
Abstract
The liver is a prime target for in vivo gene therapies using recombinant adeno-associated viral vectors. Multiple clinical trials have been undertaken for this target in the past 15 years; however, we are still to see market approval of the first liver-targeted adeno-associated virus (AAV)–based gene therapy. Inefficient expression of the therapeutic transgene, vector-induced liver toxicity and capsid, and/or transgene-mediated immune responses reported at high vector doses are the main challenges to date. One of the contributing factors to the insufficient clinical outcomes, despite highly encouraging preclinical data, is the lack of robust, biologically and clinically predictive preclinical models. To this end, this study reports findings of a functional evaluation of 6 AAV vectors in 12 preclinical models of the human liver, with the aim to uncover which combination of models is the most relevant for the identification of AAV capsid variant for safe and efficient transgene delivery to primary human hepatocytes. The results, generated by studies in models ranging from immortalized cells, iPSC-derived and primary hepatocytes, and primary human hepatic organoids to in vivo models, increased our understanding of the strengths and weaknesses of each system. This should allow the development of novel gene therapies targeting the human liver.
INTRODUCTION
Recombinant adeno-associated viral (rAAV) vectors are versatile delivery tools composed of a single-stranded DNA genome flanked by 145-bp inverted terminal repeats, packaged within an icosahedral protein capsid. The adeno-associated virus (AAV), from which this vector system was derived, is a nonpathogenic helper-dependent parvovirus with multiple naturally occurring serotypes, including the prototypical serotype 2 (AAV2). 1,2 AAV2 was the first variant to be vectorized and is the best understood serotype, still used in many studies to date. 3,4 The structure and amino acid sequence of the nonenveloped AAV capsid is the main determinant of tropism. 5 Therefore, modifying the viral capsid has been used as a strategy to target specific cell types and organs for therapeutic applications. 6
Clinical success of gene therapy trials using AAV vectors has led to the authorization of products for three indications to date: RPE65-associated retinal dystrophy (AAV2 capsid; Luxturna™), 7 spinal muscular atrophy (AAV9 capsid; Zolgensma™), 8 and lipoprotein lipase deficiency (AAV1 capsid, Glybera™; no longer available). 9 Although these AAV-based products target different organs (the eye, the central nervous system, or the muscles, respectively), therapies targeting disorders of other organs, such as the liver, have not reached market approval to date.
The liver is an important clinical target for gene therapies because of its key role in metabolism and homeostasis. Most of the experience in liver gene transfer using AAV vectors has been obtained in clinical trials for two coagulation disorders: hemophilia A and B. 10,11 Data from these trials have been encouraging and showed a relatively good safety profile. However, clinical studies conducted to date pointed out several challenges that need to be overcome to facilitate approval of therapeutic products for these diseases and expanding AAVs as therapeutics for other liver disorders. These challenges include the activation of the immune system following vector administration, unexpectedly low efficiency of targeting human hepatocytes in vivo, and liver toxicity associated with the administration of high vector doses. 12
The development of immune responses toward the therapeutic vector, resulting in the reduction of transgene expression, was first observed in a phase I/II study that utilized AAV2 to express Factor IX to treat hemophilia B. 13 AAV2 is endemic to the human population and thus many patients who could benefit from AAV2-based therapeutics have developed immunity to this serotype during their lifetimes, including six of seven patients enrolled in the first systemic clinical AAV2 study. Elevation of liver transaminases and CD8+ T cells against AAV were detected following vector administration through the hepatic artery. 13,14
Increase in Factor IX levels was only detected in two patients and it was transient, a striking contrast to data obtained in preclinical studies in mice and nonhuman primates (NHPs), which showed long-term transgene expression. 15 Although disappointing overall, the study confirmed the relative safety of rAAV-mediated liver gene transfer. 16 Critically, however, the activation of the immune system was not observed in any of the studies performed in animal models, highlighting the limitations of the model systems used to develop and validate new AAV therapeutics before clinical implementation.
Subsequent liver-targeted trials utilized other serotypes, such as AAV8 17 and AAV5, 18 both selected based on preclinical data in mice and NHPs. 19,20 In a pivotal trial sponsored by St. Jude Children's Research Hospital, a self-complementary AAV8 vector encoding Factor IX was administered to seronegative patients at three different doses. 21 Although long-term clinical efficacy was achieved, an early increase in liver transaminases was observed in the high-dose cohort. 22 Immune adverse events in liver clinical trials can generally be controlled by the administration of corticosteroids to prevent elimination of transduced cells and thus therapeutic transgene expression. Nevertheless, prevalence of neutralizing antibodies (NAbs) reduces the pool of patients that may be able to benefit from novel experimental therapies.
However, clinical studies suggest that anti-AAV5 antibodies do not preclude successful liver transduction with AAV5-based vectors. 23 This vector serotype has also been used to deliver Factor IX at relatively high vector doses (2 × 1013 vector genomes [vg]/kg) with no significant T cell–mediated inflammation, 24,25 although it must be considered that this serotype is also less efficient than others at transducing hepatocytes in animal models. 19
Despite these current limitations, it remains clear that vector serotype selection plays a crucial role in obtaining the desired clinical outcomes. AAV serotypes used in clinical studies are selected based on data generated in preclinical, frequently murine, models. However, clinical data obtained with AAV2, AAV5, and AAV8 clearly indicate that AAV liver tropism, which can be species specific, 20 can differ significantly between the murine or NHP preclinical models and human patients. 11
One way to overcome this issue has been using “humanized” models to functionally evaluate the existing AAV variants for their ability to transduce human hepatocytes in vivo. The same models can also be used to identify novel capsids with improved liver tropism. To this end, bioengineered capsids with high tropism toward human hepatocytes, such as AAV-LK0326 and AAV-NP59, 27 were developed in xenografted Fah-/-/Rag2-/-/Il2rg-/- (FRG) 28 mice demonstrating the validity of this approach. The shuffled capsid AAV-LK03, bearing high sequence similarity to the natural serotype AAV3b, 1,29 has been the first non-natural AAV to be used in clinical studies and led to stable therapeutic levels of Factor VIII expression in 16 of 18 hemophilia A patients. 30
Two patients treated at the highest dose in this study lost Factor VIII expression likely as a result of immune activation against the vector. 30 AAV-NP59, a highly functional variant selected in humanized FRG (hFRG), which differs from prototypical AAV2 at 11 amino acids only, 31 is yet to be tested in the clinic. Another interesting approach was recently published by the Asokan laboratory in the area of AAV capsid engineering for the central nervous system. 32 In this study, a cross-species compatible capsid was engineered by directed evolution in pigs, mice, and NHPs. The resulting capsid offers cross-species functionality as a result of the successive selection rounds that were performed in the three animal species.
The clinical progress is further affected by our inability to directly compare clinical data obtained from liver gene transfer studies using different AAV vectors not only owing to the differences imposed by the individual AAV variants used, but also owing to the lack of consistency regarding preclinical models used. Furthermore, vector manufacturing protocols, quantification methods, and transgene expression cassettes differ between the individual studies conducted to date. 33 Finally, patient-to-patient variability adds yet another level of complexity and “noise” in clinical data, making it very difficult to draw conclusions on how individual vector performance compares with one another.
The choice of the therapeutic cassette is dictated by the specific indication being targeted, and the patient-to-patient differences are impossible to overcome. However, the lack of consistency in the preclinical models used to select the rAAV variant needs to be addressed to determine critical decisions such as selection of the vector type and clinical vector dose. Advances in this respect will enable the successful development of novel effective and safe gene therapeutics.
With this in mind, we set out to compare AAV-based gene transfer efficiency targeting the liver in 12 frequently used preclinical models, including in vitro models, such as hepatic cell lines, human-induced pluripotent stem cell (hiPSC)–derived hepatocytes (iHeps), and adult stem cell–derived hepatic organoids. However, the focus was on ex vivo models, such as 2D and 3D primary NHP and human hepatocytes cultures, and in vivo models, including murine and human hepatocytes in xenograft mice and NHPs. To ensure the data obtained were not unique to the specific AAV variant used in the study, we performed the studies using six natural and bioengineered AAV variants, including four that have previously been utilized in liver-directed clinical studies.
Moreover, to increase quality and impact of the study by minimizing experimental noise, we used a well-characterized barcode approach, which allowed us to compare the individual vectors at the cell entry and transgene expression levels in parallel using next-generation sequencing (NGS) in each of the models. 34 –36 This study was aimed to understand the differences between the models and what will be required to address future preclinical translation. On top of the expected differences between the models in respect to their serological and immunological properties, we identified surprising differences between NHP and human hepatocytes that might explain some of lower-than-expected outcomes of clinical trials to date.
MATERIALS AND METHODS
Cell culture conditions and cell origins
AAV production and anti-AAV neutralization assays were performed in a human embryonic kidney (HEK) 293T cell line (Cat. No. CRL-3216; ATCC). HEK293T cells were cultured in Dulbecco's modified Eagle's medium (DMEM; Cat. No. 11965; Gibco) supplemented with 10% fetal bovine serum (FBS; Cat. No. F9423; Sigma-Aldrich), 1 × Pen Strep (Cat. No. 15070; Gibco), and 25 mM HEPES (Cat. No. 15630; Gibco). Human hepatocellular carcinoma 7 (HuH-7) and hepatocellular carcinoma HepG2 cells were provided by Dr Jerome Laurence (The University of Sydney) and Prof. Ian E. Alexander, respectively, and cultured in DMEM supplemented with 10% FBS, 1 × Pen Step, and 1 × nonessential amino acids (Cat. No. 11140; Gibco).
Cell transductions
Transductions were performed as previously published. 36,37 In brief, AAVs were added the indicated amount of rAAV capsid or vector mix to the cells, changing media after 6–8 h and harvesting cells for DNA/RNA or flow cytometry processing 72 h after rAAV exposure, unless otherwise specified.
Origin and culture of iHEP
Frozen iHeps (from ChiPSC18) were purchased at Takara Bio Europe AB, thawed, plated, and maintained according to the manufacturer's instructions in media included in the kit (Cat. No. Y10134; Cellartis Enhanced hiPS-HEP v2). In brief, 8.2 × 105 cells per well were thawed and seeded in a 24-well plate, exposed to AAVs after 5 days in culture, and harvested 7 days after exposure.
Primary human hepatocytes in 2D and 3D culture
Human (HUM4198; Lonza) and rhesus macaque (Cat. No. MKR103; Lonza) primary hepatocytes were used for 2D and 3D culture systems. For 2D culture, 24-well plates were coated with collagen for 45 min. After washing the coated wells with phosphate-buffered saline, primary hepatocytes were seeded 400,000 cells/well in complete hepatocyte plating media (HCM kit; Cat. No. CC-3198; Lonza). After 4 h of incubation at 37°C and 5% CO2, media were removed and gently covered with hepatocyte maintaining media (HCM kit; Cat. No. CC-3198; Lonza) containing 0.25 mg/mL Matrigel (Cat. No. 354234; Corning) and incubated at 37°C for 90 min. The AAV mix was added diluted in hepatocyte basal media (HBM; Cat. No. CC-3199; Lonza). Media were changed daily for 3 days, until harvest using Cell Recovery Solution (Cat. No. 354253; BD) and processing for NGS.
The 3D printed hydrogels containing human and rhesus hepatocytes were generated using a Rastrum Cell Printer (Inventia, Sydney, Australia). The cell printing followed the manufacturer's instructions and previously published protocols. 38,39 In brief, hepatocytes were thawed, resuspended in crosslinker solution (Inventia), and printed in 96-well plates at 8,000 cells/well. Cells were maintained in HBM and AAVs were added as described previously. Cells were harvested as whole printed gels and processed for NGS.
Primary human and simian hepatocytes engrafted into FRG mice
Cynomolgus and rhesus macaque primary hepatocytes were purchased from Lonza (Cat. No. MKC118 and Cat. No. MKR103). Human hepatocytes were also purchased from Lonza (Cat. No. HUM181971) and corresponded to a 15-month-old donor.
The engraftment procedure was performed as previously published. 28,40 Mouse studies were supported by the BioResources Core Facility at Children's Medical Research Institute. All animal care and experimental procedures were approved by the joint Children's Medical Research Institute and The Children's Hospital at Westmead Animal Care and Ethics Committee. The FRG mice were housed, treated, and killed following previously published methods. 40
Liver organoid transduction
Human liver organoids were generated as previously described 41 and used for research purposes with approval from the human ethics committee of School of Biosciences, University of Melbourne (Ethics No. 1851272). To carry out transduction with AAV, the Matrigel-supported planar infection method was adapted. 42 In brief, mature liver organoids embedded in Matrigel domes were isolated by dispersing Matrigel with cold basal media. After centrifugation, the medium was discarded, and the organoid pellet was suspended with expansion medium containing 10 μM Y-27632 (Cat. No. S1049; Selleckchem). The AAV cocktail was added to the medium at the described dose, and then the organoid–AAV mixture was transferred to a 24-well plate precoated with 80 μL of 75% Matrigel.
The organoid–AAV mixtures were incubated at 37°C with 5% CO2 for 12 h in a planar manner after which organoids on the Matrigel surface were collected, transferred to a tube, centrifuged, and supernatant discarded. The organoids were then washed with cold basal media followed by centrifugation. After the final wash and centrifugation, the organoids were returned to 3D culture by resuspending in Matrigel and seeding at 50 μL per well into 24-well plates. Once the Matrigel had set, 450 μL of expansion culture medium (Supplementary Table S1) was added and then replaced every other day for 7 days. To harvest, the organoids were suspended in cold basal media after the medium was discarded, pelleted by centrifugation, and then snap frozen until processing for DNA and RNA extraction. All centrifugations were carried out at 400 g at 4°C for 5 min.
Polymerase chain reaction
Standard and Illumina amplicon-seq NGS polymerase chain reactions (PCRs) were performed using Q5 (Cat. No. M0491; NEB), dNTPs (Cat. No. N0447; NEB), and primers (all Sigma-Aldrich; Supplementary Table S2) and were performed strictly following previously published protocols. 36
AAV production
All AAV capsids used in this study were produced using polyethylenimine transfection of the LSP-GFP-barcode (LSP-BC) transgene cassette, 31,37,43,44 as well as adenovirus and Rep2-Cap2/3/5/8/LK03/NP59 helper plasmids using previously described methods. 37 The resulting cell lysates and purified media were either purified using iodixanol gradients (all experiments apart from NHP) or CsCl ultracentrifugation (for NHP vectors) following the previously published protocols, respectively. 26,36 AAV titers were established using quantitative PCR and enhanced green fluorescent protein (eGFP) primers following previously published methods. 36,45 The capsids were then mixed at an equimolar ratio as previously described. 36
Neutralization assays
For experiments using the NHP, neutralization assays determining the anti-capsid antibodies for the different AAVs for all indicated timepoints were performed after the following protocol. At day 1, HEK293T cells were seeded into a 96-well plate at a density of 104 cells/well. At day 2, NHP sera were diluted in DMEM supplemented with 2% FBS in a total volume of 100 μL, beginning with a 1:5 dilution followed by dilution series of 1:3 and mixed with a dose of 104 vg/cell of the corresponding AAV serotype coding for luciferase that were incubated for 2 h at 37°C. The mix was subsequently used to transduce target cells. Each serum dilution was tested in duplicate.
Negative controls of nontransduced cells, as well as positive controls of cells transduced without AAVs not preincubated with NHP serum were included in each plate. The transduced cells were incubated for 48 h before quantification of luciferase activity was performed. Light emission from each well was measured in photons/s. The NAb titer was calculated using the highest dilution for which the percentage of light emission was 50% of positive control without serum. A 1:5 dilution of serum reducing the vector transduction by 50% or more was considered positive. The highest positive serum dilution determined the NAb titer.
For antibody determination in human serum samples, the assay was performed as previously described. 46 In brief, HuH-7 cells were incubated with heat-inactivated sera at dilution starting from 1:5, continuing in twofold serial dilutions to 1:1,280. The diluted serum samples were incubated for 1 h at 37°C with the individual AAV capsids diluted in an equal volume of DMEM. rAAV vectors were incubated at the same concentration to reach a predetermined final variant-dependent dose into a 100 μL final volume for transduction. The appropriate dose used was 6,000 vg/cell for AAV2, 2,000 vg/cell for AAV3, 40,000 vg/cell for AAV5, 25,000 vg/cell for AAV8, 2,000 vg/cell for AAV-LK03, and 4,000 vg/cell for AAV-NP59. Pooled human serum samples were used as a positive control.
Quantification of GFP-positive cells was performed by mean fluorescence using flow cytometry 72 h after rAAV exposure. A 1:5 dilution of serum reducing the vector transduction by 50% or more was considered positive. The highest positive serum dilution determined the NAb titer.
Human serum samples
Human serum samples from the Immunology laboratory, Great Ormond Street Hospital for Children NHS Foundation Trust, London, United Kingdom were anonymously analyzed following the guidelines of the Royal College of Pathologists.
NHP work
Animal procedures were approved by the ethical committee for animal testing of the University of Navarra and by the Department of Health of the government of Navarra (Comité de Etica para la Experimentación Animal code: 038/15) and performed according to the guidelines from the institutional ethics commission. Animal welfare checks were performed by animal care staff twice daily.
One young adult male Macaca fascicularis NHP was tested negative for anti-AAV NAbs for AAV2, AAV5, and AAV-LK03 and with low seropositivity against AAV3, AAV8, and AAV-NP59.
On day 0, the NHP was anesthetized, blood was drawn to obtain serum, and the animal was subjected to the immunoadsorption process (described in Salas et al. 47 ). Within the following 30 min after immunoadsorption, the vector was infused via the saphenous vein over 10 min. Blood was collected at 1 h, 24 h, and 7 days after administration of the vector. At day 7, the animal was killed, and different organs and tissues were collected for further analysis.
DNA and RNA extraction from cells and tissue samples
DNA and RNA were isolated from the cell pellets from the in vitro and ex vivo experiments using the AllPrep DNA/RNA Mini Kit (Cat. No. 80204; QIAGEN) following the manufacturer's instructions.
DNA from the mouse, NHP, and human hepatocytes from xenograft FRG mice and NHP tissues were isolated using phenol–chloroform extraction after proteinase K digestion following previously published protocols. 36 RNA from the mouse, NHP, and human hepatocytes from xenograft FRG mice and NHP tissues was extracted using the TriReagent (Cat. No. T9424; Sigma)–chloroform protocol previously published. 36,37
Reverse transcription of extracted RNA
Clean-up of extracted RNA was performed using TURBO DNase (Cat. No. AM1907; Invitrogen) twice for 1 h, followed by incubation with DNAse inactivation reagent following the manufacturer's instructions. The DNase-treated RNA was then used for cDNA synthesis using the SuperScript IV First-Strand Synthesis System (Cat. No. 18091050; Invitrogen) following the manufacturer's instructions using 2 μM of WPRE-binding primer (WPRE_R; Supplementary Table S2) to specifically synthesize the barcoded ssAAV-LSP-GFP-BC-WPRE cDNA.
Next-generation sequencing
The NGS amplicons were prepared and analyzed as previously published. 36,37
Normalization of NGS reads
NGS data obtained from all samples were normalized to the barcode contribution of the respective input (as indicated previously). Read counts for each sample and each variant were multiplied by the variant-specific “normalization coefficient” of the respective input, which was calculated as follows:
RESULTS AND DISCUSSION
Study design
To compare the performance of different AAV variants in preclinical models of the human liver, we created an equimolar mix of the following six AAV variants: AAV2, AAV3b, AAV5, AAV8, AAV-LK03, and AAV-NP59; encoding barcoded expression cassettes compatible with NGS-based readout at the cell entry (DNA) and transgene expression (RNA/cDNA) levels. 31,36,43 AAV2, AAV5, AAV8, and the bioengineered AAV-LK03 chosen as clinical data from liver-targeted human studies was publicly available. 11 AAV-NP59 and AAV3b were included because they were the bioengineered variant of AAV2 and the closest natural relative of AAV-LK03, respectively (Supplementary Fig. S1).
The mix of the six AAV candidates was used to transduce all different preclinical models evaluated in this study, whereas the individual AAV candidates underwent seroprevalence studies using individual human sera. The functional data obtained were compared with publicly available data on AAV performance in clinical trials as well as between the models to identify differences (Supplementary Fig. S1).
In vitro and ex vivo models of the human liver
The simplest models of human hepatocytes are based on cell lines derived from hepatocellular carcinoma, such as HuH-7, or hepatocellular blastoma, such as HepG2 cells. 48,49 These lines are immortalized and self-renewing, allowing for low-cost high-throughput experimentation using standard laboratory equipment and reagents. To evaluate both cell types for their potential to serve as biologically predictive models of human primary hepatocyte transduction, cells were transduced at a dose of 1,000 and 200 vg/cell and were harvested 72 h after AAV exposure.
Cell pellets were processed for DNA and RNA/cDNA, which allowed us to evaluate relative vector performance at the cell entry and transgene expression levels, respectively (Supplementary Fig. S2). The NGS results showed that AAV2 outperformed the other variants at the DNA and RNA levels in both HuH-7 and HepG2 cells. Of interest, whereas AAV-LK03 and AAV3b performed similarly at the cell entry level (DNA) in HuH-7 cells, AAV-LK03 outperformed AAV3b at the transgene expression level (RNA). In HepG2 cells, AAV-LK03 and AAV3b performed similarly but were less efficient at both DNA and RNA/cDNA levels than AAV5. The strong performance for AAV2 in those cell lines was expected based on data from HuH-7 cells we reported previously. 36
Next, we studied the six vectors in iHeps and adult stem cell–derived ductal organoids. It quickly became apparent that the transcriptional dominance of AAV2, as shown in the immortalized cell lines, did not fully translate to iHeps. AAV2 was still able to enter the cells at the highest efficiency at the DNA level, followed by AAV-LK03, AAV3b, AAV5, AAV-NP59, and AAV8 (Fig. 1b), but at the transgene expression level, AAV-LK03 outperformed all other vectors (Fig. 1c).
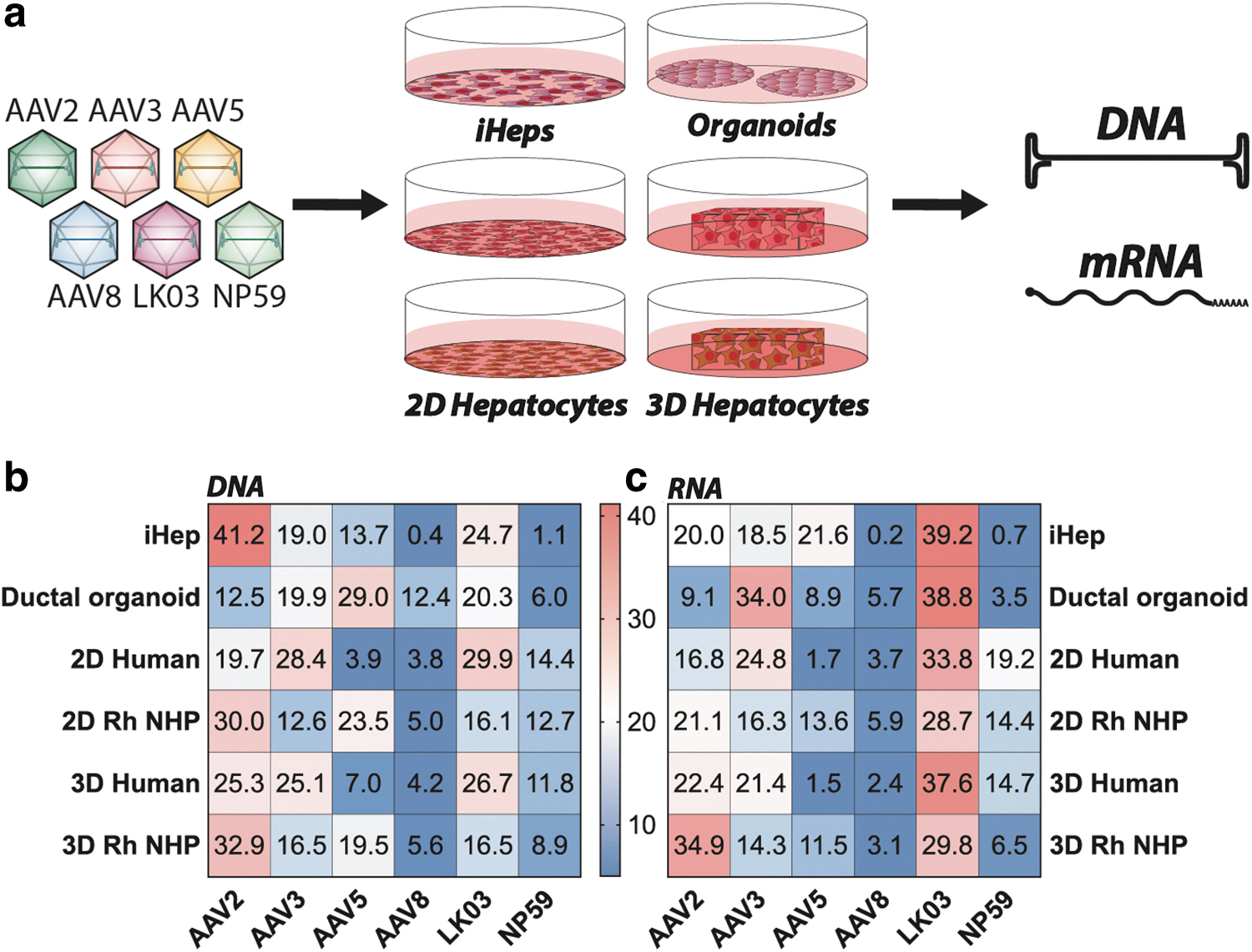
Ex vivo results in human and NHP liver models.
Using adult stem cell–derived ductal organoids consisting of liver ductal progenitor cells, 50 we found AAV5 to be most effective at entering cells (29% of NGS reads at the DNA level) (Fig. 1b). However, the efficient entry of AAV5 did not lead to efficient transgene expression, where only 8.9% of the NGS reads from RNA/cDNA could be attributed to this variant. Instead, AAV-LK03 (38.8%) and AAV3b (34%) were most efficient at transgene expression in the organoids (Fig. 1c), despite less efficient entry (20.3% and 19.9% DNA NSG reads for AAV-LK03 and AAV3b, respectively). The observed decrease in the performance of AAV2 might indicate reduced importance of binding to heparan sulfate proteoglycan (HSPG) as a critical step for cell entry. 43
To understand how the previous findings translate to primary cells ex vivo, human and rhesus monkey (Macaca mulatta) hepatocytes were seeded in 2D culture as well as 3D-printed in a hydrogel. 51 The 2D cultured hepatocytes from human and NHP were exposed to three different AAV doses (1,000, 500, and 200 vg/cell) and harvested 3 days after exposure to AAV. The hepatocytes of human origin were most efficiently entered by AAV-LK03 and AAV3b, followed by AAV2, AAV-NP59, AAV5, and AAV8 (Fig. 1b). In contrast, rhesus monkey primary hepatocytes were most efficiently entered by AAV2, followed by AAV5, AAV-LK03, AAV-NP59, AAV3b, and AAV8 (Fig. 1b), showing a marked difference compared with transduction observed in the human hepatocytes.
However, at the level of transgene expression, AAV-LK03 was the most efficient variant in both species. In human hepatocytes, it was followed by AAV3b, AAV-NP59, AAV2, AAV8, and AAV5, whereas in simian hepatocytes it was followed by AAV2, AAV3b, AAV-NP59, AAV5, and AAV8 (Fig. 1c).
As the next step, we wanted to transduce the same cells, but 3D printed in a hydrogel substrate. 38 However, before doing so, we evaluate the potential effect of the 3D culturing system on primary hepatocytes by performing RNAseq using cells before and after 3D culture (Supplementary Fig. S3). The results showed that although expression of most genes did not change substantially, several genes underwent upregulation and downregulation after 3 days of the 3D culture (Supplementary Fig. S3b and Supplementary Table S3). For the human hepatocytes, the most upregulated gene was a long noncoding RNA (PCAT1) with the proposed function of regulating genes implicated in increased cell proliferation, migration, and invasion. 52,53 Owing to a lack of comprehensive annotation coverage of the rhesus monkey genome, the RNAseq data recovered for this species was less informative than the human data.
Hepatocytes in 3D hydrogel cultures were exposed to a dose of 500 vg/cell and cells were harvested and processed for analysis 3 days later. Results obtained showed number of differences compared with results obtained with conventional 2D cultures. Consistent with the 2D cultures, AAV-LK03 entered 3D-printed human hepatocytes with the highest efficiency among the vectors tested but was more closely followed by AAV2 and AAV3b. AAV-NP59, AAV5, and AAV8 performing substantially less efficiently. In the 3D-printed simian hepatocytes, AAV2 was found to be the most effective variant at cell entry, followed by AAV5, AAV3b, and AAV-LK03, with AAV-NP59 and AAV8 being the weakest performers (Fig. 1b). At the transgene expression level (RNA), AAV2 gained in function in both human and rhesus cells compared with 2D cultures.
The data from 2D versus 3D culture systems as well as human versus NHP hepatocytes led to interesting observations. Although AAV2 worked in 2D and 3D cultures of both species, there was a substantial increase in AAV2 performance in the 3D culture system over the 2D culture. This observation could be explained with strong reliance on HSPGs in the 3D-printed hepatocytes, a question we explored further in subsequent studies. Furthermore, the data showed that AAV5 had a markedly higher performance in NHP-cultured hepatocytes than in human hepatocytes, which might explain why clinical trials using AAV5 need very high vector doses and have a lower efficacy than NHP data would suggest. 24,25
Another upregulated gene that is potentially relevant for AAV biology was glypican proteoglycan 6, a cell surface protein known to harbor HSPGs. 54 This could explain the increased transduction by AAV2 and decreased transduction by AAV-NP59, which has lower affinity to HSPG (Fig. 1), 31 in the 3D printed human hepatocytes compared with the conventionally cultured human hepatocytes.
In summary, in the simplest models of human hepatocytes, the immortalized cancer cell lines, AAV2 performed substantially better than all other variants tested. This performance decreased in stem cell–derived models and primary cells, where the performance of the bioengineered variant AAV-LK03 improved in both human and simian cells. The bioengineered AAV-NP59 also seemed to have improved in primary cells of human origin compared with its performance in immortalized cells and stem cell–derived models. One of the most interesting observations was the relatively variable performance of AAV5 across the models tested. The performance was low in HuH-7 cells and primary human hepatocytes, whereas a relatively high performance was observed in HepG2 cells, stem cell–derived iHeps, and ductal organoids, as well as primary NHP hepatocytes. This might indicate that AAV5 (the most distantly related AAV capsid of the ones chosen for this study) might utilize distinct cell entry and transduction mechanism.
Xenograft in vivo models of human and NHPs livers
Having studied the six vectors in several in vitro and ex vivo models, we next wanted to evaluate one of the commonly used in vivo xenograft model of the human liver, namely the FRG mouse. 28 To facilitate the comparison with the data obtained from the ex vivo studies, we used primary human hepatocytes and primary rhesus hepatocytes, same as in the 2D and 3D culture studies, to engraft livers of female FRG mice. In addition, with the aim to increase the impact of the study, we included primary hepatocytes from the cynomolgus monkey (M. fascicularis). The use of a xenograft model, engrafted with either human or NHP hepatocytes, enabled a side-by-side comparison of vector tropism in murine and human or NHP cells in vivo.
Thus, we generated hFRG and two types of “simianized” FRG, RhFRG, and CyFRG, based on rhesus and cynomolgus origin of cells, respectively. Animals were allowed to repopulate to a replacement index ranging from 15% to 70% and were subsequently systemically injected with the equimolar mix of the six barcoded AAV vectors (Fig. 2a). Livers were harvested 7 days after transduction. Analysis of vector function at the DNA (cell entry) level was performed in sorted GFP+ and unsorted (total “bulk” fraction) human and simian cells, whereas analysis at the RNA level (transgene expression) was only performed on human and simian cells sorted based on the vector-encoded GFP marker (GFP+).

NHP and human xenograft in vivo results.
At the cell entry level, AAV-NP59 was the most effective variant in all three xenograft models irrespective of analysis being performed on GFP+-sorted or bulk cells (Fig. 2b, c). In bulk human cells, AAV-NP59 was followed by AAV-LK03/AAV3b, AAV2, and AAV8, with AAV5 being the weakest performer. The order of vectors based on cell entry efficiency was overall similar in GFP+ human cells, with the exception that the relative contribution of AAV2 decreased substantially, suggesting that AAV2 transduced human cells but was less efficient at driving transgene expression. We also observed a relative drop for AAV3b and a corresponding increase in signal for AAV-NP59 (Fig. 2c).
Looking at functional transduction (RNA/cDNA) of human hepatocytes in the FRG model, AAV-NP59 performed best in GFP+ human hepatocytes, with AAV-LK03, AAV3b/AAV8, AAV2, and AAV5 following behind.
The results for vector entry into macaque hepatocytes engrafted in FRG mice (RhFRG and CyFRG) were very similar to those obtained in humanized mice with AAV-NP59 being the serotype most efficient at cell entry (Fig. 2b). However, in bulk macaque hepatocytes, AAV-NP59 was followed by AAV8 (instead of AAV-LK03), AAV2 (instead of AAV3b), AAV-LK03, AAV3b, and AAV5 (Fig. 2b). When analyzing GFP+ cells, we observed that highly performing variants AAV-NP59, AAV8, and AAV-LK03 showed an overall gain in contribution at the entry level, performance of AAV3b did not change substantially, whereas AAV2 and AAV5 showed a drop in efficiency compared with unsorted cells (Fig. 2c). Data from analyzed RNA confirmed this trend with AAV-NP59 showing by far the strongest contribution in simian cells sorted for GFP expression. AAV8 was the second-best performing variant and AAV-LK03, AAV3b, AAV2, and AAV5 variants had lower contributions at the transcriptional level (Fig. 2d).
Expectedly, this experiment indicated that the analysis of vector performance at the DNA level using cells sorted for transgene expression (GFP+) is more closely aligned with the analysis at the RNA level than when analyzing DNA from bulk human/NHP hepatocytes. However, bulk DNA data are useful to gain insight into the cell–vector interactions that are not leading to strong transgene expression. The analysis at the DNA level revealed that xenograft models show the same trend regarding AAV5's performance in human and NHP hepatocytes. The in vivo xenograft data indicated that AAV5 interacts with, or enters, NHP hepatocytes relatively well but encounters some intracellular block, preventing it from efficiently completing all necessary steps that lead to transgene expression.
The high performance of AAV-NP59 in hFRGs was expected based on previously generated data that showed a strong advantage over the five other AAVs used in this study. 36 The fact that we see a similar trend for the NHP-repopulated FRG mice was a very interesting finding, which may indicate a high performance of this variant in human/primate hepatocytes or a particularly xenograft-specific high performance.
NHP in vivo transduction
In the next part of the study, we compared the performance of the six vectors in vivo in a widely accepted preclinical model of human liver, the NHP (Fig. 3a). To enable studies of multiple vectors in the same immunocompetent animal, the cynomolgus monkey underwent immunoadsorption (antibody depletion) to reduce antibody concentration, as previously described. 47 Following this treatment, the NHP was infused with 4.2 × 1013 vg total (1.3 × 1013 vg/kg; 7.0 × 1012 vg/variant) of the barcoded AAV mix. The animal was killed 1 week after systemic vector infusion and 21 different tissues were harvested and processed for downstream analysis.
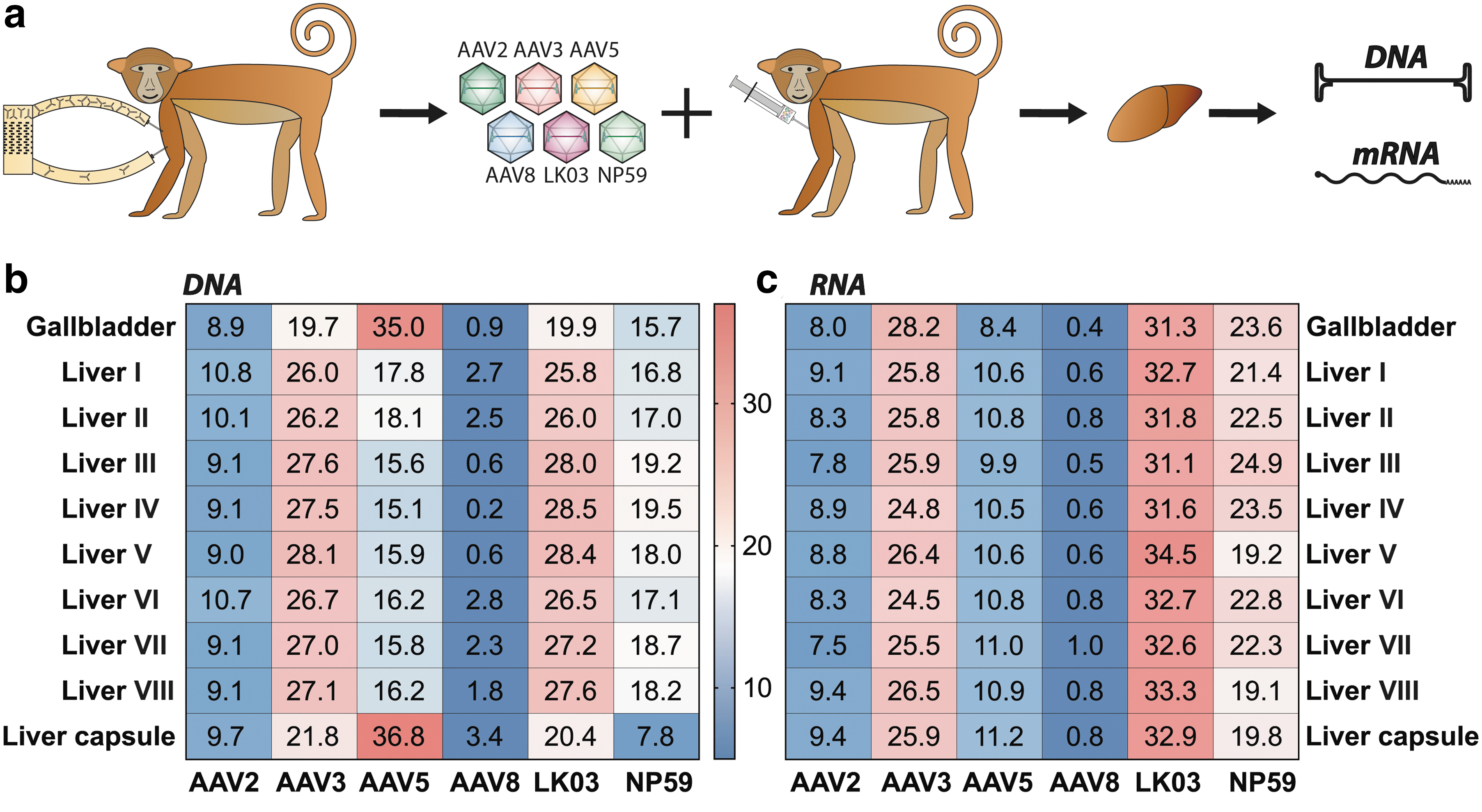
In vivo results cynomolgus monkey liver.
The samples were analyzed for vector copy number using droplet digital polymerase chain reaction (ddPCR) and transgene expression using reverse-transcriptase-ddPCR (Supplementary Table S2; Fig. 4b). As the liver was the main organ of interest in this study, samples were taken from eight different regions of the liver (see Supplementary Fig. S4a for indication of the liver regions analyzed) as well as from the gallbladder and the liver capsule and were analyzed for individual vector performance at the cell entry (DNA) and transgene expression (RNA/cDNA) levels using NGS. As expected based on previous publications, 36,55 and the fact that all six vectors studied are known to be liver tropic, vector copy number analysis showed that at the dose used the liver, gallbladder, and spleen were the organs with the highest levels of transduction (Supplementary Fig. S4b).
AAV-treated NHP serum analysis.
Nonliver organs appeared to be most efficiently entered by AAV5 (Supplementary Fig. S4c). Whether these results are truly reflecting the ubiquitous activity of AAV5 or are an artifact of the very low vector copy number in these organs cannot be inferred from this dataset. Unsurprisingly, given that the GFP transgene expression was driven by the ApoE/hAAT liver-restrictive promoter, transgene expression could only be detected in the liver and gallbladder (Supplementary Fig. S4b). 37,56,57
With the caveat that data were obtained from a single NHP, NGS analysis of liver samples showed that AAV-LK03 and AAV3b were the most effective variants at transducing most regions of the liver. AAV-NP59 was the next best performer, followed closely by AAV5. Of interest, AAV5 was the serotype that entered cells most efficiently in the gallbladder and liver capsule (Fig. 3b). AAV2 and AAV8 were the least efficient serotypes at cell entry (Fig. 3b). In terms of transgene expression, AAV-LK03 was the best performing variant, followed by AAV3b and AAV-NP59. AAV5, AAV2, and AAV8 performed relatively poorly (Fig. 3c). Although these observations require replication in additional NHPs, the hierarchies of capsid performance observed were sufficiently distinctive to offer preliminary insights worthy of discussion.
As the NHP experiment was terminated just 1 week after vector infusion, it is possible that expression from some of the AAV variants may not have reached the peak level. 58 It is therefore possible that AAVs that entered well (such as AAV5) could have, with time, led to higher mRNA expression compared with AAVs that entered less efficiently, but appear to have higher kinetics of expression (such as AAV-NP59). Although the authors appreciated the fact that the timing of the study could directly affect the study outcome, the main reason for the shorter timeline was to ensure consistency between ex vivo (1 week or less) and xenograft in vivo (1 week) experiments.
Based on previously published data, we were not surprised by the high performance of AAV-LK03. 55 It was also interesting to see how much better AAV-NP59 performed compared with the prototypical AAV2, which is highly homologous at the protein level, but potentially tissue culture adapted. 43 This indicates that the previously published advantage of lower HSPG binding could be beneficial in in vivo xenograft mouse models as well as NHP models. 31 As AAV-NP59 has not been evaluated in human studies, we can only rely on the hFRG, Rh/CyFRG and in vivo NHP data to infer clinical efficiency of this variant. Our data strongly suggest that AAV-NP59 would most likely perform substantially better than AAV2, but less efficiently than AAV3b/AAV-LK03, as we can see that the performance of AAV-NP59 in the CyFRG mice was overestimated compared with performance in Cynomolgus macaque in vivo. Finally, the most surprising finding from the NHP experiment was the very low AAV8 performance, 55 which warranted further investigation.
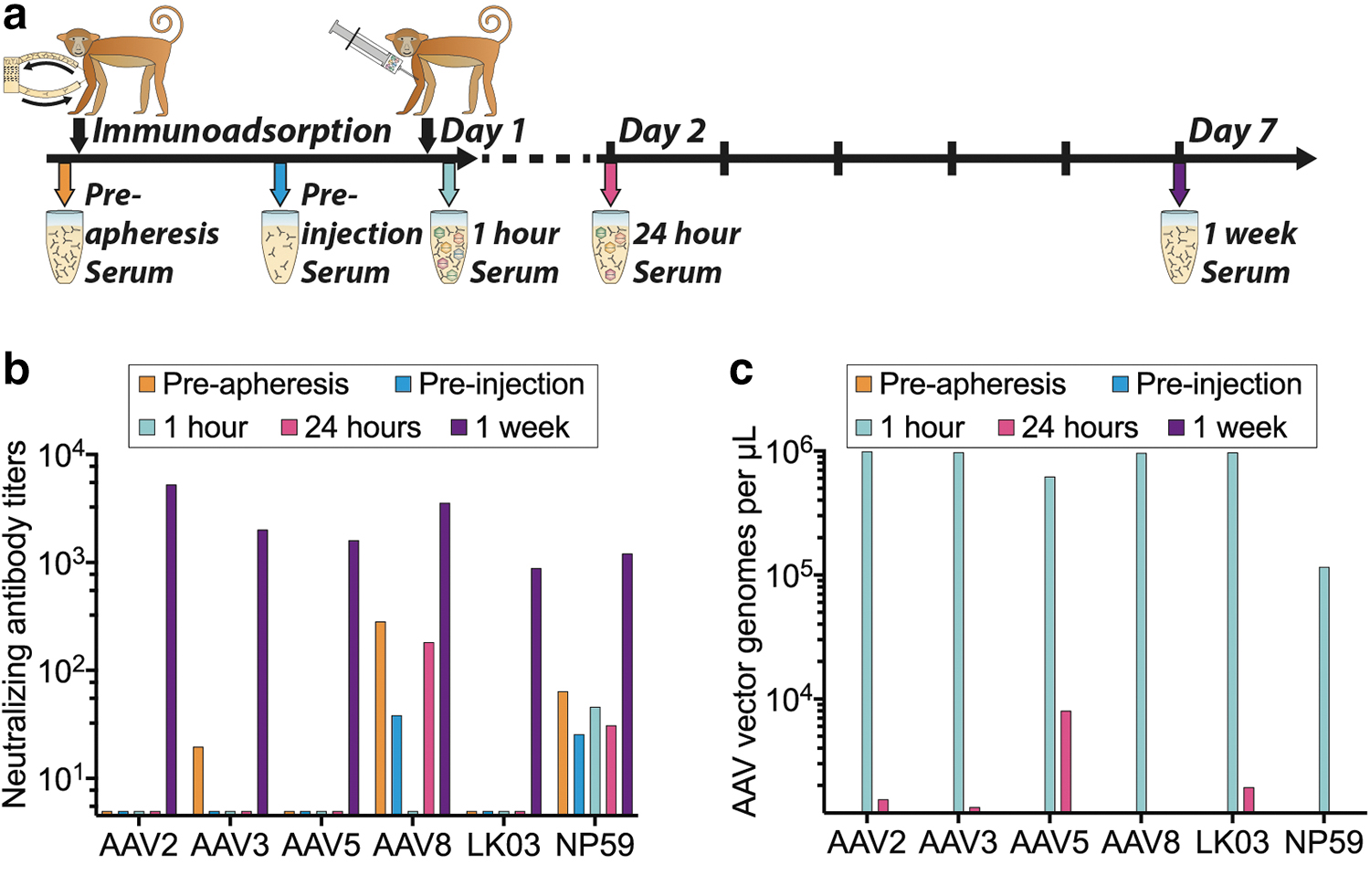
NHP serum analysis
Driven by the fact that AAV8 performance in the NHP liver was lower than anticipated based on published data, 55 we analyzed the levels of anti AAV NAbs in the serum harvested before AAV infusion. In addition, the clearance of AAVs from the serum was quantified. Both seroreactivity and AAV clearance were evaluated at five time points (Fig. 4a).
The NAb titers showed that the NHP had pre-existing NAbs against AAV3b, AAV8, and AAV-NP59 before apheresis. These NAb titers were reduced by the apheresis in all cases. Although the anti-AAV3 NAbs were effectively removed, antibodies against AAV8 and AAV-NP59 were not fully eliminated (Fig. 4b).
Seven days after vector administration we detected high NAb titers against all six AAV variants (Fig. 4b). Previous publications showed that even low NAb titers against AAV8 capsids could have a strong neutralization effect in vivo in NHPs, and that this effect was substantially greater than expectations based on results from in vitro neutralization assays. 59,60 These published results lead us to the conclusion that the presence of residual anti-AAV8 NAbs can potentially explain, at least partially, the low performance of AAV8 vector in vivo. 47,59
Although our data align well with published results, it is important to note that different methods of generating neutralization data can yield widely different results. This was highlighted by the comparison of in vitro and in vivo–generated NAb data published by Wang et al. in the case for AAV8. 60 The main reason for the divergence reported by the author was that AAVs transduce different cells with varying efficiencies (AAV2 is much better in vitro than in vivo compared with AAV8, and vice versa). Lower transduction efficiency means less sensitivity when evaluating antibody titers by neutralization and therefore every assay will be different depending on which doses and target cells are being used and whether adenoviral coinfection is used to boost transduction. 60
With this in mind, we attempted to reduce experimental variability caused by varying transduction titers by establishing the required vector doses to achieve high transduction efficiency before the NAb assay for each of the AAVs. Although we understood that this approach does not address all the ambiguities of the neutralization assay, we hypothesize that it helped improve accuracy and thus the robustness of our data.
Analysis of AAV vector genomes in serum confirmed that substantial levels of AAV vectors were in circulation 1 h after the injection, and that most of the vectors were cleared within the first 24 h postinfusion. Particle concentrations were very similar between all variants apart from AAV-NP59, which showed an almost 10-fold lower concentration in the serum at the 1-h time point compared with all other variants (Fig. 4c), potentially indicating a faster uptake of AAV-NP59 by the liver, uptake by other tissues, or an uptake by certain immune cells owing to the observed interaction with NHP serum (Fig. 4b).
Effect of NHP serum on the transduction of AAV vectors in xenograft models of the human liver
Next, we wanted to take advantage of the humanized and “simianized” FRG models to investigate the potential impact of the anti-AAV NAbs in the NHP serum on vector transduction of primary hepatocytes. Using methods previously described, 40 the equimolar mix of AAVs was coincubated at a range of dilutions with NHP serum collected after the apheresis but before vector administration (Fig. 4a, “preinjection serum”), and thus contained small titer of anti-AAV8 and anti-AAV-NP59 NAbs (Fig. 4b). The serum–AAV mix was subsequently injected into FRG mice repopulated with primary hepatocytes from either Rhesus macaque, Cynomolgus macaque, or human origin (Fig. 5a). Human and NHP hepatocytes, as well as murine hepatocytes, were recovered from livers harvested 7 days after systemic administration of the serum–AAV mix and individual vector transduction was analyzed at the DNA level using NGS of the barcoded genomic region.
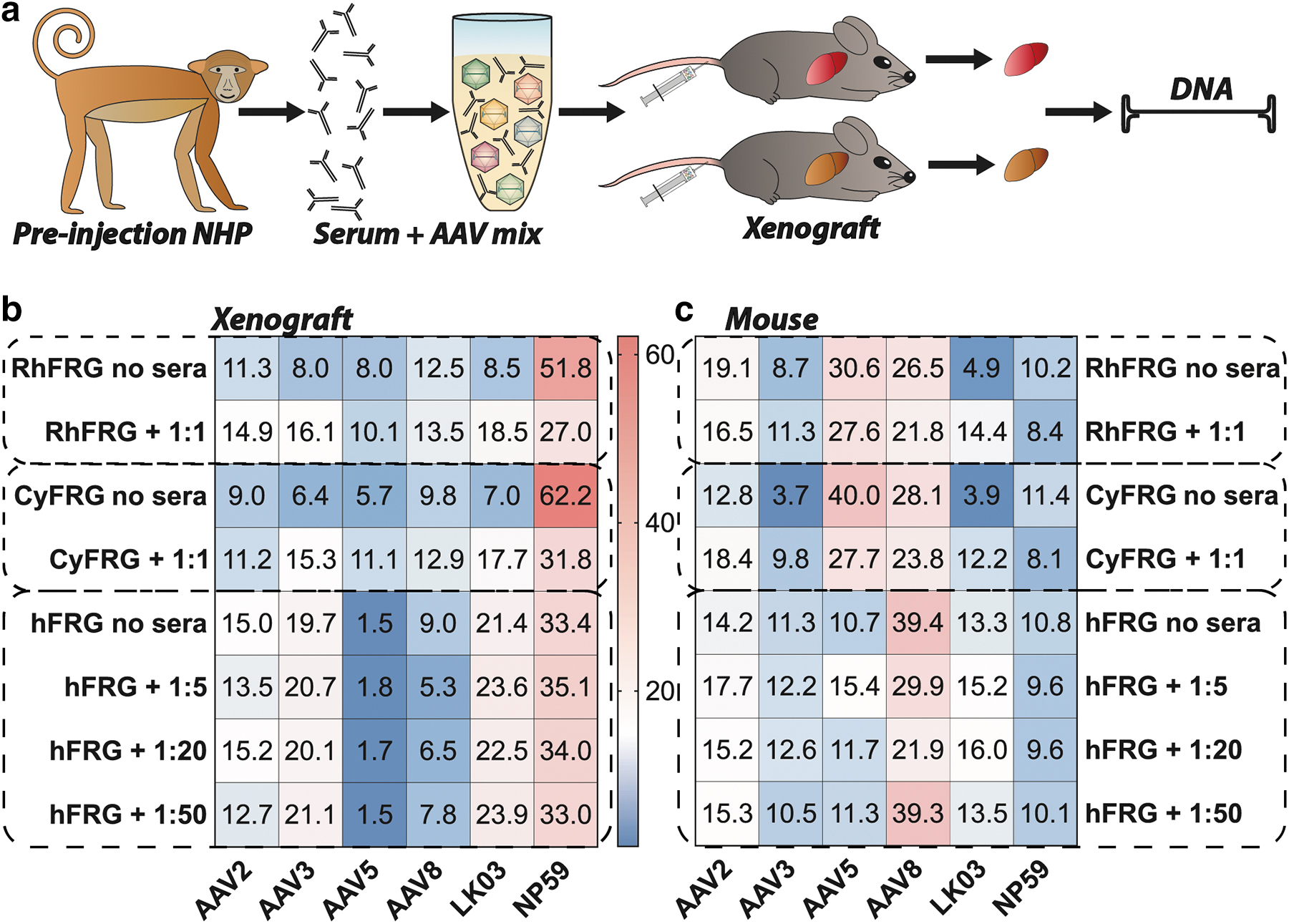
In vivo transduction with NHP preinjection serum-incubated AAV mix.
AAV-NP59 was the top performer at the DNA level in FRG mice repopulated with Rhesus and Cynomolgus hepatocytes with and without vector preincubation with serum. However, the AAV-NP59 contribution in the group treated with the serum was substantially lower than that in the group transduced with untreated vectors (Fig. 5b), indicating that the anti-AAV-NP59 antibodies were partially neutralizing the vector and thus decreasing its performance. Of interest, there was no detected drop in the transduction efficiency of AAV8 following incubation with NHP sera. However, it is important to note that NGS percentages are relative to one another and thus the substantial drop in contribution from AAV-NP59 could mask a potentially reduced efficiency of neutralized AAV8. Indeed, relative transduction of all other vectors increased as the contribution of AAV-NP59 decreased, with AAV8 and AAV2 showing the lowest increase in transduction. This could indicate that the sera contained NAbs against those two variants.
Of interest, studies in FRG repopulated with human hepatocytes (hFRG) showed that performance of AAV-NP59 was not affected by the anti-AAV NAbs-containing serum and neither was the performance of AAV2, AAV3b, AAV5, or AAV-LK03, but the performance of AAV8 was reduced at the higher serum concentrations (Fig. 5b). All data shown as “Rh/Cy/hFRG no sera” are also used in Fig. 2b and are shown again for ease of comparability.
Finally, analysis of the mouse hepatocytes recovered from the chimeric livers showed a mild drop in the performance of AAV8 and AAV-NP59 for NHP and human-repopulated mice (Fig. 5c). Of interest, performance of AAV3b and AAV-LK03 in “simianized” FRGs appeared to have improved slightly following preincubation with NHP sera. Although this can be partially explained by the previously mentioned fact that NGS reads for each vector are relative to one another, the effect could also indicate an active interaction between AAV3-like capsids with components of the NHP serum, as similar findings for some AAVs have been reported for interactions with human sera in mice. 61 It is also important to note that the immunodeficient FRG mouse model may not fully recapitulate what happens to AAV–antibody complexes in immunocompetent NHPs in vivo, as many immune cells are not fully developed.
Seroprevalence of NAbs against capsids used in this study
As transduction efficiency of an AAV capsid can be negatively affected by NAbs, pre-existing immunity can exclude patients from an AAV gene therapy trial or clinical treatment. 62 Therefore, we assessed the seroprevalence of NAbs against AAV variants used in this study in 85 human samples. Samples were collected from individuals younger than 1-year old (17%), aged 1–5 years (35%), 6–10 years (16%), 11–20 years (12%), and older than 20 years (20%). The overall seroprevalence of NAb ranged from 14% (AAV5) to 29% (AAV3b) (Fig. 6a).
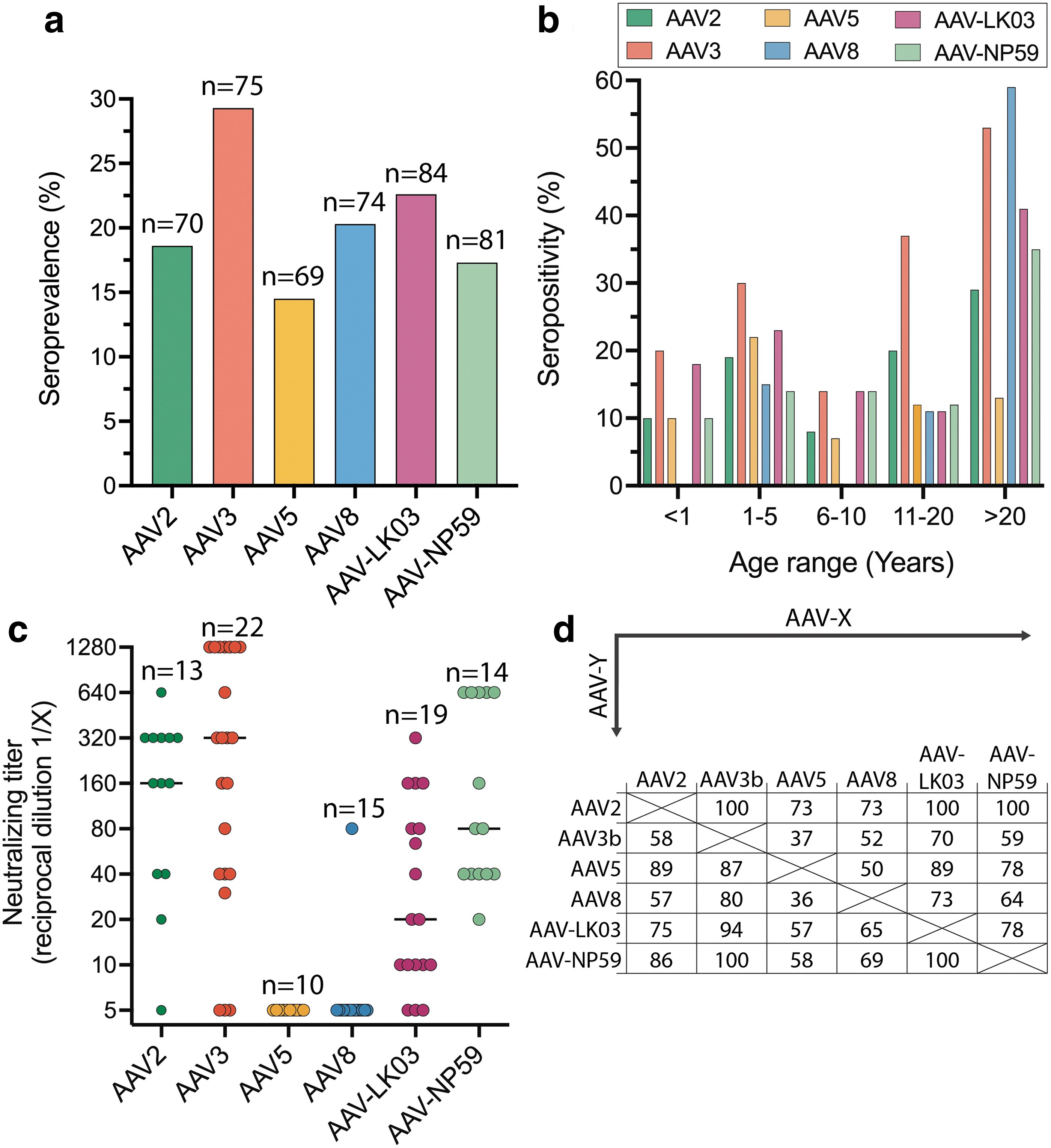
Seroprevalence and titers of NAbs of liver-tropic capsids.
Seroprevalence was low during the first years of age and increased after the age of 10 years (Fig. 6b). NAb titers are higher for AAV3b, AAV2, and AAV-NP59 with median of 1/320, 1/160 and 1/80, respectively. Lower NAb titers were observed for AAV5, AAV8, and AAV-LK03 with medians of 1/5, 1/5 and 1/20, respectively (Fig. 6c). Strong cross-reactivity with other liver-tropic capsids tested was detected for AAV2, AAV-NP59, and AAV5 (Fig. 6d).
In the cohort of plasma samples tested for seroprevalence, 80% were from persons aged 20 years or younger. This work corroborates previous findings that most pediatric individuals have not yet developed anti-AAV antibodies, which emphasizes a decisive immunological advantage of targeting this age group. 63,64 The seroprevalence rates increased rapidly in teenage and adulthood where NAb seroprevalence rates could be as high as 80% for the some AAV serotypes. 27,64 –68 Our data for sera from the adult population showed lower neutralization rates compared with other seroprevalence studies 66 but the findings were in accordance with our previous work in the British population. 46 AAV2, AAV3b, and surprisingly AAV-NP59 showed higher titers compared with AAV5, AAV8, and AAV-LK03, although the use of a higher dose for AAV5 and AAV8 may have reduced the sensitivity and partly underestimated the titers. 69
NAb cross-reactivity was high between some liver-tropic capsids. 46,64,66 These findings support the need for innovative immunosuppression protocols or antibody reduction methods to allow successful transduction in preimmunized patients and readministration, if needed. 62 Antibody reduction has previously been performed either by removing all antibodies (as has been used for the NHP in the presented study) 47 or by specifically removing anti-AAV antibodies. 70,71 Another recently reported option is to use IgG degrading enzymes, which would be infused systemically before AAV delivery. 72,73 These methods would be especially relevant for use in infants, who are only passively immunized through adoptive transfer from the mother and do not have memory cells specific against AAV epitopes, making it less likely for their immune system to be activated.
Conclusions
Expectedly, we observed that the interaction of the AAV vectors and the target hepatocytes differed in in vitro and ex vivo cells as well as xenograft models and in vivo NHP transductions, recognizing the potential limitation of our conclusions arising from using only a single NHP in our study. However, although a perfectly predictive preclinical model does not exist, our study shows that each model provides a unique insight into the vector function. Yet, without the benefit of clinical data, where each of the vectors would be tested for the delivery of the same transgene cassette to the liver, it is impossible to determine, with a high level of certainty, which of the models is the most predictive of human outcome.
Based on our results and the fact that each model brings a unique perspective that adds to the overall functional evaluation of AAV vectors, we propose that multiple models should be used to paint a more complete picture and help us make the most informed decision as to which vector should be used in each clinical application. To do so, it is critical to understand the strengths and weaknesses of each model. Specifically, our data confirmed that many tissue culture models are overly dependent on strong AAV binding to HSPG, which may not be directly applicable to an in vivo setting. 31,43
We also found that AAV5 generally performed better in primary NHP hepatocytes ex and in vivo compared with human hepatocytes in the same experimental settings. As this finding was consistent between models, it may explain the lower-than-expected outcomes in several clinical trials using AAV5 to target the human liver. 24,25 As AAV8 performed better in NHP-FRGs than in hFRGs, our data could suggest that a similar mechanism could affect AAV8's performance in human hepatocytes.
In general, our study showed that the FRG mouse model offers high flexibility and utility as it can be repopulated with primary hepatocytes from human and NHPs. 74 Thus, this xenograft model allows investigators to gain a unique insight into the cross-species transferability of the AAV performances data from NHPs, the most sought after preclinical model of human liver, to human patients. Furthermore, our data showed that the correlation between data obtained from NHP and xenograft model was not perfect. This could be owing to complex, and not fully understood, interactions between xenograft and mouse hepatocytes, competition in AAV uptake between the species, or the absence of a complete immune system in the mice. One conclusion that becomes apparent from our study was that compared with the NHP data, the NHP hepatocytes in the FRG mouse appear to have an increased uptake of AAV-NP59 and a reduced uptake of AAV5.
However, the NHP model may not be perfect either. Apart from ethical considerations around the use of NHPs in biomedical research, availability and cost can be prohibitive. The cost and availability of NHPs is also affected by the fact that animals need to be screened for pre-existing anti-AAV NAbs. Finally, the fact that wild-type, outbred NHPs are used, leads to the requirement of using higher number of animals per group to account for natural differences between “subjects.”
Based on the data presented, our current understanding of the individual preclinical models, as well as our insights into the AAV–cell interactions, we propose that initial studies of liver-targeting AAVs should include hFRG mice in the presence of human serum and/or pooled IgG before initiating studies involving large animals.
It is, however, critical to note that all models used in this study have a number of critical limitations that could not have been addressed in this article. For example, no model system was yet found to fully recapitulate the anti-AAV cellular immune responses seen in clinical trials. 13,14 Although the immune-deficient FRG mice are not the most suitable model to test immune responses to transduction, a hybrid xenograft FRG mouse containing the hematopoietic system and the hepatocytes from matching human donors might be a possibility in the future.
Based on data from a hemophilia A clinical trial for AAV-LK0330 as well as data from this study (good efficiency at transducing NHP and human hepatocytes ex vivo and in vivo in the xenograft model and the NHP, and relatively low pre-existing immunity in the general population), we anticipate that the next-generation bioengineered AAV-LK03 and AAV-NP59 vectors will be strong clinical candidates for liver targeted therapies.
Footnotes
AUTHORs' CONTRIBUTIONS
A.W., M.C.-C., E.Z., D.S.G., D.P.P., S.A.W., J.B., G.G-A., and L.L. designed the experiments. A.W., M.C-C., K.L.D., E.Z., D.S.G., R.G.N., S.S., M.K., A.M., S.F., D.P.P., B.M.T., E.V., S.L.W., S.A.W., and L.L. generated reagents, protocols, performed experiments, and analyzed data. A.W., A.K.A., and L.L. wrote the article and generated the figures. All authors reviewed, edited, and commented on the article.
DISCLAIMER
The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
AUTHOR DISCLOSURE
L.L., I.E.A. and A.J.T. have commercial affiliations. L.L. and I.A.E. have consulted on technologies discussed in this article. L.L. and I.A.E. have stock and/or equity in companies with technologies broadly related to this study. L.L. is a co-inventor of, and receives licensing royalties from, several AAV variants used in the study. A.L.M. and T.E.H. are employees, shareholders, and/or optionees of Inventia Life Science Pty. Ltd. Inventia has an interest in commercializing the 3D bioprinting technology. All other authors declare no competing financial interests.
FUNDING INFORMATION
This work was supported by project grants from the Australian National Health and Medical Research Council (NHMRC) to L.L. and I.E.A. (APP1108311, APP1156431 and APP1161583) and Paediatrio Paediatric Precision Medicine Program to L.L. (PPM1K5116/RD274). Work presented in Figs. 3 and ![]() were supported by funding from LogicBio Therapeutics. L.L. was also supported by research grants from the Department of Science and Higher Education of Ministry of National Defense, Republic of Poland, (“Kościuszko” k/10/8047/DNiSW/T—WIHE/3) and from the National Science Centre, Republic of Poland (OPUS 13) (UMO-2017/25/B/NZ1/02790).
were supported by funding from LogicBio Therapeutics. L.L. was also supported by research grants from the Department of Science and Higher Education of Ministry of National Defense, Republic of Poland, (“Kościuszko” k/10/8047/DNiSW/T—WIHE/3) and from the National Science Centre, Republic of Poland (OPUS 13) (UMO-2017/25/B/NZ1/02790).
The work of I.E.A. was also supported by an Australian Research Council (ARC) Discovery Project (DP150101253). A.J.T. was supported by funding from The Wellcome Trust (Grant No. 217112/Z/19/Z AJT). This work was supported by funding to J.B. from the NIHR Great Ormond Street Hospital Biomedical Research Centre; Medical Research Council Grant/Award Number: MR/T008024/1; National Institute for Health Research; Innovate UK Biomedical Catalyst Early stage award 14720; Nutricia Metabolic Research Grant; London Advanced Therapy/Confidence in Collaboration award 2CiC017.
SUPPLEMENTARY MATERIAL
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.