
Abstract
Wound healing has been greatly challenging in different acute and chronic skin injuries. Among them, nonrevascularizable critical limb ischemic ulcers, venous leg ulcers, and diabetic lower limb or extremity ulcers are well-known refractory skin injuries that are difficult to treat. Partly differentiated, progenitor cell-based graft transplantation or direct injection of autologous stem cells might promote the wound healing process. Studies aiming to comprehensively analyze the effects of cell therapy on skin wound healing could provide clinical evidence for skin injury treatment. Different databases were searched for full-text publications on the comparison between cell therapy and regular therapy. Heterogeneity was detected by the I 2 method, and a fixed effect model was applied for data pooling if heterogeneity was absent. Publication bias was analyzed using a funnel plot, and 10 studies were finally included in this study. After a long-term follow-up, fewer patients underwent major amputation in the cell therapy group, compared with the standard therapy group, and those in the cell therapy group were characterized by a smaller ulcer area. Moreover, there was a significant difference in the wound healing rate between the intervention and control groups. However, pain caused by skin wounds was hardly mitigated by cell therapy in patients with critical limb ischemia. In this study, cell therapy proved effective in decreasing the size of ulcers and improving the wound closure rate. Additionally, the major amputation rate was decreased in the cell therapy group. However, the symptoms of pain were hardly alleviated by cell therapy in patients with cutaneous ulcers caused by peripheral artery disease-related critical limb ischemia.
Introduction
Wound healing is a ubiquitous challenge in surgical practice. 1,2 In general, wounds have various etiologies, including peripheral artery-related ischemic disease, venous thrombotic disease, diabetes mellitus, trauma, burn injury, and operative procedures. 3 Maintenance of physiological homeostasis is highly dependent on the integrity of the skin. As the largest organ, the skin can protect the organism from being invaded by biologically, chemically, or physically harmful factors. However, if the process of skin wound healing is hampered, the subcutaneous inner structure is hazardously exposed to different harmful factors, therefore immunoinflammatory injury could occur. Acute wound formation or chronic refractory wounds are significantly correlated with mortality and morbidity. 4 In addition, persistently unhealed wounds can bring great burden and extra cost to the medical care system. 5,6 In essence, wound healing involves restoring the integrity of the skin and mucosa, involving multifactorial and complicated self-repair mechanisms. 2,3 Incomplete wound healing leads to wound disclosure, and sustained wound disclosure for more than 1 month indicates a chronic phase of wound healing, also called a refractory wound. 7 Moreover, wound size should be considered in refractory wounds, and larger wound sizes are more difficult to treat. 2 –4 If the depth of the wound gets to the dermis, a cutaneous ulcer can be finally formed. It is well known that the disease process of diabetic foot ulcer, peripheral artery ischemic limb ulcer, or venous thrombotic lower limb ulcer could last for a long time and the related wound could be very difficult to treat. It has been reported that the effect of a regular regimen on limb cutaneous ulcers underlying critical limb ischemia is very limited. The size of the skin wound could only be slightly improved, and ulcer symptoms could be barely alleviated by wound care and dressing (regular treatment). 1,8,9 For diabetic foot ulcers, the therapeutic efficacy is not yet optimistic. Traditional therapeutic methods such as wound care and dressing are ineffective, and major amputation seemed to be inevitable in the long-term disease course. 10,11 Skin substitutes, which are repeatedly verified therapeutic methods to treat ulcerated wounds, show great safety and efficacy. Despite their clinical significance, the cost of skin substitutes is relatively high, which imposes an economic burden on patients and health care systems. 5,6 Chronic skin ulcers are hardly corrected by conventional treatment and therefore novel therapeutic methods should be developed. Platelet-rich plasma (PRP) has an advantage in accelerating wound healing 12 ; however, it was not clear whether PRP could improve diabetic foot and critical limb ischemic ulcers. 13 Cytokines that could potentially stimulate tissue regeneration have been reported to theoretically cure skin wounds; however, only platelet-derived growth factor has been shown to improve wound healing in a double-blinded, randomized controlled trial (RCT), although with a rather modest result. 14 Considering the process of wound healing involving multifactor and different repair mechanisms, a cocktail-like cytokine mix might be more effective, ignoring tremendously increased treatment expense. 1
Progenitor cells are a group of cells with different phases of differentiation, they can secrete cytokines, and they have the potential to differentiate into specific cell types within a certain circumference. 15 –17 Consequently, tissue repair and regeneration could be attained by progenitor cell transplants. Progenitor cell-based therapy is regarded as an alternative method of wound treatment. The emergence of cell therapy throws light on the treatment of chronic cutaneous ulcers underlying diabetes mellitus and peripheral artery/vein-related disease. In recent years, clinical experiences and evidences of cell therapy have been accumulated; however, controversial debates on the effects of cell therapy still exist. 17,18 Moreover, the sample size in a previous clinical study was relatively small. As a result, this study aimed to integrate existing studies and comprehensively investigate the efficacy of cell therapy based on pooled data from 10 clinical studies. 19 –28 To date, this study was the first to integrate data from studies on various types of cell therapies to treat skin wounds of different etiologies. This study was characterized by a relatively large sample size, aiming to evaluate the efficacy of cell therapy on chronic cutaneous ulcers underlying diabetic foot ulcers and peripheral, vascular, disease-related skin wounds.
Materials and Methods
Literature retrieval
The literature retrieval strategy was developed in accordance with Cochrane methods. Science Direct, SpringerLink, Web of Science, Cochrane Central Register of Controlled Trials, CINAHL, MEDLINE, ProQuest, and Network Digital Library databases were searched between January 2000 and March 2020, using key words such as wound healing, skin ulcer, cell therapy, stem cell, diabetic foot ulcer, critical limb ischemia, and venous thrombotic leg ulcer. The guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses were used to report this study. 29
Inclusion/exclusion criteria of candidate studies
Study filtration conformed to the patient, intervention, comparison, and outcome inclusion and exclusion criteria. Two investigators who were blinded to the study design were nominated to check the quality and eligibility of all retrieved studies and they collected the data independently. The inclusion criteria were as follows: English language publications; comparison between the cell therapy in addition to regular treatment regimen and the regular treatment regimen only; chronic cutaneous ulcer, which was characterized by a disease course of more than 1 month and the depth of wound getting to the dermis; underlying skin ulcer caused by three major diseases, including peripheral artery-related ischemic disease, venous thrombotic disease, and diabetes mellitus; full-text publication; having a follow-up duration of more than 3 months; human studies; and having a randomized and prospective design. Exclusion criteria included the following: cross-sectional studies, case studies (case reports or case series), single-arm studies (without parallel control), and review articles. If different publications were searched from the same cohort, the one with the largest sample size and most comprehensive data was chosen for further analysis.
Data collection and extraction
Data of interest, such as the number of total patients and the number of patients with events, were collected. Baseline demographic data and follow-up data were also collected. Outcomes of different treatments included changes in ulcer size, major amputation rate, pain score evaluated by the numerical rating scale (NRS), pain-free walking distance, and rest pain level.
Process of synthesizing and analyzing the extracted data
The analysis model was determined by the heterogeneity of the extracted data. If the data had a high degree of heterogeneity, a random effect model was adopted for analysis. For homogeneous data, a fixed effect model was used to integrate data and compare the effects of different therapies. After the data process, a suitable formula was chosen to calculate the pooled relative risk (RR) value. Visualization of the result was achieved using a forest plot. The risk of bias was assessed using the Cochrane risk of bias tool.
Statistics
Statistical heterogeneity of the extracted data was evaluated using the inverse variance (I-V) formula. Statistical analysis was performed using the Stata software 12.0 (Stata Corp., College Station, TX). For continuous variables, the standard mean difference was calculated, while the pooled RR value was calculated for categorical variables. Begg's and Egger's methods were applied to analyze the publication bias, and the result was illustrated by a funnel plot. All p-values were two-tailed, and the significant statistical parameter was set at 0.05 (95% confidential interval [CI]).
Results
Literature retrieval and demographic description of included studies at baseline
Literature search, data extraction, and the summary of characteristics of the included studies were performed by two independent investigators who were not informed of the study design. All 2,678 articles were searched, 489 were excluded for duplication, and 274 articles without full-text were excluded. Additionally, 1,905 articles were excluded for not matching the inclusion and exclusion criteria. Ten studies were finally filtrated and verified. 19 –28 The specific process of publication screening and validation is shown in the flow chart (Fig. 1). In Supplementary Table S1, the demography of patients in the included studies at baseline is described. Gender, age, proportion of race, body–mass index, concomitant medication, disease condition before cell therapy treatment, and other baseline characteristics seemed to be comparable among different studies (Supplementary Table S1). Characteristics of included studies are shown in Supplementary Table S2. In addition, quality assessment of eligible literatures is shown in Supplementary Table S3.
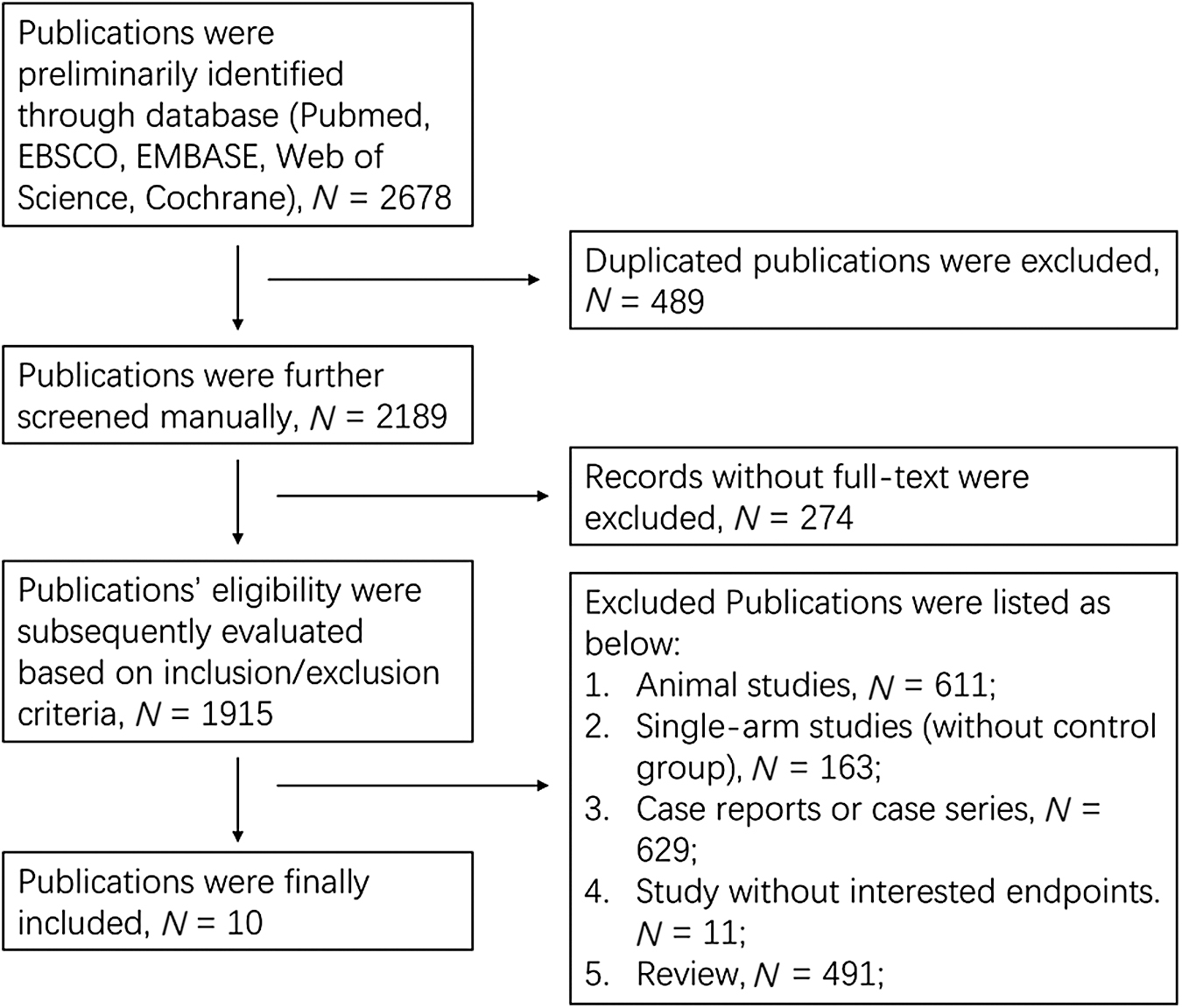
Literature screening and filtration.
Effects of cell therapy on ulcer size shrinkage and wound closure
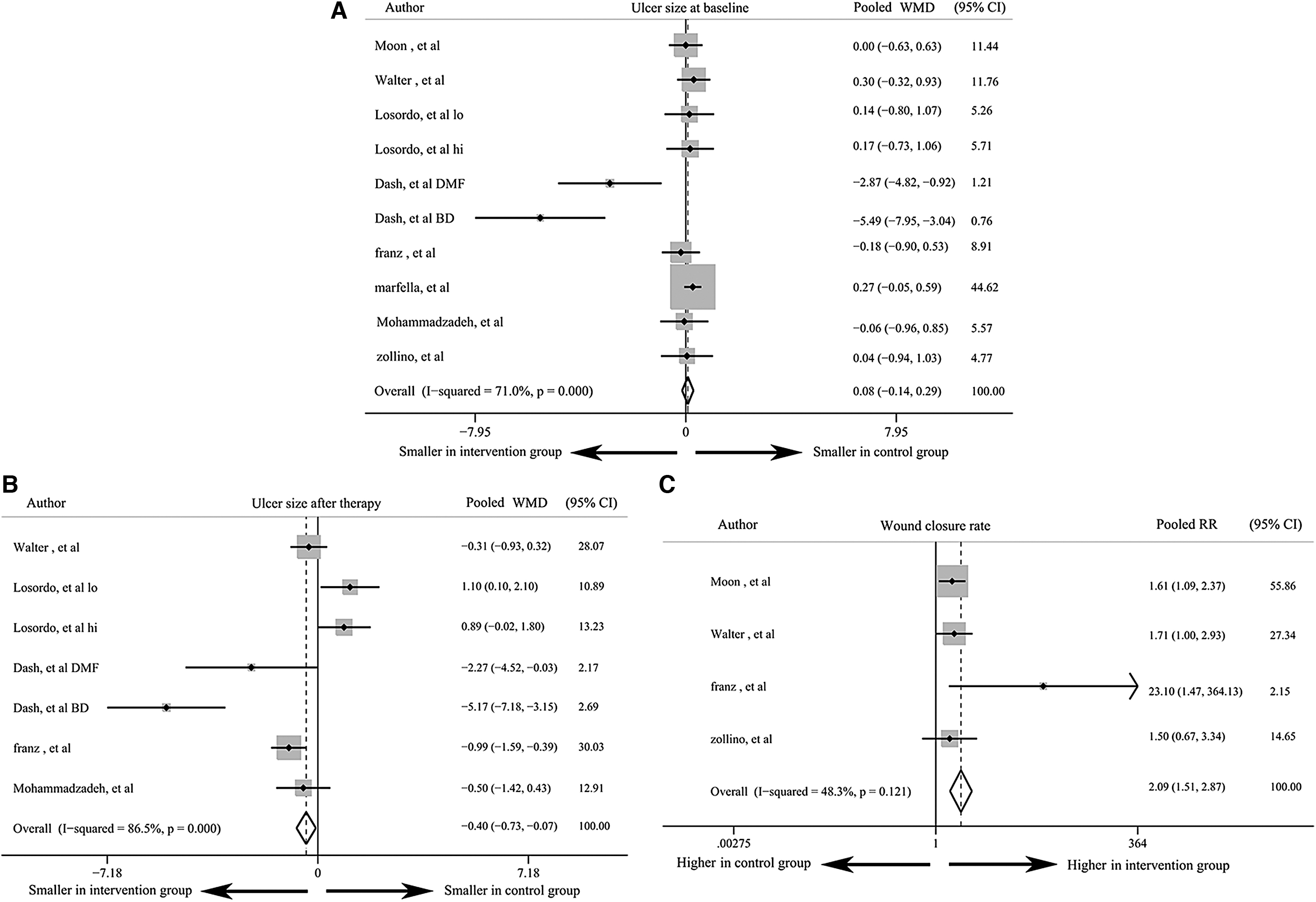
Five studies reported changes in ulcer size, and four studies reported the rate of wound closure. Significant heterogeneity was detected among these studies, regarding ulcer size (p < 0.001), and the random effect model was used in the analysis. Ulcer size of patients in the control and intervention groups showed no difference at baseline (weighted mean difference [WMD] = 0.08 cm2, 95% CI: −0.14 to 0.29), indicating similar disease conditions between groups (Fig. 2A). After several months, the ulcer size significantly decreased in the cell therapy group compared with the control group (WMD = −0.4 cm2, 95% CI: −0.73 to 0.07). Decreased ulcer size could not verify the efficacy of cell therapy (Fig. 2B), let alone wound healing (complete wound closure), which could further validate the efficacy of cell therapy. Therefore, the wound closure rate was compared between the groups. There was no heterogeneity in data on the wound closure rate, and the fixed effect model was subsequently used. Patients in the cell therapy group had a higher wound closure rate than those in the control group (pooled RR = 2.09, 95% CI: 1.51–2.87). Compared with ulcer shrinkage, complete wound closure was a more solid evidence of the efficacy of cell therapy (Fig. 2C).
Effects of cell therapy on ulcer size shrinkage and wound closure: comparison of ulcer size at baseline
Major amputation rate was hardly influenced
The rate of major amputation was reported in four studies. Therefore, data were extracted and synthesized, showing no heterogeneity (I 2 = 0, p > 0.05). Major amputation of the limb and extremity seemed to be unavoidable in the end phase of diabetic foot ulcers or peripheral, vascular, disease-related skin wounds. Early and timely intervention for cutaneous ulcers was the key step to prevent major amputation. In this study, cell therapy was shown to decrease the rate of major amputation (Fig. 3). The amputation rate was modestly, but significantly, influenced by cell therapy compared with the conventional treatment (pooled RR = 0.5, 95% CI: 0.27–0.93). This might be partly attributed to the heterogeneous disease conditions among patients within each study group, although disease conditions between the control and intervention groups were comparable (similar level of ulcer size at baseline). This indicated that cell therapy applied in the early phase could decrease the amputation rate more effectively.
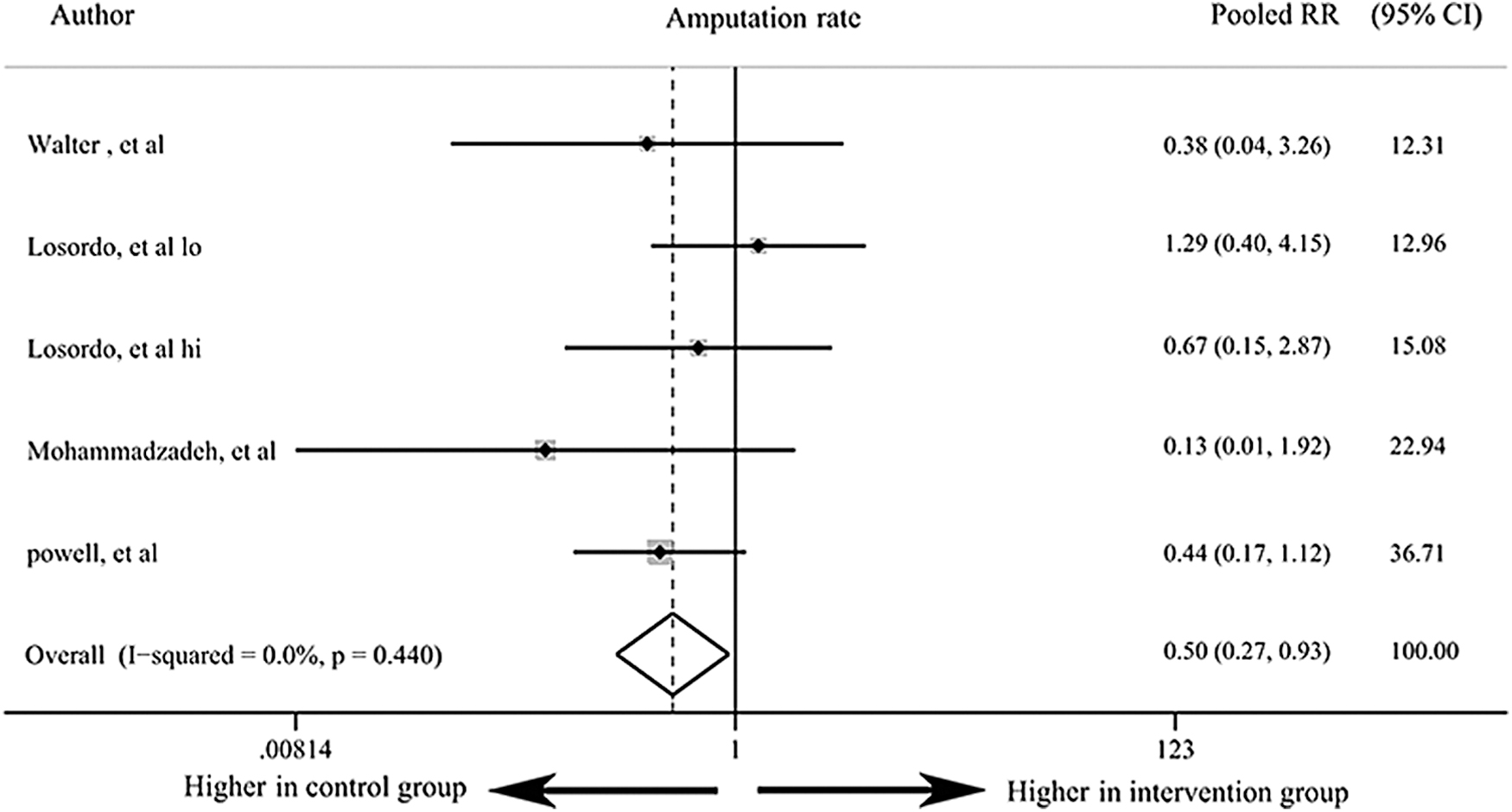
Difference in major amputation rates between groups after therapy.
Alleviation of symptomatic pain
Alleviating or even eradicating pain caused by wounds could apparently improve the quality of the patient's life. In this synthetic study, the effect of cell therapy on pain was assessed in three dimensions: the NRS score, pain-free walking distance, and level of rest pain. The difference in NRS scores between the groups was compared in two studies (I 2 > 50%), and the NRS score (Fig. 4A) tended to be lower and almost significant in the cell therapy group (WMD = −0.49, 95% CI: −1 to 0.02). The pain-free walking distance data were integrated and investigated in two other studies (I 2 > 50%), and the pain-free walking distance (Fig. 4B) was longer in the cell therapy group (WMD = 0.11, 95% CI: −0.44 to 0.66). The levels of rest pain (Fig. 4C) between the control and intervention groups were compared (I 2 > 50%), and it seemed that cell therapy-treated patients had a lower incidence of rest pain (pooled OR = 0.91, 95% CI: 0.77–1.07). These three parameters, which were all acquired through subjective judgment of patients, could fluctuate heavily. Pain indicators could be influenced by multiple factors, especially psychological factors, and these confounding factors might lead to bias.
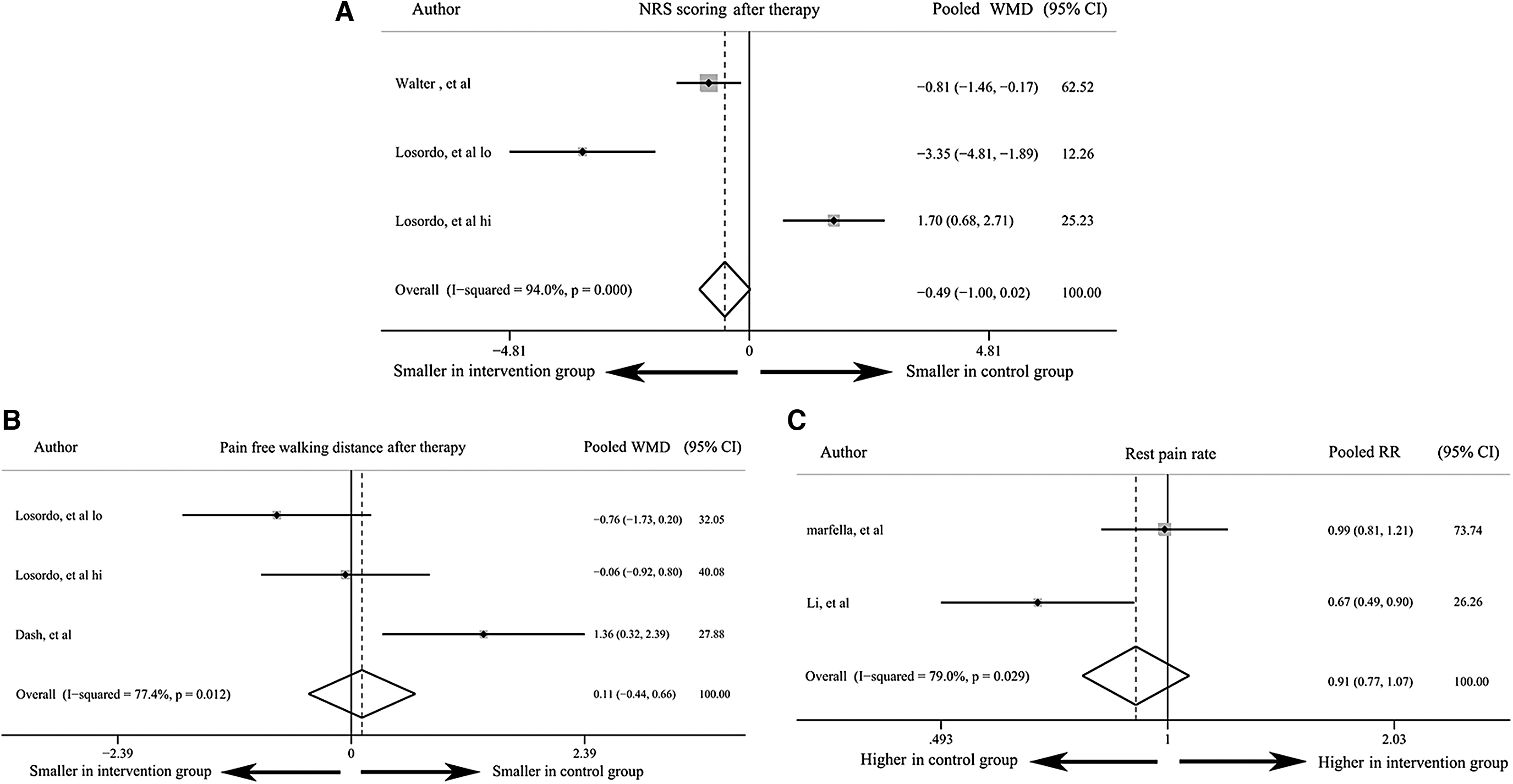
Evaluation of symptomatic pain in three dimensions: the NRS score between groups was compared
Publication bias analysis
The representative publication bias analysis by Begg's and Egger's tests showed a symmetrical distribution of included publications (Begg's test: p = 0.881; Egger's test: p = 0.433). These results indicated no publication bias among the articles included in this study (Supplementary Fig. S1).
Discussion
This synthetic study quantitatively analyzed data extracted from previously published, randomized, controlled clinical studies. 19 –28 This comprehensive investigation aimed to evaluate the effect of cell therapy on chronic cutaneous ulcers underlying diabetes mellitus and peripheral artery- and vein-related diseases. Different types of cell therapies, for instance, the bioengineered bilayered living cellular construct, allogeneic adipose-derived stem cells (ADSCs), bone marrow mononuclear cells, autologous CD34+ cells, autologous bone marrow-derived mesenchymal stem cells, cryopreserved placental tissue wound matrix, circulating bone marrow-derived endothelial progenitor cells, autologous granulocyte colony-stimulating factor-mobilized peripheral mononuclear cells, and autologous tissue repair cells, were regarded as the same method of intervention and they were applied to treat chronic skin ulcers. Changes in the ulcer size, ulcer wound closure rate, major amputation rate, pain score evaluated by the NRS, pain-free walking distance, and rest pain level were listed as the outcomes of cell therapy. In summary, cell therapy could significantly reduce the area of the skin wound, improve the wound closure rate, and decrease the major amputation rate. However, parameters reflecting pain, including the NRS pain score, reduction of rest pain level, and increase in the pain-free walking distance, were not improved by cell therapy. Nonetheless, the efficacy of cell therapy was preliminarily verified in this study.
Progenitor cells are a group of cells with different phases of differentiation, they can secrete cytokines, and they have the potential to differentiate into specific cell types within a certain circumference. 15,17 Progenitor cell-based graft therapy, also known as stem cell transplantation, has been proven to be very effective in hematopoietic diseases. 30 Moreover, cell therapy has also been applied in type I diabetes, 31 nervous system diseases, 32 autoimmune diseases, 33 respiratory diseases, and metabolic diseases. 34 The ability of cell therapy-induced tissue/organ regeneration or repair made it possible for refractory cutaneous ulcers to be curable. Evidence from basic research has revealed the critical role of cell therapy in skin wound healing. Rong et al. reported that stem cells effectively accelerated the wound closure rate and enhanced wound healing, which is possibly a result of the mechanism of transforming wound dermal fibroblasts into their fetal counterparts in a murine model. 35 Hamada et al. reported that autogenic ADSCs can promote vascularization and wound healing. 36 Luo et al. concluded that the use of ADSCs partially modulates microskin function and enhances wound healing by promoting angiogenesis in a full-thickness, skin defect mouse model. 37 Afterward, cell therapy underwent the transition from bench to bedside, and some pilot clinical trials offered clues for further studies. 38,39 Consequently, tissue repair and regeneration could be attained by progenitor cell transplants. Progenitor cell-based therapy is regarded as an alternative method of wound treatment. The emergence of cell therapy throws light on the treatment of chronic cutaneous ulcers underlying diabetes mellitus and peripheral artery- and vein-related diseases. However, some studies have acquired modest negative results regarding the efficacy of cell therapy. 17,27,40
Some meta-analyses have attempted to address the contradiction among different studies. It has been reported that in critical limb ischemia, cell therapy could not bring therapeutic benefit to wound healing. 40 Another meta-analysis centered on diabetic foot ulcers argued that stem cell-based therapy could enhance the healing of diabetic foot ulcers and is associated with lesser pain, a lower amputation rate, and improved prognosis, compared with normal treatment. 41 Regardless of etiology, this study included patients with chronic skin ulcers caused by either diabetes or peripheral vascular disease, concentrating more on the wound lesion (skin ulcer). In this study, cell therapy was proven to significantly decrease the ulcer size within a few months (3–6 months), indicating its efficacy in facilitating wound healing. Ulcer sizes between the intervention and control groups at baseline showed no difference, suggesting minimal heterogeneity in the included patients. However, the wound closure rate showed modest improvement and this was probably attributed to the relatively short follow-up duration. Contrarily, elongation of the cell therapy span could further increase the rate of wound closure. However, the therapeutic potency of the cell graft might disappear over time, resulting in incomplete wound closure. Patients could suffer from harsh pain resulting from skin wounds, especially deep cutaneous ulcers. Our study suggested that cell therapy could hardly alleviate pain in patients with critical limb ischemia. In this synthetic study, the effect of cell therapy on pain was assessed in three dimensions: the NRS score, pain-free walking distance, and level of rest pain. These three parameters, which were all acquired through subjective judgments of patients, could fluctuate heavily. Among them, the NRS score could be particularly influenced by patient's cognitive ability; hence, the visual analog scale might be used as a substitute for NRS. 42 Pain indicators could be influenced by multiple factors, especially psychological factors, and these confounding factors might lead to bias. In patients with diabetic foot ulcers, little pain is usually felt due to concomitant diabetic peripheral neuropathy. The major amputation rate seemed to show a modest difference between the groups, and this could be attributed to the severity of the disease condition at baseline and heterogeneity originating from the difference in disease course. Although the disease conditions between the control and intervention groups were comparable, heterogeneous disease conditions might exist within each study group. Further studies with more stringent inclusion/exclusion criteria are required in future to ensure that all patients have similar disease conditions at baseline. Nonetheless, our study still indicated that cell therapy applied in the early phase could more effectively improve the amputation rate.
Due to lack of sufficient data on cell therapy-related adverse event assessment, safety evaluation of cell therapy should be discussed in the future. The present study preliminarily confirmed the effects of cell therapy on chronic cutaneous ulcers, especially on decreasing the size of ulcers and increasing the rate of wound healing. Nevertheless, a long-term follow-up duration is required to further investigate the efficacy and safety of cell therapy for treating chronic cutaneous ulcers.
Limitations
First, with the lack of studies focusing on a specific type of cell therapy, heterogeneity might exist among different cell therapy types and this could lead to system bias. More focused clinical studies are required to solve this problem. Second, due to insufficient data on cell therapy-related adverse event assessment, the safety evaluation of cell therapy was not discussed in this study. Additionally, some literature from 10 quoted RCTs still lacks validity as the number of cases included in this meta-analysis is merely in the low two-digit range and the randomization is still questionable. Considering the limitations mentioned above, a well-designed RCT study to evaluate the efficacy and safety of cell therapy is required in future.
Conclusions
To date, this study was the first to integrate data from studies on various types of cell therapies to treat skin wounds of different etiologies. This study was characterized by a relatively large sample size, aiming to evaluate the efficacy of cell therapy on chronic cutaneous ulcers underlying diabetic foot ulcers and peripheral vascular disease-related skin wounds. In this study, within a follow-up duration of at least 3 months, cell therapy proved effective in decreasing the size of ulcers and improving the wound closure rate. Additionally, the major amputation rate was decreased in the cell therapy group. However, the symptoms of pain were hardly alleviated by cell therapy in patients with cutaneous ulcers caused by peripheral artery disease-related critical limb ischemia.
Ethics Approval and Consent to Participate
This meta-analysis did not involve ethics approval application.
Availability of Data and Material
The datasets used and/or analyzed during this study are available from the corresponding author upon reasonable request.
Footnotes
Authors' Contributions
Y.D. and X.S. carried out the studies, participated in collecting data, and drafted the manuscript. Q.Y. performed the statistical analysis and participated in its design. All authors have read and approved the final manuscript.
Author Disclosure
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.