
Abstract
This study evaluated the efficacy of rAd-p53 (Gendicine®) followed by chemotherapy for the treatment of uterine sarcoma. Twelve cases of uterine sarcoma treated at Shengjing Hospital were retrospectively analyzed. Among the 12 patients, one had primary cancer, and 11 had recurrent cancer. For the recurrent cases, the interval between the first operation and diagnosis of recurrence, or progression-free survival time 1 (PFS1), was 1–18 months (median 3 months). All patients were treated with local application of rAd-p53 followed by chemotherapy (local injection of bleomycin and i.v. infusion of cisplatin, epirubicin, and isocyclophosphamide). Efficacy was evaluated, and the rates of complete remission (CR) and partial remission (PR) were calculated. During follow-up, PFS time 2 (PFS2) after the baseline period and overall survival (OS) time after the baseline period of rAd-p53 treatment data were obtained. The treatment resulted in one CR, seven PR, three with stable disease (SD), and one with progressive disease (PD). The remission rate (CR + PR) was 66.7%, and the responsive (CR + PR + SD) rate was 91.7%. PFS2 ranged from 2 to 62 months, with a median of 13 months, which is 10 months longer than that of PFS1; this difference was statistically significant (p = 0.0038). The OS time ranged from 6 to 62 months, with a median of 24 months. Following the combined treatment, four of the patients underwent a second debulking surgery. Of the two patients with liver metastases, one had CR of liver foci, and one had PR. Up to the follow-up date of the two patients who survived, one was tumor-free for 60 months. The PFS2 for the other patient was 39 months. This patient survived with tumor for 53 months with slow disease progression. The remaining 10 patients died. Local application of rAd-p53 combined with local injection of bleomycin and intravenous infusion of cisplatin, epirubicin and isocyclophosphamide was effective for treatment of uterine sarcoma, especially for patients with liver metastases. For patients with uterine sarcoma who do not have the opportunity for surgery, this regimen can be used as a new adjuvant therapy to obtain a surgical opportunity that allows further debulking of the tumor mass.
Introduction
U
An increasing number of studies show that gene therapies, particularly those involving wild-type human tumor suppressor p53, are a promising antitumor strategy. 6 p53 protein is the most important tumor suppressor in humans. In many cancer types, mutations in the TP53 gene result in loss of function, and such mutations are associated with poor prognosis. Wild-type p53 regulates diverse cellular processes, such as cell-cycle arrest, senescence, apoptosis, and autophagy. 7 p53-mediated induction of cell-cycle arrest fosters DNA repair and stabilizes the genome prior to cell division. At the same time, p53 can induce apoptosis by promoting expression of pro-apoptotic BCL-2 family members. Given its role in regulating the cell cycle, DNA repair, and apoptosis, the TP53 gene has long been a target for gene therapy to treat cancer. Gene therapy using wild-type p53 was achieved with rAd-p53 (Gendicine®) that consists of a recombinant adenovirus carrying a therapeutic wild-type TP53 gene in place of the E1 gene. 8,9 In rAd-p53-infected tumor cells, the adenovirus genome carrying the therapeutic TP53 gene is translocated to the nucleus where p53 protein is expressed. Restoring tumor suppressor functions and strong wt-p53 protein expression is effective against tumors. 8,10 –14 A series of studies has shown that p53 may play an antitumor role through the following mechanisms: (1) regulation of cell-cycle and apoptosis-related gene expression to induce apoptosis through transcription-dependent pathways in the nucleus and non-transcriptional pathways in the mitochondria and Golgi bodies 15 –23 ; (2) downregulation of multidrug resistance gene expression and subsequent increased sensitivity of tumor cells to chemoradiotherapy 24,25 ; (3) downregulation of VEGF gene expression and inhibition of tumor angiogenesis 26 –28 ; and (4) promotion of antitumor immune responses through bystander effect, so that a large number of immune cells such as natural killer (NK) cells accumulate near the tumor to kill tumor cells. 29 –32 It has been reported that rAd-p53 is very effective against a variety of malignancies, including colon, glioma, lung, ovarian, advanced head and neck tumors, and advanced cervical cancer. 13,14,33 –39 Several clinical trials involving rAd-p53 treatment, especially for head and neck tumors, have been carried out in China. 33,34,36,39 –42 In vitro and clinical studies conducted by Li et al. showed that rAd-p53 could strongly inhibit cell proliferation, induce apoptosis, and arrest the cell cycle in stage G1 in p53(–) oral dysplastic keratinocytes, and that patients with dysplastic oral leukoplakia exhibited clinical responses to rAd-p53 treatment. 41 rAd-p53 has been administered via intratumoral injection, perfusion, and intravenous (i.v.) infusion in various clinical trials. 33,34,39,41,43 –45 In the cases examined for this study, intratumoral injection and intraperitoneal (i.p.) perfusion were used for rAd-p53 administration. Here, it was found that rAd-p53 is also highly effective for treating uterine sarcoma in the clinic, which has not been reported previously. To evaluate the efficacy and safety of combined rAd-p53 and chemotherapeutic drugs, the clinical results of 12 patients treated at Shengjing Hospital between 2009 and 2015 were analyzed, with previous studies of the TP53 gene research taken into account for data analysis.
Methods
Patient selection and information
Of 12 cases of uterine sarcoma, 11 had recurrent cancer and one had primary cancer (patient 11). All patients were treated with rAd-p53 combined with chemotherapy. Clinical data for age, pathological type and stage, initial surgical treatment, postoperative adjuvant treatment, and recurrence interval were collected (Table 1). The patients ranged in age from 43 to 62 years old, with an average age of 52.25 ± 2.01 years. There were four cases of each pathological type: uLMS, CS, and ESS. Five patients were stage III, and one each had stage 1 and stage IV disease. The remaining five patients had unknown stage due to lack of original data. Adjuvant chemotherapy was performed in 3/11 cases of cancer that recurred after the first operation. Progression-free survival (PFS) time between the initial surgery and diagnosis of recurrence of all cases except for patient 11 was defined as PFS Time 1 (PFS1), which ranged from 1 to 18 months, with a median of 3 months. The patient with primary cancer underwent surgical treatment in the Netherlands. The tumor could not be resected due to a rich blood supply and extensive invasion of surrounding tissues. Pathological typing showed the tumor was CS.
General information on the 12 cases
LMS, leiomyosarcoma; CS, carcinosarcoma; ESS, endometrial stromal sarcoma.
Ethics approval
All patients in this study signed medical informed consent, and all agreed to treatment with rAd-p53 and chemotherapy. The study was approved by the Ethics Committee of Shengjing Hospital affiliated with China Medical University and was performed according to the tenets of the Declaration of Helsinki.
Local injection of rAd-p53 and bleomycin and i.v. infusion of chemotherapeutic agents
Recombinant adenoviral p53 (Gendicine®; ShenZhen SiBiono GeneTech, Shenzhen, China) is a recombinant human serotype 5 adenovirus. The E1 region of this adenovirus is replaced by a human wild-type p53 expression cassette. 36,46 Human embryonic kidney 293 cells grown in a bioreactor were used to produce the recombinant adenovirus, which was further processed and chromatographically purified. Recombinant adenoviral p53 at 1 × 1012 virus particles (vp) per 2 mL ampule was stored at −70°C. Frozen rAd-p53 was thawed at room temperature prior to use. rAd-p53 (1–2 × 1012 vp) was diluted in 4–10 mL of normal saline, followed by multipoint injection into the tumor under ultrasound guidance. If the tumor could not be punctured in the abdominal cavity or if there was a large amount of ascites, i.p. perfusion was performed. For i.p. perfusion, 2 × 1012 vp rAd-p53 was diluted in 500 mL of normal saline. Hepatic artery perfusion of rAd-p53 was performed selectively to treat liver lesions.
Chemotherapeutic agents to treat uterine sarcoma were bleomycin, cisplatin, isocyclophosphamide, and epirubicin. After 72 h at the peak of rAd-p53 transfection, patients underwent i.v. infusion of the PEI chemotherapy regimen: cisplatin (P; 60–70 mg/m2; day 1), epirubicin (E; 60 mg/m2; day 1), and isocyclophosphamide (I; 1.5; g/m2; days 1–3). At the same time, 15–30 mg local multipoint injection of bleomycin into the tumor was carried out under ultrasound guidance.
Patients in this study received two to five cycles of rAd-p53 combination treatment within 2–4 months. The rAd-p53 doses were 1–2 × 1012 vp per patient per treatment. The patients' vital signs were monitored for 1–2 h after each rAd-p53 injection. The combination chemotherapy began 72 h after the first rAd-p53 injection. The treatment periods were separated by 21 days.
After the rAd-p53 combination treatment, some patients received repeated salvage surgery. Post-treatment outcomes of patients who underwent no other salvage therapy after repeated surgery were assessed postoperatively. Patients who experienced post-treatment recurrence during follow-up were given additional chemotherapy with a new salvage therapy regimen. Post-treatment outcomes of these patients were assessed prior to salvage therapy.
Efficacy evaluation
The initial application of rAd-p53 was defined as the baseline period. Response Evaluation Criteria in Solid Tumors version 1.1 (RESIST1.1) were used to evaluate treatment efficacy, which was graded into complete remission (CR), partial remission (PR), stable disease (SD), and progressive disease (PD). The remission rate was calculated as (CR + PR)/total and the responsive rate as (CR + PR + SD)/total.
Follow-up
Follow-up was conducted as a clinic visit or via telephone interview after treatment up to the time of death or September 2017. The PFS time between the baseline period and the next recurrence was defined as PFS2. The time between the baseline period and death or September 2017 was defined as the overall survival time (OS).
Statistical analysis
SPSS for Windows v13.0 (SPSS, Inc., Chicago, IL) was used for statistical analysis. Quantitative data of skewed distribution were expressed as the median, and PFS curves and OS curves were estimated and plotted using the Kaplan–Meier method.
Results
Overall efficacy evaluation
The target foci of the 12 patients were located in the pelvic cavity and/or abdominal cavity. The sum of the longest diameters of target foci ranged from 2.8 to 32.4 cm, and the median was 13.2 cm. At baseline, two and three patients had liver and lung metastases, respectively. The maximum number of courses of rAd-p53 combined with chemotherapy treatment was five, and the average number of treatment courses was 2.5. Patient 3 was evaluated as CR (PR after rAd-p53 combined with chemotherapy treatment, and then achieved tumor-free survival after undergoing successful debulking surgery). In the remaining patients, seven patients achieved PR, three achieved SD, and one achieved PD. The remission rate (CR + PR)/total, 8/12, was 66.7%, and the responsive rate (CR + PR + SD)/total, 11/12, was 91.7% (Table 2).
Overall efficacy evaluation
No progression up to the end of follow-up.
Patient was alive at the end of follow-up.
SD, stable disease; PR, partial remission; CR, complete remission; PD, progressive disease.
Patients 9 and 10 had “good” PFS2 but “poor” OS. After treatment with rAd-p53 via intra-arterial infusion, the liver metastatic tumor in patient 9 regressed well (Supplementary Fig. S1A and B; before and after combined treatment; Supplementary Data are available online at
Follow-up continued through September 2017, with a maximum duration of 62 months and a median of 24 months. All 11 patients progressed, except for patient 3 who did not progress. PFS2 ranged from 2 to 62 months, with a median of 13 months, which was higher than that of PFS1 (median 3 months). The difference in median time between PFS1 and PFS2 was statistically significant (p = 0.0038; Fig. 1).

Progression-free survival time 2 (PFS2) ranged from 2 to 62 months, with a median of 13 months, higher than that of PFS1, the median of which is 3 months. The comparison between the two is statistically significant (p = 0.0038).
The OS (after the baseline period) of the 12 patients ranged from 6 to 62 months, with a median of 24 months. At the end of the follow-up period, only two patients survived. Patient 3 had no disease progression, and OS was 62 months. The PFS2 of the other patient, patient 6, reached 39 months after PR. This patient is currently living with the tumor and has an OS of 53 months. The remaining 10 cases died (Fig. 2).
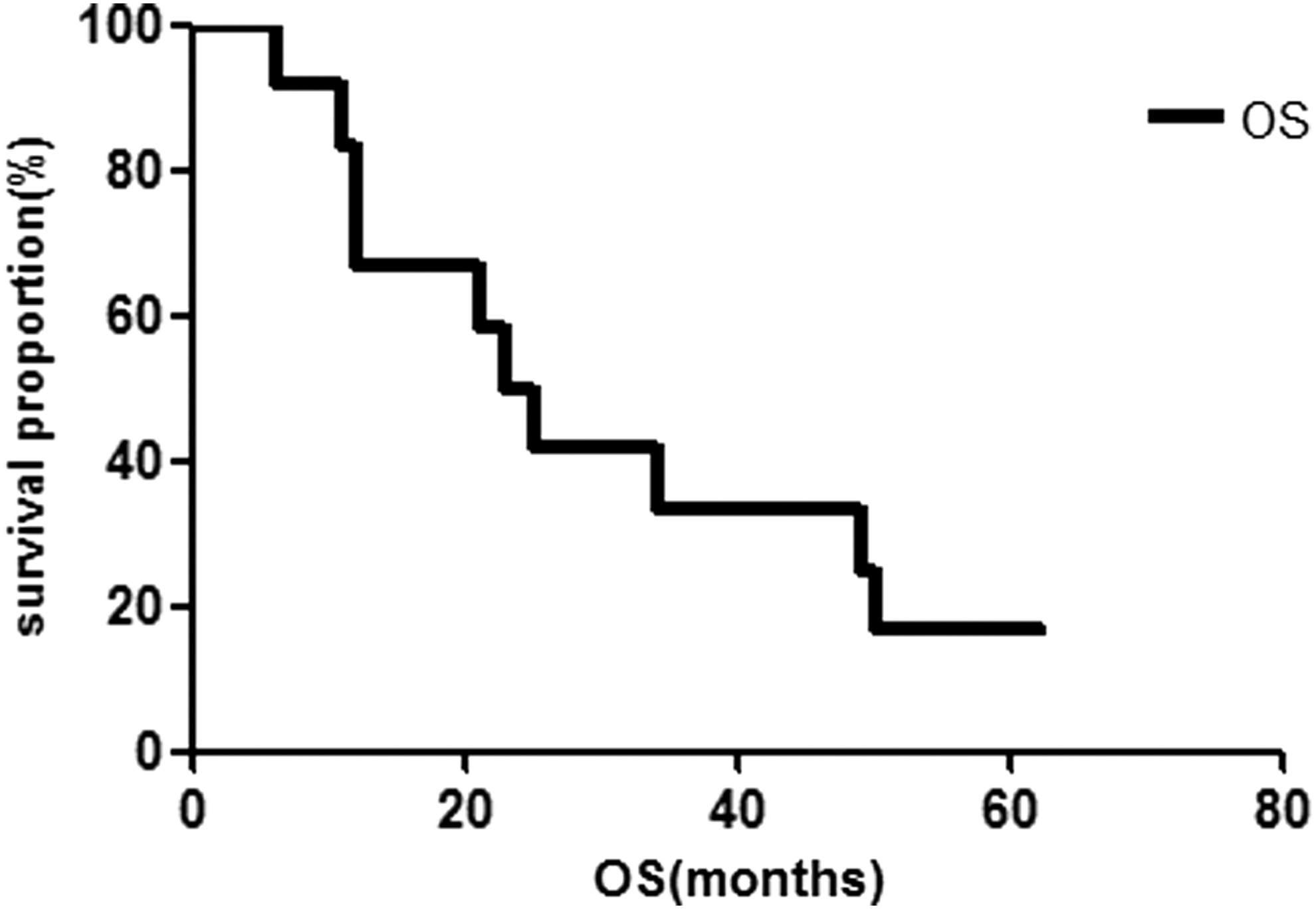
Overall survival (OS) time after the baseline period of the 12 patients ranged from 6 to 62 months, with a median of 24 months. Only two patients (patients 3 and 6) survived. The remaining 10 cases were all dead.
Operation results after combined treatment
Of the 12 patients, four (33.3%) could undergo repeated surgery after treatment with rAd-p53 followed by chemotherapy. Among these four patients, patient 3 (Supplementary Fig. S2A–C; before and after combined treatment and after repeated operation) and patient 5 (Supplementary Fig. S3A and B; before and after combined treatment) were found to have pelvic and abdominal recurrence 3 months after the initial operation and could not undergo surgery to the size of the lesion and its adherence to surrounding tissue/organs. After two courses of combined treatment with rAd-p53, the sum of the longest diameter of the target foci rapidly reduced to 22 cm and 7.8 cm, respectively, and successful tumor mass reduction (RO) was performed in both patients. At the end of the follow-up period, patient 3 had survived without tumor for 60 months and patient 5 had a PFS2 of 16 months and an OS of 50 months. The tumor of another patient, patient 7 (Supplementary Fig. S4A and B; before and after combined treatment), recurred 9 months after the initial operation, and recurred again in the pelvic cavity 2 months after the second operation. The target lesion diameter was 4.8 cm. After treatment with rAd-p53 combined with chemotherapy, the diameter of the lesion was reduced to 1.4 cm. After 9 months (PFS2), the size of the pelvic lesions in this patient slowly increased, and the patient refused chemotherapy, so a third tumor debulking surgery was performed. Without any treatment after the operation, the patient survived for 15 months without tumor, with an OS of 49 months. Pelvic tumor masses were found in patient 2 (Supplementary Fig. S5A and B; before and after combined treatment) about 3 months after the initial operation, with a diameter of 10.0 cm. The tumor reached the vaginal orifice through the vaginal cuff and was accompanied by pulmonary metastasis. After treatment with rAd-p53 combined with chemotherapy, the tumor diameter was rapidly reduced to 6 cm and the tumor became necrotic, softened, and fell away. The residual mass was removed completely without obvious bleeding. The pathological results showed denatured and necrotic tissue, and no tumor cells were found. The local vaginal lesions achieved remission pathologically. The patient ceased treatment for economic reasons and died from lung metastases progression.
Therapeutic effect on liver metastases
At the baseline period, two patients, patients 9 and 11, suffered from liver metastases. The liver lesions of patient 9 initially achieved PR after rAd-p53 combined treatment, but the patient later stopped using rAd-p53, and the liver lesions progressed and new lung lesions appeared. The tumor could not be controlled, and this patient died. The recurrent liver lesions were large and present in multiple locations in patient 11 (Supplementary Fig. S6A and B; before and after combined treatment), and the sum of the lesions' longest diameters was 14 cm. With one-time hepatic artery perfusion of rAd-p53 followed by two courses of pelvic focus rAd-p53 injection, the liver lesions disappeared completely, and the pelvic lesions rapidly reduced. The PFS2 for this patient was 30 months, and OS was 34 months.
Side effects
Considering fever following injection with rAd-p53 as a side effect, 8/12 patients had degree I fever, and all recovered without intervention. The other four patients had degree II fever and recovered after intramuscular injection of arginine acetylsalicylate. No other serious related side effects occurred.
Discussion
Tumors occur as a result of the accumulation of mutations in multiple genes. Among genes that encode proteins in the human genome, 550 carrying driver mutations could cause human cancer. p53 plays an important role in limiting gene mutations and stabilizing the genome and thus is called the “guardian of the genome.” 47 Although genomic instability is not required for tumorigenesis, deletion of p53 allows cells that carry a wide range of genetic errors to survive. 48 The emergence of genomic instability also increases the frequency of new gene mutations. Diverse gene mutations in tumor cells increase the malignant behavior of tumor cells, and can even lead to drug resistance after recurrence. 49,50 Together, these conditions can produce poor prognosis for cancer patients.
Several studies have highlighted the importance of p53 in cancer dynamics. Tumor cells lacking a wild-type p53 gene were shown to have significantly increased resistance to chemoradiotherapy. 51 A study by Wei et al. study showed chemoresistance in cancer that was previously been attributed to gene mutations or deficiency. 52 In addition, the presence of a wild-type p53 gene may increase the sensitivity of tumor cells to chemotherapeutic agents by downregulating MDR1 expression and upregulating that of TopoII α, which could even reverse the resistance of tumor cells to chemotherapeutic agents. 24,25 Introduction of Ad-p53 into a mouse model of breast cancer increased the number of apoptotic cancer cells, while the sensitivity to adriamycin increased by 18.1-fold, together with a 50% reduction in adriamycin IC50. Levels of MDR1 mRNA and P-glycoprotein all decreased in these mice. 53 Another study found that Ad-p53 combined with cisplatin, paclitaxel, doxorubicin, 5-FU, etoposide, and methotrexate inhibited tumor cell proliferation more efficiently in head and neck, ovary, prostate, and mammary gland cancers compared to chemotherapy alone. 54 In an in vivo study, wild-type human p53 gene increased the median survival time in a mouse model of pancreatic cancer by 37 days and increased the sensitivity of pancreatic cancer cells to gemcitabine. 55 Bleomycin-induced apoptosis was also reported to be related to the p53 gene. 56 Adenovirus-mediated introduction of a wild-type p53 gene and mutant type p53 gene into non-small-cell lung cancer and colon cancer lines showed that the bleomycin sensitivity of tumor cells expressing wild-type p53 was significantly higher than that of tumor cells expressing mutant type p53 gene. Furthermore, the sensitivity of wild-type p53 positive cells to bleomycin was reduced after transfection of a mutant p53 gene into wild-type p53 cells, while introduction of wild-type p53 gene into p53-deficient cells increased the sensitivity to bleomycin. 57
In this study, the median PFS1 was only 3 months after the first operation in patients with uterine sarcoma, indicating a very high degree of malignancy. At 72 h after intratumoral injection of rAd-p53 (the peak effect of viral vector transfection), bleomycin was locally injected into the tumor, and cisplatin, epirubicin, and isocyclophosphamide were infused i.v. These chemotherapeutic drugs affect DNA replication in tumor cells. The transfected wild-type p53 induces apoptosis of tumor cells with damaged DNA after chemotherapy treatment that enhances sensitivity of tumor cells to chemotherapy. In particular, the effectiveness of bleomycin topical treatment could not be ruled out. Bleomycin can cause cell death by intercalating into and cleaving DNA, and transfected p53 can enhance the likelihood that cells with damaged DNA will be cleared by apoptosis. As such, the chemotherapy agents and rAd-p53 could have synergistic and sequential effects that are important for increasing PFS. Indeed, following the combination therapy, the median PFS2 was significantly prolonged to 13 months. The longest OS without and with tumor was 62 and 53 months, respectively, demonstrating that rAd-p53 combined with chemotherapy can diminish malignant behavior of tumor cells to improve the prognosis of uterine sarcoma patients.
Although data concerning p53 mutation status were not available for the study patients, it is speculated that better treatment outcomes may not necessarily be attributable to correction of endogenous p53 mutations. Among the three pathological types of uterine sarcoma, ESS, LMS and CS, the frequency of TP53 gene mutation was high, particularly for LMS and CS: 17% (1/6 cases), 24% (55/255 cases), and 36% (59/164 cases), respectively. Meanwhile, the rate of p53 protein overexpression was 27%, 38%, and 73%, respectively. 58 As such, the likelihood of p53 gene mutation occurring in uterine sarcoma is high. An in vitro study conducted by Wolf et al. showed that exogenous p53 can be successfully expressed and detected as an immunoreactive protein. Moreover, exogenous p53 can upregulate p21 expression downstream of p53 in ovarian cancer cells, regardless of the expression status of endogenous p53. 59 Other studies of nude mice with ovarian cancer showed that p53 gene therapy combined with chemotherapy can enhance the expression of tumor suppressor genes, such as P21 and Bax, regardless of the expression status of endogenous p53. 60,61
Uterine sarcoma is a chemotherapy-insensitive tumor. One of the most effective chemotherapies for recurrent uterine sarcoma in current clinical practice is the isocyclophosphamide, doxorubicin, and cisplatin (IAP) regimen reported by Yamagami et al. 62 In the 11 patients with recurrent uterine sarcoma in this study, the CR + PR was 36.4% and the CR + PR + SD was 90.9%. In an earlier study, Hensley et al. treated 34 patients with recurrent uLMS using gemcitabine combined with docetaxel. The CR + PR for these patients was 52.9%, and the CR + PR + SD was 74%. 63 Here, the overall remission rate (CR + PR) and response rate (CR + PR + SD) for the chemotherapy combined with rAd-p53 regimen was 66.7% and 91.7%, respectively, which was significantly higher than that of other studies in the literature.
Because of the frequent insensitivity of radiotherapy and chemotherapy, surgery is still the first choice to treat recurrent uterine sarcoma. Unfortunately, around 70% of uterine sarcoma patients cannot undergo surgery due to the large size of pelvic and abdominal tumors, as well as tumor infiltration into surrounding tissues or distant metastasis (lung and liver metastasis). The proportion of patients who could eventually receive repeated surgery was even lower at <10%. In this study, four (33%) patients obtained satisfactory tumor reduction surgery after treatment with rAd-p53. They could not undergo surgery prior to this treatment because of recurrence of large pelvic and abdominal tumors, extensive invasion of pelvic organs, and “frozen pelvis.” All of these patients had the opportunity for reoperation after treatment with rAd-p53 combined with chemotherapy. During the reoperation for patient 3, the tumor showed a complete capsule, was limited in size, and had a poor blood supply (Supplementary Fig. S7). Most of the lesions were composed of necrotic tissue. The tumor in patient 2 reached the vaginal orifice through the vaginal cuff shortly after the initial operation. The tumor size was rapidly reduced after treatment with rAd-p53 combined with chemotherapy, and the residual mass could be completely removed without open surgery or obvious bleeding. The pathological results showed that the mass was composed of necrotic tissue and had no tumor cells. No new distant metastases were seen among the four patients, except for patient 5 who had liver and lung metastases. The analysis indicates that these outcomes may be related to p53 function.
As previously shown, deletion of wild-type p53 can induce gene amplification through cell-cycle changes. 64 Cells expressing oncogenes can thus continue to proliferate without restriction, and apoptosis ceases. Re-expression of wild-type p53 can restore cell-cycle regulation in tumor cells carrying mutant p53 alleles, which greatly reduces the frequency of gene amplification and DNA repair-related mutations, and also alters the malignant behavior of tumor cells by preventing accumulation of oncogene mutations. 65 In addition, the presence of decreased blood flow and an intact capsule in tumor tissues seen during reoperation, as well as diminished distant metastases, indicated that the physiological response of the p53 gene is not a simple on and off switch, but instead is part of a dense and interconnected network of multiple regulators and effectors. For example, studies have reported that p53 can inhibit tumor angiogenesis 26,27 while promoting DNA repair and apoptosis in tumor tissue. 66 p53 can also inhibit adhesion, invasion, and metastasis of tumor cells by downregulating expression of matrix metalloproteinases (MMP) 67 –69 and regulating the function of different sets of target genes under different conditions, leading to a series of cascade reactions. 70
In this study, patient 11 only received a one-time hepatic artery perfusion of rAd-p53 followed by two courses of pelvic focus injection of rAd-p53, but the liver lesions disappeared completely. The possible cause for this unexpected result could be due to a first pass effect of rAd-p53 and bleomycin injected i.p. into the pelvic tumor through the liver, as suggested by a study by Wang et al. in which injection of adenovirus vector showed virus accumulation in the liver 72 h after injection, which demonstrated a first-pass effect of the adenovirus vector in the liver. 71 Lung lesions of patients with lung metastases in this study were not well controlled, which indicated that rAd-p53 injected locally through the pelvic and abdominal cavity was basically depleted after the first pass effect of the liver. This outcome further showed that rAd-p53 plays an important role in combination therapy, which is supported by results from a clinical trial reported by Li et al., 40 indicating that intra-arterial infusion of combined rAd-p53 and chemotherapy significantly increased the survival rate of patients with oral squamous-cell carcinoma compared with intra-arterial chemotherapy. This possibility could be further verified by use of rAd-p53 therapy to treat pulmonary metastases.
In addition to maintaining genomic integrity and regulating the “classic” pathways of cell-cycle arrest and apoptosis, p53 also controls “non-classical” pathways such as autophagy, metabolism, and cellular plasticity. p53 also plays an important role in immune regulation. For example, p53 induces the senescence-associated secretory phenotype (SASP) to create an immunosuppressive microenvironment, and stimulates macrophages and NK cells to enhance immune surveillance and inhibit cancer. 72 p53 also directly regulates NK cell transcription, enhancing the ability of these cells to kill tumor cells, and activates the antitumor immune response. 73 Furthermore, a recent study found a new noncellular autonomous mechanism for p53, which stimulates the innate immune system to maintain tissue stability and inhibit tumorigenesis. 74
The rAd-p53 used in this study involved delivery of human wild-type p53 gene by a recombinant adenovirus type 5 vector that infects tumor cells. The main defense strategy of the human immune system against viruses is to activate interferon (IFN)-mediated immune responses. Type I IFN signaling can activate transcription of the p53 gene and then upregulate expression of genes that can promote cell-cycle arrest, apoptosis, and intracellular immunity. In turn, p53 target genes can promote the secretion and signaling of IFN, indicating that type I IFN and p53 are part of an important positive feedback loop of antiviral immunity. 75,76 Therefore, it is inferred that after application of rAd-p53, a positive feedback loop of antiviral immunity between IFN and p53 is formed. As the level of p53 increases, its action is more effective, allowing the viral vector of rAd-p53 to act indirectly as an antitumor agent.
Studies have shown that at a relatively low-stress baseline, p53 can also maintain the expression of many important tumor suppressor genes, including PTEN, STK11, MiR-34a, and KDM6A. 77 In this study, the OS of the longest tumor-free survival patient, patient 3, was 62 months. For patient 6, the residual tumor was stable for 39 months, and the tumor cells grew slowly. This patient survived with the tumor for 53 months, during which time the tumor may have behaved more like a benign mass and generated no distant metastases. This finding may indicate that rAd-p53 not only changes the malignant behavior of tumor cells, but could also mobilize the synergistic effect of immune surveillance and induce apoptosis in the tumor cell microenvironment.
In conclusion, rAd-p53 combined with chemotherapy is effective for treating various uterine sarcomas. For patients with recurrent lesions confined to the pelvic and abdominal cavity who cannot undergo surgery due to large tumor size or unclear tumor boundaries, rAd-p53 combined with chemotherapy can be effectively applied for two to three courses to create satisfactory opportunities for debulking surgery.
Footnotes
Acknowledgments
The authors wish to thank the doctors in the Department of Obstetrics and Gynecology, Shengjing Hospital of China Medical University, for their encouragement and collaboration for this research.
Author Disclosure
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.