
Abstract
Netherton syndrome (NS) is a rare autosomal recessive skin disorder caused by mutations in SPINK5. It is a debilitating condition with notable mortality in the early years of life. There is no curative treatment. We undertook a nonrandomized, open-label, feasibility, and safety study using autologous keratinocytes transduced with a lentiviral vector encoding SPINK5 under the control of the human involucrin promoter. Six NS subjects were recruited, and gene-modified epithelial sheets were successfully generated in three of five subjects. The sheets exhibited expression of correctly sized lympho-epithelial Kazal-type-related inhibitor (LEKTI) protein after modification. One subject was grafted with a 20 cm2 gene-modified graft on the left anterior thigh without any adverse complications and was monitored by serial sampling for 12 months. Recovery within the graft area was compared against an area outside by morphology, proviral copy number and expression of the SPINK5 encoded protein, LEKTI, and its downstream target kallikrein 5, which exhibited transient functional correction. The study confirmed the feasibility of generating lentiviral gene-modified epidermal sheets for inherited skin diseases such as NS, but sustained LEKTI expression is likely to require the identification, targeting, and engraftment of long-lived keratinocyte stem cell populations for durable therapeutic effects. Important learning points for the application of gene-modified epidermal sheets are discussed.
Introduction
Netherton syndrome (NS) is a rare autosomal recessive skin disorder caused by mutations in the gene SPINK5. 1 It is a debilitating condition characterized by ichthyosiform erythroderma, atopic diathesis, and defective skin barrier at or soon after birth. 2 The prognosis of NS is poor with notable mortality in the early years of life due to life-threatening complications, such as bronchopneumonia, sepsis, and hypernatremic dehydration secondary to severe water loss through the defective skin barrier. The causative gene SPINK5 encodes the protein lympho-epithelial Kazal-type-related inhibitor (LEKTI). 3 It is a serine protease inhibitor expressed in the uppermost compartments of the epidermis and plays a critical role in the regulation of two serine proteases kallikrein (KLK) 5 and KLK7, which hydrolyze the extracellular corneodesmosomes in the skin. 4,5 In NS patients, mutations in SPINK5 cause truncated protein expression, resulting in loss of activity of LEKTI. 6,7 As a consequence, hyperactivated KLKs excessively degrade corneodesmosomes and cleave proelastase 2, leading to a defective skin barrier. 5,8 –11
Current treatments for NS are largely symptom based, relying on the use of emollients, corticosteroids, and antibacterials, but these treatments have limited benefit. Gene therapy offers the prospect of disease amelioration of genetic skin disorders.
Gene-based correction of junctional epidermolysis bullosa (JEB) was first reported over a decade ago following ex vivo gamma-retroviral transduction of epidermal stem cells and grafting of corrected epidermal sheets.
12
That study provided important proof-of-principle evidence that correction of skin stem cells can afford effective therapy of genetic skin conditions. A similar approach was recently reported for treatment of a subject with JEB with complete epidermal loss across 80% of body surface area,
13
and there are ongoing skin sheet gene therapy trials for recessive dystrophic epidermolysis bullosa in the United States
14
and Austria (
We previously modeled gene therapy for the correction of NS using ex vivo lentiviral-modified epidermal sheets in human:murine chimeras. 15 We developed a third-generation self-inactivating lentiviral vector encoding a codon optimized cDNA for SPINK5 under the control of a 572-bp enhancer derived from human involucrin promoter. 16 Reversal of abnormal NS features and restoration of normal human skin architecture in gene-corrected grafts with compartment-specific reconstitution of LEKTI expression were confirmed in humanized chimeras. 15,16 We now report the application of a Good Manufacturing Practice (GMP)-compliant process for generating gene-modified epithelial sheets 17 in a feasibility and safety study for patients with NS and report 12-month follow-up results from the first grafted patient.
Materials and Methods
Study approval
The trial was approved by the Gene Therapy Advisory Committee (GTAC; Ref No. GTAC188) and the Medicines and Healthcare Products Regulatory Agency (MHRA; Ref No. EUDRACT 2011-003212-22). It was registered with
Clinical trial protocol
Detailed information about the recruitment criteria of subjects, consent forms, the preparation of GMP-compliant lentiviral vector stocks, the production and release of investigational medicinal products (IMPs), grafting of gene-modified epithelial sheets, and schedule of clinical monitoring was published previously. 17
Patient recruitment, consent, and skin procurement
Patients aged 16 years or older with a clinical diagnosis of NS were identified from Guy's and St. Thomas' Hospitals and referrals from NHS Ayrshire and Arran University Hospital Crosshouse, Scotland. After confirmation of biallelic SPINK5 mutations, patients were invited to participate in the clinical trial. Following informed consent, patients with NS were screened against the eligibility criteria as previously published. 17 Those eligible were recruited for the study and a 6-mm punch biopsy was obtained from an area of intact uninflamed skin under local anesthesia (1% xylocaine). The skin procurement was then sent to the Gene Therapy Laboratory for manufacture of gene-modified epithelial sheet. Grafting took place in the outpatient theaters at St. Thomas' Hospital and follow-up visits took place in the dermatology clinics at Guy's Hospital.
Mutation detections in SPINK5
Mutations in SPINK5 were confirmed by direct Sanger sequence analysis by the North East Thames Regional Genetics Laboratory, Great Ormond Street Hospital (GOSH) NHS Foundation Trust.
Keratinocyte culture, transduction, and epithelial sheet culture for the generation of IMP
The production of GMP-compliant IMP was carried out at the Gene Therapy Laboratory, GOSH NHS Foundation Trust, a GMP-compliant facility approved by the MHRA in the United Kingdom (MIA(IMP) 17328).
Primary keratinocytes were isolated from a 6-mm skin biopsy by incubation with 0.25% trypsin-EDTA for 3 h. Dissociated keratinocytes from the skin were seeded in a T25 flask with i3T3 cells and grown in Green's medium 17 supplemented with penicillin and streptomycin (100 units/100 μg/mL; Pharmacy in GOSH, London, United Kingdom). After reaching confluence, cells were passaged and seeded in fresh flasks and transduced with lentiviral vector LV-INVO-SP. No antibiotics were added to Green's medium after this point. 17 Transduced cells were further cultured in 100-mm dishes to form epithelial sheets. Frozen irradiated murine fibroblasts 3T3 cells (i3T3) were freshly thawed and added to keratinocyte cultures with a density of 0.6–1.6 × 106 cells per T25 flask. Epithelial sheets were harvested by 2 mg/mL dispase in phosphate-buffered saline solution, then attached to Tricotex (Smith & Nephew, Hull, United Kingdom), and packed in a sterile container for grafting. Frozen i3T3 cells and all media, reagents, and chemistry for keratinocytes and sheet cultures were supplied by Regenerys (Sheffield, United Kingdom).
Hematoxylin and eosin staining, immunofluorescence staining, and immunoblotting
Punch skin biopsies taken from NS patients were formalin fixed and paraffin wax embedded, sectioned, and stained with hematoxylin and eosin (H&E) at the Histopathology Department, GOSH NHS Foundation Trust. Immunofluorescence staining for LEKTI was performed on the paraffin sections (6 μm thickness) using methods previously described. 15 A custom-made affinity-purified rabbit polyclonal antibody directed against the C-terminus of LEKTI 15 was used (Eurogentec, Southampton, United Kingdom). A polyclonal anti-human KLK5 antibody (H-55; Santa Cruz, Heidelberg, Germany) was used at the dilution of 1:250 for the immunostaining of KLK5. Stained tissues were imaged using an upright light microscope (Zeiss Axiovert) or Zeiss confocal microscope LSM 710 (Zeiss, Cambridge, United Kingdom) and images were processed using Adobe Photoshop CS (Adobe Systems, Inc., San Jose, CA).
Immunoblotting for LEKTI expression was carried out in cells or sheet lysates using a monoclonal anti-LEKTI antibody (1C11G6; Invitrogen, Paisley, United Kingdom) as detailed previously. 15
Quantitative PCR
Integrated vector copy number (VCN) was assessed in transduced cells by quantitative PCR (qPCR) using primers (F-CAGGACTCGGCTTGCTGAAG and R-TCCCCCGCTTAATACTGACG) and probe (FAM-CGCACGGCAAGAGGCGAGG-TAMRA) designed to target the HIV Psi packaging element of the lentiviral vector LV-INVO-SP, and in comparison to signal generated for the housekeeping gene human albumin (F-GCTGCTATCTCTTGTGGGCTGT, R-ACTCATGGGAGCTGCTGGTTC, probe: VIC-CCTGTCATGCCCACACAAATCTCTCC-TAMRA). Integrated copy number was calculated with the aid of standard curves generated using plasmids encoding the vector and cDNA for human albumin.
Linear amplification–mediated PCR and integration site mapping
DNA from P003 was extracted from transduced and nontransduced epithelial sheets before grafting and a skin biopsy taken from the area of grafting at 3 months after grafting were used for lentiviral vector integration site (IS) analysis. Linear amplification–mediated (LAM) PCR was used to identify lentiviral vector flanking genomic sequences in these samples, as described previously. 18 Triplicates for each sample were amplified, and subsequent library preparation 19,20 was carried out for deep sequencing by MiSeq (Illumina) to determine lentiviral integration profiles and potential clonal dominance. Raw sequence data were trimmed according to sequence quality (Phred 30). Only sequences with 100% sequence identity barcodes were further analyzed. Primary IS annotation was conducted by using GENE-IS (version 1.2). 21
Image analysis
Immunofluorescence images were taken using a Zeiss confocal microscopy LSM710, and the intensities of optical sections were quantified using the ImageJ. Briefly, three nonoverlapping but adjacent optical sections were recorded and saved digitally from each slide using a 40 × NA1.2W objective. Acquisition settings were identical for all samples. Images were straightened by tracing a line along the cornified layer using the ImageJ straighten function, and then, the fluorescence intensity was measured across a 150 μm section to a depth of 250 μm. Three images per sample were analyzed, and the mean intensity was plotted. Data were corrected for nonspecific background staining from secondary antibody-stained controls.
Transepidermal water loss
Transepidermal water loss (TEWL) was measured to assess skin barrier function before and after grafting used a VapoMeter (Delfin Technologies, Surrey, United Kingdom). Three measurements were taken at each time point to obtain an average value.
ELISPOT assay
Peripheral blood mononuclear cells (PBMCs) were isolated from ethylenediaminetetraacetic acid-treated peripheral blood samples by density gradient centrifugation using Lymphoprep (Axis Shield, Oslo, Norway) and stored in liquid nitrogen. Immediately before ELISPOT assay, the cells were thawed and the number of viable cells was established using trypan blue staining. The human IFN-γ ELISPOT Kit (BD Biosciences, Berkshire, United Kingdom) was used according to the manufacturer's instructions. Briefly, 1 × 105 of viable cells were seeded per well in a plate precoated with interferon (IFN)-γ antibody and incubated with 1.2 μg/mL full-length rLEKTI (Oxford Expression Technologies, Oxford, United Kingdom) for 16 h at 37°C. Staphylococcal Enterotoxin B Fragment (1 μg/mL) (Sigma, Dorset, United Kingdom) or 10% fetal bovine serum (Labtech International, Heathfield, United Kingdom) in RPMI medium (Life Technologies, Paisley, United Kingdom) was used as controls. Reaction plates were read using AID ELISPOT reader (AID GmbH, Strassberg, Germany), and positive spots were quantified.
Statistics
Statistical analysis of single-factor analysis of variance (ANOVA) and post hoc t-test between two groups were performed where applicable in the study data, and a p-value of ≤0.05 was used to determine statistical significance.
Results
Subjects with NS
Six patients (P001–P006), two females and four males, aged 16–39 years, with NS were recruited for the study. Mutations in SPINK5 and baseline reduction of LEKTI expression were confirmed by Sanger sequencing in DNAs and immunostaining in skin biopsies (Supplementary Table S1 and Supplementary Fig. S1). All patients were found to harbor compound heterozygous mutations in SPINK5, which caused frameshifts, premature termination of codons, or intron retention, resulting in truncated or abnormal LEKTI protein expression. In all cases, skin swabs were taken before skin procurement for microbiological screening. Subjects with bacterial growth were treated with appropriate antibiotics for 10 days. TEWL measurements, blood samples, and photographs of the skin were collected for baseline recording.
Generation of GMP-compliant lentiviral gene-modified epithelial sheets
In compliance with regulatory and ethics approvals and with informed consent, a skin biopsy (6 mm) from the anterolateral aspect of the thigh was taken from each patient and primary keratinocytes, including keratinocyte stem cells, were isolated and cocultured with irradiated 3T3 (i3T3) feeder cells in a T25 flask. Where skin-resistant bacteria were detected on previous skin swabs, or if there was known hypersensitivity to penicillin, vancomycin, and streptomycin (50 or 100 μg/mL) were substituted in the culture. Keratinocytes were passaged when counts reached ∼3 × 106 and subcultured in three fresh T25 flasks at ∼1 × 106 cells per flask (P1), against with i3T3 cells. After 24–48 h, P1 keratinocytes were exposed to a single round of lentiviral vector LV-INVO-SP (2 × 108 IU/mL) transduction for 6 h at a multiplicity of infection of 20. One control flask was retained without transduction. P1 keratinocytes were then cultured and expanded to ∼2 to 3 × 106 cells per flask and passaged and reseeded in a 100-mm culture dish for sheet culture (P2).
Mature epithelial sheets in which cultured keratinocytes reached stable confluence formed in 2–3 weeks. One week before harvesting the sheet for grafting, one of two transduced sheets, and the nontransduced sheet, were harvested for assessments of transduction efficiency, including proviral copy number by qPCR, and LEKTI expression by in situ immunostaining and immunoblotting. Where release criteria were met, 17 the other transduced sheet (the IMP) was harvested following brief trypsinization of any residual i3T3 cells and was then cultured in Green's medium (free of cholera-toxin) for 3 days. The cultured sheet was finally detached by Dispase treatment and subjected to final release checks, before delivery to the theater for grafting (Supplementary Fig. S2).
Five sheet cultures were generated from five individual skin biopsies from P002 to P006. All cultured sheets were successfully transduced with LV-INVO-SP lentiviral vector with an average proviral copy number ranging from 1.8 to 11.6 per cell (Supplementary Table S2).
Successful transduction was further confirmed by detection of LEKTI expression using immunoblotting (Fig. 1). An ∼148 kDa full-length LEKTI band was observed in samples from sheets generated using normal keratinocytes or transduced NS keratinocytes. There was an additional smaller band (∼120 kDa) in samples from normal keratinocytes/sheet but not in samples from transduced NS keratinocytes/sheets because the vectorized codon optimized SPINK5 cDNA encoded a longer 15 domain LEKTI isoform and not the alternatively spliced 13 domain LEKTI isoform. 22 Additional smaller bands were also detected in normal keratinocyte-derived sheets and transduced NS sheets. 23 Neither full-length nor cleaved LEKTI was detected in nontransduced NS samples.

The expression of LEKTI in cultured keratinocytes and sheet transduced with the LV-INVO-SP virus. An overexpressed 15-domain LEKTI isoform band (∼148 kDa) and several cleaved LEKTI with small sizes were detected in the transduced NS keratinocytes or sheets (trans) and normal keratinocytes and sheets (NKC). No positive bands were detected in nontransduced NS keratinocytes and sheets (UT). In each blotting, the first three lanes were loaded cell lysates from cultured keratinocytes before sheet culture. The last three lanes were loaded lysates from harvested sheet cultures, except for the patient 006 where only sheet samples were loaded. The samples from P005 were too little to perform the assay. The expression of β-actin was used as internal and loading control. dpt, days post-transduction; LEKTI, lympho-epithelial Kazal-type-related inhibitor; NKC, normal keratinocytes and sheets; NS, Netherton syndrome; UT, nontransduced NS keratinocytes and sheets.
All five patient-derived transduced keratinocyte populations progressed to epithelial sheet culture, with three of the five cultures (P002, P003, and P004) maturing sufficiently to form the requisite sheets over a 23- to 25-day period. These met the release criteria based on scores for clarity, size, integrity, color, and lift ability. There was comparable LEKTI expression in NS sheets transduced with LV-INVO-SP virus compared with the sheets generated using normal donor keratinocytes, whereas there was no LEKTI expression in control sheets generated using nontransduced NS keratinocytes, examined by in situ immunofluorescence staining (Fig. 2). The total duration of the process from the expansion of newly isolated keratinocytes from a skin biopsy to sheet lifting was ∼44 days.
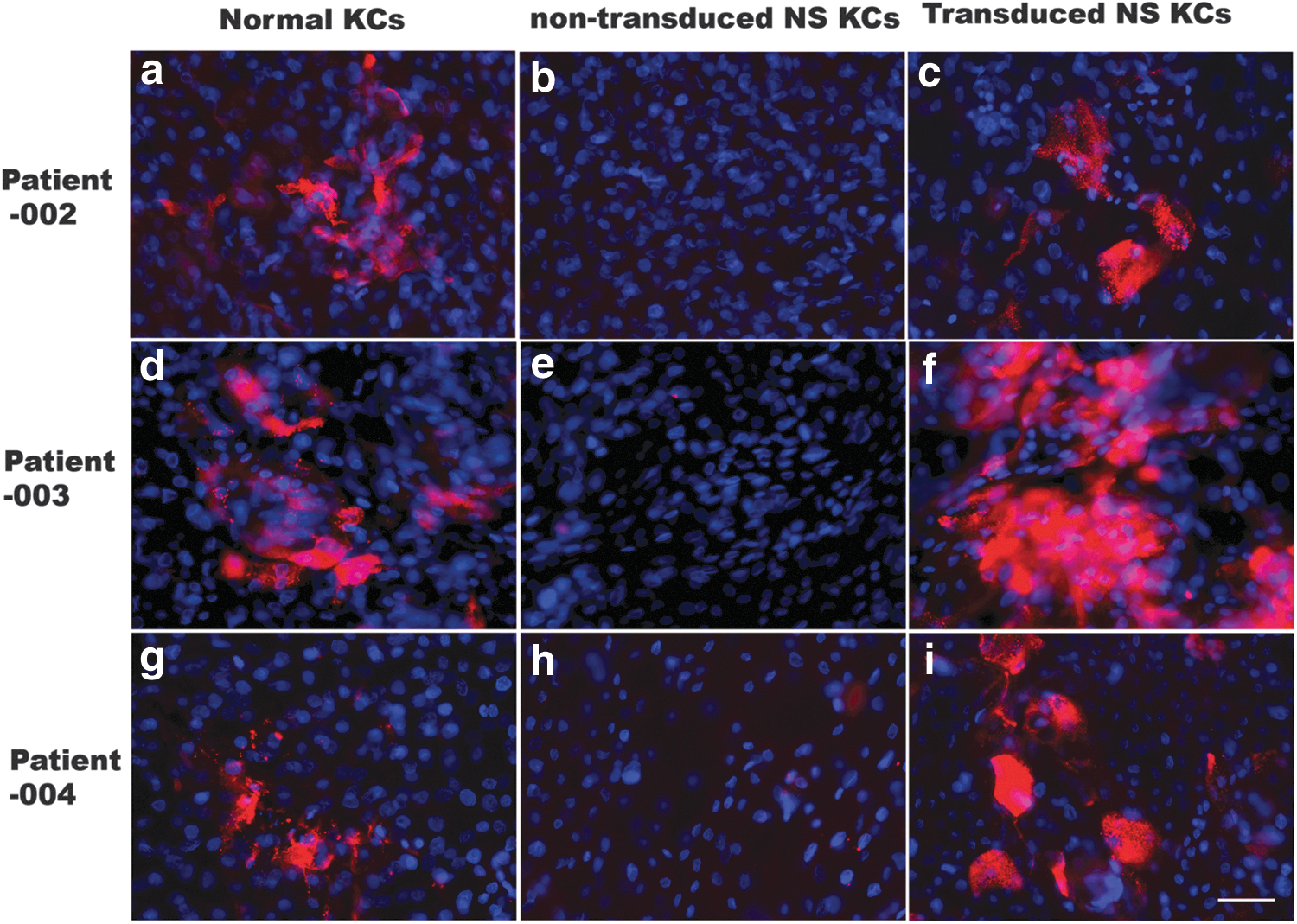
The expression of LEKTI in the gene-modified epithelial sheets. The epithelial sheets were generated using nontransduced or transduced keratinocytes from patients with NS (NS KCs) and normal donor keratinocytes (normal KCs) that were run in parallel as positive control. The expression of LEKTI was examined by in situ immunofluorescence staining. There was a comparable LEKTI expression (red) in the transduced sheets
Two epithelial sheets (P005 and P006) did not meet the release criteria. These sheet cultures exhibited either overgrowth of fibroblasts or dominant differentiated keratinocytes in the epithelial cultures, which probably inhibited the formation of a cohesive epithelial sheet (Supplementary Fig. S3). The overgrowth of fibroblasts was of human origin and not derived from murine 3T3 feeder cells, as confirmed by qPCR using specific primers for murine SPINK5 DNA.
Gene-modified epithelial sheet grafting and clinical observations
Two subjects with successfully generated grafts were withdrawn before grafting; one became unavailable within the scheduled grafting period and the other was considered clinically unstable.
Patient P003 was prepared with a 4 × 5 cm (20 cm2) graft bed on the anterolateral aspect of the left thigh by a surgical de-epidermization under local anesthetic. The upper epidermis was removed and the gene-modified epithelial sheet was attached on the de-epidermized bed, with an externalized Tricotex dressing. Mepitel soaked in saline was placed on the grafted area, and then, Mepitel film was applied to secure the graft in place (Fig. 3b). A Coban™ dressing was further applied on the top of Mepitel film. The patient was discharged from the hospital on the same day. Post-graft monitoring of the patient lasted for 12 months. Visual inspection showed that the graft looked healthy with an epithelialized appearance within the first week and complete healing with mild post-inflammatory hyperpigmentation at 1 month (Fig. 3c, d). Three months after grafting, the graft had blended with the surrounding skin (Fig. 3e). There were no signs of infection or other complications.
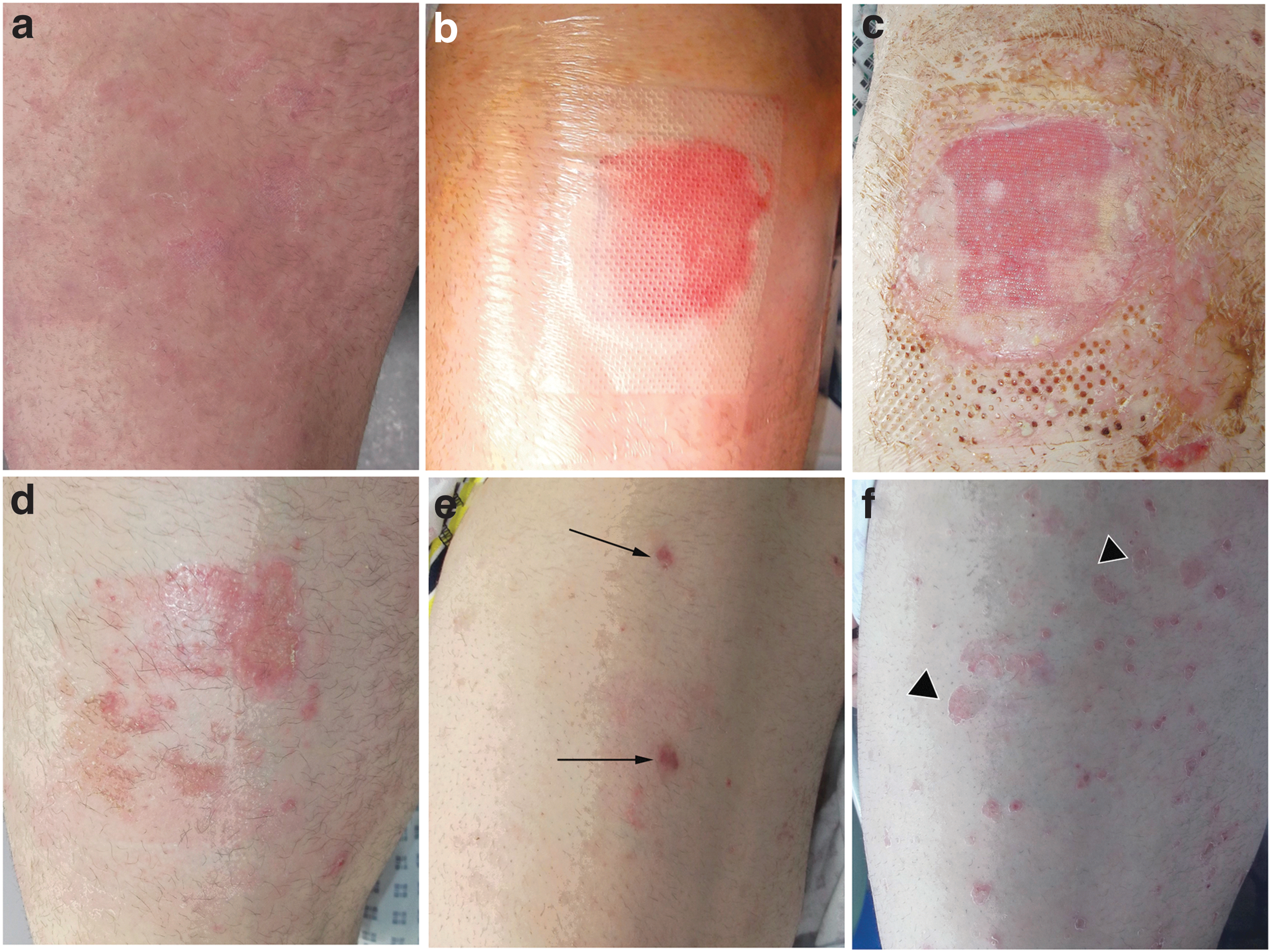
Gene-modified epithelial sheet graft on the patient (003) with NS. The photos were taken from the anterolateral aspect of left thigh in the patient before grafting
Transient detection of proviral vector and the expression of LEKTI in the graft
Paired serial skin biopsies were taken at months 1, 3, 6, and 12 after grafting. Each pair included a biopsy from within the graft area and another one from outside the graft area ∼4 cm away from the edge of the graft. Proviral copy numbers, LEKTI expression, and skin morphology were examined in the biopsies. VCN could be detected within the graft area after 3 months (0.0015 VCN per cell). The expression of LEKTI was also detected but at levels lower than that in normal skin and declined over time until barely detectable by month 6 (Fig. 4e–g). A very weak LEKTI signal was detected in the biopsy sample taken from outside the graft area at month 1 (Fig. 4i).
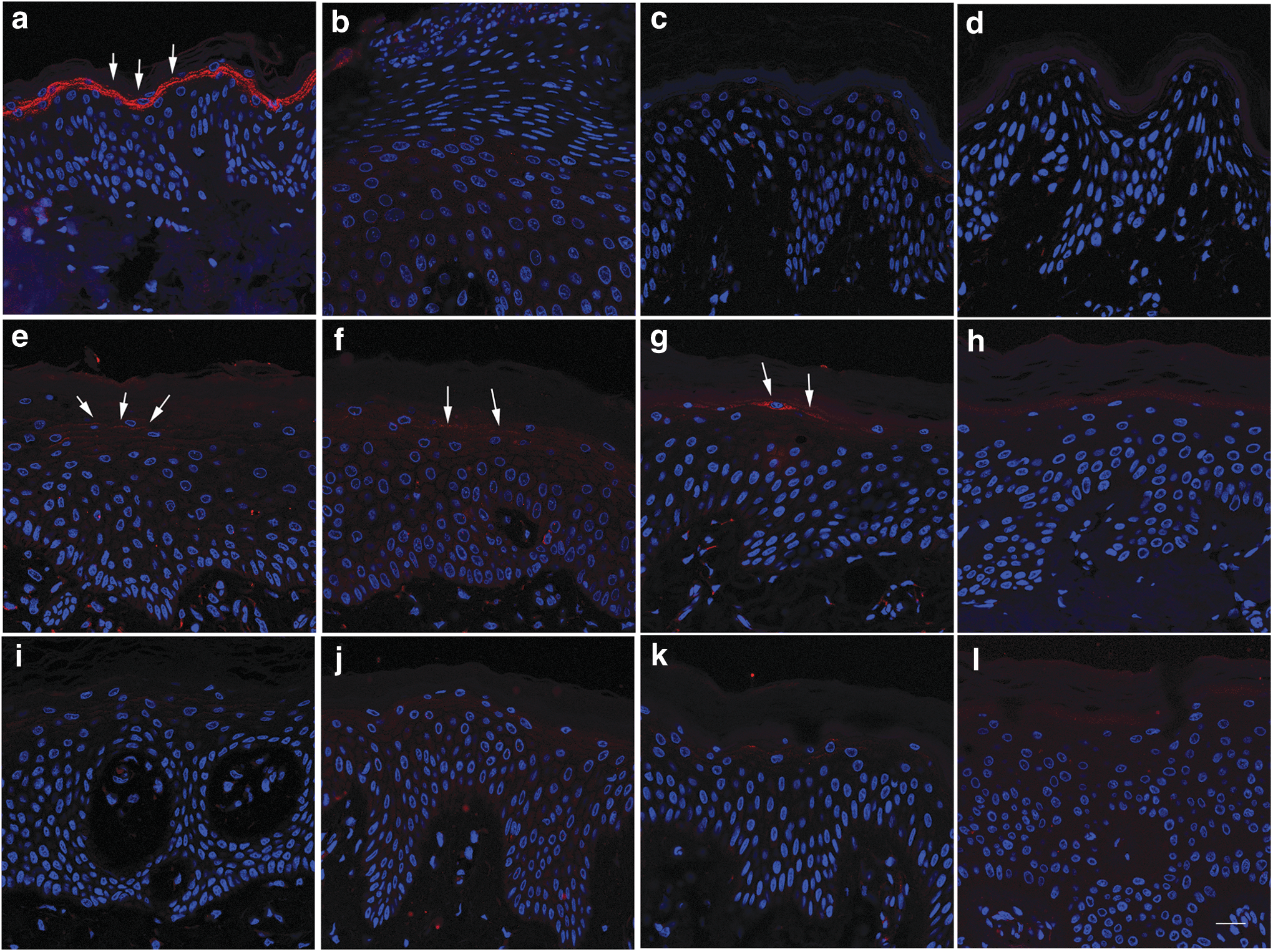
The expression of LEKTI in the grafted and outside grafted skin in P003. In the normal skin, LEKTI was highly expressed in the stratum granular layer
Lentiviral ISs were evaluated in nontransduced and transduced epithelial sheets before grafting and a skin biopsy taken from the area 3 months after grafting. LAM-PCR revealed a polyclonal IS pattern for transduced epithelial sheet before grafting, but only revealed few bands in the skin biopsy sample, likely due to the limited amount of modified DNA recovered from the biopsy (Supplementary Fig. S4a). Deep sequencing results obtained by MiSeq sequencing recovered 828,609 raw sequencing reads, which revealed 215 unique and precisely mappable ISs (Supplementary Table S3). Bioinformatic analyses of sequenced LAM-PCR amplicons found that transduced cells had a polyclonal IS pattern with no preferred integration in or near genes previously involved in serious adverse events in other gene therapy studies (Supplementary Fig. S4b).
Biopsy histology assessed by H&E staining was comparable for hypergranulosis, psoriasiform cornification (integrity of cornified layer, parakeratosis, exfoliated corneocytes), and lymphohistiocytic infiltration. 17 Mild morphological differences were noted including reduced rete ridges at months 1 and 3 (Fig. 5c–f vs. g–j) and a lower density of nuclei in the upper compartment of the epidermis within the graft area at months 1 and 3 (Fig. 5c, d) compared with the outside graft area at time points and late time points (Fig. 5g, h and e, f).
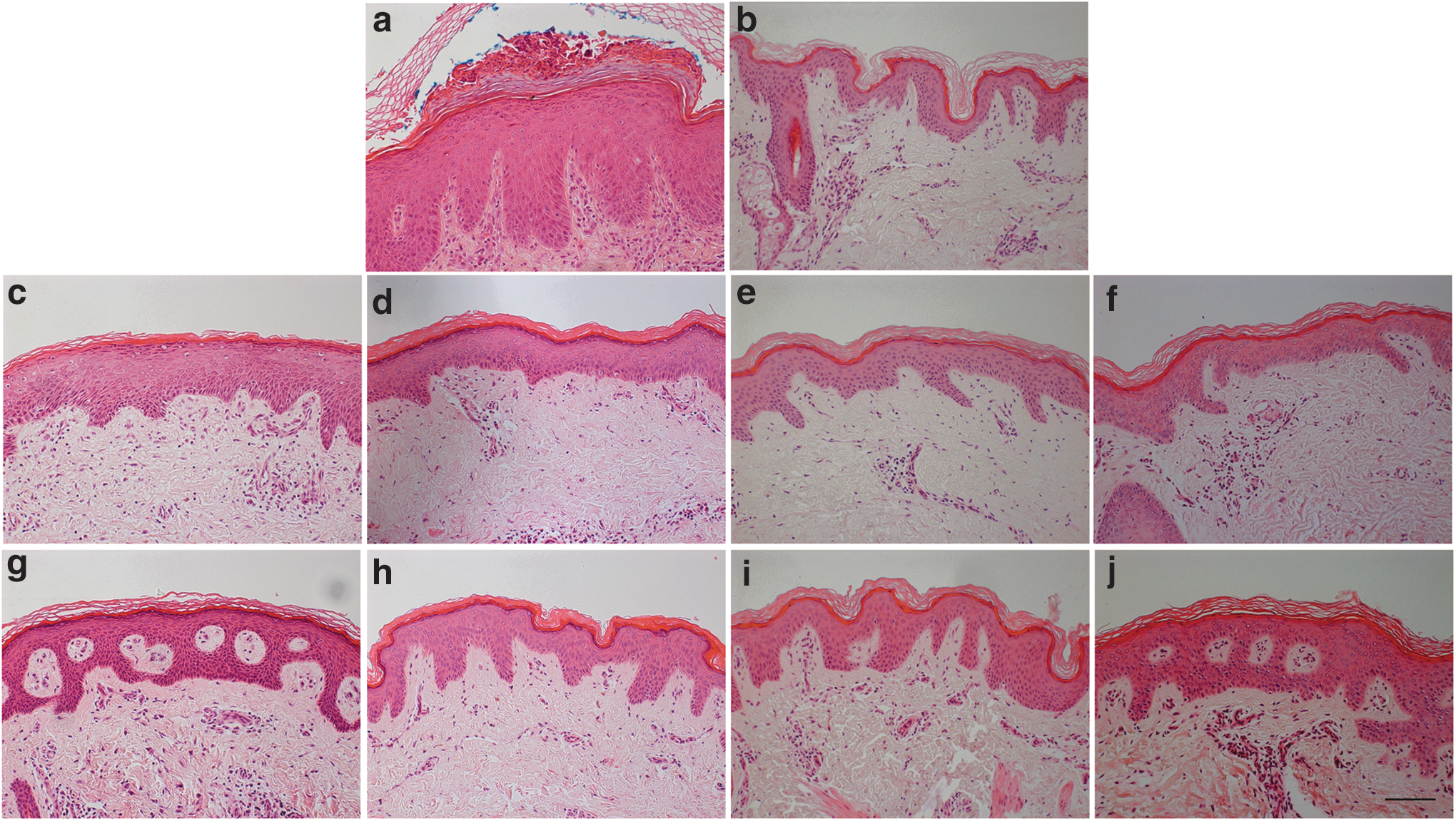
Histology of P003 skin within and outside the gene-modified epithelial graft. Skin biopsies were taken from lesional skin
Functional correction of LEKTI confirmed by expression patterns of KLK5
To evaluate the functional restoration of LEKTI on gene-modified sheets, the expression of KLK5, usually controlled by LEKTI, was examined. In the normal healthy skin, KLK5 was expressed and localized within the cornified layer of the epidermis, whereas in the NS skin, KLK5 was displaced to the lower suprabasal layers of the epidermis (Fig. 6a, c). Image analysis captured these differences as a sharp intensity peak at the cornified layer in normal skin compared with a shifted peak in suprabasal layers in P003 (Fig. 6m, n). At month 1, the peak within the graft area was similar to that found in normal donor skin, indicating a correction of KLK5 expression (Fig. 6e, p). Interestingly, the area outside the grafted skin also showed a similar expression pattern to the normal skin (Fig. 6f, q). However, KLK5 expression has reverted by months 3, 6, and 12 (Fig. 6r–w). The ratio of KLK5 expression between cornified and suprabasal layers was significantly different in samples taken from normal and NS baseline skin at months 1 and 3 outside skin samples and at months 6 and 12 inside and outside skin samples (p < 0.05, ANOVA and post hoc t-test). However, there were no differences between normal and inside skin samples taken at months 1 and 3 (p = 0.48 and 0.06, ANOVA and post hoc t-test). All these findings were consistent with transient expression and functional correction of LEKTI within the gene-modified epithelial graft.
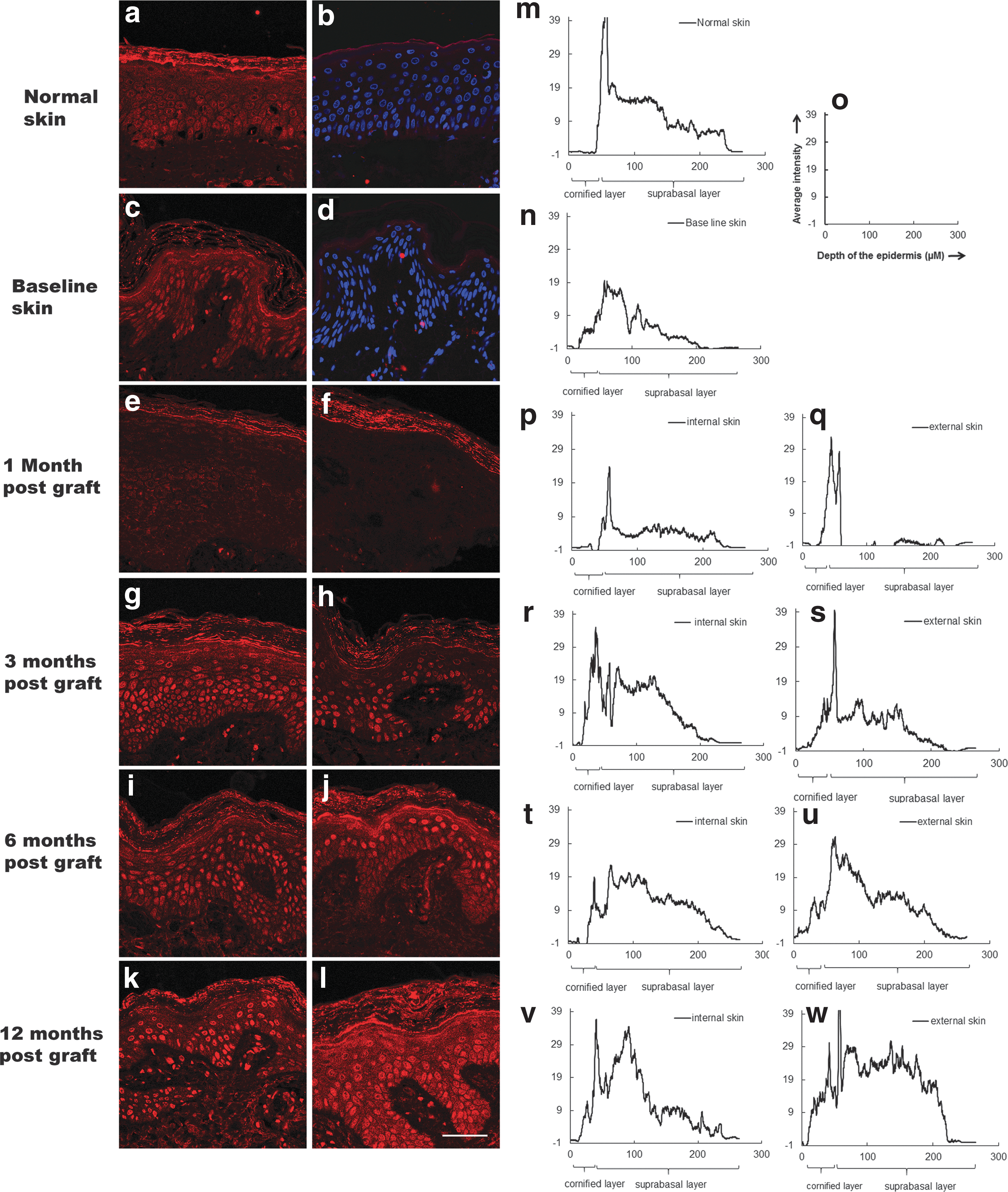
The expression of LEKTI downstream target KLK5 in the grafts. Reduced KLK5 (red color) was observed in the grafted
Skin barrier function and host immune responses to LEKTI
TEWL was also measured before and after grafting in the patient using the VapoMeter with results showing no significant changes of TEWL before and after grafting.
Immune response following sheet grafting was assessed by examining peripheral blood cellular IFN-γ immune responses against the LEKTI protein using ELISPOT assay. There was an increased number of positive spots at month 12, which may have indicated cell-mediated immunity against the graft; however, the difference compared with the baseline PBMC sample was not significant (ANOVA, p = 0.08) (Supplementary Table S4). Such assessments of systemic cellular responses may not reflect localized tissue immune activity or capture possible antibody-mediated responses, and secondary challenge was not part of the study design or approval.
Discussion
This study aimed to determine the feasibility and safety of lentiviral gene-modified epithelial sheets in NS. Techniques for growing and expanding human keratinocytes, including keratinocyte stem cells, and culture as an epithelial sheet for autografts have been applied for more than 25 years 24 and are widely used in clinics for burn patients and chronic ulcers. This technique has been adopted in gene therapy for genetic skin conditions, in which autologous keratinocytes are genetically modified before being cultured as an epithelial sheet. 12 There is a recent successful case that utilized a retroviral gene-modified keratinocyte sheet therapy in JEB. 13 We used a similar approach successfully generating three gene-modified epithelial sheets for autografting, demonstrating the feasibility of lentiviral gene modification of primary keratinocytes.
A self-inactivating lentiviral vector configuration was used as previous studies have reported that this vector system was safe for the modification of hematopoietic stem cells in conditions, such as severe Wiskott–Aldrich syndrome, adrenoleukodystrophy, and beta thalassemia. 25,26 However, vector integration analysis has rarely been performed on primary keratinocytes. A report for self-inactivating murine leukemia virus vectors in primary keratinocytes previously reported a reduced “genotoxic” profile in transduced cells. 27 ISs for lentiviral vectors in a spontaneously immortalized keratinocyte cell line (HaCat) were also reported with integration preferences for gene and gene-rich regions as expected. 28,29 In this first application of lentiviral modification of primary keratinocytes, we analyzed ISs in lentiviral gene-modified epithelial sheets following lentiviral vector transduction and found no preference for ISs in or near genes previously associated with serious adverse events such as MDS1, EVI1, and LMO2 following gamma retroviral transduction of hematopoietic stem cell. 30 The detection of multiple ISs and polyclonal clonal contribution in primary keratinocytes suggested that no clonal dominance had occurred during the ex vivo culture period. Unfortunately, the limited recovery of modified DNA from biopsy samples precluded detailed characterization of ISs after grafting.
We found transient (less than 3 months) restoration of LEKTI expression and possible correction of a LEKTI downstream protein KLK5 expression, which was consistent with one to two cycles of keratinocyte proliferation and differentiation. This in turn suggested that the epithelial sheet was derived mostly from paraclones/meroclones, which exhibit relatively shorter replicative lifespans. 31 Skin-derived keratinocytes are heterogeneous, containing differentiated keratinocytes and stem cells. Using the culture approach established by Rheinwald and Green, 32 dissociated keratinocytes including keratinocyte stem cells can be cultured and form keratinocyte colonies in vitro. As only 0.1–1% of cells can form colonies, which have a great influence on the expansion of the keratinocyte population, it is of vital important to ensure a high plating efficiency of freshly isolated keratinocytes to support colony formation. The most influential factor for plating efficiency was probably the density of irradiated 3T3 feeder cells. 3T3 feeder cells secrete soluble factors into the culture medium and deposit basal lamina glycoproteins on the culture dish surface required for keratinocyte attachment, colony formation, prevention of early differentiation, and avoidance of human fibroblast overgrowth. 33 Our preclinical data had indicated successful holoclone formation and no evidence showed senescence and/or cytotoxicity in induced keratinocytes, 15 although preclinical study had used fresh irradiated 3T3 cells, whereas for the trial, frozen i3T3 were used to ensure GMP compliance. Two previous reports of successful gene-modified epidermal sheet therapy for JEB 12,13 with the grafted epithelial sheet exhibiting functional gene expression for more than 6 years in the first case 34 and more than 3 years in the second case. 13 Their evidence suggested that long-lasting, self-renewing keratinocyte stem cells had engrafted. Both trials used fresh-made irradiated feeder cells. We used a commercially sourced supply of frozen i3T3 cells, which had been previously characterized and banked with a certain level of batch-to-batch variation. The variation between batches of frozen i3T3 could further cause insufficient densities of feeder cells at the beginning of cultures, resulting in low plating efficiency and colony formation, overgrown fibroblasts, and/or early differentiated keratinocytes. This could explain failure to form a cohesive epithelial sheet due to overgrowth of human fibroblasts and/or dominance of differentiated keratinocytes in two subjects. Thus, an additional in-process quality controls in future studies may include clone-forming assays and quantification of surrogate stem cell markers, such as p63 and keratin 15. Alternative read-outs using single-cell RNA transcriptome analysis may allow identification of distinct stem cell populations within heterogeneous primary keratinocytes. 35 Approaches with feeder-free keratinocyte culture system have also been developed but have yet to be fully evaluated in clinical trials. 14,36
In the NS trial, it appears that residual basal layer cells may have persisted within the graft bed after a surgical de-epidermization, which manifested as differences in nuclei densities between upper and lower parts of the epidermis, as shown in Fig. 1c and d. When cells dissociated from the shaved epidermis from the graft bed were cultured, almost no colonies grew in the culture (data not shown), suggesting that a proportion of original keratinocytes may have remained in the graft area and these cells subsequently competed with the grafted population. The depth of de-epidermization may be critical factor and bed preparation in NS may be more complicated than in JEB as NS patients retain intact derma-epidermal compartment. Surgical denuding of the area and complete elimination of the basal compartment, and its resident stem cells, could result in scarring if the grafting process fails or is incomplete.
In conclusion, the lentiviral delivery platform and processes used for transducing primary keratinocytes and grafting of a modified autologous epithelial sheet were found safe and feasible. However, to ensure engraftment of long-lived stem cell populations and sustained protein expression, identification, isolation, and modification of critical keratinocyte stem cell populations are required.
Footnotes
Acknowledgments
The helpful support of Fiona McKay, clinical genetics at GOSH, and Wang Wei at Genewerks, Germany. Supported by the Moulton Charity in the United Kingdom, Newlife for Disabled Children, and the National Institute for Health Research (NIHR) Biomedical Research Centre based at Great Ormond Street Hospital/Institute of Child Health, and Guy's and St. Thomas' NHS Foundation Trust and King's College London and the GSTT NIHR Clinical Research Facility. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, or the Department of Health. Dr. Wei-Li Di is Great Ormond Street Hospital Children's Charity Senior Lecturer. Prof. Adrian J. Thrasher is a Wellcome Trust Senior Fellow in Clinical Science. Prof. Waseem Qasim is NIHR Research Professor (RP-2014-05-007).
Author Disclosure
The authors have declared that no competing financial interests exist in relation to this study. Profs. Qasim and Thrasher hold interests in Orchard Therapeutics.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.