
Abstract
Dual-targeting chimeric antigen receptor (CAR)-T cell therapy has been proposed as a potential solution for overcoming antigen escape during anti-CD19 CAR-T treatment. We performed this systematic review and meta-analysis to investigate the efficacy and safety of this novel treatment in patients with B cell non-Hodgkin lymphoma (B-NHL) and B cell acute lymphoblastic leukemia (B-ALL). We systematically searched relevant literature based on databases (PubMed, Web of Science, Embase and Cochrane) and conference abstracts. The primary outcomes measured were the best objective response rate (ORR) or complete response (CR), 12-month overall survival (OS) and progression-free survival (PFS), cytokine release syndrome (CRS), and neurotoxicity. Fifteen registered prospective open-label clinical trials were included. Among the 260 patients with B-NHL, the pooled best ORR and CR were 77% (95% confidence interval [CI]: 0.71–0.82) and 52% (95% CI: 0.40–0.63), respectively, and the pooled 12-month PFS and OS were 54.0% (95% CI: 0.47–0.61) and 66.0% (95% CI: 0.56–0.77), respectively. In the 159 patients with B-ALL, the combined best CR was observed to be 92% (95% CI: 0.82–0.99) and the pooled 12-month PFS and OS were 65.0% (95% CI: 0.51–0.77) and 73.0% (95% CI: 0.56–0.92), respectively. Moreover, in B-NHL patients, grade ≥3 CRS was observed in 14.0% (95% CI: 0.04–0.29) of these patients, and 5.0% (95% CI: 0.02–0.08) showed grade ≥3 neurotoxicity; in the case of B-ALL patients, grade ≥3 CRS and neurotoxicity occurred in 11.0% (95% CI: 0.04–0.19) and 2.0% (95% CI: 0.00–0.06), respectively. This study demonstrates the safety and clinical efficacy of dual-targeting CAR-T cell therapies in B cell malignancies. Further, well-designed randomized controlled trials are required to establish the role of dual-targeting CAR-T cell therapy in patients with B cell malignancies.
INTRODUCTION
CD19-directed chimeric antigen receptor (CAR)-T cell therapies have revolutionized the treatment paradigm for hematological malignancies, especially in patients where the disease is considered untreatable. In particular, it has enabled a new standard of care for heavily pretreated patients with B cell acute lymphoblastic leukemia (B-ALL) and B cell non-Hodgkin lymphoma (B-NHL). Despite a high complete response (CR) rate of up to 90% observed in relapsed/refractory (r/r) B-ALL, ∼50% of patients, who had received CD19 CAR-T treatment and achieved CR, relapsed within 1 year. 1 Among patients with r/r B-NHL, less than half generally achieved CR after CAR-T cell therapy, and long-term progression-free survival (PFS) ranged from 30% to 40%, suggesting that the majority of patients experienced treatment failure or relapse shortly after response. 2,3
Several potential resistance mechanisms of CD19 CAR-T cell therapies have been proposed, including tumor antigen loss, diminished function and insufficient persistence of CAR-T cells, and immunosuppressive microenvironment. Among these, the occurrence of CD19 antigen loss or downregulation has been observed in up to 25–50% of enrolled patients across clinical trials. 4,5 In patients with B-NHL, approximately one-third of relapses were accompanied by CD19 loss in tissue biopsy. 6,7 Thus, to improve the clinical efficacy of CAR-T cell therapy and reduce the likelihood of single-target loss-induced recurrence, a rational prophylaxis, which generates T cells that simultaneously target more than one B cell antigen, following a similar principle used in the well-established paradigm of multiagent combination chemotherapy regimens, is recommended. 8
Several strategies can be utilized to achieve dual-targeting, including sequential or simultaneous administration of two CAR-T cell products, cotransduction of T cells with two separate CAR vectors, tandem or bivalent CAR constructs, and bicistronic products; each has its strengths and weaknesses, and the optimal approach is yet to be defined. 8 –11
The efficacy of dual-targeting CAR-T cell therapy in B cell malignancies has been increasingly investigated in clinical studies, and a range of response rates have been achieved. 12 –15 Whether dual-targeting may overcome the limitation of CD19−relapse remains unclear, with clinical studies supporting or opposing the effectiveness of dual-targeting on antigen downregulation. 13,15 The study performed by Wang et al., in which the clinical efficacy of CD19 single-targeted and CD19/CD22 bispecific CAR-T cell therapy in patients with B-ALL were compared, demonstrated roughly equivalent remission and recurrence rates. 16 Moreover, the application of dual-targeting CAR-T cell therapies may be associated with some safety issues, including possible increased rates of adverse effects (AEs).
Although the putative effects of dual-targeting CAR-T cell therapies on B cell malignancies remain unclear, to the best of our knowledge, no attempt has been made to generate an evidence-based estimate of dual-targeting CAR-T cell therapies in B cell malignancies. Thus, in this study, we performed a systematic review and meta-analysis to summarize the overall efficacy and safety of dual-targeting CAR-T cell therapies in B cell malignancies, with the aim of guiding clinical practice of this novel treatment.
METHODS
Literature search
A systematic search of Cochrane Central Register of Controlled Trials, PubMed, Web of Science (Clarivate Analytics), and Embase was performed to identify potentially relevant clinical studies using the following searching strategy: “bispecific” or “tandem” or “dual targeting” or “bicistronic” or “co-transduction” or “sequential” or “co-administration” or “cocktail” AND “chimeric antigen receptor” or “CAR” AND “leukemia” or “lymphoma.” Additional records were retrieved by screening published conference abstracts reported by the American Society of Hematology (ASH), American Society of Clinical Oncology (ASCO), European Group for Blood and Marrow Transplantation (EBMT), and European Hematology Association (EHA). In addition, a manual search of the reference lists of all retrieved articles and abstracts from recent conferences was performed.
All records from January 2001 to May 2022 were included. When the same or overlapping cohort of patients was included in more than one publication, only the most recent or most informative report was selected for the analysis. This study was not registered on PROSPERO, but was performed in accordance with the Declaration of Helsinki with prior approval of the Institutional Review Board and the Ethics Committee from each hospital. The study followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline.
Study selection
Patient data were extracted solely from these publications, and no requests for additional original patient data were made to the authors of these studies. Data were not collected from reviews and nonscientific publications to avoid data duplication, but these sources were used to ensure accurate and appropriate data selection. Two reviewers (M.Y. and Q.Z.) independently screened all the abstracts to determine whether the studies likely met the inclusion criteria. Differences were resolved by discussion and, if necessary, by a third investigator (F.K.).
Studies were considered eligible if they met the following criteria: (1) the design was a prospective clinical trial that was registered on
The following studies were excluded from this study: (1) if the study design was retrospective or nonregistered study; (2) preclinical in vitro or animal studies; (3) case reports or case series; (4) trials testing single-target CD20 or CD22 CAR-T in patients who had a failed previous CD19 CAR-T cell therapy; (5) reviews and meta-analysis; and (6) non-English publications.
Data extraction and quality assessment
To ensure homogeneity in data gathering and entry, data extraction was performed by two experienced investigators (M.Y. and Q.Z.) independently. A third-party investigator (F.K.) was called upon to resolve any differences, and a complete consensus was reached for all of the main variables assessed in the analysis.
The following information was collected: name of the first author, year of publication, clinical trial number, CAR-T type, country, disease type, sample size, age, costimulation, transduction method, T cell origin, previous CAR exposure, previous transplantation, CAR-T dosage, follow-up, toxicity grading criteria and study outcomes such as response rates (best ORR or CR) within 3 months, survival (6-, 12-, 18-, and 24-month PFS and OS rates), antigen loss or downregulation rate, and safety outcomes (any grade CRS, grade ≥3 CRS events, any grade neurotoxicity events, and grade ≥3 neurotoxicity events). Quality assessment was performed using the Methodological Index for Nonrandomized Studies (MINORS) tool designed for interventional single-arm studies.
Statistical analysis
Meta-analysis was performed using Stata 16.0 (StataCorp;
Heterogeneity was determined using forest plots and the I 2 index. Subgroup analyses were performed to evaluate the effect of target combination and dual-targeting modality on the following outcomes, including the response rates, 12-month OS, CD19− relapse rate, grade ≥3 CRS, and neurotoxicity. We performed narrative synthesis when meta-analysis was not possible. The primary outcomes were the response rates, 12-month OS, grade ≥3 CRS, and neurotoxicity. Sensitivity analyses were performed by excluding trials that potentially biased the results of primary outcomes. A trim and fill analysis was performed to identify and correct the asymmetry of the funnel figure caused by publication bias.
RESULTS
Identification of eligible studies
The initial search yielded 1,128 records. After removing the duplicates, 469 records were excluded after screening titles and abstracts and reviewing full-text articles, mainly because they were reviews, letters, comments, or studies irrelevant to our analysis, leaving 148 that appeared to meet our selection criteria. Out of the 148 records, 133 were excluded based on the inclusion criteria of the present study—which included 31 records because of study design or aim; 30 were preclinical studies; 15 were case reports or case series; 14 were unregistered studies; 17 were reviews; 8 were duplicate publications; 12 were non-English studies; and 6 were reports that did not have the data of interest. Finally, 15 prospective articles that included 260 patients with B-NHL and 159 patients with B-ALL were included in the meta-analysis. 10,12 –15,18 –27 A detailed flowchart of the selection process was shown in Supplementary Fig. S1.
Baseline characteristics of included studies
All 15 studies, published between 2018 and 2022, were phase I–II, single-arm, noncomparative, prospective, and open-label clinical trials. The main basic characteristics of these studies were presented in Table 1. Ten studies were from China, three from the United States, and two from Europe. Most of the enrolled patients with B-NHL were middle-aged or elderly and had received multiple prior lines of treatment before infusion of CAR-T cells. In the cohort with B-ALL, pediatric or young patients were predominant. Forty-six patients with B-NHL had progressed after autologous or allogeneic (allo) hematopoietic stem cell transplantation (HSCT). Fifty-one patients with B-ALL had history of allogeneic-HSCT. There were 10 patients in the B-NHL and B-ALL cohort, respectively, who had previously received CAR-T therapies.
Baseline characteristics of included studies
Allo, allogeneic; ASTCT, the American Society for Transplantation and Cellular Therapy; Auto, autologous; CAR-T, chimeric antigen receptor T; ChiCTR, Chinese Clinical Trial Registry; CRS, cytokine release syndrome; CTCAE, the National Cancer Institute Common Terminology Criteria for Adverse Events version; FC, fludarabine+cyclophosphamide; Lee, Lee criteria; Penn, the Penn grading scale; r/r B-ALL, relapsed/refractory B cell acute lymphoblastic leukemia; r/r B-NHL, relapsed/refractory B cell non-Hodgkin lymphoma.
The target combination of CD19 and CD22 was the mainstay in most clinical trials, whereas three studies combined CD19 and CD20 targeting in patients with B-NHL. 13,24,25 In 10 studies, bispecific CAR was constructed in 1 vector, and in 5 studies, dual-targeting was achieved by infusing mixed CAR-T cells, either simultaneously or sequentially. 10,15,22,25,26 In most studies, lymphodepletion was performed with fludarabine and cyclophosphamide. Lentiviral transduction was the preferred transduction method, followed by retroviral application in three studies. 12,21,27 NCT04227015 was the only clinical trial to date, in which CRISPR/Cas9 technology was used. 23 The 4-1BB-based second-generation CAR construct was frequently used, along with other CAR-T cells with CD28 costimulatory domain alone or in combination with OX40 or 4-1BB. The origin of T cells in most studies was autologous, except for NCT04227015, where allogeneic T cells were used as bispecific CAR drivers. 23
Fourteen studies reported data about the grading of CRS and neurotoxicity. CRS scoring by the Lee system was applied in eight studies, followed by the National Cancer Institute Common Terminology Criteria for Adverse Events version (CTCAE), American Society for Transplantation and Cellular Therapy (ASTCT) and Penn. Neurotoxicity was assessed using CTCAE in eight studies, and the ASTCT scale in other studies. The follow-up duration ranged from 4.3 to 27.2 months. The quality assessment of included studies is presented in Supplementary Table S1 (MINORS), in which most trials scored 12–13 points.
Dual-targeting CAR-T treatment response rates
Eight studies reported response rates in B-NHL. 13 –15,18,20,21,24,25 Figure 1 illustrates forest plots of the best ORR and CR with 95% CI in the patients from the B-NHL group, with large B cell lymphoma (LBCL) as the main tumor type. The pooled ORR in our analysis was 77% (95% CI: 0.71–0.82, I 2 = 0.00%) without obvious heterogeneity (I 2 = 0.00%; p = 0.59). The pooled CR proportion was 52% (95% CI: 0.40–0.63) with substantial heterogeneity being detected (I 2 = 66.45%; p = 0.00). Nine studies involving 159 patients with B-ALL were available for the pooled efficacy assessment (Fig. 2). 10,12,14,15,19,22,23,26,27 Consistent with the remarkable response induced by single CD19 CAR-T, dual-targeting CAR-T cell therapy showed an impressive combined best CR up to 92% (95% CI: 0.82–0.99) in B-ALL. Significant heterogeneity was observed (I 2 = 59.92%; p = 0.01).

Forest plots of the best ORR and CR in B-NHL patients treated with dual-targeting CAR-T cells. B-NHL, B cell non-Hodgkin lymphoma; CAR-T, chimeric antigen receptor T; CI, confidence interval; CR, complete response; ORR, objective response rate.

Forest plot of the best CR in B-ALL patients treated with dual-targeting CAR-T cells. B-ALL, B cell acute lymphoblastic leukemia.
Survival after dual-targeting CAR-T treatment
In the B-NHL patient cohort, the pooled 6-, 12-, 18-, and 24-month OS values were 81.0% (95% CI: 0.73–0.90), 66.0% (95% CI: 0.56–0.77), 60.0% (95% CI: 0.47–0.78), and 55.0% (95% CI: 0.40–0.77), respectively. PFS rates at the above time points of 6, 12, 18, and 24 months were 62% (95% CI: 0.55–0.70), 54.0% (95% CI: 0.47–0.61), 54.0% (95% CI: 0.47–0.63), and 51.0% (95% CI: 0.43–0.61), respectively.
Among patients with B-ALL, the 6-, 12-, 18-, and 24-month OS values were 79.0% (95% CI: 0.74–0.91), 73.0% (95% CI: 0.56–0.92), 73% (95% CI: 0.47–0.88), and 47.0% (95% CI: 0.31–0.57), respectively, and the PFS rates at the above time points of 6, 12, 18, and 24 months were 68.0% (95% CI: 0.59–0.79), 65.0% (95% CI: 0.51–0.77), 64.0% (95% CI: 0.41–0.90), and 47.0% (95% CI: 0.28–0.90), respectively. The pooled OS and PFS rates at specific time points were aligned and shown in Fig. 3.
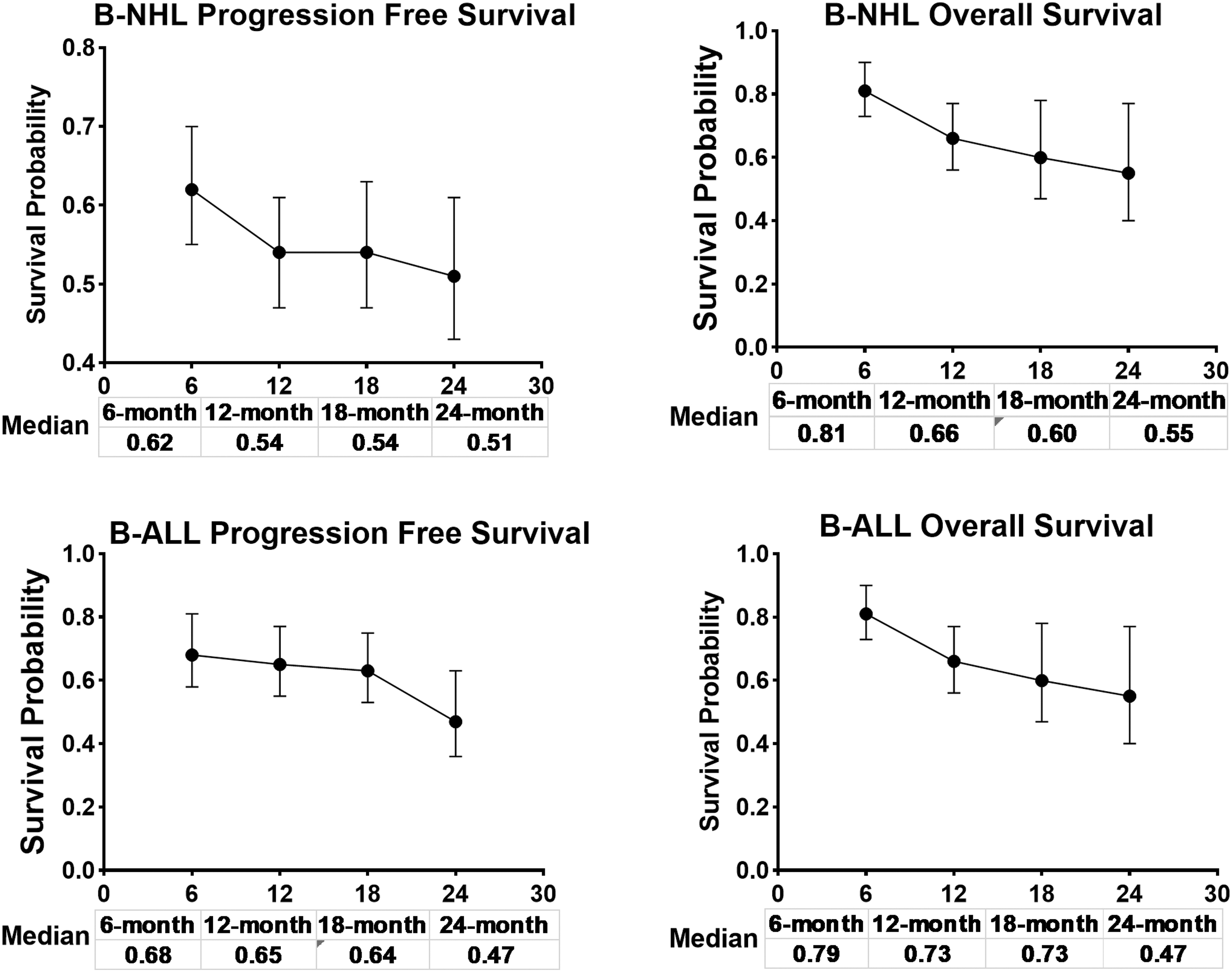
Tendency chart of PFS and OS rate in patients with B-NHL and B-ALL after treatment with dual-targeting CAR-T cells. OS, overall survival; PFS, progression-free survival.
CRS and neurotoxicity after dual-targeting CAR-T treatment
CRS and neurological toxicity are relatively unique AEs associated with CAR-T cell therapy, and they require specialized management. In the B-NHL cohort, 85.0% of (95% CI: 0.68–0.97, I 2 = 89.76%) 260 patients experienced CRS, with grade ≥3 CRS presented in 14.0% of these patients (95% CI: 0.04–0.29, I 2 = 85.78%). Neurotoxicity was present in 16.0% (95% CI: 0.09–0.26, I 2 = 65.51%) of B-NHL patients, while grade ≥3 neurotoxicity was observed in 5.0% (95% CI: 0.02–0.08, I 2 = 19.63%) of patients (Supplementary Fig. S2).
Among 160 patients with B-ALL, the pooled CRS and grade ≥3 CRS rates were 84% (95% CI: 0.64–0.98, I 2 = 83.98%) and 11.0% (95% CI: 0.04–0.19, I 2 = 38.73%), respectively. Neurotoxicity occurred in 10.0% (95% CI: 0.11–0.22, I 2 = 48.97%) of patients with B-ALL, while grade ≥3 neurotoxicity was observed in 2.0% (95% CI: 0.00–0.06, I 2 = 0.00%) of these patients (Supplementary Fig. S3).
Antigen loss or downregulation
The change in antigen expression in biopsy samples from B-NHL patients who failed from dual-targeting CAR-T treatment, was reported in five studies. 13 –15,20,24 Overall, 5 out of 48 (4%, 95% CI: 0.00–0.19, I 2 = 36.77%) patients with B-NHL showed CD19 loss at the time of progression (Supplementary Fig. S4A). Notably, Spiegel et al. reported 4 out of 14 patients relapsing with CD19 loss, with CD22 preserved. 14 Among 25 patients who had failed from CD19/CD20 bispecific CAR-T treatment, CD19 loss or downregulation was only detected in 1 case, with concurrent loss of CD20. 13,24 There was yet no clinical trial investigating CD19/CD20 dual-targeting combination in B-ALL, as the role of CD20 was not established in this type.
In the present meta-analysis of B-ALL cohort, the post-CAR antigen expression (CD19, CD22) patterns after relapses were available in eight studies. 10,12,14,15,19,22,23,26 Relapses with CD19 loss or downregulation were observed in 15 out of 59 (26%, 95% CI: 0.07–0.49, I 2 = 50.32%) patients (Supplementary Fig. S4B). Comparably, CD22 expression was relatively preserved, as the rate of CD22− relapse was only 12% (95% CI: 0.01–0.32, I 2 = 43.46%) among 58 patients (Supplementary Fig. S5).
Subgroup analyses, sensitivity analyses, and publication bias
Subgroup analyses stratifying by target combination and dual-targeting modality were performed. No significant differences were observed in treatment outcomes, including the best ORR/CR, 12-month OS, CD19− relapse, grade ≥3 CRS, and neurotoxicity (Supplementary Table S2). Each time a single study involved in the meta-analysis was deleted, the results of the meta-analysis remained insignificant with respect to all those primary outcomes, indicating that our study were roughly stable (Supplementary Fig. S6). Potential publication bias was assessed. The funnel plot did not show asymmetry. Therefore, there was no statistical evidence of publication bias for primary outcomes (Supplementary Fig. S7).
DISCUSSION
To the best of our knowledge, our study is the first meta-analysis that systematically aggregated data on dual-targeting CAR-T cell therapy outcomes. Our results indicated an impressive clinical efficacy and an acceptable safety profile for this novel treatment in r/r B cell malignancies. This new class of therapy compares favorably with the treatment afforded by conventional CD19 targeting CAR-T cells and the infusion of dual-targeted CAR-T cells may represent a feasible and reliable solution in clinical practice.
In the treatment of B-NHL with LBCL as the main pathological subtype, our analysis revealed a remarkable efficacy of the dual-targeting CAR-T approach with a best ORR of 77% (95% CI: 0.71–0.82), and CR of 52% (95% CI: 0.40–0.62), similar to those observed with axicabtagene ciloleucel (axi-cel, yescarta) or lisocabtagene maraleucel (liso-cel) in ZUMA-1 and TRANSCEND NHL-001 trials. 3,28 Equivalent potency estimates were reported in real-world experience and recently published meta-analyses of the efficacy of single targeted treatment with CD19 CAR-T cells for B-NHL. 29 –31 In addition, the present meta-analysis showed a favorable long-term survival in these patients, with pooled 12- and 24-month OS values of 66% (95% CI: 0.56–0.77) and 55% (95% CI: 0.40–0.77).
The 12-month OS was similar to that of a single CD19 CAR-T treatment for LBCL, which showed a pooled 12-month OS of 63% (95% CI: 0.56–0.70). 30 The pooled 24-month OS was not inferior to an estimated 24-month OS of 50.5% in ZUMA-1—the pivotal trial for the U.S. Food and Drug Administration (FDA) approval of axi-cel in LBCL. 3 In the pre-CAR-T era, few patients with this disease could be cured, as demonstrated by the SCHOLAR-1 study, in which only 26% of patients with r/r LBCL achieved an objective response, with a median OS of 6.3 months with standard salvage therapies. 32 In B-ALL, meta-analyses with single anti-CD19 CAR-T cell therapy reported remarkable pooling CR rates of ∼80%, with a 12-month OS of 57%. 33,34
Our results showed promising dual-targeting CAR-T cell therapy effectiveness, with a pooled best CR of 92%. In the survival analysis, the pooled 12-month OS was 79% (95% CI: 0.74–0.91) and 47% (95% CI: 0.31–0.57) at 24 months. In naive comparisons, the dual-targeting CAR approach showed comparable or favorable outcomes relative to CD19 single-targeted CAR-T treatment, nonetheless, we could not thus claim that dual-targeting CAR-T can outperform or replace the approved CD19 CAR-T cell therapy, due to the infancy of dual-targeting CAR field and the insufficient rigorism of these indirect comparisons.
The loss of CD19 is one of the major reasons for relapse after CD19 CAR-T cell treatment. The phase II trial (ZUMA-1) of axi-cel reported that 3 of 11 B-NHL patients (27.2%) were CD19− at the time of disease progression; 35 samples obtained from 4 relapsed LBCL patients after tisagenlecleucel were analyzed, and one case (25%) had absent or low CD19. 36 The pooled CD19− relapse rate was 4% in this study, indicating their potential role in mitigating target antigen downregulation. However, the heterogeneity was extremely high—loss of the CD19 antigen was roughly not seen in B-NHL trials involving CD19/CD20 targeting, whereas 29% (4/14) of patients with LBCL were reported to relapse with low CD19 diseases in the phase I trial of a CD19/CD22 bispecific CAR by Spiegel et al., despite no significant difference was observed in the subgroup analysis stratifying by target combination.
It was hardly possible to determine whether the rate was reduced compared to those observed in CD19 CAR-T treatment. Notably, a high CR rate of 70% with an impressively high median PFS (27.6 months) was reported among 87 patients with B-NHL by Zhang et al. 24 All these patients were heavily pretreated and some had extremely high tumor burdens or aggressive diseases. One patient (8%) had a loss of CD19/CD20 dual antigens and no patient lost CD19 or CD20 only, suggesting that this bispecific CAR may improve clinical responses by mitigating antigen-negative recurrence. This construct was detectable for a long time. Besides, CD20 expression was preserved in LBCL tumor biopsies from patients who relapsed after anti-CD19 CAR-T cell therapy, regardless of prior exposure to rituximab. 37 These data, along with the previous findings, suggest that dual-targeting of CD19 and CD20 might be an appropriate combination to overcome antigen loss in B-NHL.
In B-ALL, CD19− relapse is also the predominant cause of relapses after CD19 CAR-T cell treatment, occurring in 25–42% of responding patients. 1,38 The rate of CD19− relapse in pediatric reports had been closer to 50%. 39 In the present study, 26% of 59 patients with B-ALL had unsuccessful dual-targeting CAR treatment due to CD19 loss or downregulation, giving rise to an impression that leukemia CD19 loss was not that effectively prevented. In parallel, CD22 loss was detected in blasts at relapse, but its expression was relatively preserved, as the relapse rate with CD22− disease (12%) was lower than that of CD19 (26%), suggesting significant immune pressure on the CD19 antigen and more limited immune pressure on the CD22 target.
These results suggested that they may more closely resemble the experience with single CD19-targeted CAR-T, highlighting the challenges of delivering equivalent potency across targets in the context of dual-specific CARs. It was worthy to note that analysis of relapsed patient samples revealed the lack of long-term CAR-T cell persistence in most trials with CD19/CD22 CARs, despite the 4-1BB costimulation was utilized. 12 –14,19 The underlying mechanisms remain elusive, whether transduction of more complex vectors impact T cell phenotype, increase CAR-T cell exhaustion, or facilitate immune rejection warrants close monitoring. Despite the truncated persistence and suboptimal CD22 targeting, dual-targeting CAR therapeutics had yielded promising clinical outcomes. On the one hand, the CD19 antigen recognition had not been compromised, and on the other hand, these patients were likely to benefit from the suboptimal, but effective CD22-redirected activity.
These studies highlighted the importance of enhancing potency against the CD22 antigen and improving CAR-T cell persistence to fully realize the potential of dual-targeting CAR-T cell therapy in future studies.
Preclinical studies have found that bispecific (bicistronic/tandem) CAR formed superior and stable immunological synapse structures and afforded better tumor clearance than cocktail infusions, suggesting that bispecific CARs may represent the preferred choice for dual-targeting CAR therapy. 40 Nevertheless, in the pooled analysis, dual-targeting using a bispecific CAR therapy did not show any tendency of increased antitumor activity in comparison with cocktail infusions, either in B-ALL or B-NHL. It might be, at least partly, imputed to be the abrogated persistence of the infused bispecific CAR-T cells. 12,14,19 CAR-T cells can be autologous or allogeneic. Allo-CARs from healthy donors hold promise for more accessible CAR-T cell therapy, but they are subject to allo-rejection or rapid elimination by the recipient's immune system, which might compromise their clinical activities. However, only one trial used allogeneic T cells as bispecific CAR drivers, precluding subgroup analysis by T cell origin. 23
To date, allo-CAR efficacy has yet to be optimized. Despite some encouraging data in this field, many issues remain to be addressed to maximize allo-CAR effectiveness for future clinical trials. 41 The structure and manufacturing technologies of CAR-T cells are also important determinants of CAR-T cell efficacy. Due to the limitations of the data, the species of single-chain variable fragment origin, the gene transfer method and the costimulatory domain were not further analyzed, which may overlook the vital influencing factors for dual-targeting CAR-T cell efficacy and safety. Larger scale clinical studies, particularly head-to-head controlled trials, are warranted to define the contributing factors in dual-targeting CAR-T cell therapy so as to optimize the structure and manufacturing of this novel treatment.
Safety was a focus of this novel therapy. Previous research has reported that dual-targeting CAR-T cells showed significantly higher cytokine secretion in vitro and in vivo compared to single-targeted CAR-T cells, which raised the concerns of possible increased severity of CRS and neurotoxicity, two most common but harmful AEs of interest. 42,43 In the present study, CRS was mild and transient in most cases, with 14% being grade ≥3 in B-NHL. Among these patients, 5% experienced grade ≥3 neurotoxicity. This safety profile was totally acceptable, in comparison to those observed with mono CD19 CAR-T cell therapies, which showed the incidences of grade ≥3 CRS ranging from 6% to 18%, grade ≥3 neurotoxicity ranging from 5% to 16% in B-NHL. 30,44 In B-ALL, the grade ≥3 CRS and neurotoxicity were 11% and 2%, respectively, which compared favorably with that of single-targeting CAR studies with B-ALL. 33,34
Although cross-study comparisons were difficult to interpret owing to diverse designs and different reporting scales, this safety profile should roughly mirror that of the single CD19 targeting CAR-T treatment for B cell malignancies.
Several limitations of our analysis should be considered when interpreting and extrapolating the results. First, current evidence on dual-targeting CAR-T cell therapy was still in the preliminary stages, with limited clinical studies restricted to relatively small, single-center, single-arm, first-in-human trials. The heterogeneity was high in most analyses, rendering the potential of over-generalizing the results despite the random effect model being used to measure outcomes. In this setting, it was difficult to obtain a clear estimate of this novel immunotherapy and make thorough cross-study comparisons with other treatment options. Second, baseline patient characteristics including age, sex, ECOG performance score, comorbidities, clinical stage, tumor burden, previous CAR-T exposure, and history of transplantation may play important roles in treatment responses.
However, the data were limited and most trials did not report data according to prognostic subgroups, making it difficult to determine the factors potentially affecting treatment outcomes. Third, the present study was not previously registered. However, it was conducted totally according to the PRISMA guidelines, which helped to guarantee the reliability of our meta-analysis. Fourth, when OS and PFS were not provided in included studies, we extracted data through Engauge Digitizer software, which can inevitably lead to some error. In addition, various grading guidelines were used for CAR-T cell-related CRS and neurotoxicity and some safety issues affecting the universal application of CAR-T were not discussed, including febrile neutropenia, hematological toxicities, infections, hypogammaglobulinemia, and B cell aplasia.
Finally, a possible limitation is the language bias, some articles published in Chinese or other non-English languages may not have appeared in international journal databases and could have been missed by our searches. Despite these limitations, our study provided an up-to-date comprehensive overview of the feasibility and safety of dual-targeting CAR-T cell therapy in patients with r/r B cell malignancies.
CONCLUSION
In conclusion, our results showed that dual-targeting CAR-T cell therapy is relatively safe and effective, and potentially yields durable responses in a subset of patients with r/r B cell malignancies. Further, well-designed multicenter trials with longer follow-up intervals are required to establish the role of dual-targeting CAR-T cell therapy in patients with r/r B cell malignancies.
DATA AVAILABILITY STATEMENT
The datasets generated for this study are available on request to the corresponding author.
Footnotes
AUTHORs' CONTRIBUTIONS
M.Y. and Q.Z. conceived and designed the experiments. Q.Z. and F.K. analyzed the data. M.Y. and F.L. wrote the article. M.Y., Q.Z., Y.P., and L.Q. performed the literature search and the data extraction. F.L., L.G.Q., and J.W. supervised the report and the publication process. All authors contributed to the article and approved the final version of the article.
AUTHOR DISCLOSURE
The authors declared that they have no competing of interests.
FUNDING INFORMATION
This study was supported by the National Natural Science Foundation of China (81960041, 81960043), the Natural Science Foundation of Jiangxi Province (20192BAB215035, 20192ACB20030), the Cooperation Project of Science and Technology plan of Jiangxi Province (20212BDH80024), the Science and Technology Innovation Foundation of Jiangxi Province (20211ZDG02006), and the Clinical Medical Research Center of Jiangxi Province (20212BCG74001).
SUPPLEMENTARY MATERIAL
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.