
Abstract
ZD55-IL-24 is an armed oncolytic adenovirus similar but superior to ONYX-015. Virotherapeutic strategies using ZD55-IL-24 have been demonstrated to be effective against several cancer types. However, it is unclear whether the traditional administration strategy is able to exert the maximal antitumor efficacy of ZD55-IL-24. In this study, we sought to optimize the administration strategy of ZD55-IL-24 in both A375-bearing immunocompromised mouse model and B16-bearing immunocompetent mouse model. Although the underlying antitumor mechanisms are quite different, the obtained results are similar in these two mouse tumor models. We find that the antitumor efficacy of ZD55-IL-24 increases as injection times increase in both of these two models. However, no obvious increase of efficacy is observed as the dose of each injection increases. Our further investigation reveals that the administration strategy of sustained ZD55-IL-24 therapy can achieve a better therapeutic effect than the traditional administration strategy of short-term ZD55-IL-24 therapy. Furthermore, there is no need to inject every day; every 2 or 3 days of injection achieves an equivalent therapeutic efficacy. Finally, we find that the sustained rather than the traditional short-term ZD55-IL-24 therapy can synergize with anti-PD-1 therapy to reject tumors in B16-bearing immunocompetent mouse model. These findings suggest that the past administration strategy of ZD55-IL-24 is in fact suboptimal and the antitumor efficacy can be further enhanced through administration strategy optimization. This study might shed some light on the development of clinically applicable administration regimens for ZD55-IL-24 therapy.
INTRODUCTION
Gene therapy and virotherapy both made some important progress in the field of cancer therapy, but no big breakthrough has been achieved yet. Between 1999 and 2001, combination of gene therapy with virotherapy, named cancer-targeting gene virotherapy (CTGVT), was proposed to be a breakthrough cancer therapy strategy, in which tumor-targeting replicative oncolytic viruses (adenovirus, poxvirus, HSV-1, measles, etc.) were combined with therapeutic genes (IL-24, mk5, TRAIL, ST13, MnSOD, etc.) to increase antitumor efficacy. 1 –8 The antitumor effect of CTGVT is much higher compared with gene therapy alone or oncolytic virus therapy alone, no matter what therapeutic genes or oncolytic viruses were used, except that the genes and oncolytic viruses have mutual inhibitory effects, which did not occur in our already published over 100 Science Citation Index (SCI) articles in the indicated cancers. 1 CTGVT has more excellent antitumor effect than either gene therapy alone or virotherapy alone due to the fact that the oncolytic virus itself has antitumor effect and can highly replicate several hundred folds in cancer cells, and the inserted genes can also be amplified at the same magnitude. 1 ZD55-IL-24, one of the most effective CTGVT oncolytic viruses developed so far, was constructed by cloning the foreign antitumor gene mda-7/interleukin-24 (IL-24) into the tumor-targeting replicative oncolytic virus vector ZD55. 3 ZD55 is the first and the best CTGVT viral vector developed so far. It is an E1B 55-kDa gene-deleted adenovirus type 5 similar to ONYX-015, but with the marked difference of a cloning site to insert foreign antitumor genes. Other differences between ZD55 and other oncolytic adenoviruses are that ZD55 is an adenovirus type 5 homozygote and has an intact E3 region, whereas most of the other oncolytic adenoviruses are adenovirus chimaeras (e.g., ONYX-015 is a type 2/5 chimaera and Colo-Ad1 is a type 11/3 chimaera) 2,9,10 or have major deletions within the E3 region (e.g., ONYX-015, H101, and CG0070). 9 –11
Previous studies have shown that ZD55-IL-24 could selectively replicate in many types of human tumor cells and kill these cells more effectively than ONYX-015 or the replication-defective adenovirus carrying the IL-24 gene both in vitro and in vivo. 3,12,13 Combination of ZD55-IL-24 with another CTGVT oncolytic virus ZD55-TRAIL could even completely eradicate the established human colorectal cancer in nude mouse model. 14 In addition, the greatest limitation of oncolytic virotherapy is that the vast majority of oncolytic viruses cannot be administered systemically (e.g., intravenous injection and intraperitoneal injection), but must be administered intratumorally. 9,10,15,16 Hence, oncolytic viruses are difficult to be used to treat the vast majority of tumors in clinic. To overcome this limitation, we constructed a polyethylene glycol/lipids/calcium phosphate (CaP)-OncoAd (PLC-OncoAd) delivery system for ZD55-IL-24 in our recent work. 17 ZD55-IL-24, therefore, has great development prospects.
The mammalian immune system has evolved to restrict the replication and spread of invading pathogens. 18 The pre-existing and induced antiviral immune responses upon recognition of viral vectors as pathogens, hampers effective delivery and compromises adequate biodistribution required for cancer treatment. 19,20 Both specific (e.g., neutralizing antibodies or cytotoxic T lymphocytes) and nonspecific (e.g., phagocytes or antiviral cytokines) immune response mechanisms curtail the therapeutic efficacy of oncolytic adenovirus through virus clearance. 21 It is clear that intravascular administration of oncolytic adenovirus elicits a potent immune response, resulting in quick elimination and low antitumor effects. Within 24 h after intravenous administration, 90% of the oncolytic adenovirus is eliminated when it is injected by intravenous delivery. 16 Due to the considerable antiviral immune responses, oncolytic adenovirus is not well suited for administration by the strategy of systemic delivery objective to maintain the sustained potent cancer therapeutic effects. The high-level limitation of antiviral immunity in blood cannot be overcome through administration strategy optimization. However, this might not always be the case, as the components of antiviral immune responses tend to be predominantly localized in blood and faintly localized in peripheral tissues, especially at the tumor sites. 18,22 It is well known that the antiviral immune responses in peripheral tissues is much lower compared with blood. Therefore, the impact of antiviral immunity in tumor sites on antitumor activity of oncolytic adenovirus is greatly reduced. The response to intratumoral delivery, however, is not well defined as yet. The low-level limitation of antiviral immunity in tumor sites might be overcome through administration strategy optimization and tumor destruction capability of oncolytic adenovirus might be further improved after administration strategy optimization. Further investigation to this end is warranted.
In addition, the administration strategy optimization studies in mouse tumor models are an integral part of the antitumor drug development process. Administration strategy optimization data from murine might mirror clinical practice and are usually used to inform dose and schedule selection for clinical trials. They are particularly useful in situations when there are limited clinical data available to define the optimal administration strategy. It should be noted that there have been no reports on administration strategy optimization for oncolytic viruses in the literature to date. Given this critical gap in the literature, it is very significant to conduct the administration strategy optimization investigation on oncolytic viruses in mouse tumor models. To this end, administration strategy optimization studies were conducted in both A375-bearing immunocompromised mouse model and B16-bearing immunocompetent mouse model to identify optimal administration regimens that result in maximal tumor therapeutic effects of ZD55-IL-24. Further investigations to enhance antitumor activity by altering ZD55-IL-24 administration schedules in the murine model may have significance in the development of effective ZD55-IL-24 therapy for human cancer. This study provides a sound theoretical foundation for the future clinical application of ZD55-IL-24.
MATERIALS AND METHODS
Cells
All the cell lines used in this study were obtained from the Cell Bank of the Type Culture Collection of the Chinese Academy of Sciences (Shanghai, China). HEK293 cell was a human embryonic kidney cell line, transformed with Ad5 E1. B16 and A375 were the murine and human melanoma cell lines, respectively. The HEK293 and A375 cell lines were cultured in Dulbecco's modified Eagle's medium (DMEM). The B16 cell lines were cultured in RPMI-1640. Media were supplemented with 10% FBS, 50 U/mL penicillin, and 50 μg/mL streptomycin. All cell lines were maintained at 37°C with 5% CO2 and were not contaminated by mycoplasma, which was confirmed by PCR detection. 23
Adenoviruses
The recombinant adenoviruses ZD55-IL-24 used in this study have been previously described. 2,3 Briefly, ZD55 is a conditionally replicating adenovirus type 5 with E1B (55-kDa)-deleted and ZD55-IL-24 is a foreign human IL-24 gene-inserted ZD55 expressing IL-24. ZD55-IL-24 was propagated in HEK293 cells and purified by CsCl equilibrium centrifugation. Virus titers were determined by TCID50 assay using HEK293 cells and converted to plaque-forming units (PFU). The titer of ZD55-IL-24 was adjusted to 1.5 × 1010 PFU/mL.
Mice
All mice were obtained from Shanghai Laboratory Animal Center (SLAC), Chinese Academy of Sciences and maintained at ≤5 mice per cage under specific pathogen-free conditions in the Animal Care Facility of Shanghai Institute of Biochemistry and Cell Biology, Chinese Academy of Sciences. Mice were provided with water and rodent chow, and maintained under a regular 12-h light/12-h dark schedule at a constant room temperature (22°C ± 2°C). The responsible veterinarian was in charge of the diagnosis, treatment, and control of diseases in the animal facilities. All animal procedures were performed in strict accordance with the institutional guidelines and were approved by the Institutional Animal Care and Use Committee of Shanghai Institute of Biochemistry and Cell Biology, Chinese Academy of Sciences. Special attention was taken to determine the humane endpoints and to decide whether the mice should be euthanized to avoid further suffering. According to the 3Rs principle, experiments were carefully designed to minimize the use of mice and to obtain maximum amount of data. Animal experiments were reported in accordance with the ARRIVE guidelines. 24
Injection times optimization
Female C57BL/6 mice 6 weeks of age or BALB/c nude mice 4 weeks of age were obtained from SLAC and quarantined for about 2 weeks before tumor implantation. An inoculum of 1 × 106 B16 cells or 2 × 106 A375 cells was injected subcutaneously on the right flank of mice in 100 μL sterile phosphate-buffered saline (PBS). When the subcutaneous tumor size reached about 80 mm3, the mice were randomized into six groups using R software, and treatments were initiated as indicated in Figs. 1A or 3A. PBS was administered intratumorally at 50 μL/dose for five consecutive days in PBS group. ZD55-IL-24 was administered intratumorally at 25 μL/dose for only one day in EDA1-25 group. ZD55-IL-24 was administered intratumorally at 50 μL/dose for only one day in EDA1-50 group. ZD55-IL-24 was administered intratumorally at 50 μL/dose for two consecutive days in EDA2-50 group. ZD55-IL-24 was administered intratumorally at 50 μL/dose for three consecutive days in EDA3-50 group. ZD55-IL-24 was administered intratumorally at 50 μL/dose for five consecutive days in EDA5-50 group. The titer of ZD55-IL-24 was 1.5 × 1010 PFU/mL. Tumor size (volume = length × width 2 × 0.5) and body weight were measured every 2 days. Animal survival was also recorded every 2 days. Photographs of the mice were taken before the mice were euthanized. Mice were euthanized when the average tumor volume of PBS group exceeded 2,000 mm3.
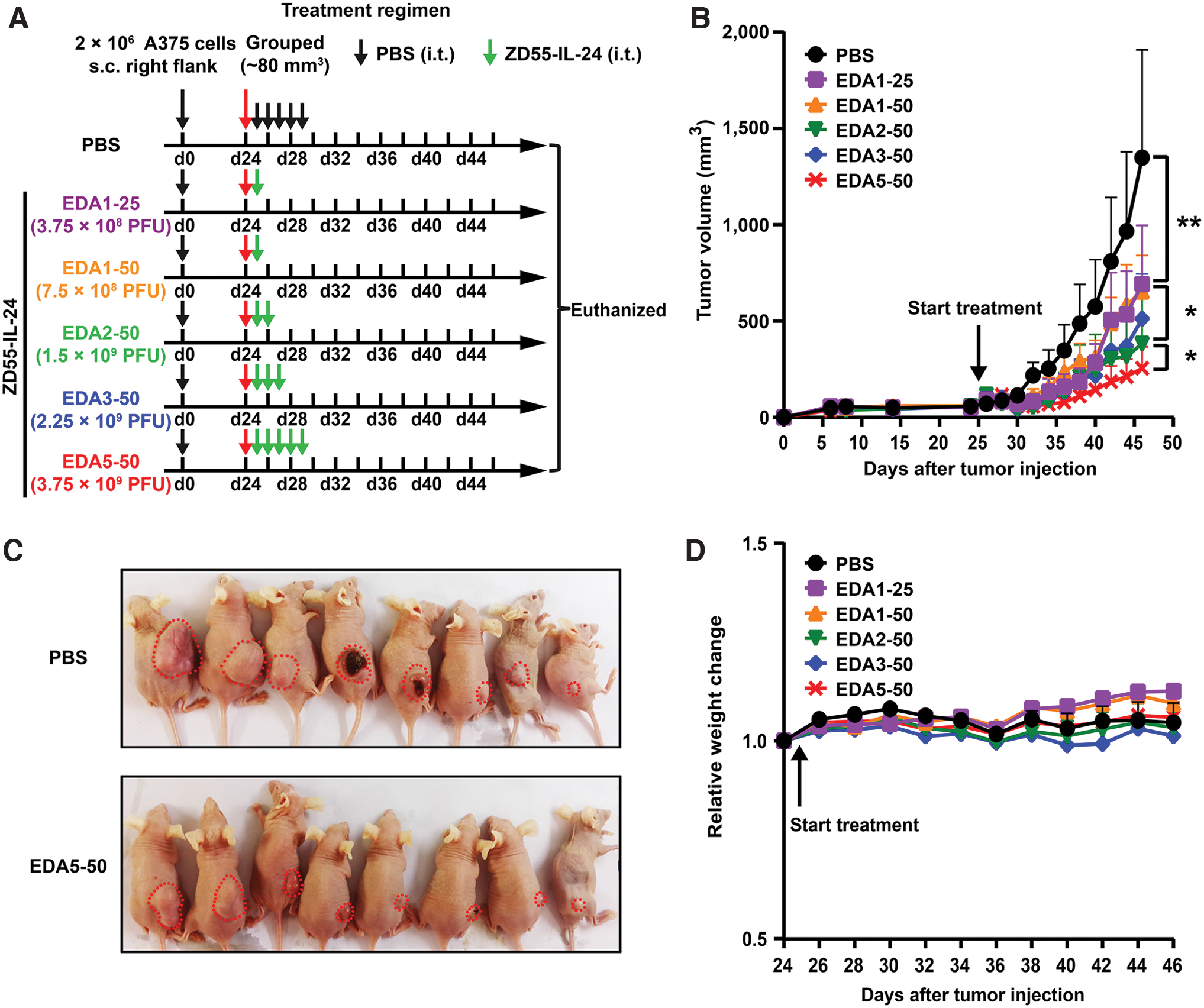
The antitumor efficacy of ZD55-IL-24 increases as injection times increase in A375-bearing immunocompromised mouse model. BALB/c nude mice were inoculated with 2 × 106 A375 human melanoma cells s.c. in the right flank and treated 25 days later (the average tumor volume was about 80 mm3) with PBS or ZD55-IL-24 via intratumoral injection as indicated.
Dose of each injection optimization
Female C57BL/6 mice 6 weeks of age or BALB/c nude mice 4 weeks of age were obtained from SLAC and quarantined for 1–2 weeks before tumor implantation. An inoculum of 1 × 106 B16 cells or 2 × 106 A375 cells was injected subcutaneously on the right flank of mice in 100 μL sterile PBS. When the subcutaneous tumor size reached about 80 mm3, the mice were randomized into five groups using R software, and treatments were initiated as indicated in Figs. 2A or 4A. PBS was administered intratumorally at 50 μL/dose for five consecutive days in PBS group. ZD55-IL-24 was administered intratumorally at 50 μL/dose for five consecutive days in EDA5-50 group. ZD55-IL-24 was administered intratumorally at 100 μL/dose for five consecutive days in EDA5-100 group. ZD55-IL-24 was administered intratumorally at 200 μL/dose for five consecutive days in EDA5-200 group. ZD55-IL-24 was administered intratumorally at 50 μL/dose every other day in EODA-50 group. The titer of ZD55-IL-24 was 1.5 × 1010 PFU/mL. Tumor size (volume = length × width 2 × 0.5) and body weight were measured every 2 days. Animal survival was also recorded every 2 days. Photographs of the mice were taken before the mice were euthanized.

The antitumor efficacy of ZD55-IL-24 does not increase significantly as the dose of each injection increases and the sustained ZD55-IL-24 therapy is superior to short-term therapy in A375-bearing immunocompromised mouse model. BALB/c nude mice were inoculated with 2 × 106 A375 human melanoma cells s.c. in the right flank and treated 25 days later (the average tumor volume was about 80 mm3) with PBS or ZD55-IL-24 via intratumoral injection as indicated.
Interval between two adjacent injections optimization
Female C57BL/6 mice 6 weeks of age were obtained from SLAC and quarantined for about 2 weeks before tumor implantation. An inoculum of 1 × 106 B16 cells was injected subcutaneously on the right flank of mice in 100 μL sterile PBS. When the subcutaneous tumor size reached about 80 mm3, the mice were randomized into four groups using R software, and treatments were initiated as indicated in Fig. 5A. PBS was administered intratumorally at 50 μL/dose every day until the experiment was terminated in PBS group. ZD55-IL-24 was administered intratumorally at 50 μL/dose every day until the experiment was terminated in EDA-50 group. ZD55-IL-24 was administered intratumorally at 50 μL/dose every other day until the experiment was terminated in EODA-50 group. ZD55-IL-24 was administered intratumorally at 50 μL/dose every 3 days until the experiment was terminated in ETDA-50 group. The titer of ZD55-IL-24 was 1.5 × 1010 PFU/mL. Tumor size (volume = length × width 2 × 0.5) and body weight were measured every 2 days. Animal survival was also recorded every 2 days. Mice were euthanized when all of the tumors in PBS group exceeded 2,000 mm3.
Combination therapy with short-term ZD55-IL-24 therapy and anti-PD-1 therapy
Female C57BL/6 mice, 6 weeks of age, were obtained from SLAC and quarantined for about 2 weeks before tumor implantation. An inoculum of 1 × 106 B16 cells was injected subcutaneously on both left and right flank of mice in 100 μL sterile PBS. When the right subcutaneous tumor size reached about 80 mm3, the mice were randomized into six groups using R software, and treatments were initiated as indicated in Fig. 6A. ZD55-IL-24 was administered intratumorally at 50 μL per dose (7.5 × 108 PFU/dose) for five consecutive days (both right and left tumors were administered). Therapeutic anti-PD-1 (BioXcell, BE0146) and isotype control antibody (BioXcell, BE0089) were administered intraperitoneally at 100 μg per dose in a volume of 100 μL antibody dilution buffer (BioXcell, IP0070) every 4 days. Tumor size (volume = length × width 2 × 0.5) was measured every 2 days, and mice were euthanized when the average tumor volume of PBS group exceeded 2,000 mm3. Photographs of the tumors resected from the sacrificed mice were taken immediately.
Combination therapy with sustained ZD55-IL-24 therapy and anti-PD-1 therapy
Female C57BL/6 mice, 6 weeks of age, were obtained from SLAC and quarantined for 2 weeks before tumor implantation. An inoculum of 1 × 106 B16 cells was injected subcutaneously on the right flank of mice in 100 μL sterile PBS. When the subcutaneous tumor xenograft size reached about 80 mm3, the mice were randomized into four groups using R software, and treatments were initiated as indicated in Fig. 7A. ZD55-IL-24 was administered intratumorally at 50 μL per dose (7.5 × 108 PFU/dose) every 3 days. Therapeutic anti-PD-1 (BioXcell, BE0146) was administered intraperitoneally at 200 μg per dose in a volume of 100 μL antibody dilution buffer (BioXcell, IP0070) every 3 days. Tumor size (volume = length × width 2 × 0.5) and body weight were measured every 2 days. Animal survival was also recorded every 2 days. Mice were euthanized when the average tumor volume of PBS group exceeded 2,000 mm3.
Statistical analyses
Statistical analyses were performed using GraphPad Prism 6.0. Comparisons between two groups were performed using Student's t-test. Comparison of multiple groups was performed by analysis of variance (ANOVA). Survival curves were analyzed using log-rank (Mantel–Cox) test. Differences were considered significant at p < 0.05 (*p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001, NS, not significant).
RESULTS
Administration strategy optimization by increasing the injection times in A375-bearing immunocompromised mouse model
Our previous studies have shown that ZD55-IL-24 had excellent antitumor activity in many immunodeficient mouse/human tumor xenograft models. 3,12 –14,25 However, it is unclear whether the therapeutic effect of ZD55-IL-24 can be further enhanced by optimizing the administration strategy. In our previous studies, ZD55-IL-24 was administered intratumorally for four or five consecutive days. 3,12,14 Therefore, we first wondered whether the antitumor efficacy of ZD55-IL-24 was affected by the injection times. In this article, to simplify reference to various ZD55-IL-24-treated groups, we created an acronym to designate the groups according to the administration method (EDA, EODA, or ETDA), total administration times (one time, two times, three times, or five times, but none represents keeping administration until the experiment is terminated) and injection volume per dose (25, 50, 100, or 200 μL). Taking EDA5-50 for instance, the “EDA” denotes every day administration (the “EODA” denotes every other day administration; the “ETDA” denotes every 3 days administration); the “5” denotes administration for five times in total; and the “50” denotes administration at 50 μL/dose. Hence, EDA5-50 denotes that ZD55-IL-24 is administered intratumorally at 50 μL/dose for five consecutive days. Similarly, EODA-50 denotes that ZD55-IL-24 is administered intratumorally at 50 μL/dose every other day until the experiment is terminated, and EDA-50 denotes that ZD55-IL-24 is administered intratumorally at 50 μL/dose every day until the experiment is terminated.
We began by testing the effect of treatment frequency on the efficacy of ZD55-IL-24 in A375-bearing immunocompromised mouse model. The dosing frequency was increased from one time (EDA1-25 and EDA1-50) to two times (EDA2-50), three times (EDA3-50), and five times (EDA5-50) (Fig. 1A). Our results indicated that the antitumor efficacy of ZD55-IL-24 in A375-bearing immunocompromised mouse model increased as injection times increased (Fig. 1B, C). On day 46, the tumor volume in the PBS-treated group was 1348.7 ± 559.7 mm3, whereas the EDA1-25 group was 692.7 ± 303.8 mm3, the EDA1-50 group was 653.3 ± 187.4 mm3, the EDA2-50 group was 381.8 ± 249.8 mm3, the EDA3-50 group was 512.6 ± 232.3 mm3, and the EDA5-50 group was 255.2 ± 111.2 mm3. The percentage of tumor growth inhibition increased from 51.6% (EDA1-50) to 62% (EDA2-50) and reached the maximum of 72.3% (EDA5-50). Of note, despite the increase in injection times, ZD55-IL-24 therapy was not associated with any significant systemic toxicity, as mice did not show shortened lifespan (no mice death) and weight loss (Fig. 1D) or abnormal appearance.
Administration strategy optimization by increasing the dose of each injection in A375-bearing immunocompromised mouse model
To understand whether the antitumor efficacy of ZD55-IL-24 was affected by the dose of each injection, we continued to optimize by increasing the dose of each injection based on EDA5-50. The dose of each injection was increased from 50 μL (EDA5-50) to 100 μL (EDA5-100) and 200 μL (EDA5-200) (Fig. 2A). No obvious increase of antitumor efficacy was observed as the dose of each injection increased (Fig. 2B), suggesting 50 μL was enough for each injection in A375-bearing immunocompromised mouse model. Furthermore, we compared the administration strategy of EDA5-50 (short-term ZD55-IL-24 therapy) with EODA-50 (sustained ZD55-IL-24 therapy) (Fig. 2A). Although a significant tumor growth inhibition was observed in EDA5-50, the tumors grew slowly as time went on (Fig. 2B). EODA-50, however, was able to completely eradicate the established tumors and did not have a relapse after stopping administration during the observation period (Fig. 2B, C). All the A375 melanoma-bearing mice in the EODA-50 group had complete remission, whereas there was no observable tumor remission in the EDA5-50 group (Fig. 2D). These data, therefore, suggested that the administration strategy of EODA-50 was superior to the administration strategy of EDA5-50, which was used in our previous studies, further indicating that the administration strategy of sustained ZD55-IL-24 therapy was superior to short-term ZD55-IL-24 therapy in A375-bearing immunocompromised mouse model. Likewise, despite the increment in the dose of each injection, ZD55-IL-24 therapy was associated with no significant systemic toxicity in A375-bearing immunocompromised mouse model, as mice did not show weight loss and shortened lifespan (no mice death) or abnormal appearance even though the injection dose was increased to 200 μL/dose (Fig. 2E).
Administration strategy optimization by increasing the injection times in B16-bearing immunocompetent mouse model
In a recent study, we found that ZD55-IL-24 not only exhibits pronounced antitumor efficacy in immunodeficient mouse model but also in immunocompetent mouse model. 26,27 However, the underlying mechanisms are quite different. Because immunocompetent mice may recognize viral vectors as antigens and initiate much more potent immune clearance leading to suboptimal dosing, we therefore carried out the same optimization in B16-bearing immunocompetent mouse model (Fig. 3A). Our results indicated that the antitumor efficacy of ZD55-IL-24 in B16-bearing immunocompetent mouse model also increased as injection times increased in a certain range (Fig. 3B), which was consistent with the results in A375-bearing immunocompromised mouse model. On day 18, the tumor volume in the PBS-treated group was 2151.1 ± 310.6 mm3, whereas the EDA1-25 group was 1175.5 ± 217.3 mm3, the EDA1-50 group was 1229.9 ± 293.6 mm3, the EDA2-50 group was 631.3 ± 99.4 mm3, the EDA3-50 group was 347.0 ± 57.0 mm3, and the EDA5-50 group was 370.6 ± 94.5 mm3. The percentage of tumor growth inhibition increased significantly from 42.8% (EDA1-50) to 70.7% (EDA2-50) and reached the maximum of 83.9% (EDA3-50). However, there was no difference in tumor inhibition between EDA3-50 group and EDA5-50 group, suggesting that the three times administration produces optimal benefits. The median survival days was also increased from 20 days (EDA1-50) to 25 days (EDA2-50) and reached the maximum of >30 days (EDA5-50) (Fig. 3C). Taken together, these results indicated that the therapeutic effect of ZD55-IL-24 in B16-bearing immunocompetent mouse model was potentiated as injection times increased, similar to the results in A375-bearing immunocompromised mouse model. However, unlike the growth inhibition observed in immunocompromised mice model, there was no benefit in increasing the frequency of administration from three times to five times in immunocompetent mice. Notably, despite increase in injection times, ZD55-IL-24 therapy was also not associated with any significant systemic toxicity in B16-bearing immunocompetent mouse model, as mice did not show shortened lifespan and weight or hair loss as well as abnormal appearance (Fig. 3C, D).
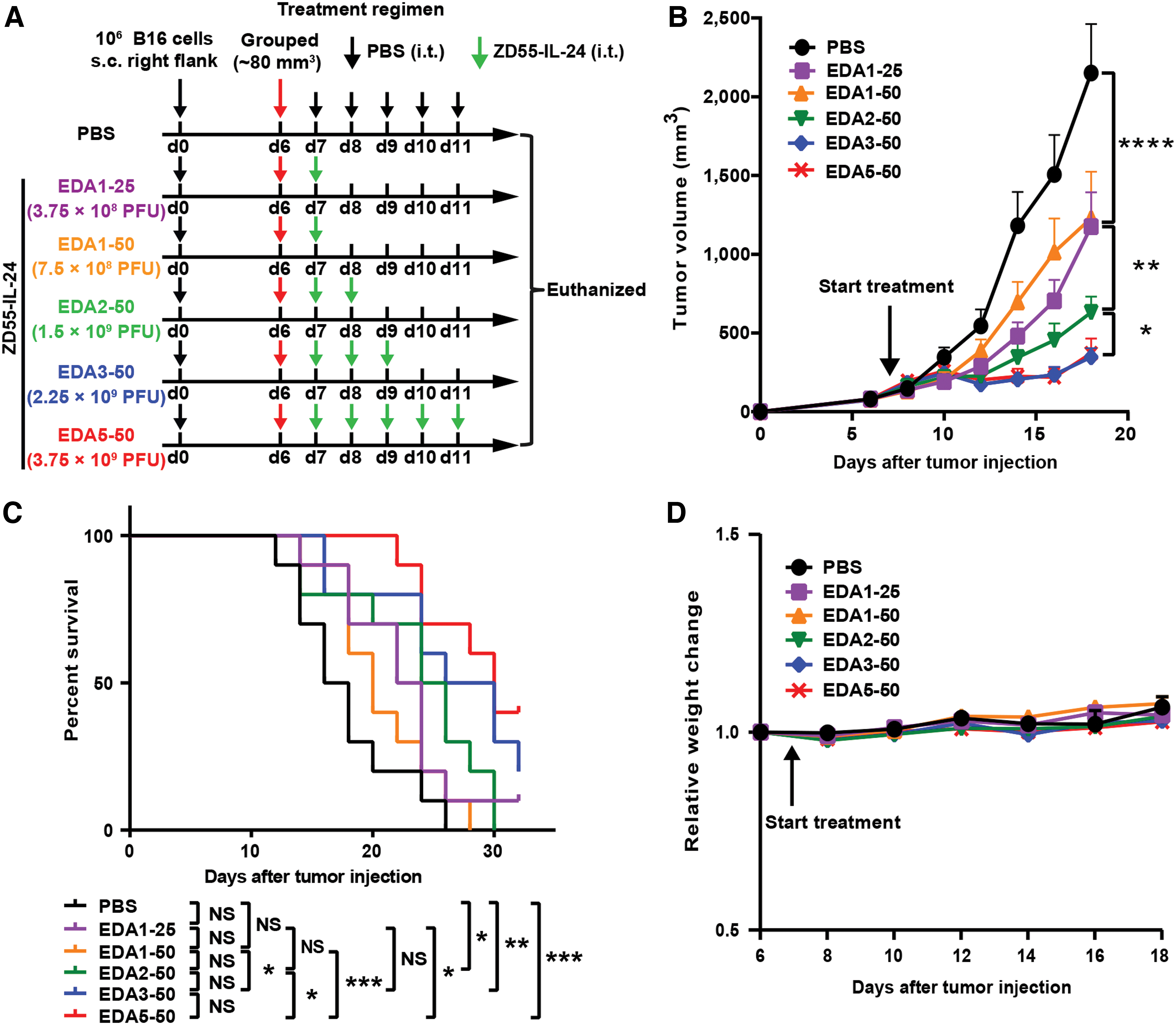
The antitumor efficacy of ZD55-IL-24 increases as injection times increase in B16-bearing immunocompetent mouse model. C57BL/6 mice were inoculated with 1 × 106 B16 murine melanoma cells s.c. in the right flank and treated 7 days later (the average tumor volume was about 80 mm3) with the indicated PBS or ZD55-IL-24.
Administration strategy optimization by increasing the dose of each injection in B16-bearing immunocompetent mouse model
Based on EDA5-50, we continued to optimize by increasing the dose of each injection in B16-bearing immunocompetent mouse model (Fig. 4A). However, both the tumor growth inhibition effect (Fig. 4B, C) and the survival rate (Fig. 4D) increased only slightly as the dose of each injection increased, showing that 50 μL was also sufficient for each injection in B16-bearing immunocompetent mouse model, which was in line with the results obtained from A375-bearing immunocompromised mouse model. Moreover, we also compared the administration strategy of EDA5-50 (short-term ZD55-IL-24 therapy) with EODA-50 (sustained ZD55-IL-24 therapy) in B16-bearing immunocompetent mouse model (Fig. 4A). Although a significant tumor growth inhibition effect was observed in EDA5-50 before day 22, tumor growth resumed in a rapid rate after day 22 (Fig. 4B), indicating that the antitumor efficacy of EDA5-50 keeps only for short term (keeping for 13 days). EODA-50, however, was able to significantly suppress the growth of tumors until the experiment was terminated (keeping for 29 days) (Fig. 4B). In addition, EODA-50 also showed survival benefit compared with EDA5-50 (Fig. 4D). These data, therefore, suggested that the administration strategy of EODA-50 was superior to EDA5-50 for the long-term therapy, although no significant differences for the short-term therapy in B16-bearing immunocompetent mouse model. Importantly, ZD55-IL-24 therapy also did not present any obvious systemic toxicity as the dose of each injection increased in B16-bearing immunocompetent mouse model, even when the injection dose was increased to 200 μL/dose (Fig. 4D, E).
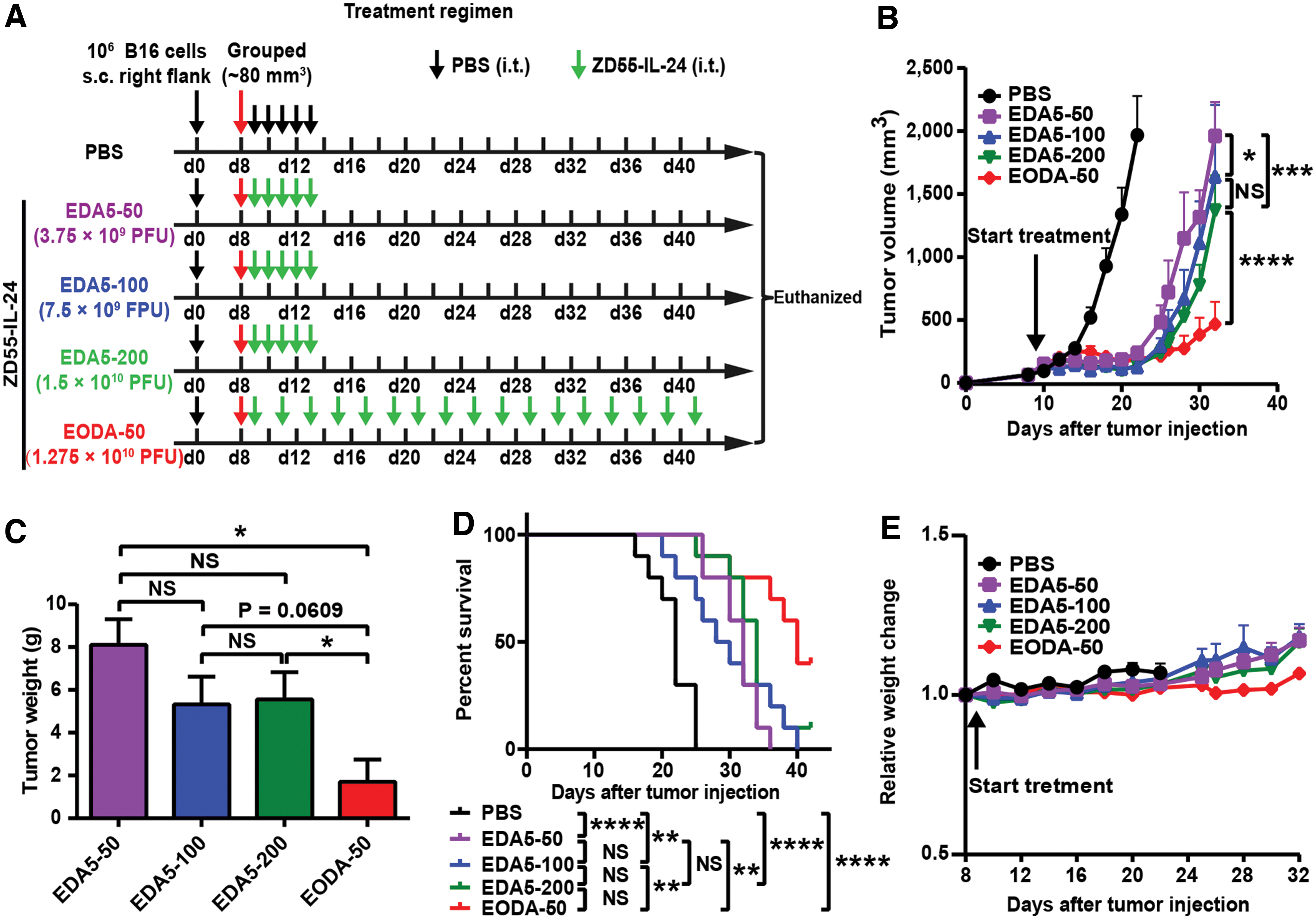
The antitumor efficacy of ZD55-IL-24 increases only slightly as the dose of each injection increases and the sustained ZD55-IL-24 therapy is also superior to short-term therapy in B16-bearing immunocompetent mouse model.
Administration strategy optimization by increasing the interval between two adjacent injections in B16-bearing immunocompetent mouse model
Based on EODA-50, we further wondered whether the tumor therapeutic efficacy of ZD55-IL-24 was affected by the interval between two adjacent injections in B16-bearing immunocompetent mouse model. The interval between two adjacent injections was increased from every other day (EODA-50) to every 2 days (ETDA-50), or shortened from every other day (EODA-50) to daily dosing (EDA-50) (Fig. 5A). Although the antitumor effect of EDA-50 appeared to increase slightly compared with EODA-50 and ETDA-50, there was no significant statistical difference (Fig. 5B–D), showing that there was no need to inject every day, and that we just need to inject every 2 or 3 days to achieve a best therapeutic efficacy of ZD55-IL-24. Similarly, ZD55-IL-24 therapy also showed without obvious systemic toxicity as the interval between two adjacent injections shortened in B16-bearing immunocompetent mouse model since the mice did not show shortened lifespan and weight or hair loss as well as abnormal appearance (Fig. 5D, E).

The antitumor efficacy of ZD55-IL-24 does not significantly increase as the interval between two adjacent injections shortens in B16-bearing immunocompetent mouse model.
The sustained but not the short-term ZD55-IL-24 therapy synergizes with PD-1 blockade therapy to reject tumors in B16-bearing immunocompetent mouse model
There is currently much enthusiasm for combining immune checkpoint blockade immunotherapy with other cancer treatment modalities. 28 –35 Motivated by this, we attempted to evaluate the synergistic effect between ZD55-IL-24 therapy and anti-PD-1 therapy in B16-bearing immunocompetent mouse model. ZD55-IL-24 was first injected by the administration strategy of EDA5-50, which was used in our previous studies (short-term injection) (Fig. 6A). Unfortunately, no significant synergy was observed between ZD55-IL-24 and anti-PD-1 antibody when ZD55-IL-24 was injected using the traditional administration strategy (Fig. 6B, C). Nonetheless, we next sought to examine using the administration strategy of ETDA-50 (long-term injection) (Fig. 7A). Of interest, we observed significant synergy between ZD55-IL-24 therapy and anti-PD-1 therapy when ZD55-IL-24 was injected using the optimized administration strategy (Fig. 7B–D). On day 20, the tumor volume in the PBS-treated group was 1546.2 ± 199.8 mm3, the ZD55-IL-24 group was 380.2 ± 76.0 mm3, the anti-PD-1 group was 713.5 ± 145.2 mm3, whereas the ZD55-IL-24/anti-PD-1 group was 194.3 ± 37.9 mm3. The percentage of tumor growth inhibition increased from 75.4% (ZD55-IL-24 group) and 53.9% (anti-PD-1 group) to 87.4% (ZD55-IL-24/anti-PD-1 group). There was also an increase in the median survival days from 28 days (ZD55-IL-24 group) and 21 days (anti-PD-1 group) to 32 days (ZD55-IL-24/anti-PD-1 group). These results thus indicated that only the sustained ZD55-IL-24 therapy was able to synergize with PD-1 blockade therapy to reject tumors in B16-bearing immunocompetent mouse model.
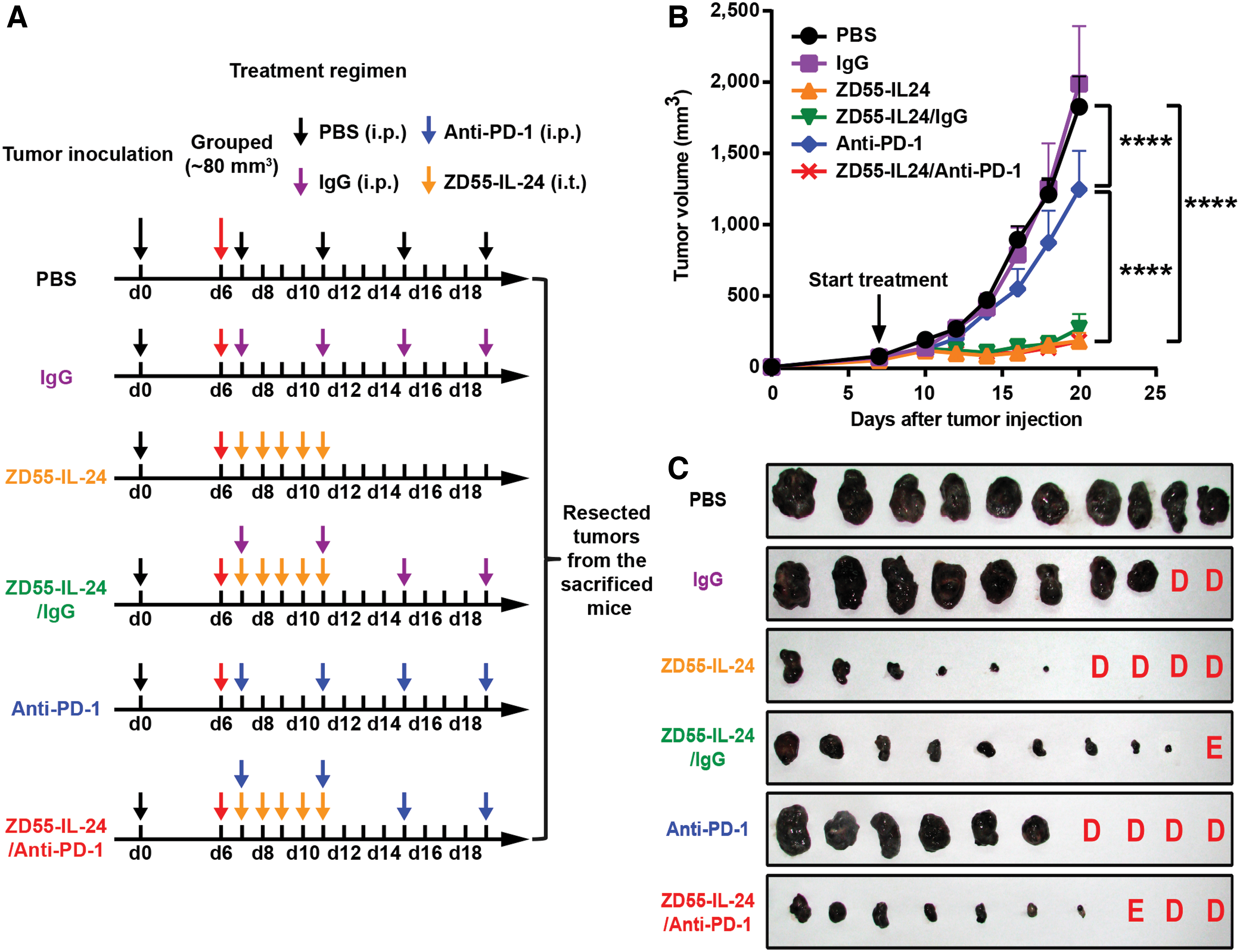
There is no therapeutic synergy in combining short-term ZD55-IL-24 therapy with anti-PD-1 therapy in B16-bearing immunocompetent mouse model. B16-bearing C57BL/6 mice were treated with PBS, anti-PD-1 antibody, isotype IgG, ZD55-IL-24 (EDA5-50), or the combination via intraperitoneal or intratumoral injection as indicated, starting when the average tumor volume was about 80 mm3.
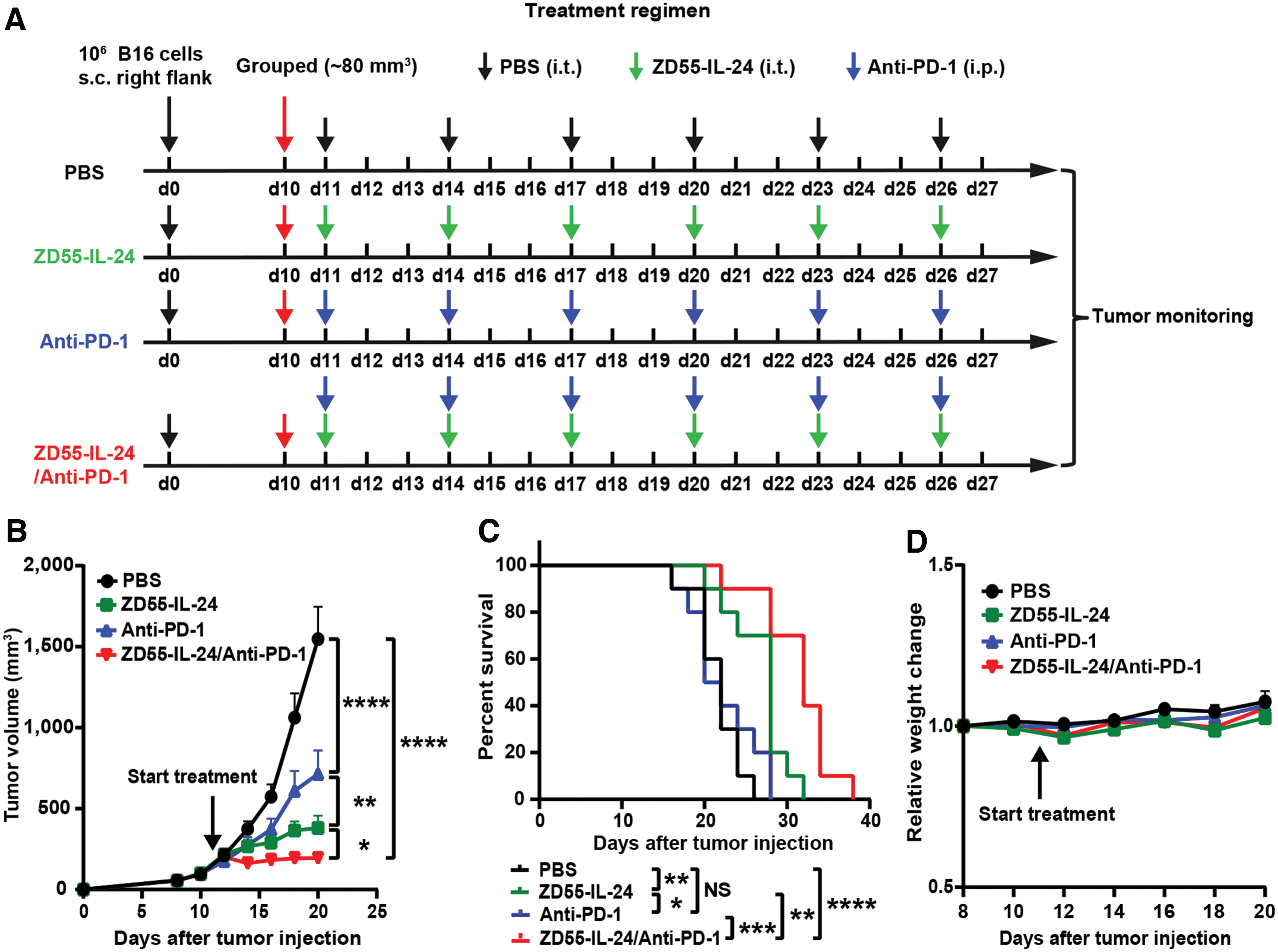
The sustained ZD55-IL-24 therapy can synergize with anti-PD-1 therapy to reject tumors in B16-bearing immunocompetent mouse model. B16-bearing C57BL/6 mice were treated with PBS, anti-PD-1 antibody, ZD55-IL-24 (ETDA-50), or the combination via intraperitoneal or intratumoral injection as indicated, starting when the average right tumor volume was about 80 mm3.
DISCUSSION
Oncolytic viruses represent a promising therapeutic platform for cancer. However, the optimal strategy for the administration of oncolytic viruses has not been established as yet. 9,10,15,21,36 –42 To this end, we attempt to optimize the administration strategy of ZD55-IL-24, which is an armed oncolytic adenovirus similar but superior to ONYX-015 in both A375-bearing immunocompromised mouse model and B16-bearing immunocompetent mouse model. We find that the antitumor efficacy of ZD55-IL-24 increases as injection times increase in A375-bearing immunocompromised mouse model. However, no obvious increase of antitumor efficacy is observed as the dose of each injection increases. In addition, we further find that the administration strategy of EODA-50 is superior to EDA5-50, which was utilized in our previous studies. Although the underlying antitumor mechanisms are quite different, the obtained results from B16-bearing immunocompetent mouse model are similar to that from A375-bearing immunocompromised mouse model. The antitumor efficacy of ZD55-IL-24 also increases as injection times increase, and increases only slightly as the dose of each injection increases in B16-bearing immunocompetent mouse model. The administration strategy of EODA-50 is superior to EDA5-50 in B16-bearing immunocompetent mouse model as well. Furthermore, our further results indicate that the tumor therapeutic effect of ZD55-IL-24 increases only slightly as the interval between two adjacent injections shortens in B16-bearing immunocompetent mouse model. Lastly, we find that ZD55-IL-24 is able to synergize with PD-1 blockade to reject tumors in B16-bearing immunocompetent mouse model when injected using the ETDA-50 administration strategy, whereas no significant synergy is observed between ZD55-IL-24 and anti-PD-1 antibody when ZD55-IL-24 is injected using the EDA5-50 administration strategy. These results indicate that the antitumor efficacy of ZD55-IL-24 can be further enhanced by administration strategy optimization.
Currently, ZD55-IL-24 can only be administered directly into tumors, making it difficult to be used to treat the vast majority of cancers in clinic, but particularly suitable for the tumors with visible lesions such as cutaneum carcinoma. As such, melanoma, which is the most aggressive type of cutaneum carcinoma is selected for the study. In addition, we find that ZD55-IL-24 not only exhibits pronounced antitumor efficacy in immunodeficient mouse model but also in immunocompetent mouse model, in our recent research. 26,27 However, the underlying mechanisms are quite different. The mechanism through which ZD55-IL-24 mediates tumor rejection in immunodeficient mouse model is mainly through the direct pathway of inducing tumor-selective cytotoxicity, whereas it is mainly through the indirect pathway of inducing systemic antitumor immunity in immunocompetent mouse model. This suggests that the results from immunocompromised mouse model might be quite different that from immunocompetent mouse model. Hence, we investigated in not only immunocompromised mice but also immunocompetent mice. Moreover, only the syngeneic murine tumor cells but not human tumor cells can establish tumor lesions in immunocompetent mice. Based on the above reasons, both A375-bearing immunocompromised and B16-bearing immunocompetent mice models were selected for the investigation in this study.
Not only do oncolytic viruses directly kill tumor cells at the end of their lytic cycle, they also produce and release a large number of progeny viruses, and the progeny viruses spread throughout a tumor, infecting other cancer cells and producing more progeny viruses. 15 Based on these characteristics, oncolytic viruses were originally thought to be effective in keeping sufficient amounts of viruses in tumors until tumors were eliminated, and only a tiny number of viral particles needed to be injected at the initial time of therapy. However, data from clinical trials showed that oncolytic viruses appeared to be short lived and would be gradually cleared by the antiviral immunity produced in patients, 11 suggesting that additional viruses needed to be periodically injected during the therapy period, otherwise the antitumor activity of oncolytic viruses might be decreased or even entirely lost as time went on. In our previous studies, ZD55-IL-24 was administered by the strategy of short-term injection (e.g., EDA5-50). 3,12 –14,25 We thus speculated that the past administration strategy used in our previous studies was unable to exert the maximal efficacy of ZD55-IL-24. Consistent with our hypothesis, we find that the administration strategy of sustained injection (e.g., EODA-50) is indeed superior to short-term injection (e.g., EDA5-50) in both immunocompetent and immunocompromised mouse model. We, therefore, conclude that the past administration strategy is suboptimal and the administration strategy of sustained injection is much better.
Cancer immunotherapy, which harnesses the host immune system to recognize and systemically eliminate both primary and metastatic tumor lesions by prompt immune surveillance and defense, is showing promise in treating patients with advanced or metastatic tumors. 43 A revolution has occurred in the field of cancer immunotherapy that was inspired by the initial invention of immune checkpoint inhibitors. 44 Antibody-based blockade of PD-1 are one of the most studied strategies for immune checkpoint inhibition. 45 Several antibodies against PD-1, such as nivolumab, have demonstrated encouraging antitumor effects in multiple clinical trials. 46 –48 Despite the exciting clinical results of anti-PD-1 antibodies for the treatment of tumors, the efficacy of the approach remains to be improved. There is a growing body of evidence to support combinatorial approaches that merge anti-PD-1 therapy with oncolytic virotherapy. 35,49 ZD55-IL-24 is an armed oncolytic adenovirus type 5 analogous but superior to ONYX-015 that has been evaluated in several clinical cancer trials but limited responses were reported, and clinical development was halted in 2003. 9 In this study, we demonstrate for the first time that only the sustained rather than the short-term ZD55-IL-24 therapy can synergize with PD-1 blockade therapy to reject tumor in B16-bearing immunocompetent mouse model, indicating that the therapeutic benefit of combining PD-1 blockade with ZD55-IL-24 is dependent on the sustained ZD55-IL-24 stimulation. These data may provide additional insights into the combination therapy of PD-1 blockade and ZD55-IL-24 in clinical practice.
Our study does present some limitations. For instance, it is well known that most murine tissues are not supportive of human adenovirus replication. Data obtained from mouse model are perhaps different from patients. This challenge, however, can only be addressed in clinical trials. Hence, further investigation in patients may yield important information. In addition, another limitation of this study is the lack of deep mechanical investigations. Further experiments will be needed to elaborate on the exact mechanisms underlying the observed phenotype. Nevertheless, this study provides a sound basis for the development of clinically applicable administration regimens for ZD55-IL-24 therapy.
CONCLUSION
In this study, we attempt to optimize the administration strategy of ZD55-IL-24 in both A375-bearing immunocompromised mouse model and B16-bearing immunocompetent mouse model. We find that the traditional administration strategy is suboptimal and the administration strategy of sustained injection is much better in both immunocompromised and immunocompetent mouse model. Our results confirm that the low-level limitation of antiviral immunity in tumor sites can indeed be overcome through administration strategy optimization, and thus further enhance the antitumor efficacy of ZD55-IL-24.
Footnotes
AUTHORS' CONTRIBUTIONS
H.-J.H. designed the studies with the help of X.-Y.L., generated most of the data along with X.L., and interpreted all the results. H.-Y.W., J.X., and J.-Q.H., helped perform animal experiments. H.-J.H. wrote the article and X.-Y.L. edited the article; H.-L.L. and J.-F.G. provided important advice for this study; A.-M.N. and L.-Y.S. provided ZD55-IL-24 and cell lines, respectively.
ACKNOWLEDGMENTS
The authors would like to thank professor Hong-Bin Ji and Wei-Guo Zou (Shanghai Institute of Biochemistry and Cell Biology, Shanghai Institutes for Biological Sciences, Chinese Academy of Sciences) for their helpful discussion.
AUTHOR DISCLOSURE
X.-Y.L., J.-F.G., and L.-Y.S. are inventors on a patent for the construction and application of ZD55-IL-24 (U.S. Patent and Trademark Office, 20090117643A1). The other authors declare no competing financial interests.
FUNDING INFORMATION
This work was supported by National Natural Science Foundation of China (81372453, 81572999, 31701220), Department of Science and Technology of Sichuan Province (2013ZZ0004), Shanghai Institutes for Biological Science, Chinese Academy of Sciences and Sichuan Huiyang Life Science and Technology Corp. Research Program (Y363S21763), and Grant from the Sino-American Joint Laboratory between Conba Group and Zhejiang Sci-Tech University.