
Abstract
Chronic renal disease or acute renal injury could result in end-stage renal disease or renal failure. Sonoporation, induced by ultrasound-targeted microbubble destruction (UTMD), has evolved as a new technology for gene delivery. It increases the transfection efficiency of the genes into target kidney tissues. Moreover, UTMD-mediated gene delivery can directly repair the damaged tissues or improve the recruitment and homing of stem cells in the recovery of injured tissues, which has the potential to act as a non-viral and effective method to current gene therapy. This article reviews the mechanisms and applications of UTMD in terms of renal disease, including diabetic nephropathy, renal carcinoma, acute kidney injury, renal interstitial fibrosis, nephrotoxic nephritis, urinary stones, and acute rejection.
Introduction
A
Numerous physical, chemical, and pharmacological strategies have been developed with nanosized particles, chemical agents, and recombinant virus to deliver genes, drugs, and stem cells into target tissues. 2 However, for these therapies, the shortcomings of inflammatory reactions and low targeting remain to be overcome. 3 Therefore, an efficient, safe, and noninvasive method to deliver genes, drugs, and stem cells into target cells is needed. In recent years, studies have indicated that ultrasound-targeted microbubble destruction (UTMD) has developed rapidly for systemically targeting genes and drugs. Upon ultrasound exposure, microbubble destruction generates microjets or microstreams that create shear stress on cells and form transient pores in cell membranes, which could enhance cell membrane permeability transiently. This method, named “sonoporation,” allows the microbubble-packaged circulating agents to enter selectively into target tissues/organ of interest 4,5 (Fig. 1). This article provides a review of UTMD-mediated gene therapy for various renal diseases (see Table 1).
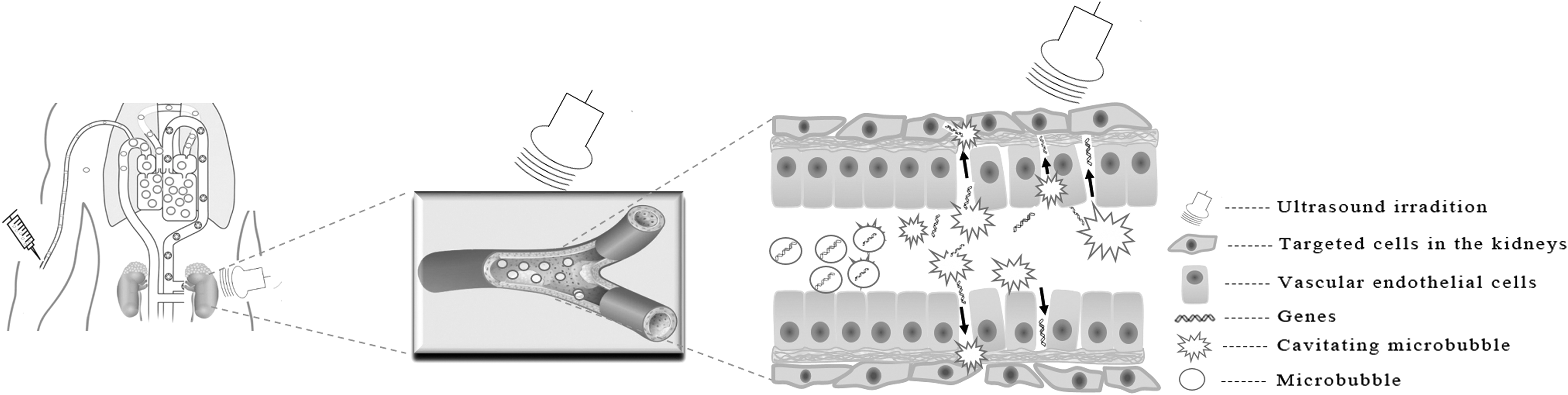
Schematic overview of sonoporation-enhanced blood vessel permeabilization. Genes bearing microbubbles were injected intravenously. Under irradiation of ultrasound, microbubbles were ruptured and subsequently disrupted the vascular endothelial integrity, perturbed cellular membranes, and increased the permeability of target cells.
Preclinical studies of UTMD in various kidney diseases
UTMD, ultrasound-targeted microbubble destruction; STZ, streptozotocin; TGF, transforming growth factor; NF-κβ, nuclear factor kappa beta; MI, mechanical index; ROS, reactive oxygen species; BMSCs, bone mesenchymal stromal cells; RCC, renal cell carcinoma; rAAV, recombinant adeno-associated virus; AKI, acute kidney injury; TNF, tumor necrosis factor; IL, interleukin; UUO, unilateral ureteral obstruction.
Current Status of Gene Therapy for Renal Diseases
Gene therapy for renal diseases
With the application of gene therapy in clinics, renal gene therapy has gained much attention because of its efficacy and safety characteristics. Current technology for renal delivery systems of therapeutic genetic materials into target tissue can generally be divided into viral vector–mediated systems and non-viral vector–mediated gene transfer systems. Over past decades, the advantages and disadvantages of the viral and non-viral vector-mediated gene transfer methods have been seen. 6
Commonly, adenovirus, adeno-associated virus (AAV), and lentivirus have been reported as viral vectors in gene transfer. 7,8 Viral systems can offer high efficiency of delivery into cells with sustained expression. Recently, Liu et al. showed that the selenoprotein P plasma 1 (SEPP1) gene could be expressed across human clear-cell renal cell carcinoma (RCC) cells by packaging the plasmid pLV-EGFP (2A) Pure-SEPP1 into the lentivirus system. 9 Schievenbusch et al. conducted a study to develop a new strategy based on AAV vector platforms to prevent renal fibrosis. They identified AAV serotype 9 (AAV9) as the most suitable delivery vector, and injected rAAV9-CMV-Ksp-hHGF into the genetic mouse model of renal tubulointerstitial fibrosis COL4A3-deficient mice by the tail vein. Results showed a remarkable attenuation of tubulointerstitial fibrosis and repression of fibrotic markers, such as collagen 1 alpha 1, platelet-derived growth factor receptor-beta, and alpha-smooth muscle actin (SMA), demonstrating the great potential of rAAV9 as an intravenously applicable vector for the combined paracrine and endocrine expression of anti-fibrogenic factors in the treatment of renal failure caused by tubulointerstitial fibrosis. 10
However, safety concerns associated with viral vectors have consistently been a focus. Viral vectors may lead to uncontrollable and insertional mutagenesis through integration of viral DNA into host chromosome and then trigger cell malignant transformation resulted by certain oncogene activation or tumor suppressor gene inhibition. 11,12 In addition, viral vectors have the potential to evoke immune responses, regardless of the vector or transgene constructs preparation, which could limit repetitive regimens. 3,13,14 These potential disadvantages may limit the therapeutic effects and hamper further development for renal disease gene therapy, which is required to develop non-viral delivery methods with low cytotoxicity, immunogenicity, and high biosafety. Non-viral methods for renal gene therapy have developed rapidly in the last decades due to their low cost, reduced pathogenicity, ease of production, and the major advantage of safety compared to viral vectors. However, there has been a long period where the application of non-viral gene delivery has been ignored because of poor efficiency and low expression of the transgenes. 15 Non-viral delivery consists of both chemical and physical methods. Physical methods include electroporation, gene gun, microinjection, and iontophoresis, directly delivering genes into the cell cytoplasm or nucleus, while chemical methods using carrier molecules include cationic lipids, polymers, and nanoparticles (NPs) to combine the negatively charged genes. 16
With its small structural size and optical and electronic characters, the nano-carrier system has overcome various issues related to a conventional viral delivery system, including lack of targeting capability. NPs are smart and are being engineered for imaging contrast agents and anticancer drugs. They are also favorable as carriers in tumor therapy by taking advantage of pathophysiological conditions, such as the spatial variations in the pH value and the enhanced permeability and retention effect. Target drug delivery carriers are capable of ferrying therapeutic genes or therapeutic agents into target disease sites while sparing healthy tissues. 17,18
However, non-viral vector-mediated gene transfer remains inefficient, and the expression duration is relatively short compared to the viral delivery method. 19 –21 Besides, the invasive operative procedure may reduce patient compliance for effective therapy. Therefore, the physical method is inappropriate for renal gene transfer because the inherent defects may outweigh the merits. Thus, the current aim is to develop a clinically efficient and safe gene transfer method. 22
The UTMD-mediated gene delivery system, with its advantages of high safety, low toxicity, specific tissue targeting, and repetitive applicability, fulfills this aim. 23,24 In 1996, Porter et al. first reported that perfluorocarbon-exposed sonicated dextrose albumin microbubbles could combine with synthetic antisense oligonucleotides and then release them in the presence of diagnostic ultrasound. 25 Generally, the main obstacles for gene delivery to target tissues are the endothelial barriers, which are formed by close apposition and alignment of endothelial cells. 26 These barriers could hinder the entry of exogenous genes into target cells when genes are administered intravascularly. Furthermore, the unique anatomy of the kidney could limit effective gene delivery due to the existing vascular endothelium barrier, which prevents the delivery genes from repairing capillary endothelial cells and visceral epithelial cells. Additionally, the exogenous genes need to be transferred across the nuclear membrane to enter the nucleus for efficient gene expression. 27 Therefore, both extracellular and intracellular barriers need to be overcome in renal gene therapy.
UTMD improves the recruitment and homing efficiency of stem cells
Bone mesenchymal stromal cells (BMSCs) are able to repair renal organs and could improve renal function. 28 The mechanisms in the process are related to paracrine and/or endocrine factors secreted by BMSCs from a cisplatin-induced renal damage model, such as VEGF, HGF, IGF1, and EGF, 29 –31 which could be a promising approach to cure many kidney diseases. In acute renal failure and DN, BMSCs were successfully functional. 32,33 Intravenous injection was used to deliver the BMSCs because of its noninvasive and promising therapeutic characteristics. While the number of BMSCs homing to kidney tissue was at very low levels (<0.1% injected dose), this limited the effective implementation of BMSC-based therapies. 34,35 The process inducing BMSCs homing to tissues involves several steps, including the chemotactic response by chemokine–chemokine receptor interactions, attachment to vascular endothelial cells, and trans-endothelial migration into the parenchyma. 36 –38
UTMD technology could be utilized for the targeted delivery of BMSCs. It improves the recruitment and homing efficiency of BMSCs. Tang et al. showed that a mild inflammatory response was induced at an intensity of 1.0 W/cm 2 ultrasound, which could enhance the homing number of BMSCs into acute kidney injury (AKI) tissue and improve kidney recovery. 39 However, the mechanisms of BMSC homing induced by UTMD are not clear. Studies have suggested that changes in the regional microenvironment are related to BMSCs' adhesion and migration, and subsequent transmigration into inflamed tissues. 40,41 Under irradition of UTMD, expression of various cytokines, integrins, and growth factors was increased. 42 Although current evidence suggests UTMD-promoted BMSC homing is related to microenvironmental changes, the mechanisms need to be further elucidated.
MEchanisms and Effects of Ultrasound Contrast Agent–Mediated Gene Therapy
UTMD promotes the uptake of surrounding macromolecules such as drugs or plasmids into target tissues, indicating a promising method for target-specific and noninvasive delivery. Reports have shown that UTMD enhances cavitation erosion and downregulates the cavitation threshold, which could cause a “spillover space” in the surface of a cell membrane lasting up to 24 hours, thus providing a way for gene entry. 43 When the acoustic pressure reaches a certain threshold, microbubbles violently collapse and induce production of intracellular reactive oxygen species and free radicals. 44 In this process, cell membrane pores are transiently formatted, resulting in an increase in membrane permeability. 45 Acoustic cavitation is regarded as the putative primary mediator of sonoporation, which is considered an interaction between disseminating gaseous inclusion and ultrasound pressure in aqueous media. 46 Hauser et al. found that under irradiation of low-intensity ultrasound, stable cavitation of microbubbles could increase the endocytotic activity of cultured cells. 47 In a review by Sirsi and Borden, the mechanisms of UTMD-mediated vascular permeability alternation were categorized into three different classes: (1) formation of transient pores in vascular endothelial cells, (2) disruption of the integrity of the vascular endothelium, and (3) stimulation of cellular uptake. 4
However, the most important factor in achieving efficient and controlled transfection is finding the optimal combination of the various transfection parameters. Usually, to obtain safe and effective delivery parameter conditions, researchers need to optimize the varied ultrasound parameters (such as sound intensity, frequency, duty cycle. and duration of exposure) and the concentrations of microbubble and DNA using the method of orthogonal experimental design.
Generally, the formation of pores in the lipid bilayer could be caused by high-intensity ultrasound alone and enhanced by the addition of microbubbles. 48 When microbubbles near cellular membranes are exposed to high-energy pulses, the microbubbles collapse, which results in high shear stress from streaming and shock waves that can lead to pore formation. 49 In addition to creating openings in cells, the cavitation response of microbubbles may also facilitate the uptake of exogenous substances such as genes into the cells through microjets. 50 Research suggests that large molecules (such as dextrans) as well as NPs can enter into the interstitial space after sonication with microbubbles. 51 –53 This vascular permeability is believed to be the result of the interaction between the microbubbles and vessel walls. Chen et al. found that volumetric expansion of the microbubbles could promote the bubbles and vessels to interact with each other. However, the oscillation could embed into the endothelium, altering vascular permeability. 54 Caskey et al. studied the effects of insonated microbubbles within ex vivo vessels and observed both asymmetric collapse and jet formation near the vessel wall. 55 With the help of high-speed photomicrography, Chen et al. studied the translational dynamics of signal microbubbles within ex vivo vessels and observed that jet formation occurs away from the vessel wall. 56,57 These studies provide evidence for understanding the physical interactions between microbubbles and vessels.
Application of Utmd-Mediated Gene Therapy for Renal Diseases
UTMD-mediated therapy in DN
DN, one of the main complications in diabetic patients, is the primary cause of end-stage renal failure around the world. 58 Studies have shown about 20–30% type I or type II diabetes mellitus patients are likely to develop DN, which increases premature mortality and morbidity in diabetic patients. 59,60 Kidney transplantation, the preferred therapy method for DN, is frequently limited due to the need for lifelong immunosuppression and the scarcity of transplantable donors. Other palliative therapeutic methods, including control of hypertension and intervention for high glucose levels, are just applied to delay the development of DN. Strong evidence indicates tight control and early intervention have the potential to slow or even reverse the progression of early DN. 61,62
UTMD provides a novel approach for the treatment of DN. Zhang et al. demonstrated that UTMD could increase the renal interstitial capillary permeability in early DN rats with no hemorrhage or necrosis by renal histology, indicating this might be a considerable therapy for enhancing delivery of drugs, genes, antifibrotic agents, or stem cells into the kidneys. 62 Furthermore, UTMD was able to deliver genes effectively and safely into the kidneys of db/db mice. Chen et al. investigated the protective role of Smad7 in a streptozotocin-induced DN mouse model and found that UTMD-mediated Smad7 transfection significantly decreased the development of microalbuminuria, transforming growth factor beta (TGF-β)/Smad3-mediated renal fibrosis, and nuclear factor kappa beta (NF-κB)/p65-driven renal inflammation. 63 Subsequently, Ka et al. further determined that overexpressed Smad7 by UTMD markedly repressed the activity of TGF-β/Smad3 and NF-κB signaling pathways, thus inhibiting diabetic kidney injury, including proteinuria, renal fibrosis, and podocyte and endothelial cell injury. 64 Besides, overexpression of kallistatin by UTMD reduced serum creatinine and BUN levels, which ameliorated glomerulosclerosis and tubulointerstitial injury and attenuated renal fibrosis by inhibiting TGF-β, thus protecting against DN in db/db mice by suppressing the interaction of advanced glycation end products and its receptor AGE-RAGE-induced oxidative stress. 65
Recently, microRNAs were the focus of UTMD-mediated delivery because of its regulation of DN onset and progression. 66 –68 MicroRNA-21 has been proved to be closely associated with fibrosis. 69,70 To investigate the therapeutic potential of microRNA-21 in diabetic kidney injury, Zhong et al. transfected microRNA-21 knockdown plasmids into the diabetic kidneys of db/db mice using UTMD technology. They found that knockdown of microRNA-21 restored Smad7 levels and suppressed activation of the TGF-β and NF-κB signaling pathways, leading to DN amelioration, along with decreased renal inflammation, microalbuminuria, and fibrosis. 71 MicroRNA-29b, a downstream inhibitor of TGF-β/Smad3-induced fibrosis and acting as a biomarker for fibrosis, may have therapeutic potential for DN. 72,73 Under diabetic conditions, Chen et al. found microRNA-29b was downregulated and associated with renal fibrosis and inflammation. However, restored renal miR-29b by UTMD was able to inhibit TGF-β-driven fibrosis and NF-κB-mediated inflammation, thus attenuating DN complications. 74 Besides the TGF-β pathway, another small GTPase, Rap1, regulates cell adhesion and proliferation. When Rap1 is delivered to the streptozotocin-induced DN mouse model, results show a decrease in DN progression and attenuation of tubular injury primarily by modulating mitochondria-derived oxidative stress. 75
In addition, transplantation of stem cells is also considered as a novel way to treat DN. Mesenchymal stem cells (MSCs) are reported to differentiate into several cell types, such as functional insulin-producing cells 76 and renal cells, 77 which may ameliorate hyperglycemia and improve renal function. 78 Zhang et al. demonstrated that transplantation of BMSCs reverted hyperglycemia and reduced renal damage. Under optimum parameters, BMSC transplantation decreased blood glucose concentrations and attenuated pancreatic islets/β-cell damage, resulting in an increase of renal interstitial capillaries permeability and VCAM-1 expression, which enhanced homing and retention of BMSCs to the kidneys. 79
Stromal cell-derived factor 1(SDF-1) is necessary for BMSCs homing through interaction with its specific functional receptor CXCR4. Wu et al. developed new covalent conjugated SDF-1-loaded microbubbles, which could improve MSC homing to DN kidneys. After the target release of SDF-1, the homing efficacy of MSCs to DN kidneys was remarkably ameliorated. 80 Besides, BMSCs show promise as a strategy because of their renoprotective potential. 81 Wang et al. demonstrated UTMD could increase the SDF-1, VCAM-1, E-selectin, and VEGF levels, which provide a suitable microenvironment for BMSC transplantation to diabetic kidneys. 82 In addition, UTMD directed to the pancreas also contributes to attenuating DN progression. Here, UTMD technology could induce islet cell regeneration through delivering insulin-regulated genes 82,83 and islet regeneration genes. 84 Compared to conservative therapy, UTMD enables gene or stem-cell delivery to the tubulointerstitial area, thus enhancing the therapeutic effect and slowing disease progression, or perhaps in the near future even reversing the progression of DN in clinical practice.
UTMD-mediated therapy in renal carcinoma
RCC is a neoplasm of the renal epithelium and accounts for approximately 90–95% of malignant neoplasms. 85,86 Recently, gene-therapy strategies have been employed for RCC with new molecular biology developments.
rAAVs are vectors of low immunogenicity and stable long-term transgene expression. 87 However, in certain cases, there may be fewer or non-permissive cell types or tissues when rAAV is used as the gene delivery vehicle. In a study by Lipkowitz et al., renal cancer cells showed only 2% transduction efficiencies of rAAV but 50% in rAAV-permissive Hela cells. 88 With the combined treatment of UTMD, the viral transfer efficiency was enhanced two- to threefold without affecting cell viability, and in vitro studies also showed an increase of rAAV2 transfer in tumors. Thus, UTMD enhanced rAAV2 transfer into less permissive RCC cells and tumors, resulting in inhibition of tumor growth. 89
Different from the viral transfer method, antibodies conjugated to the shell of microbubbles through avidin–biotin interaction lead to an accumulation of microbubbles in target sites after intravenous injection, providing new possibilities for diagnostic ultrasound imaging and drug delivery. 18 In a study by Wei et al., an anti-VEGFR2 antibody was conjugated to microbubbles and intravenously administered into an orthotopic mouse model of human RCC. As a result, microbubbles targeting VEGFR2 exhibit suitable properties for imaging angiogenesis in orthotopic models of RCC. 90 Thus, UTMD-mediated gene therapy may be a useful tool in the gene therapy of renal carcinoma.
UTMD-mediated therapy in AKI
AKI, frequently the consequence of ischemic insults, to a great extent remains a cure-resistant problem in clinics, with high mortality and morbidity rates. 91 Studies often use the renal ischemia–reperfusion injury (I/R) model to study the ischemic AKI mechanisms and treatment strategies further. Reports have shown inhibition of tumor necrosis factor alpha (TNF-α) ameliorated renal fibrosis. 92,93 Furthermore, Ryo et al. demonstrated that reduction of TNF-α expression by UTMD-mediated siTNF-α transfection inhibited the levels of kidney injury markers, such as kidney injury molecule-1 and neutrophil gelatinase-associated lipocalin, suggesting systemic administration of siRNA by UTMD could be applicable in the recovery of AKI. 5
In addition to gene therapy, intravascular transplantation of BMSCs is a promising therapeutic approach for AKI. BMSCs are reported always to home to AKI kidneys and differentiate into tubular epithelial cells, thus improving the morphologic and functional alterations. 30 However, only a limited number of BMSCs home to the target tissue. The functional CXCR-4 chemokine receptor on the surface of BMSCs decreases when passaged in culture, which impairs the homing and repair ability of BMSCs. Therefore, strategies have been developed to improve BMSCs' homing ability by upregulation of CXCR-4 receptors in BMSCs. Wang et al. found that combining UTMD and liposomes or polyethylenimine increases the recombinant plasmid pDsRed-CXCR4 transfection efficiency in vitro. Following transfection, they further proved a ninefold higher migration ability of CXCR4-modified BMSCs than control. The following in vivo experiments showed three times more transplanted BMSCs were homing and located in AKI kidneys, indicating overexpression of CXCR-4 under UTMD, which could significantly augment BMSCs' homing ability within the AKI microenvironment. 35,94 These studies provide a new approach for BMSC-based therapy of AKI, although more research needs to be conducted before clinical application.
UTMD-mediated therapy in renal interstitial fibrosis induced by a unilateral ureteral obstruction model
Renal interstitial fibrosis is a common feature of various kidney diseases that develop in end-stage renal failure. Both unilateral ureteral obstruction (UUO) and a rat remnant kidney model are used to research progressive renal diseases. 95 TGF-β acts as a key mediator in the progression of renal fibrosis. 96 Blockade of TGF-β1 with a neutralizing antibody or anti-sense oligonucleotides attenuates renal scarring, whereas overexpression of TGF-β1 may lead to renal fibrosis. 97,98 Other reports show TGF-β1 increases extracellular matrix protein synthesis through a Smad-dependent pathway. 99 To address the role of TGF-β1/Smad7 signaling in renal fibrosis, Hou et al. constructed a rat remnant kidney model. They transferred a doxycycline-regulated Smad7-expressing plasmid using an ultrasound microbubble–mediated delivery system. Results indicate that Smad7 transgene expression within the kidney blocks TGF-1/Smad7 signaling and could improve tubulointerstitial fibrosis, renal tubular atrophy, and renal tubulointerstitial mononuclear cell aggregation, 100 indicating a potential therapeutic target of TGF-1/Smad7 for treatment of renal fibrosis. In addition, the antioxidation related genes, such as intermedin, connective tissue growth factor (CTGF), and mir-433, are also reported to improve renal fibrosis. 101 –103 Qiao et al. locally overexpressed exogenous intermedin in the kidneys of a rat UUO model with an ultrasound microbubble–mediated delivery system. As a result, overexpression of intermedin remarkably attenuated UUO-induced tubular injury and blunted fibrotic response. In addition, intermedin relieved the UUO-caused α-SMA and CTGF upregulation, whereas TGF-β1 upregulation and Smad2/3 activation were not affected. 102 In line with this report, Wei et al. found knockdown of CTGF, with shCTGF plasmid-carrying microbubbles and ultrasound in a mouse UUO model, decreased the interstitial deposition of TGF-β1, a smooth-muscle actin and type I collagen, as well as reduced renal fibrosis in pathologic alterations. 103 Taken together, current research indicates that UTMD technology could provide a meaningful reduction in renal disease severity by transferring antifibrosis-related genes.
UTMD-mediated therapy in nephrotoxic nephritis
Stanniocalcin-1 (STC1), an intracrine protein, functions by having an anti-inflammatory and cytoprotective effect by inhibiting macrophages and preserving endothelial barrier function. In the STC1 transgenic mouse model, inhibitions of reactive oxygen species and renal ischemia–reperfusion injury were observed. 104,105 The shRNA transgenic mouse model is normally realized through expression of STC1 shRNA or scramble of shRNA, upon removal of a floxed reporter. UTMD technology can also deliver tyrosine kinase receptor- 2 promoter-driven Cre to the kidney to permit kidney-specific shRNA expression. As a result, delivery of tyrosine kinase receptor 2 promoter-driven Cre to STC1 shRNA transgenic kidneys can diminish the expressions of STC1 mRNA and its protein in the kidneys. STC1 silence knockdown can lead to severe proximal tubule injury characterized by a series of reactions such as vacuolization, greater generation of superoxide, cell apoptosis, and kidney failure. 106,107 With the UTMD technology to deliver Cre-expressing plasmid, knockdown of STC1 could be conditional controlled, which would provide a new way to study the mechanisms of nephrotoxic nephritis.
UTMD-mediated therapy in urinary stones
Urinary stones occur in approximately 7% of women and 13% of men. Extracorporeal shockwave lithotripsy was the first method used to fragment the stones by the formation of cavitation bubbles. However, with this method, nearly half of urinary-stone patients experienced a recurrence within 5 years. 108 The main component of most kidney stones is hydroxyapatite, which has a high affinity to bisphosphonates. 109 Microbubbles equipped with bisphosphonate tags could combine specifically with the stone but not the surrounding tissue. The method used to deliver microbubbles to the stones depends on where the stones are located. For the stones in the kidney, microbubbles could be injected percutaneously in a retrograde or anterograde way, depending on the location of the stone fragments. For stones in the ureter, the urologist can inject directly onto the stone with the help of a small catheter, or with the help of a flexible scope to inject the microbubbles into the ureteral orifice. After injection into the urinary system, the targeted bisphosphonate-laden microbubbles could affix to the surfaces/inner crevices of urinary stones. Cavitation of these microbubbles induced by a nearby source of ultrasound could fragment the targeted stones. The fragment dust or gravel can then pass through the ureter spontaneously. 109 Compared to conventional open surgery, this method enables urologists to treat patients with urinary stones in a less invasive way and with fewer morbidities, as well as to fragment the stones more thoroughly.
UTMD-mediated therapy in acute rejection
Acute rejection (AR) is a common complication after renal transplantation, and its mechanism is closely related to T cell–mediated production of inflammatory mediators and adhesion molecules. Studies have shown that NF-κB is involved in the regulation of inflammatory changes, including inflammatory factors (such as interleukin [IL]-1, IL-6, induced nitric oxide synthase, and TNF-α) and adhesion molecules such as ICAM-1 and vascular cell adhesion molecule-1. 110,111 However, silencing NF-κB expression by transfection of NF-κB decoy with UTMD preserved better graft function and histological structure. 112
Typically, patients with impaired renal allograft function need to undergo core-needle biopsy for the diagnosis of AR. However, this method is invasive, with risks such as the sample might miss AR and graft injury. 113 Ultrasound and microbubbles are accessible tools for the diagnosis of renal transplant through detection of specific biomarkers. 114 Grabner et al. conducted a new microbubble labeled with biotinylated anti-human CD-3 antibodies. They chose T cell–dependent diagnostics and evaluated CEUS targeted to T lymphocytes to assess AR. When injected with CD-3 antibodies, labeled microbubbles, and T lymphocytes, they calculated the ultrasound intensity and found that allografts undergoing AR exhibited markedly increased intensities of ultrasound signal with the administration of CD3-labeled microbubbles. This method provides a novel way to assess the early specific diagnosis of AR. 115
Conclusions and Future Perspectives
Compared to previous gene transfer methods, UTMD has evolved as a promising technology for renal disease treatment because of its low toxicity, non-immunogenicity, and simplicity. In combination with disease-suppressing genes or stem cells, UTMD may have great potential to treat different kidney diseases. It is a promising approach for the treatment of renal diseases when the detailed mechanisms are understood.
However, currently, the clinical application of UTMD is still limited, with certain questions remaining unresolved. First, ultrasound microbubbles cannot penetrate into small compartments of the kidney, including the urinary space containing podocytes, tubular lumen, and vascular endothelial space, due to their micro-sized dimensions. Second, researchers construct their own microbubbles for use in studies, and there remains a need to optimize the characteristics of microbubbles, ultrasound exposure parameters, frequency, and carrying DNAs or drugs for different renal diseases. Therefore, to develop a standardized construction method for microbubble will be very important for the application of this new technique.
Recently, the development of lipid NPs has emerged as a new field in microbubble research. Using a certain intensity of external ultrasonic irradiation, these NPs can elicit acoustic droplet vaporization, which could be changed into lipid microbubbles. As these NPs are much smaller than microbubbles, they are more promising vectors for targeting tissues and cells and may be more effective as deliverers of genes.
In conclusion, ultrasound-meditated gene delivery has great potential in treating various renal diseases. More effort is needed to overcome the unsolved obstacles detailed above. It is believed that UTMD will benefit from further development of precisely focusable ultrasound probes and improved molecular targeting strategies in renal disease treatments.
Footnotes
Acknowledgments
The authors would like to thank Ms. Linda Bowman for her assistance in the preparation of this article. This work was partly supported by the Nature Science Foundation of Ningbo (2016A610019), Ningbo Scientific Innovation Team for Environmental Hazardous Factor Control and Prevention (2016C51001), Zhejiang Key Laboratory of Pathophysiology (201703), and K.C. Wong Magna Fund in Ningbo University.
Author Disclosure
The authors indicate no potential conflicts of interest.