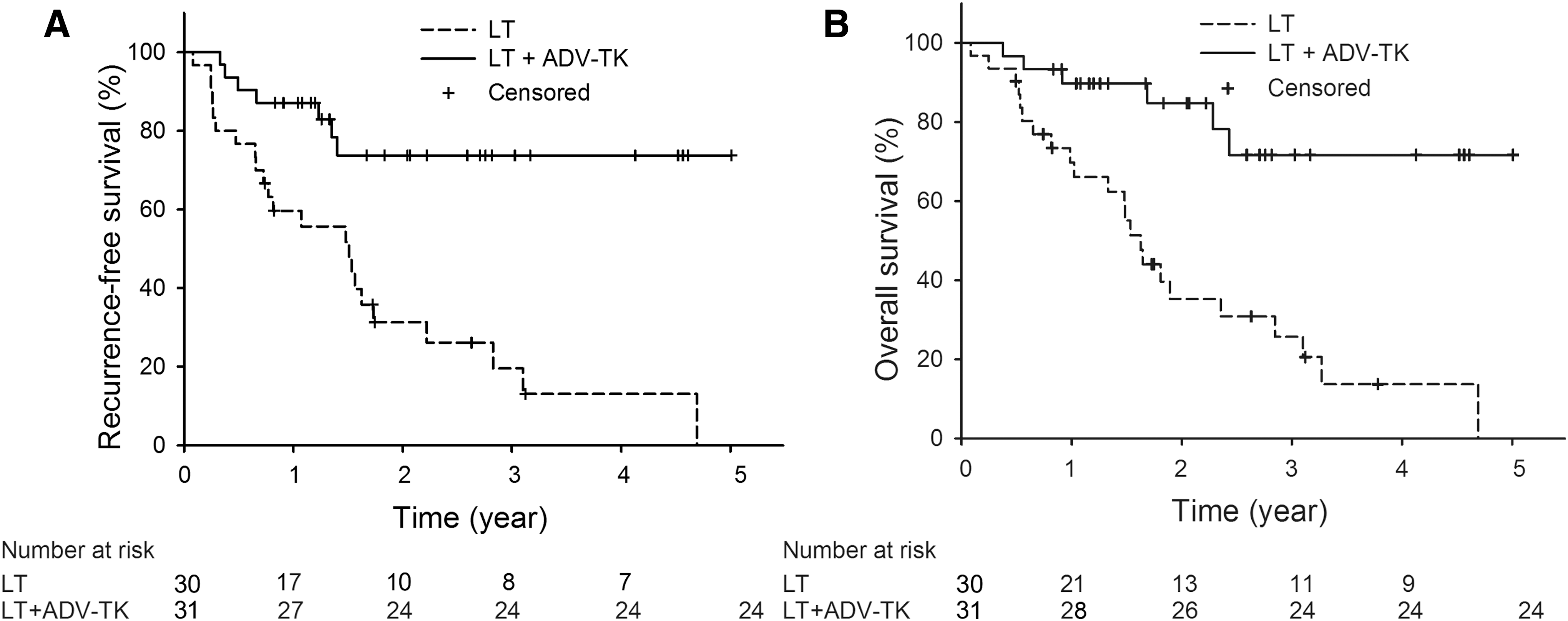
In the LT + ADV-TK/GCV group, eight cases relapsed at 1 year, and six relapsed 2–3 years after LT, making the 1- and 3-year cumulative recurrence rates 19.7% and 38.6%, respectively. In those who underwent LT but did not receive adjuvant gene therapy (LT-only), 12 cases relapsed at 1 year, and nine relapsed 2–3 years after LT, making the 1- and 3-year cumulative recurrence rates 34.1% and 76.5%, respectively (log-rank test, p = 0.03; Breslow test, p = 0.087; HR = 0.481, 95% CI 0.244–0.948, p = 0.034). In LT + ADV-TK/GCV patients, the 1- and 3-year RFS rates were 78.0% and 55.9%, respectively; the 55.9% RFS rate was maintained until the end of study. In LT-only patients, the 1- and 3-year RFS rates were 49.5% and 13.5%, respectively. Actuarial RFS probabilities significantly differed between groups (log-rank test, p < 0.001; Breslow test, p = 0.002; HR = 0.339, 95% CI 0.187–0.616, p < 0.001; Fig. 2A), indicating that double-dose ADV-TK/GCV adjuvant therapy improved RFS in advanced HCC patients who underwent LT.

RFS and OS of 81 patients according to therapy protocol.
Double-dose ADV-TK/GCV therapy improved OS in HCC patients who underwent LT
In the LT + ADV-TK/GCV group, the median follow-up time was 23 months (range 4–61 months). Five patients died at 1 year, and seven died 2–3 years after LT, making the 1- and 3-year OS rates 87.4% and 60.3%, respectively. The latter rate remained constant until the end of the 5-year follow-up period. In the LT-only group, the median follow-up time was 18 months (range 1–57 months). Fourteen patients died at 1 year, and 16 died 2–3 years after LT, making the 1- and 3-year OS rates 61.6% and 19.3%, respectively. The difference in OS rates between the two groups was significant (log-rank test, p < 0.001; HR = 0.273, 95% CI 0.141–0.532, p < 0.001; Fig. 2B), demonstrating that double-dose ADV-TK/GCV adjuvant therapy improved OS in these patients.
The main cause of death in the present study was recurrence of HCC (n = 35/81). In the LT + ADV-TK/GCV group, 10 patients died of relapse. In these patients, recurrence sites were the liver (n = 5), lung (n = 3), and both liver and lung (n = 2). In the LT-only group, 25 patients died of HCC relapse. Recurrences occurred in the liver (n = 11), lung (n = 8), bone (n = 1), and both liver and lung (n = 5). Other causes of death were infection of the biliary tract (n = 3, all LT-only), pulmonary infection (n = 3, one in LT + ADV-TK/GCV and two in LT-only), sepsis (n = 1, in LT + ADV-TK/GCV), upper gastrointestinal hemorrhage (n = 1, in LT-only), and cerebrovascular accident (n = 1, in LT-only).
Outcomes of HCC patients with or without vascular invasion
Of all 81 patients, 61 were confirmed to lack vascular invasion by post-LT pathology. In the LT + ADV-TK/GCV group (n = 31), the RFS and OS were 73.7% (log-rank test, p < 0.001; HR = 0.215, 95% CI 0.093–0.501, p < 0.001) and 68.6% (log-rank test, p < 0.001; HR = 0.241, 95% CI 0.103–0.565, p = 0.001), respectively, 5 years after LT. These differences were significant compared to the LT-only group (n = 30; Fig. 3A and B), suggesting that double-dose ADV-TK/GCV adjuvant therapy was most advantageous for patients without vascular invasion. Of the 81 patients, 20 were confirmed to harbor vascular invasion. Patient outcome varied, depending on the location of the vascular invasion. Of nine patients with intrahepatic vascular invasion, four received double-dose ADV-TK/GCV treatment; one of these patients died 22 months after LT, while the other three remained alive at the time of analysis. The other five patients did not receive ADV-TK/GCV treatment, and all died within 26 months of LT. Thus, double-dose ADV-TK/GCV adjuvant therapy potentially improved the outcomes of patients with intrahepatic invasion (Table 2). Of 11 patients with extrahepatic vascular invasion, one relapsed rapidly 8 days after LT, and 9/11 patients died 5.1–20 months after LT. There was no significant difference in outcome between groups (Table 2).
RFS and OS of 61 patients without vascular invasion.
Characteristics of 20 patients with vascular invasion
No recurrence was found at the end of follow-up.
The patient was alive at the end of follow-up.
Safety
In the LT + ADV-TK/GCV group, only 17 patients suffered mild catarrhal symptoms and light headache; 15 reported a slight fever (<38.3°C) but no chills during the first 3 days after receiving their first ADV-TK/GCV treatment. No treatment-related grade 3 or 4 liver or renal dysfunction occurred in patients who received ADV-TK/GCV injections other than abnormalities in liver and renal function caused by LT in the first 14 days after surgery. Detailed tests results are shown in Supplementary Table S1 (Supplementary Data are available online at
Discussion
The present randomized clinical trial demonstrated the RFS and OS benefits of double-dose ADV-TK/GCV gene therapy as an adjuvant to LT. Even though the present trial included a sample size of 81 patients, to the authors' knowledge, this investigation is the largest clinical trial investigating double-dose ADV-TK/GCV therapy combined with LT for HCC patients. The purpose of the current study was to improve patient outcomes further by removing the tumor burden on the liver through LT and maximally eliminating small tumor foci and micrometastases via injection of a double dose of ADV-TK into peritoneum tissues around the liver, hepatic artery system, portal vein system, and lymphatic drainage area.
Liver cancer cells migrate outside or inside the liver via the portal vein, hepatic artery, and hepatic lymph circumfluence area to cause metastases or disease recurrence. ADV-TK injection into the liver lymph circumfluence system in the posterior peritoneum has been shown to destroy most cancer cells easily and directly via the bystander effect. 13,14 Various other injection methods enable ADV-TK to access the hepatic blood circulation to kill cancer cells in the lymphatic system, blood system, and liver tissue. 20,21 Injection into the hepatic lymph circumfluence area can result in the transfection of liver cancer cells in the lymph circumfluence, while intravenous injection into the gastric omentum can return the therapeutic compound to the liver portal system through the venous system. Celiac injection enables the therapeutic compound to access the hepatic artery through the arterial system then return to the hepatic vein system, and injection into the superior mesenteric vein allows the therapeutic compound to access the peritoneal, hepatic vein, and lymphatic systems. In 2001, Reid et al. were the first to conduct a Phase I clinical trial on the intra-arterial administration of a genetically engineered, replication-selective ADV (dl1520, also known as Onyx-015) in patients with colorectal carcinoma metastatic to the liver. 22 In 2002, this team conducted a Phase II clinical trial on administration of an oncolytic replication-selective ADV (dl1520) via the same injection route. 23 The authors' research group has also used intra-arterial administration of ADV-TK in recurrent high-grade glioma, with excellent outcomes. 24
Previous intra-arterial administration of ADV-TK gene therapy was associated with an acceptable toxicity profile. 22,23 Herein, no side effects were detected after injecting ADV-TK into the celiac and superior mesenteric arteries via femoral artery puncture. During the 5-year follow-up period, obvious outcome improvements were achieved related to both RFS and OS. Generally, HCC recurrence and metastasis directly affect patient survival. Previous investigations have attempted to stop recurrence or metastasis with chemoreagents and other adjuvant therapies (e.g., sorafenib and licartin) for patients at high risk, such as those with vascular invasion or T3/T4 tumors, despite the lack of evidence supporting these strategies. In a previous trial, epirubicin was used after LT, but no benefits in HCC patients or outcomes after LT were observed. However, the current study yielded evidence of improved survival in advanced HCC patients with intrahepatic vascular invasion that received double-dose ADV-TK/GCV adjuvant therapy after LT. Although the current investigation represents a step forward from the first study, it is still limited by its small population of HCC patients who underwent LT. Future studies should include a larger patient population and an active control group using present adjuvant treatment.
The advantages of LT for HCC are widely accepted. This technique not only eliminates both cancer cells and cirrhosis, but also restores liver function, especially for HCC that develops from post-hepatitis cirrhosis. In 2016, Zhang et al. reported that 43.1% of patients had a tumor >5 cm in diameter and 22.5% had a tumor >10 cm in diameter at their first doctor visit. 25 It is not advisable to expand the criteria for LT blindly without appropriate adjuvant treatment.
To date, post-LT adjuvant therapies based on conventional chemotherapeutic agents have failed to demonstrate efficacy. Evaluation of newer agents, such as the multikinase inhibitor sorafenib, for the treatment of patients with advanced renal cancer and unresectable HCC 26 are still in early phases. 27 –29 Accordingly, more effective post-LT adjuvant therapies need to be rigorously explored. The previous 3-year follow-up investigation evaluated the efficacy and safety of ADV-TK/GCV treatment for advanced HCC patients that underwent LT. 12 In the current study, the survival follow-up time was prolonged to 5 years, and the method of administration and dosage of ADV-TK/GCV were modified. Based on the results of the original study, 19 the ADV-TK dose was increased from 5.0 × 1011 to 1.0 × 1012 viral particles. In addition to the injection areas used during surgery (e.g., the lesser curvature of the stomach, side of the abdominal aorta, head of the pancreas, surface of the right kidney, and area under the right diaphragm), the current study also injected into the celiac and superior mesenteric arteries via femoral artery puncture after LT. This strategy was implemented in an attempt to extend the ADV-TK regimen to the liver lymphatic drainage area, as well as blood carried by liver arteries and veins. Furthermore, because non-replicating ADV therapy is often limited by the low transduction efficiency of the vector, modified conditionally replicating viral vectors were further investigated to facilitate therapeutic gene expression efficiency in targeted tumor cells. 30 –32
In summary, the results of the current 5-year follow-up study confirm that patients with advanced HCC beyond the Milan criteria who lack vascular invasion can be selected as candidates for double-dose ADV-TK/GCV adjuvant therapy after LT. The size and number of tumors in the liver should not affect the prognosis if patients receive LT and an effective ADV-TK adjuvant therapy, such as the one used herein. The potential to select patients without extrahepatic vascular invasion for LT remains to be confirmed.
Footnotes
Acknowledgments
The authors would like to thank the Foundation for the Excellent Medical Staff of Beijing (2011-3-034), National Major Scientific and Technological Special Project for “Significant New Drugs Development” during the Twelfth Five-year Plan Period (2011ZX09101-001-10 and 2012ZX100002017-009), Beijing Municipal Administration of Hospitals Clinical Medicine Development of Special Funding Support (ZY201311), National Natural Science Fund of China (81090414, 81230038, 81472783, and 81025011), National Basic Research Program of China (973 Program; 2015CB553903); Chinese National Key Plan of Precision Medicine Research (2016YFC0902901), and National Science-Technology Supporting Plan Projects (2015BAI13B05).
Author Disclosure
The authors declare no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.