
Abstract
One-year results are reported of the first lipoprotein lipase deficiency (LPLD) patient treated with alipogene tiparvovec, which is indicated for the treatment of patients with genetically confirmed LPLD suffering from acute and recurrent pancreatitis attacks (PAs) despite dietary restrictions and expressing >5% of lipoprotein lipase (LPL) mass compared to a healthy control. During clinical development, alipogene tiparvovec has shown improvement of chylomicron metabolism and reduction of pancreatitis incidence up to 5.8 years post treatment. A 43-year-old female presented with severe hypertriglyceridemia (median triglyceride [TG] value of 3,465 mg/dL) and a history of 37 PAs within the last 25 years, despite treatment with fibrates, omega 3 fatty acids, and—since 2012—twice-weekly lipid apheresis. LPLD was confirmed by identification of two different pathogenic variants in the LPL gene located on separate alleles and therefore constituting a compound heterozygous state. With a detectable LPL mass level of 55.1 ng/mL, the patient was eligible for alipogene tiparvovec treatment, and in September 2015, she receved 40 injections (1 × 1012 genome copies/kg) in the muscles of her upper legs under epidural anesthesia and immunosuppressive therapy. Alipogene tiparvovec was well tolerated: no injection site or systemic reactions were observed. Median TG values decreased by 52%, dropping to 997 mg/dL at month 3 and increasing thereafter. Within the first 18 months post treatment, the patient discontinued plasmapheresis and had no abdominal pain or PAs. In March 2017, the patient suffered from a PA due to diet violation. Within the first 12 months post treatment, overall quality of life improved, and no change in humoral or cellular immune response against LPL or AAV-1 was observed. In conclusion, alipogene tiparvovec was well tolerated, with a satisfactory response to treatment. Long-term effects on the recurrence of pancreatitis continue to be monitored.
Introduction
H
The condition often presents in early childhood or—in female patients—during pregnancy. Symptoms include severe abdominal pain, repetitive colicky pain, hepatosplenomegaly, the hyperviscosity syndrome, lipaemia retinalis, and eruptive xanthomas. However, the most debilitating symptom is the recurrence of severe potentially life-threatening acute pancreatitis attacks (PAs) that occur in 30% of patients. 1
Current treatments with fibrates and other lipid-lowering medications are inadequate. Responses to ultra-low-fat diets (<20% of the daily caloric intake) and the avoidance of simple carbohydrates and alcohol tend to be poor. Acute plasmapheresis may help during an episode of acute pancreatitis, but there is lack of proven evidence through randomized controlled trials. 2
Alipogene tiparvovec (Glybera®) is an adeno-associated virus (AAV) serotype 1 (AAV-1)-based gene therapy that results in sustained expression of the naturally occurring, gain-of-function S447X variant of the human LPL gene and subsequent synthesis and secretion of active LPL by the muscle cells 3 (Fig. 1). It is approved for the treatment of adults with genetically confirmed LPLD and an LPL protein mass >5% of normal, who suffer from severe/multiple PA, despite dietary fat restrictions. Administered as a one-time series of intramuscular injections in the upper and lower legs under spinal/regional anesthesia or deep sedation, 4 alipogene tiparvovec is the first human gene therapy to be licensed for use in the Western world. 5 Experience from clinical trials has shown a long-term expression of LPL protein in injected muscles, improved postprandial chylomicron metabolism, and a decreased incidence and severity of PAs for up to 6 years. Treatment is well tolerated. The most commonly reported adverse event in the clinical trial programme was a transient injection-site reaction that generally resolved within days. 6
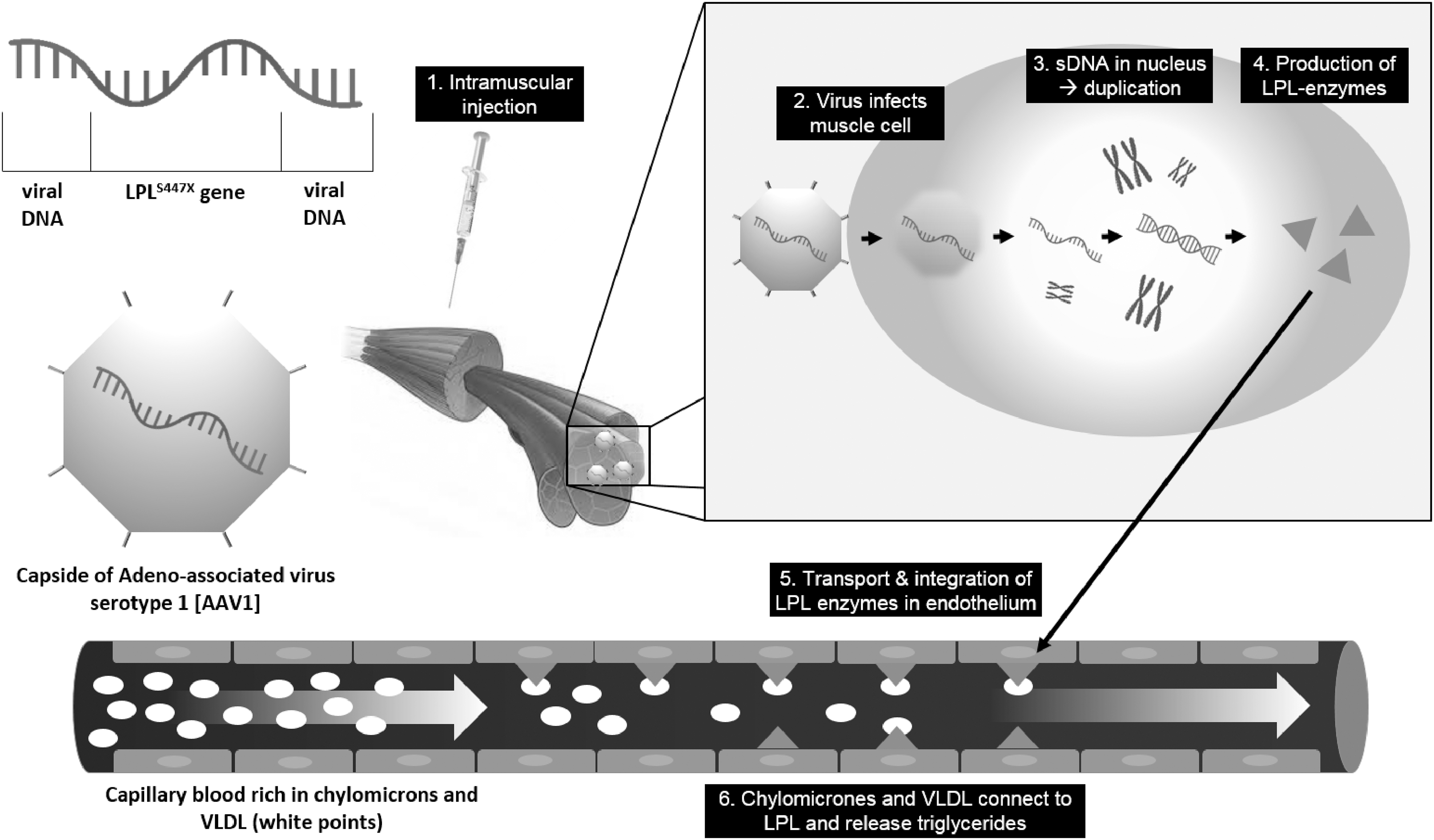
Molecular mechanism of alipogene tiparvovec. © Charité—Universitätsmedizin Berlin. DNA, deoxyribonucleic acid; LPL, lipoprotein lipase; s, serotype; VLDL, very low density lipoprotein.
As part of the Risk Management Plan—a regulatory requirement of the European Medicines Agency (EMA) and Health Canada—the “GENe therapy In the manAgement of Lipoprotein Lipase deficiency” (GENIALL) Registry was initiated in 2014 to collect data on disease characteristics and epidemiology of LPLD and to enable a continued evaluation of long-term safety and clinical response of alipogene tiparvovec. 7
This case report uses data from the GENIALL Registry to present the clinical results from the first patient treated with alipogene tiparvovec since EMA marketing authorisation.
History
A 43-year-old female presented at an outpatient lipid clinic with massive hypertriglyceridemia (triglyceride (TG) value = ∼3,500 mg/dL), despite ongoing therapy with micronized fenofibrate (160 mg/day), omega-3-fatty-acids (6,000 mg/day), and weekly lipid apheresis since September 2012. The patient had had elevated TGs since childhood and suffered from eruptive xanthoma. After other causes of severe hypertriglyceridemia were excluded, molecular genetic analysis revealed two variants in the LPL gene: c.440_443delACTA (p.N147TfsX24) and c.727T>A(p.C243S). The first variant was not described in literature, but due to its non-sense effect, it was classified as pathogenic. The second variant is listed in the Human Gene Mutation Database as causal for LPLD, 8 suggesting that the two identified variants are located on different LPL alleles, constituting a compound heterozygous status of two disease-causing variants. Allelic separation using a procedure involving ligation of polymerase chain reaction products containing both variants into a plasmid, transformation of bacteria with ligation products, and direct sequencing of plasmid inserts from bacterial clones, as described by Kassner et al. 9 confirmed compound heterozygosity for the identified LPL variants (Fig. 2).

Sequence analysis of the Lipoprotein Lipase (LPL) gene.
Despite life-style counseling (avoidance of alcohol, restriction of dietary fat and simple carbohydrates, and improvement of physical activity) and treatment with fenofibrate and omega-3-fatty acids, the patient's severe hypertriglyceridemia remained, with total TG levels between 2,574 and 4,367 mg/dL. Given the lack of response to therapy, the patient was referred for lipoprotein apheresis twice weekly for 2–3 h and underwent a total of 150 treatments between September 2012 and August 2015. TG levels were slightly reduced following each treatment by an average of 22% but typically returned to baseline levels.
The patient had a long history of PAs, compounded by an anatomical abnormality—a pancreas divisium—that increased her risk. Since her first attack during pregnancy 25 years ago, she reported >37 other attacks, 72% of which were confirmed by lipase values >1,000 IU/L. All attacks led to hospital admission, including one occasion, during a potentially life-threatening necrotizing PA, where she was admitted to the intensive care unit (ICU). Initial treatments, including biweekly lipoprotein apheresis, had no impact on the severity or frequency of these attacks. No signs of diabetes as a secondary complication of PAs have been observed to date. Whereas in the general European LPLD population in the GENIALL Registry the observed median number was five PAs per patient lifetime,
10
the 37 attacks observed in this patient were considered as an exceptionally high burden of disease. As the patient showed detectable levels of LPL mass (55.1 ng/mL), she was considered to be eligible for the first administration of alipogene tiparvovec therapy under daily practice conditions. She consented to enrolment in the GENIALL Registry in July 2014 for regular monitoring before and after treatment. As the patient was very slender, she prepared for treatment with physical training to strengthen the upper-leg muscles. To ensure diet compliance, the patient was trained to use a specific diet compliance app called “fatsecret” (
Results
Treatment with alipogene tiparvovec
After reimbursement was granted by her insurance company and informed consent was provided by the patient, treatment with alipogene tiparvovec was scheduled for September 8, 2015. To prevent any immunologic response to therapy, the patient started an immunosuppressive regimen, with mycophenolat-mofetil 500 mg 2-0-2 and ciclosporin 100 mg 1-0-1 3 days prior to treatment.
Based on the recommended dose of 1.5 × 1012 genome copies/kg of body weight and a maximum volume of 0.5 mL of solution per injection site, the patient required twenty 1 mL vials of alipogene tiparvovec, corresponding to a total of 40 injections. Injection locations were marked on the patient's upper thighs, and an epidural anesthetic was applied. The patient received an intravenous bolus of methylprednisolone (1 mg/kg) 30 min prior to the procedure, and injections were applied under aseptic conditions directed by ultrasound. The entire procedure took two hours and was without complications.
Injections were well tolerated, with no signs of inflammation at the injection sites (Fig. 3). Pain-relieving drugs were not required, and final blood controls revealed no clinically relevant immune reaction. As expected, TG levels remained high immediately following treatment due to the delayed onset of effect. The patient was discharged from hospital two days after administration.

Ultrasound controlled injection of alipogene tiparvovec and injection site of the upper legs one day after treatment with alipogene tiparvovec. © Charité—Universitätsmedizin Berlin.
Follow-up
Immunosuppressant therapy was stopped one month after treatment due to thrombocytopenia probably caused by cyclosporine. Despite this early termination of immunosuppressant therapy, no clinical signs of any local or systemic inflammation were observed.
Treatment with alipogene tiparvovec produced a 52% decrease in median TG levels 12 months after treatment (3,465 mg/dL pretreatment vs. 1,655 mg/dL post-treatment; Fig. 4). The lowest TG value of 997 mg/dL was observed 3 months after treatment, followed by an increase up to 2,456 mg/dL (month 6) and 1,974 mg/dL (month 12) thereafter, as expected based on results achieved during alipogene tiparvovec clinical development. Since the day of treatment, the patient has permanently discontinued the biweekly plasmapheresis procedure. The patient presented with a significant history of 37 PAs prior to treatment and did not report any PAs or abdominal pain within the first 18 months after treatment (Fig. 5). On March 20, 2017, the patient was hospitalized for three days for a PA due to diet violation (confirmed at her local hospital by an amylase value of 923 IU/L and abdominal ultrasound). TG levels at admission were at 2,569 mg/dL. After treatment with parenteral fluid substitution, zero-diet, and analgesic therapy, the patient fully recovered.
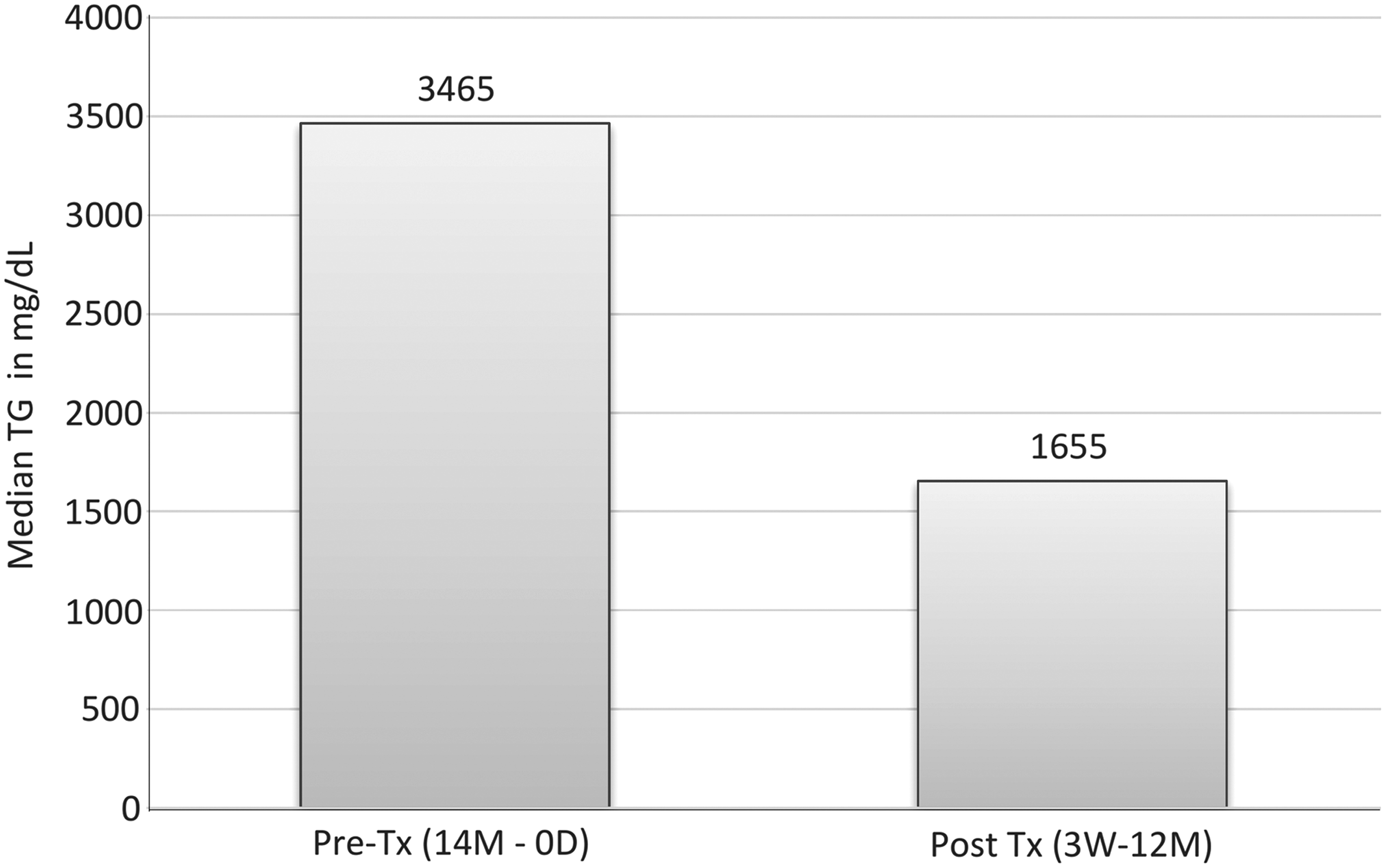
A 52% reduction in median triglyceride (TG) levels from enrolment 14 months before treatment (Pre-Tx) to treatment and after treatment (Post-Tx) with alipogene tiparvovec (week (W) 3 to month (M) 12) indicates response to treatment.

Pancreatitis attacks (PAs) before and after treatment with alipogene tiparvovec. No PA was observed within the first 18 months post treatment (Tx).
Treatment has been well tolerated, and no serious adverse events have been seen in the 20 months since administration. Results from immunological testing (before and 6 and 12 months post treatment) showed a preexisting positive humoral and cellular reactivity against the virus vector capsid (AAV-1) and no change after treatment. Specific T cells against LPL were observed neither before nor after treatment. The assay on LPL-specific antibodies showed a slight positive reaction before and after treatment, which was false-positive, as confirmed by an additional confirmatory assay. Overall, no change of humoral or cellular response before and 6 and 12 months after treatment was observed in this patient (Table 1).
Immunogenicity assessment
Measured with an enzyme-linked immunosorbent assay–based screening/confirmatory assay specific for AAV-1 or LPL. Serum samples were incubated in microtiter plates coated with AAV-1 or LPL and—after washing—with anti-human IgG/IgM/IgA conjugated with horseradish peroxidase (HRP), which binds to the Fc unit of any anti-AAV-1- or anti-LPL-Ab. Tetramethylbenzidine (TMB) reacts with bound HRP, and the amount of AAV-1/LPL Abs in the sample is related to color absorbance. A cutoff level for a positive or negative result was defined from screening of serum samples from 36 or 50 healthy volunteers, respectively. Positive results in the screening assay were subject to a confirmatory assay, in which samples were preincubated with and without AAV-1/LPL. A truly positive sample showed that preincubation with AAV-1/LPL inhibited the absorbance values above a predefined confirmation cutoff level.
Measured with a cell based assay specific for AAV-1 neutralizing antibodies with a reporter vector that carries a green fluorescent protein (GFP) gene, to which AAV-1 neutralizing antibodies bind. Transferred to wells seeded with HEK293 cells, any non-neutralized reporter vector will transduce cells and mediate expression of the fluorescent GFP measured via flow cytometry. Samples with a relative inhibition in fluorescence greater than the assay cut point were considered positive for AAV-1-specific neutralizing antibodies.
Measured by an ELISpot assay based on the detection and quantification of interferon (IFN)-gamma secreting cells upon stimulation with AAV-1 capsid or LPL in peripheral blood mononuclear cell (PBMC) samples. Cells were transferred to plates coated with a specific antibody against interferon-gamma and subsequently stimulated with AAV-1-capsid or LPL. After washing, addition of a conjugated labelled secondary antibody and subsequently a substrate solution, color development was initiated. Using an ELISpot reader, it was possible to quantify the number of spotforming cells (SFC) that were present in the test sample. Samples are said to be positive for AAV-1-reactive T cells when, upon stimulation with the antigen, the number of SPC is above a predefined assay cutoff, based on a negative control (cell media only).
Screening was positive, but confirmatory testing revealed negative response in all three samples.
The 6-month sample was uninterpretable due to lack of phytohaemagglutinin response (too few viable cells).
AAV, adeno-associated virus; Ab, antibody; LPL, lipoprotein lipase; Ig, immunoglobulin.
Whereas during the first 6 months post treatment the patient's QoL seemed to be impacted by the burden of follow-up visits and changing to a new job and buying a house, a clearer effect of QoL improvement was observed at the data collected during the 12-month post-treatment visit. The average overall QoL/overall health was impaired with a score of 63 points before treatment (reference score of general population: 72 points) 14 and improved to 83/100 points at month 12. Symptoms such as pain (general pain, pain during night, frequent bowel movements), fatigue (need to rest, feeling tired), body image (dissatisfied with body, less interest in sex, etc.), and worries about the future improved by >33% or disappeared completely. In contrast, the patient seemed to be more conscious about diet (felt more restricted in the types and amounts of food she could eat) and suffered from more indigestion (worsened by >33%). Other reported symptoms, including increased back pain and feeling weak in her arms and legs, were considered to be related to non-treatment reasons (e.g., her working environment as a nurse, or concomitant disease such as venous insufficiency).
Discussion
LPLD is a rare lipid disorder, and there is a need for greater understanding of the natural course of the disease, as well as the long-term outcomes following treatment with alipogene tiparvovec. This will be provided by data from the ongoing GENIALL Registry, which is the first and only initiative in this field, assessing the natural history of the disease, as well as the long-term safety and efficacy of gene therapy. 7
The patient presented in this case report suffered from 37 PAs in the last 25 years, all leading to hospitalization and one to ICU admission. The patient was undergoing biweekly plasmapheresis, a lengthy procedure of 2–3 hours per session, impacting on the patient's ability to work and her QoL. Within the first 18 months post treatment with alipogene tiparvovec, the patient discontinued plasmapheresis. The first pancreatitis occurred after 18 months post gene therapy treatment and discontinuation of plasmapheresis.
The patient's 52% reduction in median TG levels was sustained after 12 months of treatment. In the clinical trial programme, 5,15 –21 7/14 patients 20 reached a 40% reduction in median TG levels in the post-treatment period between 3 and 12 weeks (the primary endpoint, considered a “responder”). However, only six maintained that lower level after 26 weeks, and only four up to 5 years after dosing.
The effect of alipogene tiparvovec on reducing the number of PAs cannot be explained simply by a reduction in TG levels. 21 One possible mechanism is a shift in chylomicron metabolism from triglyceride-rich chylomicrons to triglyceride-rich very low density lipoproteins. This has been seen in clinical studies where alipogene tiparvovec has reduced the triglyceride content of the chylomicron fraction and the chylomicron TG/total plasma TG ratio throughout the postprandial period. 19 Measuring these changes in clinical practice is difficult. Currently, a radioactive tracer must be added to the patient's meal, and it was not possible to follow up our patient with this procedure in routine clinical practice. More practical and effective measurements to assess chylomicron metabolism changes need to be explored further.
A decision was made to stop immunosuppressant therapy with cyclosporine after only 1 month and earlier than the recommended 12 weeks, as the patient developed a thrombocytopenia probably aggravated by cyclosporine (as described in the SmPC), 22 but also known before in the history of the patient. Despite the early withdrawal of immunosuppressants, there were no clinical signs of any local or systemic inflammation. Immunology testing results showed a pre-existing humoral and T-cell reactivity against AAV-1 capsid before treatment, which did not change within the following 12 months of treatment. This is unsurprising, as it is known that peripheral blood mononuclear cells from healthy donors may harbour AAV-1 reactive T cells. What remains unknown is whether such T cell–mediated immunity has any effect on the efficacy of gene therapy. 23 An early study with alipogene tiparvovec did not use immunosuppressants, and all eight patients developed antibodies against AAV-1 capsid epitopes, and four developed a T-cell response against AAV-1. At the time, it was thought that the development of AAV-specific T cells could reduce the expression of LPL, as a similar effect in a gene therapy trial for haemophilia B had led to a loss of transgene-expressing cells. 21 However, later studies that did use an immunosuppressive regimen showed comparable humoral and cellular immune responses against AAV-1 capsid proteins to the trial without immunosuppressants. 24
QoL questionnaire results after 12 months show a slight improvement after treatment, in particular on pain and fatigue, but analysis of a single case is always difficult to interpret. In this case, other life changes (a new job and buying a house) may have interfered with the direct effect of the treatment on the patient's QoL. Additionally, no PAs occurred during the time QoL data were collected before treatment. If they had occurred, it is likely a greater QoL improvement would have been seen after treatment. A newly developed LPLD QoL questionnaire 12 and broader QoL data collection in the GENIALL Registry will contribute to better understanding of the impact of LPLD on patients' QoL. 7,10
Conclusion
Alipogene tiparvovec was well tolerated, and the efficacy outcome was satisfactory after 20 months of follow-up. Long-term effects on recurrence of pancreatitis are regularly monitored over a planned 15-year post-treatment period and will further contribute to better assessment of the efficacy and safety of alipogene tiparvevec. As the shift in chylomicron metabolism likely underlies the ability of alipogene tiparvovec to reduce the number of PAs, more practical and effective measurements are needed to assess chylomicron metabolism changes.
Entering daily practice of gene therapy in rare disease is still a challenge due to the ultraorphan nature of the disease itself, the number of restrictions making patients eligible for treatment, as well as the difference of reimbursement systems in the different European countries. Since marketing authorization in Europe of alipogene tiparovec in 2012, this is the first patient to be treated with alipogene tiparvovec in daily practice. Patients treated with alipogene tiparvovec might still benefit (e.g., by less strict diet restrictions) from other pharmacological treatment options in development for the treatment of LPLD. These include antisense oligionucleotides directed against ApoC-III and angiopoietin-like 3 protein mRNAs, diacylglycerol acyltransferase 1 inhibitors, and microsomal triglyceride transfer protein. 24 It is hoped that in the near future, these currently investigational therapies may offer further pharmacological interventions for individuals with LPLD.
Footnotes
Acknowledgments
GKPharmacomm assisted with the editorial preparation of this manuscript, funded by Chiesi pharmaceutici.
Author Disclosure
E.S-T. as GENIALL Steering Committee member has received consulting fees from uniQure/Chiesi. U.K. was involved in clinical trial with Sanofi, Amgen, IONIS, Pfizer, and MSD, and received honoraria for advisory boards and presentations within educational programs from Sanofi, Berlin Chemie, Amgen, Aegerion, Alexion, and Fresenius. M.D. has received consulting fees from uniQure. I.D. received a research grant from Sanofi and honorary for consultancy from uniQure biopharma B.V. T.G. received honoraria for lectures from Fresenius Medical Care. T.H. and M.W-D. have no conflict of interest.