
Abstract
The ongoing advancements in CRISPR-Cas technologies can significantly accelerate the preclinical development of both in vivo and ex vivo organ genome-editing therapeutics. One of the promising applications is to genetically modify donor organs prior to implantation. The implantation of optimized donor organs with long-lasting immunomodulatory capacity holds promise for reducing the need for lifelong potent whole-body immunosuppression in recipients. However, assessing genome-targeting interventions in a clinically relevant manner prior to clinical trials remains a major challenge owing to the limited modalities available. This study introduces a novel platform for testing genome editing in human lungs ex vivo, effectively simulating preimplantation genetic engineering of donor organs. We identified gene regulatory elements whose disruption via Cas nucleases led to the upregulation of the immunomodulatory gene interleukin 10 (IL-10). We combined this approach with adenoviral vector-mediated IL-10 delivery to create favorable kinetics for early (immediate postimplantation) graft immunomodulation. Using ex vivo organ machine perfusion and precision-cut tissue slice technology, we demonstrated the feasibility of evaluating CRISPR genome editing in human lungs. To overcome the assessment limitations in ex vivo perfused human organs, we conducted an in vivo rodent study and demonstrated both early gene induction and sustained editing of the lung. Collectively, our findings lay the groundwork for a first-in-human-organ study to overcome the current translational barriers of genome-targeting therapeutics.
INTRODUCTION
Genome editing holds significant promise for establishing enduring therapeutic effects through precise manipulation of the genome. The introduction of CRISPR-Cas technology 1 has democratized genome editing, marking the dawn of a new era in gene and cell therapies. The evolution of CRISPR tools, including base editors, 2 prime editors, high-fidelity Cas enzymes, 3,4 and protospacer adjacent motif (PAM) variants, 5 has continued to expand the scope of genetic modification and enhanced accuracy, improving the safety and efficacy of therapeutic editing. These technological advancements have ushered a growing number of candidate therapies into clinical trials, both ex vivo and in vivo. 6
One particularly exciting biomedical application is genetic engineering to create less immunogenic donor organs. The current standard post-transplant care necessitates lifelong strong systemic immunosuppression to prevent graft rejection in recipients. However, long-term whole-body immunosuppression carries significant morbidity by increasing the risk of complications, such as severe infections and malignancies, and adverse side effects such as renal dysfunction and diabetes. We hypothesized that genetically modified donor organs, designed to provide local long-lasting intragraft immunomodulation, could potentially reduce the need for maintenance high-dose systemic immunosuppression, thus addressing these critical clinical issues.
The translation of genome-targeting therapeutics faces a significant challenge in terms of human-relevant evaluation prior to initiating clinical trials. CRISPR-based therapies rely on sequence specific targeting of Cas enzymes. 6 As a result, interspecies differences of the genome can more substantially impact editing efficiency and the ensuing phenotypic changes compared with other interventions that don’t involve genome targeting. 7 In contrast to ex vivo cell therapy, where a favorable population of edited cells is selected before being introduced into the body, in vivo genome editing, where editing enzymes are directly delivered to the body, 8 and implantation of the ex vivo edited organs demand a more stringent preclinical assessment for safety. A broadly used approach for the preclinical assessment of CRISPR therapeutics combines in silico simulations, cellular profiling, and evaluation in animal studies. 9 However, each of these methods has its limitations: computational analysis often lacks biological context; cellular analysis falls short of capturing the complexities of organ and body systems; and animal studies necessitate conversion of editing design to target the genome of the target species that could compromise the relevancy in human. Humanized animals have been used to bridge this gap, 10,11 but variations persist in their genetic and epigenetic makeup, molecular functionality, and interactions of the target molecules compared with those in humans. Therefore, testing in human organs presents a unique and ideal strategy to collect key information for application in the human body, including insights into dosing and efficacy.
In the field of solid organ transplantation, the advent of machine perfusion has opened new opportunities for evaluating potential interventions in human organs ex vivo. For example, the ex vivo lung perfusion system (EVLP), 12 which enables normothermic perfusion of donor lungs, has been clinically used to assess graft function preimplantation and has been applied to evaluate gene delivery therapy, 13 protein therapy, 14 pharmacological therapy, 15 light therapy, 16 and cell-based therapies. 17 We hypothesized that assessing genome editing in ex vivo perfused human organs could offer a groundbreaking approach to the preclinical evaluation of advanced molecular therapies, such as CRISPR-based therapeutics. However, the limited duration of ex vivo perfusion posed a challenge for testing genome editing, and this feasibility had remained unresolved at this time.
In this study, we took the initial step of developing a genome-editing method to upregulate an immunomodulatory gene, IL-10, and generated optimized adenoviral vectors (AdVs) to induce early and sustained IL-10 expression for graft immunomodulation. We then applied this approach to ex vivo perfused human donor lungs. To continue monitoring the treated lung tissue beyond the duration of organ perfusion, we cultured thin tissue slices post-EVLP using precision-cut lung slice (PCLS) technology. For longer-term observations, we conducted an in vivo study using a rat model. Collectively, our findings demonstrate the feasibility of testing genome-editing interventions in a first-in-human-organ study, representing an innovative avenue for the safe and accelerated clinical translation of CRISPR therapeutics.
MATERIALS AND METHODS
Plasmid vector construction and adenoviral vector production
The guide RNAs (gRNAs) used in this study are listed in Supplementary Table S2. Oligos containing the spacer sequence of gRNAs were synthesized at ACGT Corporation (Toronto, ON, Canada) or Eurofins Genomics (Louisville, KY, USA). The annealed and phosphorylated oligos were cloned into Staphylococcus aureus Cas9 (SaCas9) plasmid (pX601-AAV-CMV::NLS-SaCas9-NLS-3xHA-bGHpA;U6::BsaI-sgRNA, 18 a gift from Feng Zhang, Addgene plasmid # 61591; http://n2t.net/addgene:61591; RRID:Addgene_61591) or gRNA expression plasmid (BPK1520, 19 a gift from Keith Joung, Addgene plasmid # 65777; http://n2t.net/addgene:65777; RRID:Addgene_65777) and used for further cloning. For the plasmids containing human IL-10 complementary DNA (IL-10 cDNA), DNA fragments containing T2A, human IL-10 cDNA, SV40 polyA, and gRNA expression cassette were synthesized as gBlock (Integrated DNA Technologies Inc., Coralville, IA, USA) and cloned into the SaCas9 expression plasmids. Plasmids were purified using EndoFree Plasmid Maxi Kit (12362, QIAGEN, Hilden, Germany) and used for transfection to cultured cells. For AdV production, the completed constructs were whole plasmid sequenced (Plasmidsaurus, Eugene, OR, USA) and functionally validated in cultured cell lines. The E1/E3-deleted replication incompetent recombinant adenovirus serotype 5 was generated at high titer by transferring the whole transgene into a shuttle vector, generating primary virus, and amplification and purification at SIRION Biotech (Munich, Germany).
Cell culture
HEK293 cell line (CRL-1573, ATCC, Manassas, VA, USA) and PT-K75 cell line (CRL-2528, ATCC, Manassas, VA, USA) were cultured in Dulbecco’s modified Eagle medium (DMEM) (11995-065, ThermoFisher Scientific, Waltham, MA, USA), and L2 cell line (CCL-149, ATCC, Manassas, VA, USA) was cultured in Ham’s F-12K media (21127022, ThermoFisher Scientific), respectively, supplemented with 10% fetal bovine serum (FBS) (A3840302, ThermoFisher Scientific) and 100 U/mL of penicillin streptomycin (15140122, ThermoFisher Scientific) at 37°C with 5% CO2.
Plasmid transfection and adenoviral vector transduction to cultured cells
Cells were seeded in 6-well plates 1 day before transfection at a density of 2 × 105 viable cells/mL for HEK293 cells, 1.5 × 105 viable cells/mL for L2 cells, and 4 × 105 viable cells/mL for PT-K75 cells. The plasmid transfection was performed using 2.5 μg/well of plasmid and 3.75 μL/well Lipofectamine 3000 reagent (L3000150, ThermoFisher Scientific) according to the manufacturer’s instructions.
For adenoviral transduction, L2 cells were seeded in 12-well plate at a density of 1.5 × 105 viable cells/mL, transduced with adenovirus by changing the media to 500 μL/well virus-containing media. After 3 h, 500 μL/well of media was added. The media was left untouched for the initial 3 days and changed —two to three times a week afterward. The media was changed 72 h before sample collection.
Ex vivo lung perfusion
The study was approved by the Research Ethics Board of University Health Network (UHN) (06–0283) and Trillium Gift of Life Network, Ontario, Canada. Human donor lungs that were not used for clinical lung transplantation and from donors who consented to research were used in this study.
The donor lungs were retrieved using the same protocol as in clinical transplantation in the Toronto Lung Transplant Program and transported at 4°C. In Case 1, the lung was stored at 10°C 20 for approximately 5 h after retrieval before starting the cannula attachment for logistical reasons. The EVLP was performed based on the standard clinical Toronto EVLP protocol 21 with some modifications. 22 Briefly, the cannulas are attached to pulmonary artery and left atrium. An endotracheal tube was inserted into the right or left main bronchus and fixed with ties. Retrograde flushing was performed using low potassium dextran solution (Perfadex Plus, XVIVO Perfusion, Gothenburg, Sweden or LungProtect® from Traferox Technologies Inc., Mississauga, Canada) after the cannula attachment.
The circuit was primed with perfusate (LPD2A from United Therapeutics, Silver Spring, MD, USA), supplemented with methylprednisolone (Solumedrol, Pfizer, New York, NY, USA), heparin sodium (Heparin LEO; LEO Pharma Inc., Toronto, ON, Canada), and meropenem (Meropenem; SteriMax Inc., Oakville, ON, Canada) using the same dose as those in the standard Toronto EVLP protocol. During the initial 1 h of EVLP, the flow was increased stepwise. The temperature was increased incrementally, and ventilation was initiated when the temperature reached 32°C, which is around 30 min from the EVLP start. The perfusate from both the pulmonary artery and left atrium side were analyzed using GEM Premier 5000 system (Werfen, Bedford, MA, USA) every hour. Bronchial wash was performed by administering 20 mL of saline into the right or left main bronchus and collected using a bronchoscope. Perfusate and bronchial wash samples were snap-frozen and stored at −80°C until analysis. Tissues were formalin fixed or snap-frozen for downstream analysis.
Adenoviral administration during EVLP
AdVs were diluted with saline to a final volume of 5 mL. The virus-containing reagent was delivered through a catheter (NA-411D-1521, Olympus Corporation, Japan) using a bronchoscope (BF-Q190, Olympus Corporation). After delivery, the lung was recruited and then returned to the maintenance ventilation setting.
PCLS of the human lung after EVLP
A low-gelling temperature agarose was prepared at 1.5% in DMEM/F-12 media (10565018, ThermoFisher Scientific). Upon completion of the EVLP, pieces of lung tissues were inflated with the warm liquid agarose, solidified on ice, and sectioned at 500 μm thickness using vibrating blade microtome (VT1200 Vibratome, Leica, Wetzlar, Germany) in Hanks' balanced salt solution (14025092, ThermoFisher Scientific) with 10 mM N-2-hydroxyethylpiperazine-N-2-ethane sulfonic acid (HEPES) (15630080, ThermoFisher Scientific). The slices were cultured in Glutamax-containing DMEM/F-12 media (10569010, ThermoFisher Scientific) supplemented with 10% FBS (A3840302, ThermoFisher Scientific), antibiotic-antimycotic (15240062, ThermoFisher Scientific), MEM Non-Essential Amino Acids Solution (11140050, ThermoFisher Scientific), 1 mM sodium pyruvate (600-100-EL, WISENT Inc., St-Bruno, QC, Canada), and 14.3 mM beta-mercaptoethanol (M6250, St. Louis, MO, USA). The culture media were changed daily. For the measurement of the secreted IL-10 protein, each slice was incubated with 1 mL/slice of culture media for 36 h. The slices were then fixed with formalin or snap-frozen for downstream analysis. Live cell staining was performed using the LIVE/DEAD™ Viability/Cytotoxicity Kit (L3224, ThermoFisher Scientific) according to the manufacturer’s instructions.
Rat study
The study was approved by the Committee of Animal Resources Center at UHN (Animal Usage Protocol # 6057). Male inbred Lewis rats (LEW/SsNHsd, 250–350 g) were purchased from Envigo (Huntingdon, United Kingdom).
The same method of viral delivery was used as in a previous work. 23 Briefly, rats were anesthetized by inhalation of isoflurane, orotracheally intubated with a 16G catheter (BD382258, BD, Franklin Lakes, NJ, USA), and ventilated (Harvard Apparatus, Holliston, MA, USA) at a tidal volume of 10 mL/kg, positive end-expiratory pressure 2 cm H2O, fraction of inspired oxygen (FiO2) 1.0, and a respiratory rate of 80 breaths per minute in the supine position. After placing the intubation tube in the left bronchus, the rat was changed to the left lateral position and 500 μL of vector containing buffer (HEPES 100 mM, MgCl2 20 mM) was delivered to the left lung through the intubation tube. After moving the intubation tube to the trachea, the rat was ventilated in the left lateral position until awakening.
Triple immunosuppression, which comprising cyclosporine (15 mg/kg/day), azathioprine (6 mg/kg/day), and methylprednisolone (30 mg/kg), was intraperitoneally injected 2 h before viral vector administration and on day 1 and day 2. After 2 h of viral delivery, methylprednisolone alone was additionally injected into the peritoneal space. From day 3 to day 28, triple suppression with a reduced dose of methylprednisolone (cyclosporine 15 mg/kg/day, azathioprine 6 mg/kg/day, and methylprednisolone 2.5 mg/kg/day) was subcutaneously injected daily.
Nucleic acid purification
In in vitro analysis, purification of RNA and genomic DNA was performed using the Allprep kit (QIAGEN) according to the manufacturer’s instructions. In nucleic acid purification from rat tissues, the RNA later-stabilized tissues (rat study) were homogenized using the TissueLyser II (QIAGEN) and then subjected to nucleic acid purification. For PCLS samples, one or two snap-frozen slices were homogenized. RNA was purified by the TRIzol (Fisher Scientific, Hampton, NH, USA) method. DNA was purified using the QIAamp DNA Mini Kit (QIAGEN).
Reverse transcription-quantitative polymerase chain reaction
cDNA was synthesized using 500 ng (cell culture and PCLS samples) or 1000 ng (rat tissue samples) of RNA and an iScript Advanced cDNA Synthesis Kit for reverse transcription-quantitative polymerase chain reaction (RT-qPCR) (Bio-Rad, Hercules, CA, USA). The cDNA reaction was diluted in 1:6 (cell culture and PCLS samples) or 1:10 (rat tissue samples), and 3 μL was applied to 10 μL RT-qPCR reaction with SsoAdvanced Universal SYBR Green Supermix (Bio-Rad) and run on a CFX384 Real-Time System (Bio-Rad Laboratories). The Ct values obtained after 40 cycles were normalized to a housekeeping gene peptidylprolyl isomerase A (ppia) and used to calculate relative expressions. The primers used in this study are listed in Supplementary Table S3. For the samples that were not detectable after 40 cycles of RT-qPCR reaction, a Ct of 40 was applied.
Analysis of genome editing using Sanger sequencing
The target genomic region was amplified from the genomic DNA using Q5® Hot Start High-Fidelity 2X Master Mix (New England Biolabs, Ipswich, MA, United States) using the primers listed in Supplementary Table S4. The PCR products were purified using the QIAquick PCR Purification Kit (28104, QIAGEN). Sanger sequencing was performed at the Center for Applied Genomics (Toronto, ON, Canada), and the data were analyzed using DECODR software. 24
Enzyme-linked immunosorbent assay
Culture media and bronchial wash samples were applied to an enzyme-linked immunosorbent assay (ELISA) plate. Snap-frozen tissue samples were homogenized in lysis buffer (10 mM HEPES pH7.9, 10 mM KCl, 0.1 mM ethylenediamine tetraacetic acid, 0.1 mM ethylene glycol-bis(beta-aminoethyl ether)-N,N,N',N'-tetra acetic acid, 0.6% Nonidet P-40 with a protease inhibitor cocktail) using TissueLyser II (QIAGEN) and subjected to protein concentration measurement with a bicinchoninic acid Protein Assay Kit (23227, ThermoFisher Scientific), according to the manufacturer’s instructions. The ELISA kits used for cytokine detection were as follows: human IL-10 in in vitro study (BMS215HS, ThermoFisher Scientific), human IL-10 in EVLP study (D1000B, R&D Systems, Minneapolis, MN), human tumour necrosis factor alpha (TNF-α) (DTA00D, R&D Systems), and rat IL-10 (BMS629, ThermoFisher Scientific).
Wet-to-dry weight ratio
The weight of lung tissues was measured before and after drying at 65°C for 72 h. The ratio was calculated as the weight of the fresh tissue divided by the weight of dried tissue.
Histology
Formalin-fixed tissues were processed and embedded in paraffin. Thin sections were cut and stained for hematoxylin and eosin and terminal deoxynucleotidyl transferase dUTP nick-end labeling at the Pathology Core of Spatio-Temporal Targeting and Amplification of Radiation Response (STTARR, Toronto, ON, Canada) at the UHN. Bright-field images were obtained using a slide scanner (APERIO CS2, Leica Biosystems).
Next-generation sequencing
The next-generation sequencing was performed to analyze editing efficiencies. The target genomic locus was PCR-amplified from 100 ng of genomic DNA using Q5® Hot Start High-Fidelity 2X Master Mix (New England Biolabs, Ipswich, MA, USA). PCR amplicons were purified using magnetic beads (Sera-Mag SpeedBeads™ Carboxyl Magnetic Beads, Cytiva). The primers used for the PCR amplification were listed in Supplementary Table S4. Adaptors and indices (TruSeq DNA UD Indexes v2; Illumina, San Diego, CA, USA) were ligated in library preparation using TruSeq Nano DNA kit (Illumina). The library was validated and sequenced on the MiSeq Reagent Nano Kit v2 300-cycles (MS-102–2002; Illumina). A 15–20% volume of PhiX was spiked in to increase the diversity of the library. Paired-end readings (150 bp) with a target depth of 3,000–10,000 reads per sample were obtained at the Center for Applied Genomics. The data were analyzed using CRPSPResso2 software. 25
Fluorescence in situ hybridization
Fluorescence in situ hybridization was performed at the Pathology Core of STTARR at UHN using RNAscope® Multiplex Fluorescent Reagent Kit v2 (323100, Advanced Cell Diagnostics, Newark, CA, USA) in combination with Opal 520, Opal 570, and Opal 690 (FP1487001KT, FP1488001 KT, and FP1497001KT, Akoya Biosciences, Marlborough, MA, USA). The probes were custom designed to specifically detect rat IL-10 messenger RNA (mRNA) and human exogenous IL-10 mRNA targeting the unique sequence in each transcript. An in-stock probe was used for SaCas9 (501621, Advanced Cell Diagnostics). The images were obtained using a fluorescent scanner (Zeiss AxioScan; Leica Biosystems) with a 20× objective lens at the UHN Advanced Optical Microscopy Facility (AOMF) (Toronto, ON, Canada).
Statistics
Data were displayed as mean ± standard deviation (SD) and analyzed using the Prism software (GraphPad Software, San Diego, CA, USA). An unpaired two-tailed Student’s t-test or one-way analysis of variance (ANOVA) followed by Bonferroni’s correction was used to analyze significance.
RESULTS
Genome editing of a regulatory element led to upregulation of IL-10
We first explored CRISPR genome-editing approaches to consistently upregulate an immunomodulatory gene in the whole organ. We selected the IL-10 gene, which encodes an anti-inflammatory and immunomodulatory cytokine, as one of the target genes for graft immunomodulation. Previous work demonstrated that the delivery of the IL-10 gene to the donor lung via AdV before implantation improved early graft function post-transplantation. 26 A limitation of this approach, however, is the short duration of transgene expression, lacking the ability to provide sustained immunomodulation. Therefore, we aimed to induce long-lasting IL-10 expression in the donor lung by altering the host genome.
To achieve significant editing in the organ, we sought to optimize CRISPR nuclease methods that can be achieved by simple delivery of the editing enzymes. We hypothesized that targeted mutagenesis of the IL-10 regulatory element could disrupt native repressor binding, leading to enhanced transcription through a derepression mechanism, as IL-10 expression is normally suppressed at a steady state. 27
Using SaCas9 nuclease and a series of gRNAs, we introduced targeted DNA double-strand breaks (DSBs) that led to insertion or deletion mutations (indels) in the cis-regulatory region of the human IL-10 gene and assessed their impact on IL-10 expression in HEK 293 cells (human kidney cell line, Fig. 1A). Targeted mutagenesis at regions 85-(nts) upstream of the transcription start site significantly enhanced human IL-10 expression (Fig. 1B) with an editing efficiency of 15.3% ± 9.6% (analysis using Sanger sequencing). The −85 locus lies within a region with a promoter-like signature. This approach also led to the upregulation of endogenous IL-10 in rat and porcine cell lines, two species used for animal studies in the translational path, using the gRNA that upregulated IL-10 in the dSaCas9-VPR system 23 or phenotypic screening, respectively (Fig. 1C).

Genome editing of the regulatory region upregulated IL-10 in vitro.
A dual mode of IL-10 expression by combining AdV-IL-10 delivery with genome editing
We aimed to develop a method that would allow for both early and sustained IL-10 expression with a single intervention. Early ischemia-reperfusion-induced injury causes primary graft dysfunction, limiting short-term lung graft outcomes, and importantly is associated with chronic lung allograft dysfunction and rejection. Therefore, addressing both early and later graft injuries could enhance the therapeutic impact of long-term graft immunomodulation. Viral vectors have shown promise for in vivo delivery of editing enzymes, 28 but genome editing and subsequent transcriptome alterations often take days, exceeding the window available for preimplantation donor organ modulation. 29,30 To achieve immediate intragraft immunomodulation postimplantation, we combined CRISPR genome editing with AdV-mediated IL-10 cDNA delivery. This dual mode of IL-10 expression (Supplementary Fig. S1A) is designed to induce initial rapid and transient IL-10 expression from the exogenous human IL-10 gene delivered by AdV, followed by induction of long-lasting endogenous IL-10 expression facilitated by CRISPR genome editing.
We developed a plasmid vector encoding the human IL-10 cDNA, SaCas9, and the gRNA targeting the −85 region of human IL-10 for AdV production. Both the exogenous human IL-10 and SaCas9 expressions were driven by a single promoter using a 2A peptide to express all three components from a single vector. In vitro assessment of this approach using plasmid vectors confirmed exogenous human IL-10 expression, genome editing, and endogenous human IL-10 upregulation (Supplementary Fig. S1B, C, and D). We then developed AdVs (AdV-hIL10-CRISPR) using this construct for testing in human lungs.
Evaluating CRISPR-based IL-10 modulation in ex vivo perfused human donor lungs
We next sought to assess CRISPR genome editing in ex vivo perfused human lungs, simulating preimplantation donor organ modulation. To investigate genome editing in human donor lungs, we sought to deliver editing vectors to human lungs during EVLP and generate tissue slices from the treated lungs using PCLS technologies to achieve observation beyond the duration of ex vivo perfusion. We first validated this protocol by assessing viability and transgene expressions in PCLS, which were generated after ex vivo treatment of the human lung (Fig. 2A). We perfused the whole human donor lung, which was declined for clinical transplantation, using a modified Toronto EVLP system 22 and selectively delivered AdV, which carry human IL-10 cDNA, SaCas9, and the gRNA, to the left lung. Viability assay using resazurin (Fig. 2B) and calcein AM staining (Fig. 2C) demonstrated retained viability of post-EVLP PCLS for at least 14 days. The PCLS from the treated left lung exhibited positive staining for Cas9 mRNA (Fig. 2D) and secretion of human IL-10 protein to the culture media (Fig. 3E), demonstrating the transgene expression.
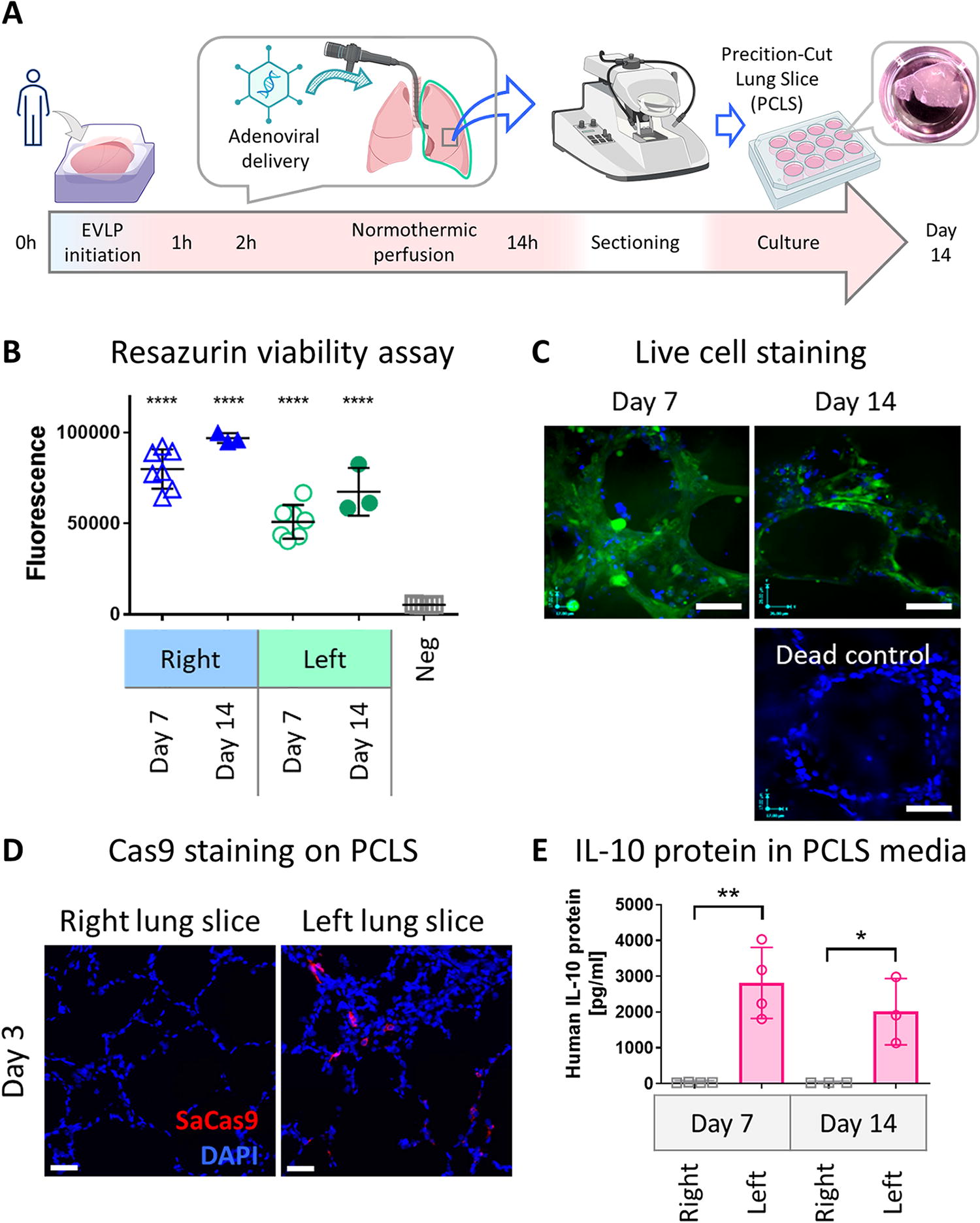
Viability and transgene expressions in PCLS generated after EVLP.
Evaluating genetic engineering in ex vivo perfused human donor lung.
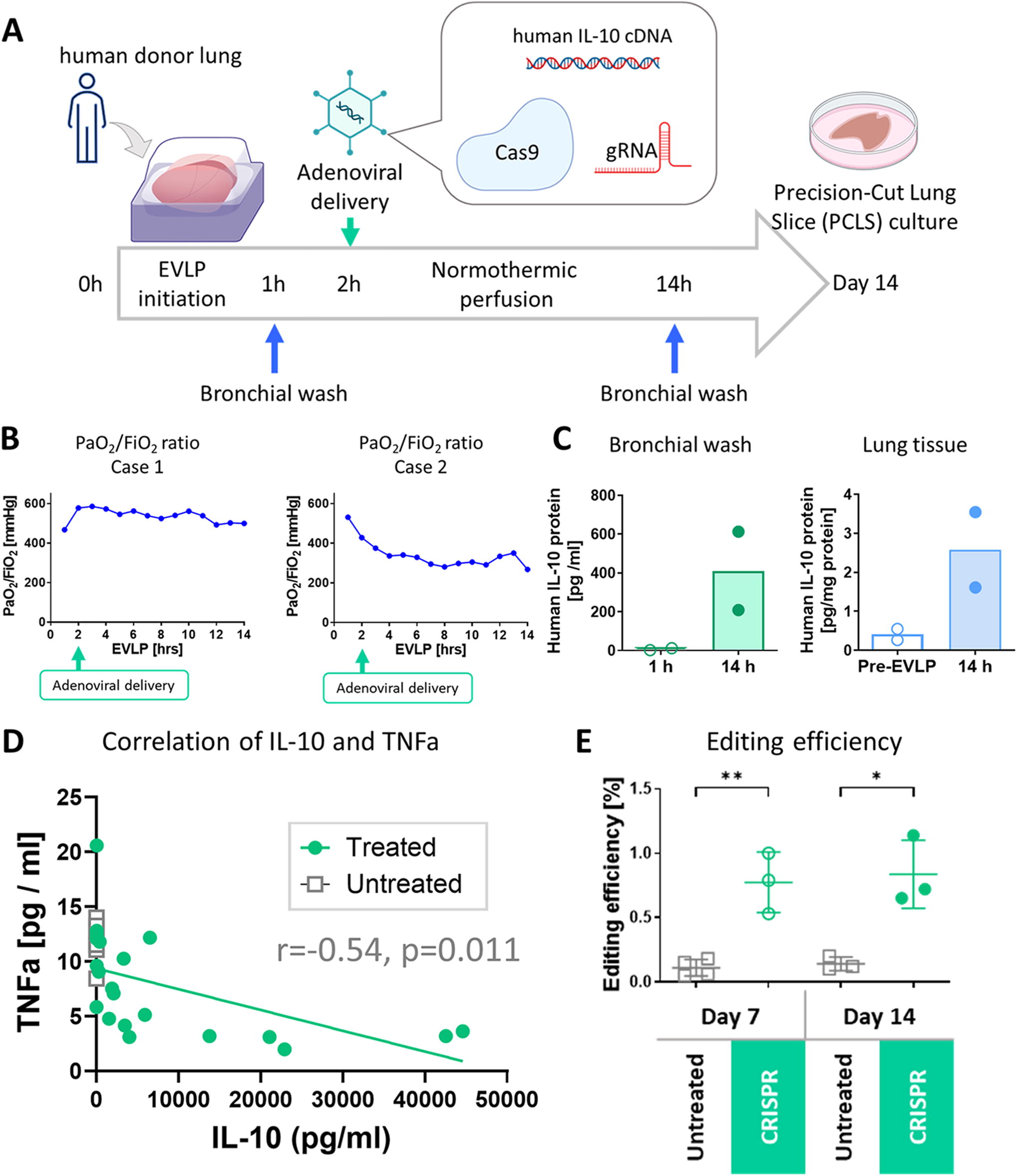
Building on these findings, we divided human lungs from two donors and perfused individually using distinct circuits (Supplementary Table S1), a design that allows for assessment of the intervention minimizing the impact on the untreated lung. The lungs were then perfused for 12 h post-intervention, a standard duration for EVLP studies, followed by PCLS culture for 14 days (Fig. 3A).
In both cases, the lungs were stably perfused for 12 h following the delivery of editing enzymes and human IL-10 cDNA (Fig. 3B). The treated lungs showed an increase in IL-10 protein levels in the bronchial wash and lung tissue (Fig. 3C) during the 12 h post-intervention perfusion period, whereas the untreated lung from Case 1 showed no increase in IL-10 protein (18.4 pg/mL at 1 h vs. 17.6 pg/mL at 14 h for bronchial wash, 0.97 ± 0.44 pg/mg protein at 14 h for tissue, respectively). IL-10 protein levels in PCLS media varied among slices prepared from different lung regions, likely due to heterogeneous vector distribution after non-aerosolized delivery (Supplementary Figure S2). Most of the PCLS from the treated lungs exhibited higher production of IL-10 protein on day 7 that was negatively correlated with the levels of TNFα (Fig. 3D). Analysis of the genomic DNA of the PCLS with high IL-10 production using next-generation sequencing detected significant editing in the treated group on both days 7 and 14 compared with the untreated group (0.77% ± 0.24% and 0.84% ± 0.27% in the treatment group vs. 0.11% ± 0.06% and 0.14% ± 0.053% in the untreated group; p = 0.0027 and 0.011 on day 7 and day 14, respectively; Fig. 3E). These findings demonstrate the feasibility of evaluating genome-editing interventions in human lungs using ex vivo organ perfusion and precision-cut tissue slices.
In vivo rat study for assessment in short- and long-term effects in the whole-body system
Although ex vivo assessment in human organs provides a direct means of evaluating interventions in organs of the target species, two significant limitations need addressing: the absence of the body system and the limited follow-up period. To overcome these, we conducted an in vivo study using a rat model. We developed an AdV that expresses human IL-10, SaCas9, and gRNA designed to target the regulatory region of rat IL-10.
In vitro assessments using AdV transduction of a rat cell line (L2) demonstrated a sequential progression of human IL-10 expression, genome editing, and subsequent upregulation of rat IL-10 (Fig. 4A and 4B), representing transgene expression and genetic and phenotypic alterations, leading to sustained IL-10 induction in the edited cells (Fig. 4C and 4D).
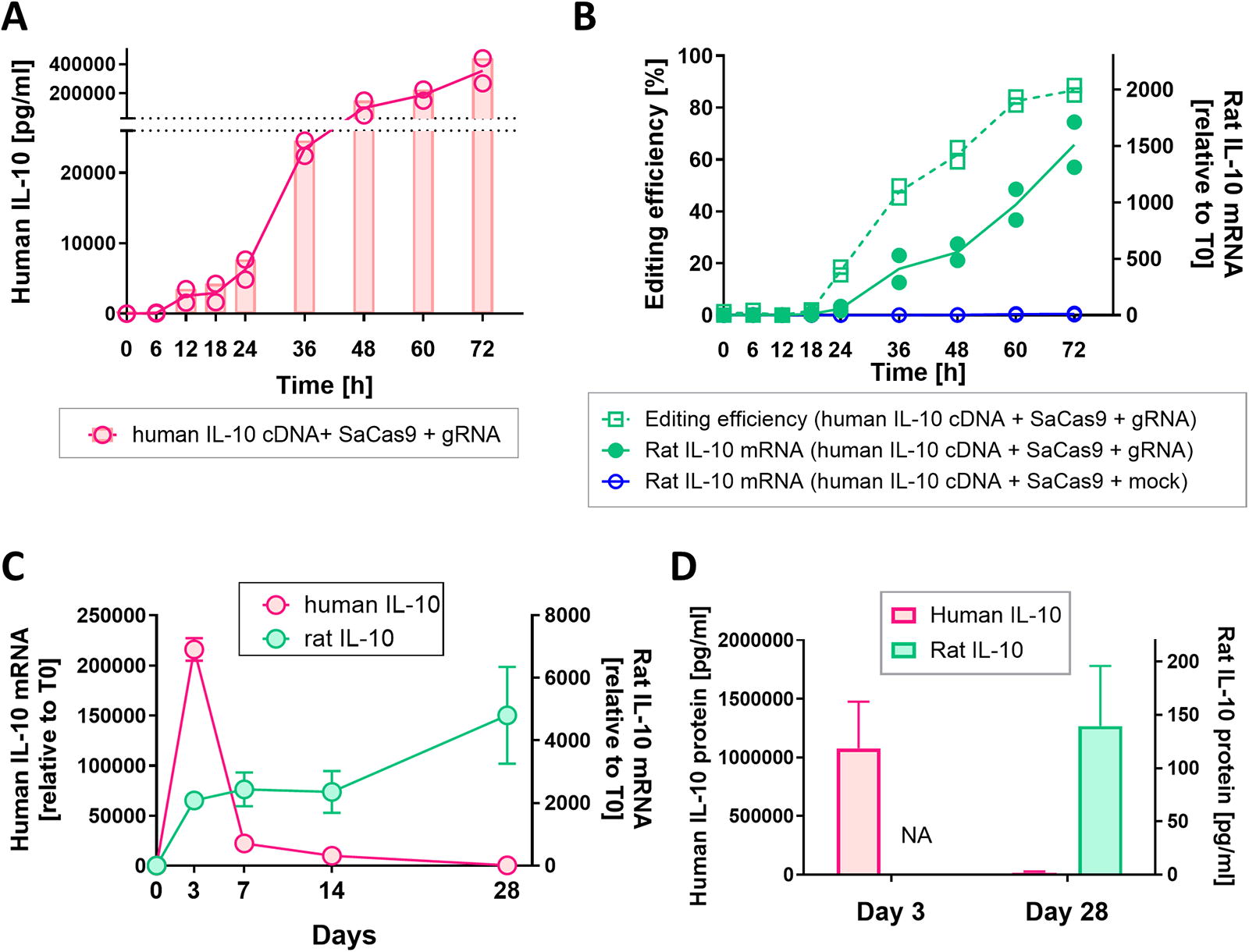
A dual mode of IL-10 expression after single dosing of adenoviral vectors in rat lung cells. L2 cells were transduced with adenoviral vectors, which express human IL-10, SaCas9, and gRNA, at a multiplicity of infection (MOI) of 1100. The culture media and cell lysate were collected at each time point. The IL-10 protein levels in the media and mRNA levels in cell lysate were measured by ELISA and RT-qPCR, respectively. In RT-qPCR analysis, relative expression to the start time (T0) is shown. Genome editing efficiency was analyzed by Sanger sequencing.
The AdV-hIL10-CRISPR was next delivered to the rat lung in vivo through the airway (Fig. 5A). The same clinical triple immunosuppression regimen used in our previous work, 23 consisting of cyclosporine, azathioprine, and methylprednisolone, was applied to mitigate inflammation after AdV-mediated delivery of Cas enzymes to the lung. Analysis of human IL-10 and SaCas9 expression in lung tissue revealed a time-related increase during the initial 3 days, followed by a steep decline by day 5 (Fig. 5B). Human IL-10 protein levels in the lung tissue exhibited an early increase, peaking between day 1 (124 ± 4.76 pg/mg protein) and day 3 (115 ± 4.56 pg/mg protein), followed by a rapid reduction (Fig. 5C). Notably, SaCas9 expression on day 3 was not significant in other tissues, such as the heart, liver, kidney, and spleen, indicating lung-selective transgene expression after trans-airway delivery (Supplementary Fig. S3A). Next-generation sequencing demonstrated a time-dependent increase in editing during the initial 5 days, reaching 2.52% ± 0.26% editing on day 5 (p < 0.0001 vs. the diluent control, Fig. 5D). The population of edited cells persisted for at least 28 days (3.84% ± 2.11%, p = 0.0048 on day 7, 1.78% ± 0.21%, p < 0.0001 on day 14, and 1.97% ± 0.46%, p < 0.0001 on day 28, Fig. 5D). Enhanced rat IL-10 mRNA levels were detected from after day 3 (Fig. 5E), showing the levels of rat IL-10 protein in the lung tissue of 30.1 ± 7.1 pg/mg protein on day 7, 42.8 ± 8.5 pg/mg protein on day 14, and 39.6 ± 6.3 pg/mg protein on day 28 (mean ± SD, n = 4 or 5). In situ hybridization of lung tissue on day 14 revealed an enhanced signal of rat IL-10 mRNA in a portion of Cas9-expressing cells (Fig. 5F), supporting IL-10 upregulation in edited cells in the lung. The treated lungs exhibited no signs of injury, with comparable wet-to-dry ratios (Supplementary Fig. S3B), a measure of lung edema, systemic PaO2:FiO2 ratio (Supplementary Fig. S3C), an indicator of oxygenation capability, and histology (Supplementary Fig. S3D) to the untreated control.

Assessment of genome editing combined with human IL-10 cDNA delivery in vivo using a rat model.
In summary, our in vivo study demonstrated that the concurrent delivery of human IL-10 cDNA and editing enzymes through a single dose of AdV can achieve early gene expression (IL-10 increase) and durable editing in lung tissue.
DISCUSSION
In this proof-of-concept study, we have successfully demonstrated the feasibility of genome editing in human lungs ex vivo. Preclinical assessment of in vivo genome-targeting therapeutics presents unique challenges rooted in interspecies genomic differences. Typically, the development of therapeutic editing begins with designing approaches targeting the human genome. However, for animal studies, gRNA and vectors must be customized for individual species. In the case of using wild-type animals recapitulating application in human, the genomic loci corresponding to the human targets are identified, and a distinct gRNA is designed based on the genomic DNA sequence of the animals. However, achieving genetic and biological identity between animals and humans using the same editing enzymes is a significant challenge. Studies using ex vivo human organs offer a direct means of assessing human-targeted editing in the intended species, bridging the gap between in silico, cellular, preclinical animal analyses and clinical trials (Fig. 6). With the recent modification of the Food and Drug Administration’s approval requirements in the United States, 31 providing for the potential avoidance of the need for animal studies, preclinical assessments using ex vivo perfused human organs are expected to gain importance.

New modalities for future translational path of genome-targeting therapeutics. Studies using ex vivo perfused human organ facilitate direct evaluation of human genome-targeting interventions in the organs of target species, overcoming the current translational gap.
Although genome editing demands long-term observations, the lack of suitable transplant models presents a challenge for extended follow-up of treated human organs. In this study, we incorporated PCLS culture technology, allowing us to monitor interventions in live lung tissue for 14 days. This integration of tissue culture techniques provided an excellent model for extended assessment of human genome editing, a previously unestablished endeavor. Furthermore, we conducted an in vivo study using a rat model to address three key aspects that are challenging to achieve in ex vivo human lung studies: (1) in vivo profiling, (2) monitoring beyond 14 days, and (3) data collection from a larger sample size. Human lungs available for research purposes declined for clinical transplant but in an acceptable condition are scarce compared with animals. Therefore, a multimodal approach that combines in vivo animal studies and ex vivo studies using human organs enabled the overall gain of a more comprehensive understanding of intervention impacts with mechanistic insights. Ongoing efforts to extend perfusion periods using modified perfusion system 32,33 and cross-circulation, 34,35 as well as the development of ex vivo human lung injury models using human plasma, 15 and an emerging human decedent model 36,37 hold the promise of further expanding the potential for preclinical assessment in the human organ.
In this study, we discovered that genetic disruption of a regulatory element enhances IL-10 expression. Gain-of-function genome editing often faces the challenge of low-efficiency DNA integration, 38,39 which limits its application to entire organs. However, the derepression approach offers a solution, achievable through simple editing methods such as generating DSBs using Cas nucleases and introducing base substitutions with base editors. These highly efficient editing techniques significantly increase the success rate of therapeutic organ editing. Potential strategies to release natural repression include (1) reducing the binding affinity of the repressor by perturbing the regulatory element, (2) reducing repressor expression, and (3) recapitulating single nucleotide polymorphism (SNPs) associated with the desired phenotype. For the IL-10 gene, the mechanism of its native repression remains unknown, prompting us to identify target loci through phenotypic screening. The region we identified does not overlap with known repressor candidate-binding motifs 40 –43 or putative silencers. 44 In addition, the region targeted in this study differs from three SNPs in the regulatory region of the IL-10 gene, namely, −592 (rs1800872), −819 (rs1800871), and −1082 (rs1800896), which are associated with elevated IL-10. 45 Therefore, to the best of our knowledge, the regulatory element edited in this study represent previously unexplored regions. Further investigations, such as high-throughput screening, would greatly support deciphering the molecular basis of IL-10 regulation. The editing efficiency we observed in lung tissue is comparable with the transduction efficacy following AdV delivery to the lung via the airway. IL-10 enhances immunomodulatory function through both paracrine and autocrine mechanisms, indicating that even a small population of edited cells could yield therapeutic benefits for graft immunomodulation. Further optimization of transduction efficiency, potentially using AAV or non-viral delivery methods, as well as fine-tuning IL-10 upregulation at the cellular level by refining the editing approach, and enhancing editing efficiency, such as using base editors for more uniform mutations, 46 would allow more precise control of IL-10 levels in the graft.
CONCLUSION
In this study, we successfully developed a genetic engineering approach for lung graft immunomodulation and demonstrated genome editing in human lungs ex vivo using organ perfusion and tissue culture technology. Our results underscore the exciting potential of using ex vivo human organs to preclinically evaluate genome-targeting and possibly other pharmaceutical interventions, thereby addressing a significant translational barrier.
Footnotes
ACKNOWLEDGMENTS
The authors thank STTARR at UHN for performing in situ hybridization and histological staining, the Center for Applied Genomics and Princess Margaret Genomics Center for next-generation sequencing, AOMF at UHN for image analysis, the Flow Cytometry Facility at the Hospital for Sick Children (SickKids) and the UHN for cell sorting, and SIRION Biotech for producing AdVs. Scientific inputs from scientists and colleagues of the Latner Thoracic Research Laboratories and Toronto Lung Transplant Program at UHN are acknowledged. K.M. was supported by UHN Transplant Competition 2020, University of Toronto’s Institute of Medical Science Open Fellowship 2020–2023, and Canadian Society of Transplantation Research Training Award 2022. B.P.K. acknowledges support from an MGH Executive Committee on Research Howard M. Goodman Fellowship and National Institutes of Health DP2-CA281401. The authors thank Catherine Zhang for creating the schematic of EVLP and the cover art. Other illustrations were created using BioRender.com software.
AUTHORS’ CONTRIBUTIONS
K.M. and S.K. conceptualized the project. K.M. performed experiments, analyzed data, and wrote the article under the supervision of S.K. S.J., J.H., A.R.D., and S.K. guided the study through program advisory committee meetings of University of Toronto graduate program. K.M., H.Y., and A.M. conducted human lung study with the help of the Toronto EVLP team. J.Y., A.A., and G.W.W. supported next-generation sequencing. Z.G., Y.Y., H.M., and C.D. provided technical assistance in experiments. A.W., M.C., and M.L. guided the study through discussion at the meetings and supported article writing. B.P.K. advised on genome editing approaches and next-generation sequencing analyses. The article was reviewed by all authors.
AUTHOR DISCLOSURE
M.C. and S.K. are co-founders of Perfusix Canada and Scientific Advisors to Lung Bioengineering. S.K. is CMO of Traferox Technologies. UHN has a patent filed and pending for technologies related to donor organ modification, on which K.M., S.J., M.C., M.L., and S.K. are inventors. S.K. and M.C.’s interests were reviewed and are managed by UHN in accordance with their conflict-of-interest policies. A.R.D. is on the Scientific Advisory Board of Acrigen. B.P.K is an inventor on patents and patent applications filed by Mass General Brigham that describe genome engineering technologies. B.P.K. is a consultant for EcoR1 capital and is a scientific advisor to Acrigen Biosciences, Life Edit Therapeutics, and Prime Medicine. B.P.K. has a financial interest in Prime Medicine, Inc., a company developing therapeutic CRISPR-Cas technologies for gene editing. B.P.K.’s interests were reviewed and are managed by MGH and MGB in accordance with their conflict-of-interest policies.
FUNDING INFORMATION
This work was supported by the UHN Foundation, New Frontiers in Research Fund—Transformation Grant (NFRFT-2020-00787), and the Canadian Institutes of Health Research (CIHR PJT-173392).
SUPPLEMENTARY MATERIAL
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.