
Abstract
One of the latest approved therapies for spinal muscular atrophy (SMA) is onasemnogene abeparvovec, which transduces motor neurons with the survival of motor neuron gene. The aim of this meta-analysis was to estimate the effect of onasemnogene abeparvovec on motor function in participants with type 1 SMA. Medline, Web of Science, Scopus, and Cochrane Library were searched for studies published from inception to August 2022. Pre-post clinical trials and observational studies determining the effect of onasemnogene abeparvovec on the Children's Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP-INTEND) score or motor milestones (i.e., head control, sit unassisted, feed orally, not use permanent ventilatory support, crawl, stand alone, and walk alone) in participants with type 1 SMA were included. Continuous outcomes (i.e., CHOP-INTEND score) were expressed as pre-post mean difference and 95% confidence interval (CI), while the proportion of participants who achieved >40, >50, and >58/60 points on the CHOP-INTEND and the achievement of the motor milestones were expressed as proportions and 95% CI. A random effects meta-analysis was conducted on each outcome, and the baseline CHOP-INTEND score was considered a covariate. Eleven studies were included in the systematic review, and four were included in the meta-analyses. Onasemnogene abeparvovec improved CHOP-INTEND scores by 11.06 (9.47 to 12.65) and 14.14 (12.42 to 15.86) points at 3 and 6 months postinfusion, respectively. Moreover, 87%, 51%, and 12% achieved CHOP-INTEND scores of >40, >50, and >58/60 points, respectively. However, this proportion increased to 100% in presymptomatic participants with greater baseline CHOP-INTEND. Motor milestones were also improved, especially in presymptomatic participants. Our systematic review not only showed a marked improvement in motor function in type 1 SMA but also showed that treatment in the presymptomatic stage improves the development of these children toward an evolution close to normal for their age.
INTRODUCTION
Spinal muscular atrophy (SMA) is a rare autosomal recessive disease usually caused by homozygous mutations in the survival motor neuron 1 gene (SMN1, location 5q13.2) and has an incidence of 1 per 6,000–10,000 live births. 1 –3 SMN1 encodes the SMN protein, which has an important role in cell homeostasis, spliceosome assembly, ribonucleoprotein biogenesis, cytoskeletal dynamics, and bioenergetic pathways. 4 The absence of SMN results in motor neuron death, causing hypotonia and progressive proximal weakness and bulbar and intercostal muscle involvement. In the medium term, respiratory failure, nutritional problems, scoliosis, hip dislocation, and thoracic deformities occur. 5 Upon suspicion of SMA, the diagnosis is made by genetic testing confirming a homozygous deletion of SMN1 exon 7.
Moreover, the number of copies of the homologous SMN2 gene (location 5q13.2) is determined, through which alternative splicing partially makes up for the SMN protein deficit by 10% per copy, modulating the SMA phenotype. 1,4 Thus, SMA type 1 is the most severe and common form of SMA (50% of cases), and children with SMA type 1 have 1, 2 and, in some cases, 3 copies of SMN2, 1,6 onset of symptoms before 6 months of age, and a life expectancy of <2 years without respiratory support. 7,8
Until recently, there were only palliative interventions in SMA type 1, such as physical therapy: nutritional, orthopedic, and respiratory interventions, as well as medication and vaccination to prevent respiratory complications. 9 However, the development of nusinersen substantially changed the prognosis of children with SMA. Nusinersen is an intrathecally administered antisense oligonucleotide that binds to intron 7 of SMN2 messenger RNA (mRNA), increasing SMN synthesis. 10,11 Another drug developed for SMA and targeting SMN2 is orally administered risdiplam, which is a small molecule that also promotes SMN2 exon 7 inclusion. 12,13
Finally, onasemnogene abeparvovec (Zolgensma®) is the first SMN gene replacement therapy. It uses a nonreplicating adeno-associated virus 9 (AAV9) containing a copy of the complete SMN gene under the control of a hybrid cytomegalovirus enhancer/chicken-β-actin promoter. Approved by the Food and Drug Administration and the European Medicines Agency, 14 onasemnogene abeparvovec is used in children with SMA under 2 years of age; its administration is intravenous in a single dose, with AAV9 crossing the blood–brain barrier, spreading throughout the central nervous system and transducing motor neurons with its genetic material starting to synthesize SMN. 15 –19
Because SMA is a rare disease and onasemnogene abeparvovec has only recently been developed, the available evidence on its efficacy and safety is limited. Therefore, this systematic review and meta-analysis aimed to synthesize the evidence and estimate the effect of onasemnogene abeparvovec on motor function and the most relevant motor milestones in participants with type 1 SMA.
METHODS
This systematic review and meta-analysis were conducted according to the Cochrane Collaboration Handbook 20 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 21 and it was previously registered in PROSPERO (registration number: CRD42022302224).
Search strategy
We systematically searched the Medline (using PubMed), Web of Science, Scopus, and Cochrane Library databases for data published from inception until August 2022. We also searched the gray literature, including the ClinicalTrials.gov, EudraCT, Google Scholar, OpenGrey, and Networked Digital Library of Theses and Dissertations databases. The search terms included zolgensma, onasemnogene abeparvovec, onasemnogene, abeparvovec, avxs-101, gene therapy, genetic therapy, spinal muscular atrophy, sma, trial, randomized clinical trial, randomised clinical trial, clinical trial, pre-post study, pre-post intervention*, observational, prospective, retrospective. The references of the included studies and previous reviews were also searched. When necessary, the authors of the studies were contacted. The search was carried out independently by two authors (C.P.-M. and I.C.-R.). Mendeley software was used as a reference manager. The complete search is described in Supplementary Appendix S1.
Inclusion/exclusion criteria
The inclusion criteria were as follows: (1) participants—children with type 1 SMA. When the study did not specify the SMA type but reported individual data according to the SMN2 copy number, participants with two copies of SMN2 were considered. Exceptionally, studies that included participants with two and three copies, the majority being those with two copies, although they did not separate the result for these. The exclusive study in SMA type 1 and the prioritization of participants with two copies of SMN2 was because they have an onset before 2 years of age, this being a requirement of the different drug agencies, some countries do not have it approved for children with SMA with more than three copies of SMN2, SMA type 1 is the most studied and, finally, the disparity in the number of copies of SMN2 copies would make it difficult to compare and interpret the results; (2) intervention—onasemnogene abeparvovec; (3) outcomes—primary outcome, including Children's Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP-INTEND) score. This outcome measures motor function and has a score from 0 to 64, with higher scores for those with better motor function, and is especially useful in nonsitters. 5,15 It was determined as the pre-post mean difference and as a proportion of participants who achieved values >40, >50, and >58/60. This last cutoff point (i.e., 58/60) was not strictly defined as a single value, as it was an ad hoc included outcome (see Modifications to the Initial Protocol section), and due to the great interest of this outcome, it was included as reported by each author or, exceptionally, according to the available data; and secondary outcomes, including the proportion of participants achieving major motor milestones (i.e., crawls, oral feeding, head control, not permanent ventilatory support, sitting >5 s, sitting >10 s, sitting >30 s, standing alone, walking alone); and the proportion of participants who had adverse events (i.e., drug-related adverse events, drug-related serious adverse events, elevated aminotransferases, severe elevated aminotransferases, elevated alanine transferases [ALT], severe elevated ALT, elevated aspartate aminotransferases [AST], severe elevated AST, abnormal coagulation, severe abnormal coagulation); and (4) design—randomized clinical trials, pre-post clinical trials with a single intervention arm, extension studies, and retrospective or prospective observational studies.
The exclusion criteria were as follows: (1) participants—the inclusion of participants with phenotypically milder SMA, without being able to separate them in the analyses; (2) design—single case study report.
The study selection was conducted independently by two reviewers (C.P.-M. and I.C.-R.), and disagreements were resolved by consensus or by a third reviewer (V.M.-V.).
Data extraction
An ad hoc table was performed with data extracted from the included studies, including (1) reference (author, year); (2) country/countries; (3) design, including trial registration number and the phase of the trial (if applicable); (4) participants (sample, age at infusion, CHOP-INTEND basal); (5) intervention (dose, length from infusion to assessment of outcomes); and (6) outcomes (CHOP-INTEND, motor milestones, safety profile).
Data extraction was conducted independently by two reviewers (C.P.-M. and I.C.-R.), and disagreements were resolved by consensus or by a third reviewer (V.M.-V.).
Risk of bias assessment
We assessed the risk of bias using the Quality Assessment Tool for Before-After (Pre-Post) Studies with No Control Group from the United States National Institutes of Health National Heart, Lung, and Blood Institute. 22 This tool consists of 12 items that assess the study design, the statistical analysis used, and the development of the intervention. Finally, a quality rating is given, which can be good, fair, or poor. If the rating is poor, an explanation should be given.
The risk of bias assessment was conducted independently by two reviewers (C.P.-M. and I.C.-R.), and disagreements were resolved by consensus or by a third reviewer (V.M.-V.).
Data synthesis
An ad hoc table synthesizing the results of the included studies was performed. Whenever possible, the estimates made by the authors of each study were considered. When this was not possible, but individual participant data were available, we calculated the effect of the drug on the corresponding outcome using a paired t-test. Continuous outcomes were estimated as a mean difference and 95% confidence interval (95% CI), specifying (if possible) the month of evaluation (3 or 6 months postinfusion), while dichotomous outcomes were estimated as the proportion of participants (and 95% CI) who achieved the proposed CHOP-INTEND cutoffs (i.e., 40, 50, and 58/60), the motor milestone, or had the adverse event.
Random effects meta-analyses 23 were performed, including clinical trials for each outcome and displayed using forest plots. Observational studies were excluded from the meta-analyses to homogenize the baseline characteristics of the participants of the studies included in the meta-analyses as much as possible (e.g., age at infusion), as well as to avoid the limitations of observational studies and, perhaps, the overlap of some participants of clinical trials in some observational studies. The I 2 statistic was used to assess heterogeneity. It was considered not important if <30%, moderate if 30–50%, substantial if 50–75%, and considerable if >75%. The p-value was also considered. When the I 2 statistic could not be obtained, a visual inspection was performed. 20 Finally, a sensitivity analysis and a publication bias assessment were performed using the Egger test 24 for the CHOP-INTEND mean difference outcome at 3 and 6 months postinfusion, and publication bias was considered if p > 0.10.
Statistical analyses were performed with STATA SE software, version 15. For dichotomous variables, the statistical package metaprop was used.
Modifications to the initial protocol
Initially, the protocol did not include the proportion of participants who reached the proposed CHOP-INTEND values. However, the last published trial forced inclusion of this outcome. Not only the pre-post difference matters but also the proportion of participants who achieve greater improvements with respect to the natural history of the disease and, especially, according to the stage of the disease. We also decided to include studies that included the combination of onasemnogene abeparvovec with nusinersen or risdiplam to see if it offered additional benefit. Finally, since our study mainly focused on the efficacy of onasemnogene abeparvovec, we decided to exclude outcomes from the safety profile of observational studies.
RESULTS
Of the 785 records identified, 11 studies were included in the systematic review (Table 1), 25 –35 4 were included in the meta-analysis, 25 –28 6 were excluded for not having a design of interest, and 1 was excluded for not including outcomes of interest (Supplementary Table S1 and Supplementary Fig. S1).
Baseline characteristics of the participants in the included studies
Dose determined as vector genomes (vg) per kilogram (kg) of weight.
Length determined as the mean time between drug infusion and the last evaluation.
CHOP-INTEND, Children's Hospital of Philadelphia Infant Test of Neuromuscular Disorders; NA, not available/not applicable; TN, age at nusinersen infusion; TOA, age at onasemnogene abeparvovec infusion.
All were studies of onasemnogene abeparvovec as the main treatment, except in two studies, 31,34 in which nusinersen was administered first and later onasemnogene abeparvovec (except in one participant who received onasemnogene abeparvovec first). However, most observational studies included participants previously treated with nusinersen. Seven studies included participants from the United States, 25,26,28,29,32,33,35 three from Europe, 27,28,34 two from Asia, 28,31 and one from Oceania. 30 The sample size, excluding the extension studies, was 129 participants, of which 81 belonged to clinical trials and, therefore, were included in the meta-analyses. The age at onasemnogene abeparvovec infusion ranged from 0.7 to 4.1 months in clinical trials and from 9.7 to 14.6 months in retrospective observational studies. The dosage of onasemnogene abeparvovec ranged from 1.1 × 1014 to 2.0 × 1014 vector genomes per kilogram (vg/kg). All studies reported the CHOP-INTEND, some motor milestones, and, in clinical trials, the safety profile.
The baseline characteristics of the participants are shown in Table 1, the distribution of participants in each study according to the number of copies of SMN2 and the use of other gene therapies are detailed in Supplementary Table S2, the definition of the adverse events in Supplementary Table S3, the classifications of permanent use of ventilatory support and oral feeding in Supplementary Table S4, and the protocol for the use of glucocorticoids (prednisolone) in Supplementary Table S5.
Systematic review
Tables 2 and 3 summarized the effect of onasemnogene abeparvovec on CHOP-INTEND, Supplementary Table S6 on the major motor milestones, Supplementary Table S7 the age at which the relevant motor milestones were achieved, and Supplementary Table S8 on the safety profile.
Efficacy of onasemnogene abeparvovec in Children's Hospital of Philadelphia Infant Test of Neuromuscular Disorders
For all participants (2 + 3 SMN2 copies).
TN, age at nusinersen infusion; TOA, age at onasemnogene abeparvovec infusion.
Proportion of participants who achieved the cutoffs proposed in the Children's Hospital of Philadelphia Infant Test of Neuromuscular Disorders
In clinical trials, CHOP-INTEND increased significantly at 3 and 6 months by ∼12 and 14 points, respectively, independent of baseline CHOP-INTEND. However, in presymptomatic participants, 28 all participants achieved a CHOP-INTEND score >58/60. Furthermore, >50% of participants were able to feed orally, have head control, and sit for >30 s in the trials. These milestones were more pronounced in the study in the presymptomatic population, with a proportion of 0.71 who were able to walk alone. Moreover, in these latter participants, the motor milestones were achieved before. Conversely, extension studies 29,32 showed that motor milestones were maintained in the long term, while observational studies also showed increases in CHOP-INTEND and a good response in motor milestones. Finally, adverse events were common, with an increase in transaminases in ∼≈20% of participants.
Risk of bias assessment
According to the Quality Assessment Tool for Before-After (Pre-Post) Studies With No Control Group from the United States National Institutes of Health National Heart, Lung, and Blood Institute, 2 of 11 studies (18.2%) were rated as “fair” in the overall bias assessment, and the rest (81.8%) were rated as “good.” No study specified that the statistical assessor was blinded, and there were some concerns about sample size in some studies. The full risk of bias assessment is detailed in Supplementary Table S9.
Meta-analysis
The CHOP-INTEND score at 3 and 6 months postinfusion increased by 11.06 (9.47 to 12.65) and 14.14 (12.42 to 15.86), respectively. Moreover, the proportion of participants achieving CHOP-INTEND values >40, >50, and >58/60 was 0.87 (0.74 to 1.01), 0.51 (0.38 to 0.64), and 0.12 (0.04 to 0.21), respectively (Fig. 1). The proportion of participants achieving motor milestones was as follows: the ability to crawl and stand alone was 0.04 (−0.01 to 0.09); oral feeding was 0.74 (0.58 to 0.91), maintaining head control was 0.85 (0.76 to 0.93), the ability to sit independently for more than 10 and 30 s was 0.63 (0.42 to 0.85) and 0.60 (0.45 to 0.76), not using permanent ventilatory support was 0.96 (0.90 to 1.01), and walking alone was 0.20 (0.02 to 0.39) (Supplementary Fig. S2).
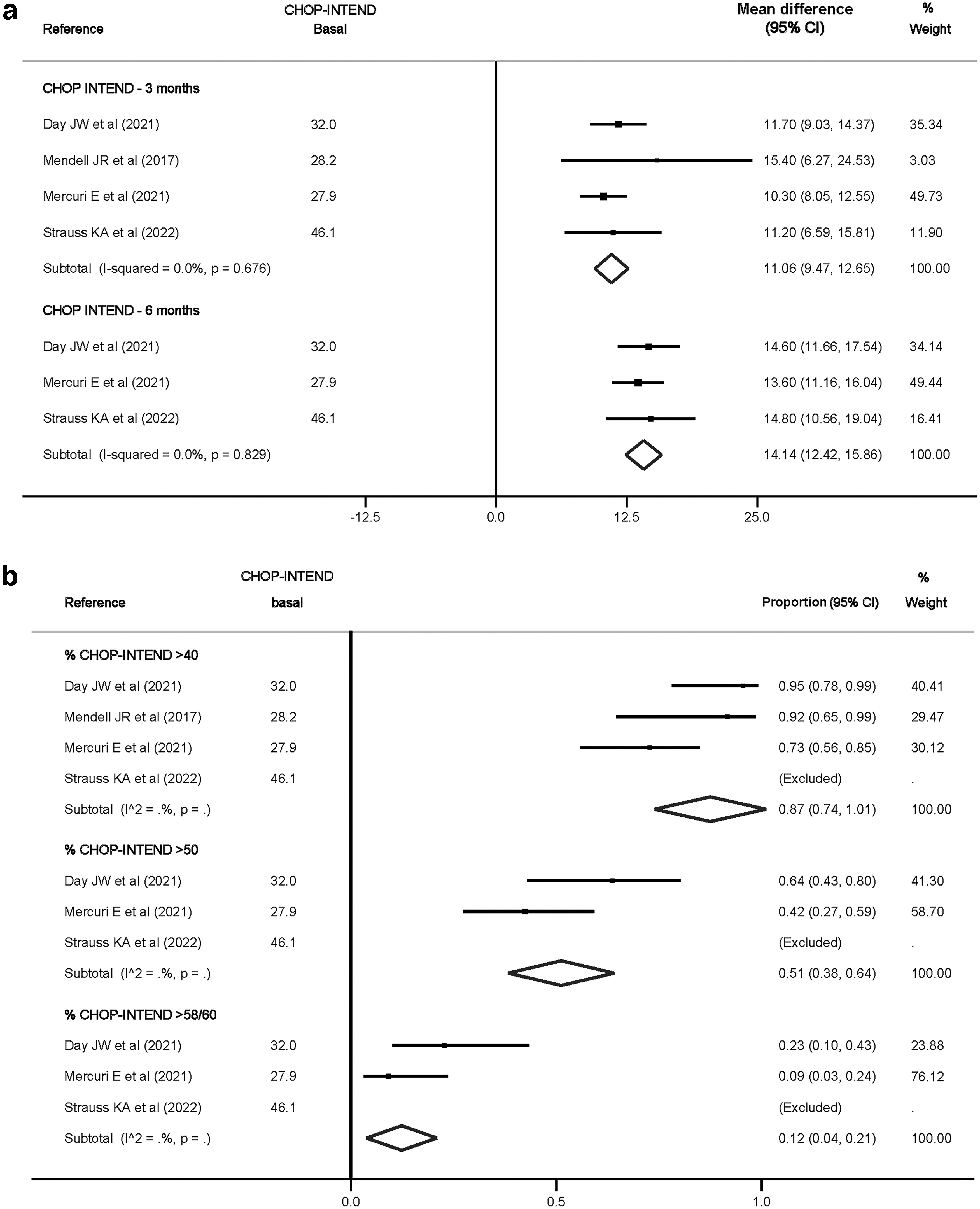
Pooled estimates of the effect of onasemnogene abeparvovec on CHOP-INTEND at 3 and 6 months postinfusion in clinical trials, measured as pre-post mean difference and 95% confidence interval
Regarding the safety profile, the drug had a rate of adverse events of 0.57 (0.37 to 0.77); a rate of drug-related serious adverse events of 0.16 (0.06 to 0.26); a rate of elevated and severely elevated ALT of 0.16 (0.06 to 0.26) and 0.04 (−0.01 to 0.08), respectively; a rate of elevated AST and severely elevated AST of 0.21 (0.12 to 0.31) and 0.04 (−0.01 to 0.08), respectively; a rate of elevated transaminases and severely elevated transaminases of 0.16 (0.00 to 0.31) and 0.04 (−0.01 to 0.08), respectively; and a rate of abnormal coagulation of 0.04 (−0.01 to 0.08) (Supplementary Fig. S3).
Heterogeneity was not important in the CHOP-INTEND meta-analyses at 3 and 6 months. (I 2 = 0.0%, p = 0.676, and p = 0.829, respectively) (Fig. 1). However, for the events adverse and for the ability to walk alone, the heterogeneity was substantial and considerable (I 2 = 74.33, p = 0.01 and I 2 = 90.43, p = 0.00, respectively) (Supplementary Figs. S2 and S3), while in the rest of the outcomes, it could not be estimated, although visually, one study 28 had results that would be expected to increase heterogeneity for the proportion of participants who achieved CHOP-INTEND values >50 and >58/60 (Fig. 1).
Sensitivity analysis and publication bias assessment
Sensitivity analysis did not show that any study significantly affected the final estimation. Moreover, there was no publication bias in the CHOP-INTEND at 3 and 6 months postinfusion (p = 0.215 and p = 0.402, respectively) (Supplementary Fig. S4).
DISCUSSION
Main findings
This systematic review and meta-analysis provides an estimate of the effect of onasemnogene abeparvovec on key outcomes that are affected by type 1 SMA. Our results showed a statistically significant posttreatment improvement of 14 points in the CHOP-INTEND score at 6 months postinfusion, in addition to 87% of participants who achieved more than 40 points and 12% more than 58/60 points. Furthermore, this improvement appeared to be strongly associated with the stage of the disease at which the drug was administered, with a higher proportion of participants achieving the motor milestones studied and at a significantly younger age when administered at a presymptomatic stage. Finally, hepatic and coagulation disorders were frequent, requiring prophylactic treatment with corticosteroids and adaptation according to the evolution of the participants.
Interpretation
In natural history study cohorts, children with SMA with two copies of SMN2 have rapid decreases in CHOP-INTEND score, 36 estimated to be between 1.02 and 1.71 points/month, 37,38 which contrasts with the increases of 11 and 14 points at 3- and 6 months postinfusion of onasemnogene abeparvovec observed in our study. This increase in the CHOP-INTEND score was not dependent on their baseline values, at least in the ranges studied in the trials. However, interestingly, presymptomatically treated participants achieved maximal or near-maximal CHOP-INTEND scores, something that did not occur once SMA manifested. This is consistent with what was observed in participants with two copies of SMN2 treated presymptomatically with nusinersen in the NURTURE trial, 39 with 67% of participants reaching the maximum value of 64.
None of the motor milestones in our study had been previously observed in natural history study cohorts, including unaided sitting, crawling, standing, and walking, while head control was rarely achieved. Furthermore, at 20 months of age, only 8% of the children with SMA could live without respiratory support. 7,37,38,40 However, our study showed that a large proportion of participants achieved head control, oral feeding, unaided sitting, and no permanent use of ventilatory support, and 20% were even able to walk alone, with presymptomatically treated participants achieving the highest proportion, 71%, and with a development close to what would be expected in the healthy population. Moreover, these motor milestones seem to be maintained in the long term. 29,32
Although this was not the aim of this review, an interesting aspect of the trials in presymptomatic participants should be highlighted, which explains the motor improvement. Motor decline is associated with impaired compound muscle action potential (CMAP), a good indicator of disease status and progression. 38,41,42 Conversely, participants with two SMN2 copies in the SPR1NT and NURTURE trials increased peritoneal CMAP from 3.9 and 3.2 mV to 4.5 and ≈4.8 mV for onasemnogene abeparvovec and nusinersen, respectively. Thus, this stabilization or increase in CMAP correlates well with the improvement in motor function and motor milestones achieved. 39
Adverse events related to onasemnogene abeparvovec were frequent and sometimes serious and satisfactorily managed in trials, although there was one death in an observational study. 34 Approximately 15–20% of participants suffered alterations of aminotransferases, AST and ALT, and in 5% of participants, they had severe alterations. Although the incidence of adverse events could not be correlated with the dose or age of participants, a lower incidence of serious adverse events in younger participants cannot be ruled out. 28 These alterations were successfully treated with prednisolone, which can also increase the response to treatment by suppressing the antigen specific T-cell response that can clear the transduced cells and thus the loss of transgene expression. 26
A few mechanisms have been proposed to explain the adverse events. In addition to the alteration of baseline liver function in SMA, leading to possible steatosis and dyslipidemia, 43 the liver is one of the organs most transduced by the drug, which could cause hepatocellular damage due to inflammation, immune response with activation of Kupffer cells, and hepatocellular necrosis. 44 Moreover, transient coagulation abnormalities due to platelet depletion were observed in 5% of the participants. 45,46 The specific mechanism by which the drug increases the risk of these disorders is unknown, although it is likely that these participants have a baseline predisposition. 47
Our study has some implications. First, the main implication is probably the importance of early or asymptomatic detection of the disease, with the aim of starting treatment early and optimizing the benefits of therapy. Thus, neonatal screening for SMA would be of great importance, especially in countries that have approved gene therapies increasing the life expectancy and quality of life of these children. Although our study did not compare the efficacy of onasemnogene abeparvovec versus nusinersen, the high efficacy of both in presymptomatic participants is noteworthy. Second, children’ liver function should be carefully evaluated for the early detection of severe alterations in transaminase levels. 48 Moreover, after drug infusion, other drugs with hepatotoxic potential should be avoided. 49 Third, future trials or observational studies are needed to analyze the efficacy and safety of combining onasemnogene abeparvovec with other gene therapies, including nusinersen or risdiplam, since, in addition to potentially offering extra benefits, it cannot be ruled out that previous treatment with nusinersen or risdiplam may improve the efficacy of onasemnogene abeparvovec by improving the disease stage in symptomatic participants.
Limitations
Some limitations should be acknowledged. First, we included trials without a control group because the high a priori expectations of the drug made it unethical to include a control group. Second, the number of trials and participants was limited, leading to some uncertainty in the results. This was especially important in some observational studies, which included samples from very few participants. Third, the CHOP-INTEND cutoff point of 58/60 depended on the study and available data. Because it is not a concrete value, the estimates obtained should be considered with caution. Fourth, the limited number of participants might have led to overlooking some potentially severe adverse effects, such as thrombotic microangiopathy. 50 Fifth, observational studies were not included in our analyses because they had very few participants with type 1 SMA, and in addition, some participants might be represented in observational studies and clinical trials. Sixth, some children with SMA had previous treatment with nusinersen. This limitation was particularly important in the observational studies, with the inclusion of a significant number of participants previously treated with nusinersen, making interpretation of the results difficult. Seventh, when the authors did not separate the type of SMA but included the number of copies of SMN2, only participants with two copies were considered to have type 1 SMA. However, it cannot be ruled out that there were participants with type 1 SMA and three copies of SMN2. Eighth, some outcomes (e.g., use of permanent respiratory ventilation and oral feeding) were not homogeneously determined in the different included studies.
CONCLUSIONS
Onasemnogene abeparvovec, a drug recently approved in the United States and the European Union, is effective in improving the progression of type 1 SMA in terms of motor function and in almost all motor milestones that were previously never or rarely achieved. Moreover, this improvement depends on the stage of the disease at which the drug is administered, with presymptomatic participants obtaining the greatest benefits, reaching CHOP-INTEND values >60 in all or almost all participants, and reaching motor milestones such as walk alone in three out of four participants. Finally, onasemnogene abeparvovec caused adverse events in some participants, some of which were severe; however, they were successfully managed, and considering the severity of SMA, the adverse events could be considered tolerable.
DATA STATEMENT
The original contributions presented in the study are included in the article/Supplementary Data, and further inquiries can be directed to the corresponding author/s.
Footnotes
AUTHORs' CONTRIBUTIONS
Conceptualization: C.P.-M.; methodology: C.P.-M. and I.C.-R.; data curation and investigation: C.P.-M. and I.C.-R.; formal analysis: C.P.-M., M.L.-L.-T., I.M.-G., and E.R.-G.; validation and visualization: M.L.-L.-T., I.M.-G., and E.R.-G.; writing—original draft preparation: C.P.-M., I.C.-R., and V.M.-V.; writing—review and editing: all authors; supervision: I.C.-R. and V.M.-V.; funding acquisition: V.M.-V.; project administration: V.M.-V. All authors have read and agreed to the published version of the article.
AUTHOR DISCLOSURE
The authors have no conflicts of interest relevant to this article to disclose.
FUNDING INFORMATION
C.P.-M. is supported by a grant from the Universidad de Castilla-La Mancha (2018-CPUCLM-7939) and by the European Regional Development Fund. The funder/sponsor did not participate in the work.
SUPPLEMENTARY MATERIAL
Supplementary Appendix S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.