
Abstract
Seventy-five percent of patients with beta thalassemia (β-thalassemia) do not have human leukocyte antigen–matched siblings and until recently had no access to a curative treatment. Gene therapy is a promising treatment that can be proposed to these patients. This study estimates its cost and efficacy. In a monocentric retrospective study and cost-efficacy analysis, this study compared the two-year outcomes and costs of patients with β-thalassemia treated by gene therapy and hematopoietic stem-cell transplantation (HSCT). Grade III and grade IV complications, hospitalizations, and length of stay were extracted from the hospital discharge data. Costs were estimated from hospital accounting information and national cost studies. A total of seven patients with β-thalassemia treated between 2009 and 2016 were included, of whom four received gene therapy. Patients treated by gene therapy were older and had fewer complications and hospital admissions. Infectious complications were three times more frequent for patients treated with HSCT than for gene therapy. Average costs were €608,086 for patients treated by gene therapy and €215,571 for HSCT. The total cost of the vector was 48% of the total cost of gene therapy. Gene therapy as a curative alternative for patients lacking human leukocyte antigen–matched donors was costlier but resulted in fewer complications than HSCT.
Background
The management of beta thalassemia (β-thalassemia) requires lifelong red blood cell transfusion, iron chelation, splenectomy, or allogeneic hematopoietic stem-cell transplantation (HSCT), 1 all of which impose a significant patient burden and high costs to healthcare systems. 2,3 HSCT was until recently the only existing curative treatment and requires a human leukocyte antigen (HLA) identical donor. 4,5 The concept of gene therapy for β-thalassemia has moved from bench to bedside and is a promising treatment approach for patients with no matching donor available. 6 –9 While long-term studies are underway in multiple centers in Europe and the United States, proof-of-principle of efficacy and safety has already been obtained in patients with β-thalassemia. 10 –12 In addition to safety and effectiveness, the cost of gene therapy versus other options needs to be considered. 13,14 Both gene therapy and HSCT are curative options for β-thalassemia. From a health policy perspective, comparing gene therapy to another curative option such as HSCT makes sense, as HSCT is a benchmark for what the health-care system is willing to pay as a cure for β-thalassemia.
The objective of this study was to assess the cost, efficacy, and cost-efficacy of gene therapy compared to HSCT for patients with major β-thalassemia.
Methods
Study design
A retrospective comparative monocentric study was carried out using the diagnosis-related group (DRG) specific cost accounting database of the hospital, which includes data on treatments, medical procedures, and diagnosis using the International Classification of Diseases (ICD). *
Population
Patients were identified by their diagnosis related groups (27Z023 and 27Z03Z: allogenic and autologous hematopoietic stem cells), their ICD-10 code (D58.8, D56.0, D56.1, D56.9: hereditary hemolytic anemia/hemoglobinopathy and β-thalassemia), and procedural codes for treatments (Z948.00, Z94.801, FELF009, and FELF010). The ICD-10 code for the identification of treatment failure (T86.01) was also used. Patients with major β-thalassemia receiving curative treatment with HSCT or gene therapy at Necker Hospital, a French reference center for hematological diseases were compared for a 2-year period following treatment. All β-thalassemic patients treated between 2009 and 2016 were included if they received either treatment.
Outcomes
The primary efficacy endpoint was 2-year survival without major complications, defined for HSCT as grade III or grade IV graft-versus-host disease (GvHD), opportunistic infections, or death. Major complications post gene therapy were defined as treatment failure requiring transfusions 50% more frequently than before gene therapy. Complications were identified using ICD-10 codes in the hospital discharge database and graded according to the CTCAE v5.0. †
Resources used and costs
All admissions were identified using record linkage, and out-of-hospital resources were included based on current treatment protocols. Hospital resources consisted of consultations, laboratory tests, and, for HSCT patients, the antirejection medication cyclosporine/mycophénolate mofétil (Cellcept®). For the preparation phase, health-care resources common to gene therapy and HSCT consisted of: Pre-collection tests: HLA molecular typing, consultation pre-transplant (1 h). Specialist's consultations: medical (1 h), psychological (30 min), social (30 min), ophthalmology (30 min), stomatology (30 min), ear, nose, and throat (30 min), gynecology (30 min). Tests (in relation to the graft procedure): HLA control, thoracic scanner, brain nuclear magnetic resonance, heart ultrasound, pulmonary function technology, viral serology. Ovariectomy.
Specific resource use for HSCT also included donor costs (initial workup and bone-marrow collection). Resources were valued from the viewpoint of the health-care system with a 2-year time horizon. A secondary analysis was carried out from the societal perspective to take into account productivity losses.
All hospital admissions were valued by the production cost based upon the DRG adjusted for length of stay. Consultations and laboratory tests were valued by the national tariff, drugs by their list price, treatment duration, and patients' weight (see Table 1).
Index of resources and unit costs
Costs vary, depending on packaging used for each class of age. All costs are in 2017 euros.
HSCT, hematopoietic stem-cell transplantation; NA, not available.
Costs of gene therapy (excluding the cost of the vector) were obtained with a micro costing approach that identified all relevant cost components and valued each for all patients using duration of the procedure, staff, and supplies as variables. The corresponding unit costs were obtained from the finance department of the hospital (Table 1, Supplementary Table S1, and Supplementary File S1). The cost of the viral vector was estimated based on average cost of viral vector in studies sponsored by Assistance Publique Hôpitaux de Paris. The average cost per patient was €244,000/patient. The cost of the vector is based on its titer and on required specifications at the time of production which were ≥1 × 10–8 TU/mL. Manufacturing cost of the vector was estimated and included equipment, infrastructure costs, energy, security, consumables, qualification, and human resources.
Finally, indirect costs were included in a secondary analysis. Prior to allograft, the presence of both parents is mandatory for minor donors (aged <18 years) for a 1-day hospitalization and for a separate discussion at a district court. In addition, it was hypothesized that at least one parent would accompany the child at each consultation or hospitalization, preferably the mother, and miss a day of work. An average productivity loss per day was estimated based on French average monthly gross wages for men and women to which were added average employer social charges of 42% of gross wage. 15 An average daily gross wage of €186 for females and €226 for males was considered. The productivity loss was calculated based on the number of days of length of stay and considering that the mother would at least be present. In addition, for HSCT, the presence of the father prior to HSCT was added for a day of hospitalization and a day in the district court to address transplant-related legal issues.
Analyses
Descriptive analyses were carried out for age, hospital length of stay, cost of inpatient and outpatient admission, and amount and type of hospital use (intensive care, hematology ward, emergency room). Continuous variables are expressed as the mean, median, and minimum/maximum or standard deviation and categorical variables as percentages. Continuous variables were compared using the t-test for normally distributed variables and nonparametric tests (Kruskal–Wallis test) for non-normally distributed variables. Categorical variables were compared using Pearson's chi-square test. The threshold for significance was set at 5% (p-value of <0.05). No sample size calculation was performed a priori.
The uncertainty in deterministic sensitivity analyses was described. The following variables were included: patients' weight, increasing the number of patients treated by gene therapy in the coming years, and 5- or 10-year equipment amortization duration. The average weight in the gene therapy population was 61 kg. Assuming that treating younger patients will impact on average cost, this analysis was performed by decreasing the average weight by 20% and 30%.
An additional sensitivity analysis was performed on cost and efficacy using the bootstrap method. Bootstrap simulation methods were chosen, as they can be used to model small samples, complex data, and non-standard models and to assess uncertainty.
All analyses were performed using SAS v9.4 (SAS Corp., Cary, NC).
Results
Seven patients with β-thalassemia treated at Necker hospital between 2009 and 2016 were identified, four of whom were treated by gene therapy and three by HSCT. A comparison of the care pathways is shown in Fig. 1. Gene therapy patients were aged between 16 and 20 years, while two out of three patients treated by HSCT were younger than three years old and one was eight years old. No patient died during the follow-up period, but one patient treated by HSCT had a GvHD. Patient characteristics are presented in Table 2.
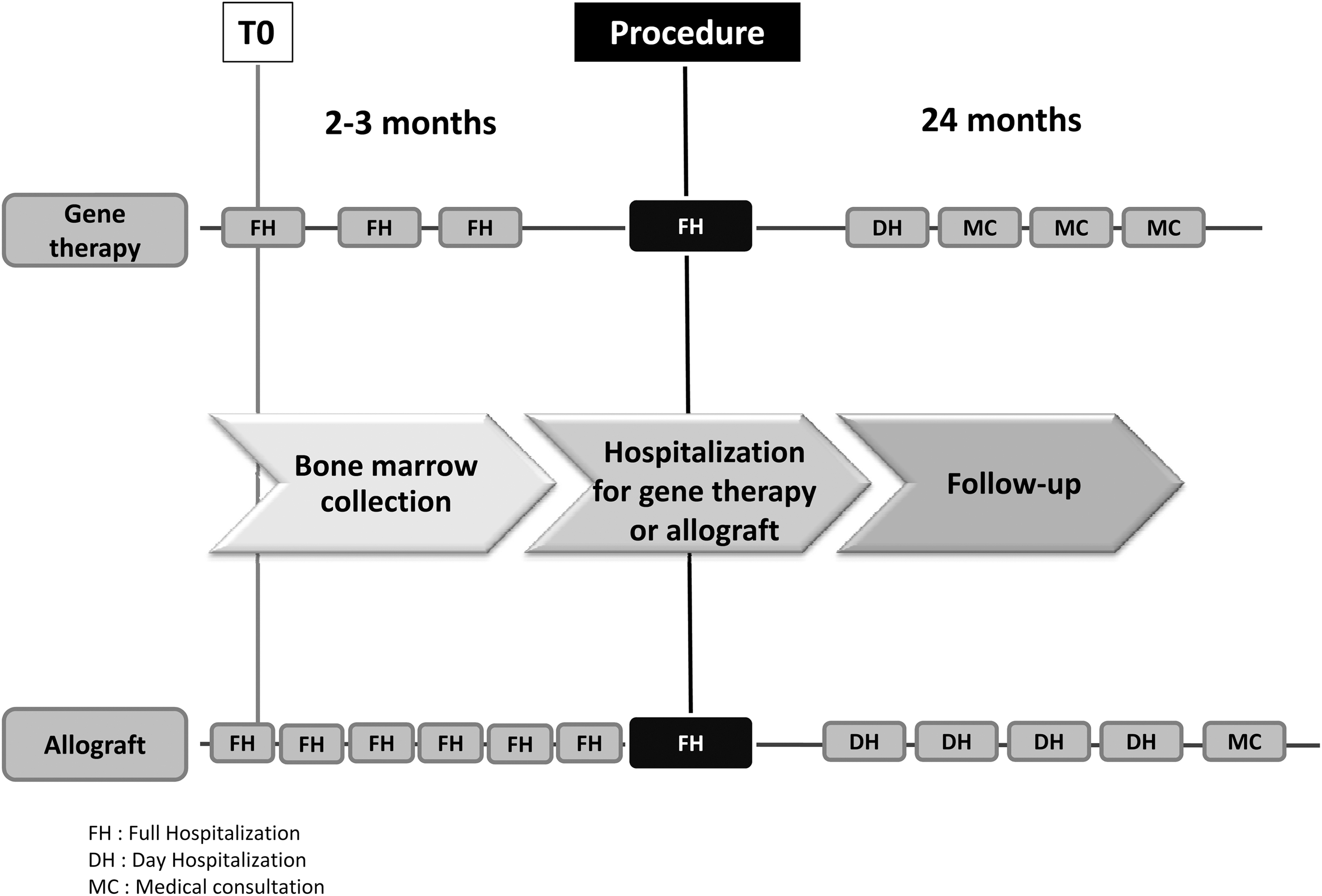
Gene therapy and hematopoietic stem-cell transplantation (HSCT) patient pathway. For each treatment, an overview of the patient pathway is summarized. The preparation phase lasts an average of 2–3 months before the procedure. Hospital admissions during the preparation phase include treatments, biological tests, imaging, and bone-marrow collection. Patients treated by gene therapy experience a reduced number of full hospitalization days during the preparation phase: 3 days versus 6 days on average for HSCT. The care pathway for donors (preparation phase) for HSCT patients is not considered in this figure.
Patient characteristics and resources
Values in square brackets are standard deviation; values in parentheses are min–max or median. Average number of hospitalizations includes complete and day hospitalization. For complications: average number of complications (N), average complication grading, and % of patients with complications (%). Complications due to conditioning regimen are induced by the use of myelo-ablative drugs.
Costs
Preparation phase
The preparation phase was more expensive for gene therapy than for HSCT (Table 3, Supplementary File S1, and Supplementary Table S1 for detailed fixed and variable costs). The difference was due to complex biology tests, which accounted for 97% of all laboratory costs during the preparation phase for gene therapy. Biology costs comprised the harvesting of stem cells, their analysis (such as hemoglobin chains detection by chromatography), and their preparation (immunoselection of CD34+, transduction of cells, quality, microbiological, and transduction efficiency controls). Costs of treatment, medical devices, and hospitalizations were also higher for gene therapy. The number of days in the intensive care unit was identical in both groups (4 days). However, hospitalizations in intensive care cost on average €929/day for gene therapy versus €686/day for HSCT.
Average 2-year cost per patient in euros of gene therapy and HSCT
Costs are presented in euros. Values in square brackets are standard deviations.
Based on four patients per year on a 10-year amortization basis.
The global purchasing amount of equipment used in the laboratory is €900,000. It is used 50% of the time by gene therapy, which gives an amount of €450,000 as the investment cost that is amortized over 10 years. For four patients treated annually, the average cost of equipment use of the laboratory is €11,250/patient.
Treatments include medication and medical devices (and hyper-transfusion for the preparation phase).
Procedural phase
During the procedural phase, total average medical costs (excluding vector costs) were relatively homogeneous between both treatments: €188,334 for gene therapy versus €173,497 for HSCT. Treatments costs were inferior for HSCT (€35,552/patient) than for gene therapy (€68,216/patient excluding viral vector costs or €362,656 including them).
Follow-up
During the follow-up phase, patients treated with gene therapy presented on average lower costs for biology, treatments, imaging, and inpatient and outpatient admissions.
In the gene therapy group, the vector represented 48% of the total average 2-year costs. In the HSCT group, inpatient and outpatient admissions represented 44% of total costs. For both treatments, the cost driver was the procedural phase.
In the secondary analysis, productivity loss was higher in the HSCT group compared to the gene therapy group (€13,971/patient vs. €7,545/patient).
Efficacy
No patient died during the follow-up period. Patients with gene therapy did not experience any major complications, whereas one grade IV GvHD occurred in the HSCT group (Table 1). Infectious complications were more frequent in HSCT patients (six episodes/patient) than for gene therapy (two episodes/patient). Other complications for gene therapy were drug-induced medullar aplasia (two episodes) and systemic inflammatory response syndrome without organ failure (two episodes), ICD-10 codes D61.1 and R65.0, respectively. For HSCT, most frequent complications were cystitis (two episodes), hematuria (two episodes), urinary retention (two episodes), and chronic pain (three episodes), ICD-10 codes R31, R33, N30.8, and R52.2, respectively. Both groups experienced complications induced by the use of myelo-ablative drugs of moderate protein-energy malnutrition (two episodes for gene therapy and for HSCT). Grade II and grade III complications were more frequent for HSCT than for gene therapy patients, with an average of one readmission post medical procedure in the gene therapy group compared to four for HSCT patients. Gene therapy patients had on average five complications compared to 11 for HSCT patients (from medical procedure to last follow-up).
Cost-efficacy analysis
Figure 2 shows a comparison of costs and outcomes for both treatments on a cost-effectiveness plane. Replications in the upper-right quadrant indicate that based on available data, gene therapy would always be more effective and more costly than HSCT.

Bootstrap of average cost and avoided complications. Bootstrap methods were used to examine the distribution of the incremental cost and incremental effectiveness across the cost-effectiveness plane for complications. A cost-effectiveness plane presents differences in costs and outcomes (here, a reduction of complications) between two treatments. To model the difference of cost and mean avoided complications, 1,000 iterations were performed. Comparing gene therapy and HSCT in a bootstrap simulation, the number of complications was lower but the cost was higher for gene therapy, confirming that gene therapy is more costly and more efficacious. Analyses were performed using Microsoft® Excel (2010; Microsoft Corporation, Redmond, WA) and SAS v9.3 (SAS Institute, Inc., Cary, NC).
Univariate measurement of uncertainty
The scenario of treating younger and lighter patients by reducing patient weight by 20% and 30% was explored, and this resulted in average 2-year gene therapy costs of €559,285 and €534,885, respectively, compared to the total current baseline of €608,086 (Fig. 3). Thus, treating younger patients could induce a decrease in the average 2-year costs for gene therapy by 8% for a 20% average weight reduction and 12% for a 30% average weight reduction.
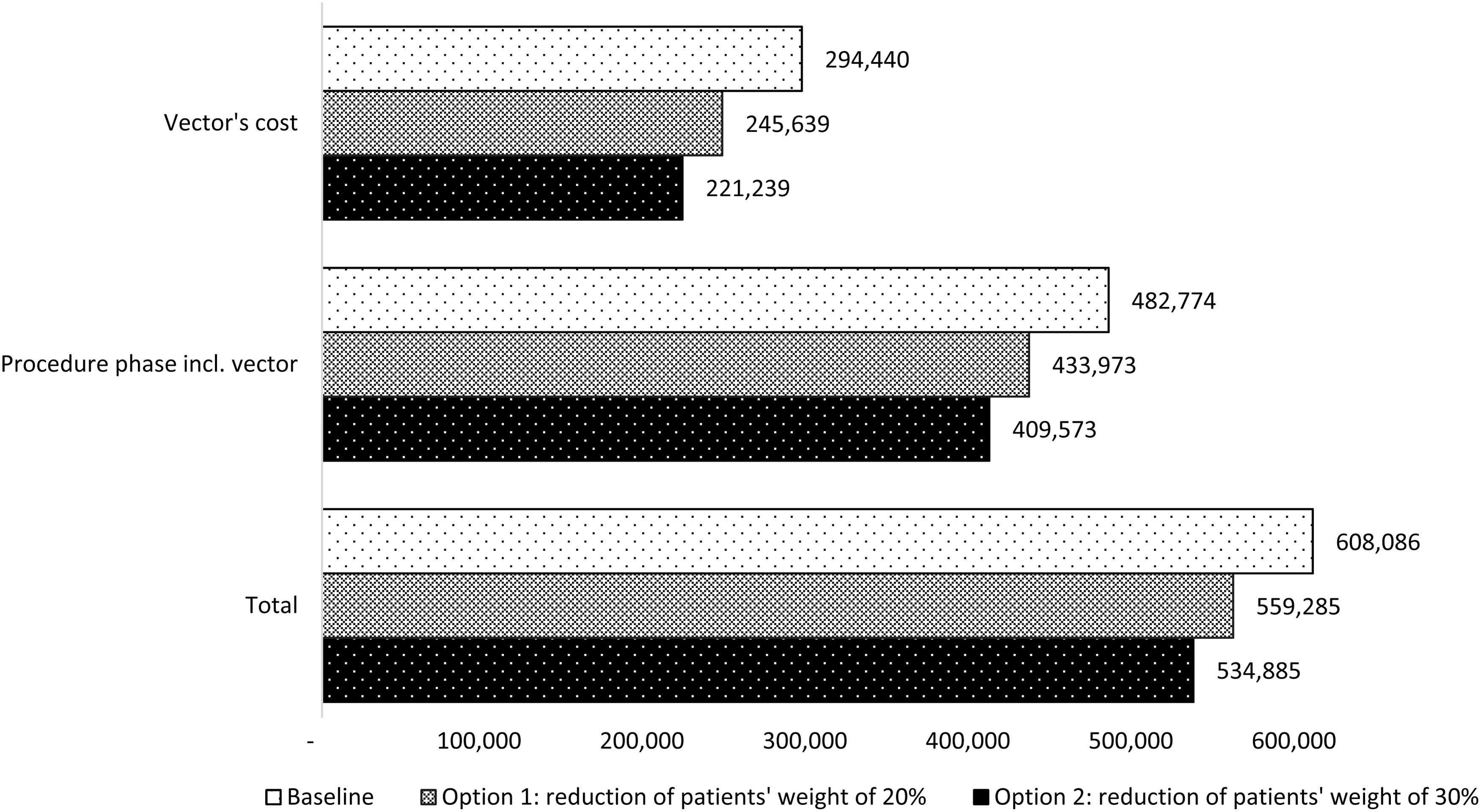
Measurement of uncertainty by univariate sensitivity analyses testing the reduction of patients' weight. The costs of gene therapy were varied, assuming first a reduction of 20% and second a reduction of 30% in patient weight (48 and 42 kg, respectively). The impact of such a reduction in weight on vectors, procedural phase (including vector cost), and total cost was compared. The average total decrease was 8%, from €608,086 to €559,285, for 48 kg average weight and of 12% for 42 kg average weight, with a total cost of €534,885.
Increasing the number of patients treated by gene therapy impacted manufacturing costs. Doubling the number of patients treated to eight per year decreased the average manufacturing cost to €42,415 compared to €50,440 (equipment amortization on 10 years) with a further decrease to €37,599 for 20 patients treated (Fig. 4).

Measurement of uncertainty. Evolution of manufacturing cost according to number of patients treated. The manufacturing cost decrease depending on the duration of equipment amortization was compared: 5 versus 10 years. This includes equipment, consumables, staff, fixed costs, and equipment annual maintenance (estimated as 9% of equipment cost), with a discount rate of 4%. On a 5-year amortization basis, the average cost of production is €61,690 per patient for four patients treated; on a 10-year basis, the cost is €50,440. Doubling the number of patients (eight patients treated) will decrease production costs to €48,040 on a 5-year amortization basis and to €42,415 on a 10-year basis. For 20 patients treated, production costs will be <€40,000, regardless of the amortization duration chosen.
Discussion
The medical outcomes and costs of four patients with major β-thalassemia who received gene therapy were compared to three patients treated with HSCT. Gene therapy patients experienced fewer complications and hospital admissions and shorter length of hospital stay but cost on average an additional €300,000–400,000 per patient. The difference in cost between treatments was explained by differences in procedural costs and the preparation phase required for gene therapy: immunoselection of CD34+, transduction of cells, quality, microbiological, and transduction efficiency controls. An important part of the total cost of gene therapy was the high cost of the viral vector. This high cost was driven by the quantity and type of vector. Necker Hospital purchased the lentiviral vector in quantities established a priori to ensure transfusion independence; the vector was re-engineered by the transplant team with highly skilled human resources, requirements in safety, quality efficacy, and regulatory compliance to advanced therapy medicinal products and Good Manufacturing Practice demands. 16 –18
Patients' genetic characteristics also had an impact: gene therapy patients were aged on average 18 years, and three of the four patients had βE/β0 genotypes, β0 mutations being more difficult to treat than β+. 10
At the moment, preparation and procedure costs are higher for gene therapy than for HSCT. But an increase in manufacturer competition and evolution of practices should decrease these costs. As an example, until 2015, donor follow-up was performed in day hospitalizations and, since January 2016, in outpatient departments. This led to an average decrease of €2,141 for the preparation phase for gene therapy.
As gene therapy is an innovative technique, patients benefited from a reinforced follow-up in the months following the procedure. However, in this study, follow-up costs were inferior to HSCT follow-up costs and should diminish in the coming years.
The major limit of this study is the small sample size due to the rare disease type, with an annual incidence of 1/10,000 in Europe, and the limited number of centers performing gene therapy. An advantage of this monocentric study is the completeness of the data collection and the consistency of the costing methodology. As gene therapy is a recent technique, a longer follow-up is necessary to quantify the long-term health benefits.
Information on donors and sociodemographic data of the patients' families was not available, and thus it was not possible to estimate transportation costs to the reference center, accommodation, or compensation for day work loss and other financial burdens in either treatment group. 19,20 These missing costs are positively correlated to the number of hospital days. Since the number of hospital days was higher for HSCT patients, the total cost difference may have been overestimated. The frequency and duration of stay in hospital may also have an impact on the quality of life of patients. 21 In the present sample, three out of seven patients were of school age, meaning that more frequent hospital stays would lead to more missed school days and more lost working days for the parents. Moreover, allografted children at Necker hospital had sibling donors who were thus geno-identical donors. For an unrelated donor, additional costs, time, and resources for research in donor registries would be necessary.
Comparing the costs in the present study to the literature, it was found that HSCT was estimated at €132,169 in Norway for adults, and that in the United States, median costs at 100 days after procedure were $289,283 (€255,225) for patients following the myelo-ablative regimen. 22,23 The same study found higher costs for pediatric patients ($585,300 or €516,400). The difference between the results could be due in part to the fact that HSCT costs are higher for patients with unrelated donors: 24 $317,994 (€280,544) in adults with nonmalignant diseases, while patients in the present study had sibling donors. To the best of the authors' knowledge, there has been no study on the cost of gene therapy in children with β-thalassemia. Even if it is presently more expensive than HSCT, gene therapy should become more affordable in the coming years, as increased competition between suppliers should favor a decrease in the vector's price and manufacturing costs. However, its long-term efficacy and costs still need to be assessed in order to have a more global view of the long-term effects on the health-care system. Weidlich estimated a total cost of £483,454 (€543,222) per pediatric patient without curative treatment for managing major β-thalassemia (routine tests and specialist consultations, blood transfusion, ICT, complications management) over 50 years. 25,26
As the cost of the vector is based on the titer of the vector, an increase of the titer or the use of better transduction processes, which require less vector, can dramatically reduce the cost per patient. While the cost of gene therapy may appear high at 2 years, considering a future decrease of manufacturing cost and if its curative effect is long-lasting, it could lead to long-term savings, which could facilitate the payer's approval.
Conclusion
Fewer complications of all grades were observed in the gene therapy group, which could be a curative option for β-thalassemic patients with no histocompatible donor. Results would have been even more favorable if pheno- or haplo-identical stem-cell transplantation had been retained as comparators. Only β-thalassemia was considered, but other pathologies can be treated by gene therapy such as sickle-cell disease, severe combined immunodeficiency, Wiskott–Aldrich syndrome, muscular dystrophy, or chronic granulomatous disease. 17 Treating more patients would lower the average cost per patient of gene therapy.
Footnotes
Acknowledgments
We would like to acknowledge Morgane Michel, a–c Meryl Darlington, a and Arnaud Nze Ossima, a,c for their support, and Alexandre Drezet, d Jeremy Magalon, d Laure Caccavelli, d Marine Lezoray, d and Isabelle Thuret for their support in collecting Hôpital Necker's manufacturing cost. The whole study (design of the study, data collection, analysis and interpretation, and writing of the article) was funded by Assistance Publique—Hôpitaux de Paris.
The Phase I/II study HGB205 “An Open Label Study Evaluating the Safety and Efficacy of Gene Therapy of the β-Hemoglobinopathies (Sickle Cell Anemia and β-thalassemia Major) by Transplantation of Autologous CD34+ Stem Cells Transduced Ex Vivo with a Lentiviral βA-T87Q-Globin (LentiGlobin® BB305) Vector” was registered with the Eudract number: 2012-000695-42. Authorization from French Agence Nationale de Sécurité du Médicament (ANSM) was obtained on December 21, 2012. The study was registered on
Author Disclosure
The authors declare that they have no competing interests.
Supplementary Material
Supplementary File S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.