
Abstract
In a previous limb-girdle muscular dystrophy type 2D (LGMD2D) clinical trial, robust alpha-sarcoglycan gene expression was confirmed following intramuscular gene (SGCA) transfer. This paved the way for first-in-human isolated limb infusion (ILI) gene transfer trial to the lower limbs. Delivery of
Introduction
In a proof-of-principle clinical trial, robust alpha-sarcoglycan (α-SG) gene expression was achieved in limb-girdle muscular dystrophy type 2D (LGMD2D), following intramuscular (i.m.) gene delivery mediated by adeno-associated virus (AAV) under control of a muscle-specific promoter (tMCK).
1,2
The
Following these initial i.m. studies, strategies to achieve clinically meaningful outcomes were considered. Prolonging ambulation was targeted as an efficacy outcome that could be potentially achieved by delivery of recombinant AAV (rAAV) carrying the SGCA gene via an intravascular route. A decision was made to deliver self-complementary
For clinical translation, preclinical proof-of-principle experiments were directed at demonstrating efficacy by increasing tetanic force and resistance to eccentric contraction accompanied by robust dystrophin and utrophin expression following gene delivery through the femoral artery without high volume or high pressure in the mdx mouse. 15,16 Advanced preclinical studies consisting of ILI gene transfer to the nonhuman primate (NHP) simulated a paradigm that could potentially be applied in a clinical setting for gene transfer. The vascular anatomy of the monkey provided the opportunity to explore ILI delivery of FLAG tagged transgenes to test the efficiency and safety of gene transfer to the quadriceps and gastrocnemius muscles of the NHP. 16 The favorable gene expression in the rhesus macaques paved the way for a clinical trial in LGMD2D subjects. This report describes the results of an open-label, single-site, Phase I/II, first-in-human gene transfer using ILI to test safety and efficacy in a form of muscular dystrophy with minimal cardiac requirements.
Methods
Study subjects
Six total LGMD2D patients were enrolled in an ILI gene-delivery trial. All subjects enrolled in this trial had documented biallelic SGCA mutations that predicted amino-acid substitutions known to be causative for LGMD2D. All patients were put on prednisone 1mg/kg/day for 1 month starting one day prior to gene transfer. Exclusion criteria were the same as previously published. 1,2 Informed consent was obtained by the Principal Investigator in compliance with 21CFR50 and the International Conference on Harmonisation guidelines before entering the trial and was signed by parents and subjects (for those aged 9–17 years). Pre–gene transfer immune studies included serum-neutralizing antibodies to AAVrh74 and interferon-gamma (IFN-γ) enzyme-linked immunospot (ELISpot) assay for both AAV capsid proteins and the α-SG protein. Criteria excluding participation were pregnancy; active viral infections, including human immunodeficiency virus, hepatitis A, B, or C, known autoimmune disease, and presence of cardiomyopathy; diabetes; or organ system abnormalities of the bone marrow, liver, or kidney.
This was a single-site, investigator-initiated, open-label, dose-ascending, ILI trial of
The FDA mandated that the first-in-human ILI gene therapy trial be done in a single limb of a non-ambulatory adult with LGMD2D (E-01) to establish safety. The first candidate, Cohort 1A, received 1 × 1012 vg/kg
Description of LGMD2D cohorts at baseline
LGMD2D, limb-girdle muscular dystrophy type 2D.
Outcome measures
The primary outcome for this clinical trial was safety and tolerability of gene transfer of SGCA under control of a muscle-specific promoter, tMCK using a scAAVrh74 vector, adapting a limb-saving cancer chemotherapy method to muscular dystrophy. This was a first-in-human gene-delivery trial using ILI as the method for safe, relatively easily performed gene replacement therapy. Functional outcomes included the North Star Ambulatory Assessment Scale (NSAA), stair climbing, and the distance walked using the six-minute walk test (6MWT). Confirmatory strength testing employed force generation quantified by maximum voluntary isometric contraction testing (MVICT) 17 –20 of knee extensors (quadriceps muscle), a direct target of ILI through the femoral artery. Force generation required sustained contraction for 5 s. Final data were based on two trials with ≤10% error between efforts and 20 s of rest between trials.
Muscle biopsies provided the source for confirming vector delivery and SGCA protein expression as judged by immunofluorescence, quantified immunoblot analysis, and vector copy number based on previously published methods. 1,2,18,19 Pre- and post-gene delivery to quadricep-muscle biopsies on day 180 were performed on four subjects (E-03, E04, E-05, and E-06). Opposite extremity biopsies were done to avoid scar tissue from the first biopsy that could impede interpretation. Subject E-01, an adult with LGMD2D, volunteered for a single-limb infusion safety study and had only a post gene-delivery muscle biopsy. Pre- and post-treatment muscle biopsies were scheduled for E-02. However, a post-treatment biopsy was deferred at parental request, given that progressive muscle weakness during follow-up resulting in loss of ambulation.
Immune studies
All subjects met the criteria for serum-binding antibody level against AAVrh74 and AAV8 no greater than 1:50 before gene transfer. 6 This was determined by enzyme-linked immunosorbent assay to the viral capsid, as previously described. 21 Follow-up titers post gene transfer included days 7, 14, 28, 42, 60, and 90 and every 3 months for the remainder of the trial. Pre-screening and follow-up studies to identify potential T-cell immunity were done on these same days using IFN-γ ELISpot according to previously described methods. 6,21 Antigens for the ELISpot assay included three AAV capsid peptide pools and the full α-SG protein. 1,2
Vector production
The rAAV,
ILI procedure
The proposed clinical trial is a dose-escalation study of
For each cohort, vector was prepared by the research investigational pharmacy service, brought to the catheterization suite on ice, and allowed to warm to room temperature. With the balloons inflated, a pre-flush 2 mL/kg of lactated Ringer's solution (LRs) was infused over approximately 1 min, and then the prescribed vector-dosing regimen was infused through the femoral artery with a total of 8 mL/kg LRs over approximately 2 min. After the infusion was complete, a 10 min dwell time permitted maximum skeletal muscle transduction. Skin mottling was observed, starting at the upper thigh and progressing distally as the infusion progressed. After 10 min of isolation, the extremity was flushed using the arterial catheter with 2 mL/kg of LRs for 1 min. The arterial balloon was deflated and removed, followed by deflation and removal of the venous balloon. Direct pressure was applied to control bleeding at the site of catheter insertion. Normal color was restored to the extremity, as were pulses over the femoral artery and in the distal extremity circulation. The opposite extremity then underwent the same procedure. After both legs were infused, all equipment and syringes were properly discarded, and the patient was returned to the recovery suite where full consciousness and vital signs returned to normal before they were taken back to their hospital room.
Results
Adult non-ambulatory LGMD subject (cohort 1A)
This was a pilot clinical trial that included six subjects (four males), as shown in Table 1. Safety was initially established in an adult non-ambulatory LGMD2D subject (E-01) dosed in a single limb. MVICT of knee extensors showed an increase in muscle force generation (47%) on the side of gene delivery (Table 2). Post gene transfer gene expression and vector genome copy numbers were assessed in the tibialis anterior muscle, validating increases at day 180 (Figs. 1 and 2). IF showed α-SG expression in the sarcolemma that was quantified by Western blot, revealing 35% of normal control.
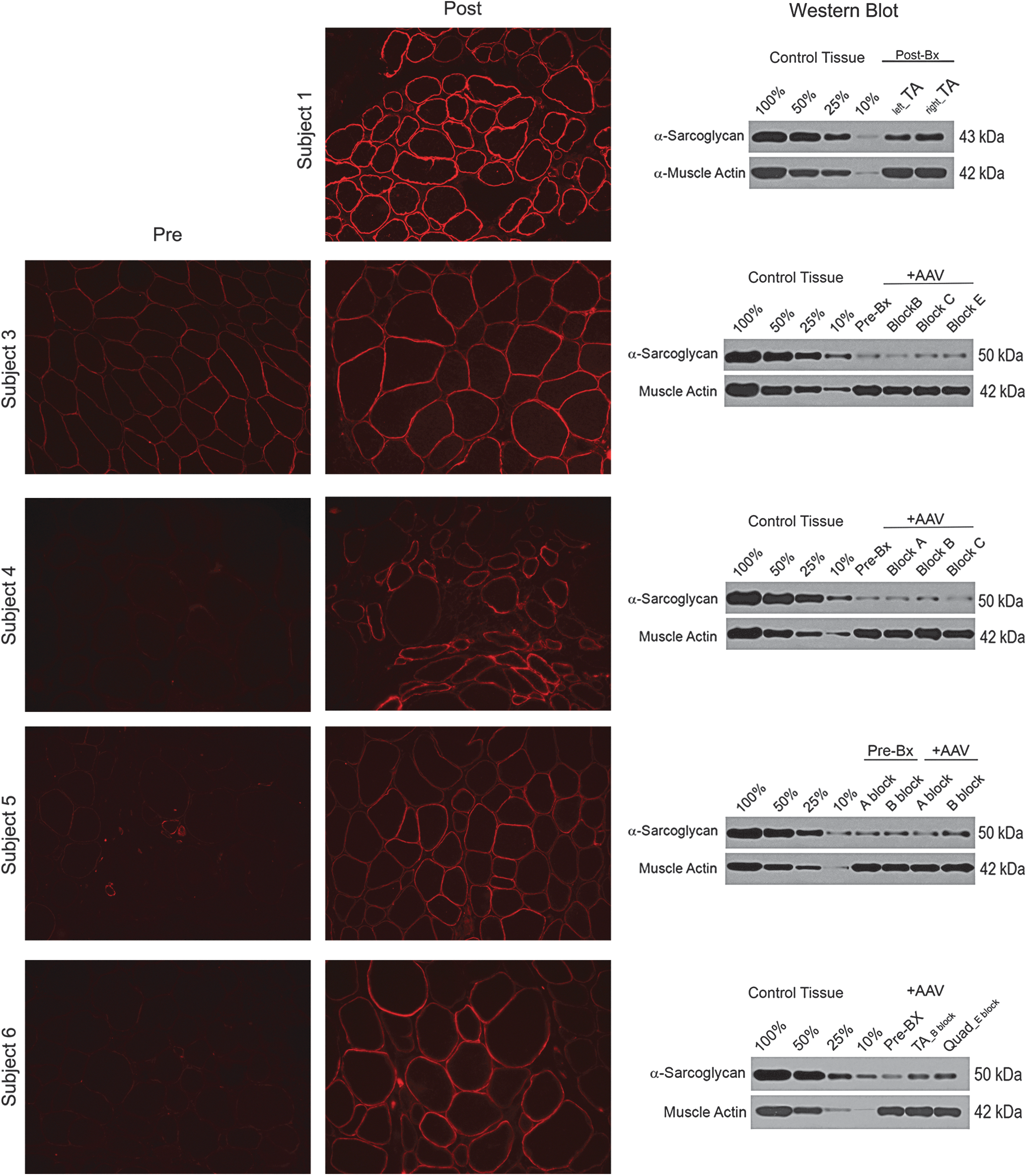
SGCA expression following isolated limb infusion (ILI). SGCA gene expression demonstrated by immunofluorescence following alpha-sarcoglycan (α-SG) antibody staining of muscle biopsies taken post gene transfer for subject 1 (tibialis anterior) and pre and post gene transfer for subjects 3–6 (quadriceps). Except for subject 1 where it could not be compared, membrane staining intensity post gene transfer showed increased intensity. Confirmation of gene expression by quantitative Western blots revealed an increase in α-SG protein compared to baseline as follows: subject 3: 38%; subject 4: 12.5%; subject 5: 22%; and subject 6: 172%. Comparisons as a percent of normal for each subject were as follows: subject 1: 35%; subject 3: 14%; subject 4: 16%; subject 5: 15%; and subject 6: 25%. Western blots were quantified using a four-point standard curve (10%, 25%, 50%, and 100%) generated from non-dystrophic normal control muscle samples and normalized for muscle content using muscle actin as a loading control (lower band).

Vector genome copy number following ILI. Delivery of
Functional outcomes of ILI gene transfer
Post gene-transfer muscle biopsy done on TA.
No ambulatory change pre and post gene therapy.
Lost ambulation post gene therapy.
ILI, isolated limb infusion; MVICT, maximum voluntary isometric contraction testing (reported in kilograms); 6MWT, six-minute walk test (reported as distance walked in meters); BL, baseline; AMB, ambulation; TA, tibialis anterior; Δ, percent change in 6MWT meters from baseline to end of study (all patients completed 2 years).
Ambulatory LGMD2D cohort 1B (low dose) and cohort 2 (high dose)
Five LGMD2D patients (cohort 1B: subjects E-02, E-03, and E-04; cohort 2: subjects E-05 and E-06) were ambulatory at the time of screening and initiation of gene transfer (Tables 1 and 2). Muscle biopsies were performed on all subjects at day 180. Two ambulatory subjects, one in each dosing cohort (E-02, age 9 years; E-05, age 12 years) were unable to maintain independent ambulation during this 2-year clinical trial. MVICT decreased in E-02 (22% right; 28% left). E-05 had minimal change in MVICT (reduced by 1% right and 4% left) and no significant change in muscle-fiber size (pre 62.13 ± 24.97 and post 67.38 ± 22.84).
Subjects E-04 and E-06 maintained ambulation with reduced MVICT. E-04 modestly declined on 6MWT (24%), and E-06 minimally increased (5%). Subject E-03 stood out because MVICT increased in both limbs (increased 59% right and 68% left), as did his increase in quadriceps muscle-fiber size (28%). However, distance walked on the 6MWT remain unchanged (declined 2%).
For cohorts 1B and 2, muscle-biopsy results provide clear evidence that transgene was delivered to the muscles of the lower limbs through this ILI approach. SGCA gene expression pre and post treatment shows increased staining intensity by immunofluorescence confirmed by Western blot (Fig. 1). The percent α-SG increased in subjects 3–6 (14–25% of normal). The increase in vector genome copy numbers for each patient post gene transfer is shown in Fig. 2 (subject 3: 5.4e3 vg/μg; subject 4: 5.02e3 vg/μg; subject 5: 6.48e3 vg/μg; and subject 6: 7.76e4 vg/μg; 0.03–0.54 copies/nuclei).
Adverse events
Overall, for the six subjects treated, ILI-AAV gene delivery was well tolerated. Catheter placement and positioning the balloons to isolate the limbs took between 1 and 1.5 h. The procedure, done under conscious sedation, was well tolerated. There was skin mottling and dusky discoloration of the leg during gene infusion that persisted during dwell time, with rapid clearing as the limb was re-perfused. Mild soreness with applied pressure or while walking was experienced at the site of entry in the groin, reaching a peak by day 3, with bluish discoloration that persisted for several days. No hemorrhages were encountered, and no patients had deep-vein thrombosis/thrombophlebitis. Viral delivery caused no side effects, and there were no adverse events/serious adverse events (SAEs) directly related to transgene or AAV. Anti-AAVRh74 IgG antibody titers were monitored throughout the trial and peaked between 3 and 6 months before they declined slightly and maintained a plateau (Supplementary Fig. S1). An elevation of T-cell responses as measured by ELISpot assays to AAVrh74 was observed during the trial (Supplementary Fig. S2), similar to other Phase I clinical trial gene-delivery studies. 6,22 T-cell response to AAVrh74 usually peaked at 1–4 weeks following gene delivery, never reaching SAE level, and there were no corresponding elevations of liver enzymes and no clinical manifestations. An ILI study may be expected to protect hepatocytes from excess exposure to viral delivery by isolation of the extremity during infusion of vector. Clinical chemistries throughout the trial remained normal.
Two of the participants in the trial, E-03 and E-06, had episodes of rhabdomyolysis/myoglobinuria reported before (by history) and during the trial (each had two occurrences). The episodes during the trial were documented by peak elevated creatine kinase levels between 59,171 IU/L (E-03) and 68,500 IU/L (E-06). Rhabdomyolysis was precipitated by excessive activity events, despite advice to the contrary (E-03 fencing competitions; E-06 participation as cheerleader). No long-term consequences were seen; patients were kept well hydrated and rested during brief hospitalizations with treatment by intravenous hydration. Sarcoglycanopathies have an increased predisposition to episodes of myoglobinuria and hyperCKemia, including LGMD2C, 24 2E, 25 and 2D. 26 –29 Subject E-02 suffered multiple limb fractures related to falls that had no relationship to transgene or AAV.
Discussion
The objective of this translational gene therapy trial was to establish if ILI would provide significant clinical improvement in LGMD2D with α-SG deficiency with potential application to other forms of muscular dystrophy. The rational for ILI gene delivery is based on targeting gene delivery to the predominant area of need; α-SG deficiency spares the heart in most cases. The disability is caused by lower-limb muscle weakness until late in the course of the disease. ILI, if effective, provides a means of gene replacement using a reduced viral load to correct the defect in the targeted extremity. Achieving clinical efficacy with ILI diminishes the cost for viral production compared to the demands for high viral load needed for systemic gene delivery. 6 According to some investigators, concerns remain regarding the safety of high-dose AAV gene delivery. 30 ILI offers an alternative route of gene transfer using less viral load compared to systemic delivery, especially for neuromuscular diseases starting later in childhood or early adult life where patient size increases the dosing requirements and cost.
In developing strategies for gene delivery through isolated limbs, both ILP and ILI were considered. The differences were important, considering that ILP is far more invasive as a surgical procedure compared to ILI, requiring only radiologically guided percutaneous insertion of catheters to the femoral artery and vein. 7,11,12 Cardiopulmonary bypass is not necessary for ILI, and gene transfer requires only delivery of vector by manual push with a syringe, in contrast to a high-flow pump with limb recirculation when targeting neoplasia. 9,31 Efficacy is somewhat less for ILI compared to ILP treatment of limb sarcoma and melanoma, but both have the potential to be effective. 11,13 Considering the risk–benefit ratio for a disease with far fewer life-threatening consequences like LGMD, the choice favoring ILI was justified.
The functional outcomes for the ILI LGMD2D study were partially improved in a subset of subjects. Based on the 6MWT for five ambulatory LGMD2D subjects aged 8–13 years, two lost ambulation, one declined in distance walked (24%), and two others showed no change (decreased 2%, increased 5%). The gene-expression data for SGCA on muscle biopsy was visualized by immunofluorescence 32 and confirmed by Western blot quantification and vector genome counts, providing unequivocal evidence of gene delivery through the femoral artery. The limited functional outcome improvement was likely contributed to by poor delivery to proximal muscles (hip flexors, hip abductors, and hip extensors), limiting the distance walked on the 6MWT and the ability to maintain ambulation. Importantly, subjects who improved on MVICT correlated with SGCA expression and increased fiber size. Improvement in outcomes might require higher viral doses and different catheter placement to infuse the replacement gene to more proximal muscle targets.
The current study demonstrates the challenge of transducing major muscle groups in the extremities that contribute to gait and 6MWTs. The methods used in this trial were not adequate to improve major motor functions. Apart from systemic delivery to target all muscles, options for ILI studies in the future will be to increase the dose of virus or catheterize vessels that feed more proximal muscles. The iliac artery could be a choice but presents more challenges for extremity isolation, the objective of ILI. In this study, limb delivery of
Footnotes
Acknowledgments
The support of our Regulatory Operations and Drug Development Core at Nationwide Children's Hospital, including Chris Shilling, MS, and Patricia C. Sondergaard, PhD, was helpful and appreciated. Our GMP vector Manufacturing Core at Nationwide Children's Hospital provided
Author Disclosure
J.R.M. is a Principal Investigator in the Center for Gene Therapy at Nationwide Children's Hospital. L.R.R.-K. is Vice-President for Gene Therapy, Sarepta Therapeutics. No competing financial interests exist for these contributors or for the remaining authors.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.