
Abstract

SUMMARY OF THE GM2 EXTERNALLY LED PATIENT-FOCUSED DRUG DEVELOPMENT MEETING
Executive summary
GM2 gangliosidosis (Tay-Sachs and Sandhoff diseases) is a rare condition that steadily destroys nerve cells in the brain and spinal cord. Patients with GM2 lose fundamental abilities such as mobility, speech, and swallowing. GM2 imposes an incalculable burden on the patient and the family as it requires constant vigilance and upends every aspect of their lives while inflicting severe physical, emotional, and mental tolls. The childhood forms of GM2 are fatal, while the late-onset form in adults has progressively debilitating physical and mental health impacts.
There are no FDA-approved treatments that target the underlying cause of GM2. While a cure is the ultimate goal, the GM2 community would welcome any treatment that could help preserve even the most fundamental functions, such as the ability for a child to smile or hold their parent’s hand or for an adult to walk without a constant fear of falling. To achieve that, parents of young children with GM2 and adults living with late-onset GM2 are willing to take greater risks in drug development in the hopes of improving their daily functioning, as the quality of life was deemed much more important than merely extending survival.
On February 15, 2024, the National Tay-Sachs & Allied Diseases Association (NTSAD) convened an Externally Led Patient-Focused Drug Development (EL-PFDD) meeting on GM2. The goal of this meeting was to enable the FDA and other important drug development stakeholders to hear firsthand from patients and caregivers about their journey with Tay-Sachs and Sandhoff diseases and what would be the most meaningful for patients in terms of future treatments. The expert presentations, patient and caregiver video stories, panelist discussions, caller remarks, meeting polling data, and comments submitted online during and after the meeting provided the content for this “Voice of the Patient” report.
Key meeting themes
Testimonials throughout the meeting painted a clear picture of the devastation caused by GM2. While the different onsets of GM2 (infantile, juvenile, and adult) vary in their symptoms, impact, and outcomes, several common themes emerged, as noted below and explored throughout the report. GM2 gangliosidosis, known as Tay-Sachs and Sandhoff diseases, is a rare neurodegenerative condition that is fatal in children (infantile/juvenile form) and progressively disabling in adults (late-onset form). Children with the infantile onset form of GM2 do not typically live past 5 years of age, while those with juvenile onset can survive into adolescence. Adults living with the late-onset form of GM2 may experience worsening physical limitations and potential impacts on their mental health, ranging from anxiety/depression to psychosis, all of which compromise their ability to live independently. Patients with GM2 endure a heartbreaking journey marked by relentless disease progression that strips away abilities they once had, including their capacity to walk, talk, and eat. Parents watch in agony as their children who appear at first to be healthy and thriving, regress as they lose basic abilities and miss developmental milestones. Adults living with late-onset GM2 confront a continuous and frustrating decline in their capabilities, with a constant dread of the next fall, further loss of function, or mental decline. GM2 is all-consuming for the patient, caregiver, and family as a whole, with patients often entirely dependent on others for every aspect of daily life. Parents of young children described the intense nature of GM2, which requires constant vigilance and upends every aspect of their lives. Adults living with the late-onset form of GM2 fear further decline and what that means for their ability to care for themselves or others. There are no FDA-approved treatments that can alter the cruel course of GM2, which is fatal in children and life-altering in adults. Parents are powerless to help their children who face a “death sentence.” Every day that passes without a disease-modifying treatment, patients lose more and more of their abilities, robbing them of precious moments with loved ones and chipping away at their quality of life. Although the hope is for a cure, parents and patients would be grateful for a treatment that slows or halts disease progression to preserve basic abilities, such as communicating clearly, holding the hand of a loved one, walking with minimal assistance, or eating independently. Parents of young children and adults living with GM2 are willing to take on greater risks to improve their daily functioning, noting that quality of life matters more than merely extending survival.
A treatment that offers small gains or marginal improvements would be a lifeline for the GM2 community, providing hope in the face of overwhelming daily challenges.
INTRODUCTION
The Externally Led Patient-Focused Drug Development (EL-PFDD) meeting on GM2 gangliosidosis (Tay-Sachs and Sandhoff diseases) was held on February 15, 2024. The EL-PFDD initiative by the U.S. FDA emerged from the realization that the firsthand experiences of patients, caregivers, and families provide vital insights that can inform the development and evaluation of new therapies.
The information gathered at the meeting and summarized in this report may guide therapeutic development and inform the FDA’s evaluation of potential therapies that address GM2. Involving patients and families in the drug development process can help bring to light what matters most for those affected with rare diseases such as GM2. The hope is that this information will help fuel the development of new treatments, accelerate their approvals, and ultimately improve the lives of those impacted by these diseases, which cause untold heartbreak and devastation.
The EL-PFDD meeting was organized by NTSAD, one of the oldest advocacy organizations in the United States for rare genetic diseases, founded nearly 70 years ago. NTSAD puts family support at the cornerstone of its mission while also nurturing community, cultivating collaborations, and advancing research.
GM2 GANGLIOSIDOSIS (GM2): TAY-SACHS AND SANDHOFF DISEASES
GM2 is a rare life-limiting lysosomal storage disorder. Lysosomes house specific enzymes responsible for breaking down and recycling molecules within the body. GM2 is caused by a mutation in either the HEXA gene (associated with Tay-Sachs) or the HEXAB gene (linked to Sandhoff disease), impairing the β-hexosaminidase enzyme from breaking down and recycling gangliosides within the body’s cells. As a result, toxic gangliosides accumulate in the cells and tissues, resulting in progressive damage primarily affecting nerve cells in the brain and spinal cord and leading to eventual death of the cells. Tay-Sachs and Sandhoff diseases are inherited in an autosomal recessive pattern, meaning that an affected child has received one altered copy of the gene from each of their parents.
There are no FDA-approved treatments that address the underlying disease. Treatments for symptoms include anticonvulsants (for seizures), muscle relaxers (for spasticity), gastric tube placement (for aspirations and nutrition when a child can no longer eat by mouth safely), antibiotics (for infections), and others.
GM2 is ultra-rare, affecting fewer than an estimated 1,000 people in the United States (based on NTSAD-recorded cases), with the infantile form the most common. Although originally believed to exclusively affect individuals of Jewish descent, Tay-Sachs and Sandhoff diseases are now acknowledged as conditions that transcend ethnic boundaries. Tay-Sachs is more common than Sandhoff’s disease.
Infantile onset (3–6 months)
Elevated noise sensitivity, exaggerated startle, hypotonia (decreased muscle tone), developmental arrest, reduced vocalization, spasticity (stiff or rigid muscles), seizures, cherry-red maculae, diminished eyesight, as well as loss of the ability to sit, move the head side-to-side and reach for an object.
Only half of infantile patients gain the ability to sit independently, and all that gain the ability lose it within an average of 1 year.
Only half of patients survive to 3–4 years of age.
Juvenile onset (2–5 years)
Gait problems, speech difficulties, incoordination, intellectual deficits and delays, muscle weakness and wasting, feet deformities, incontinence, behavioral/psychiatric issues, feeding problems, seizures, visual problems, and more.
Clinical features are more heterogeneous compared to infantile GM2.
Late onset (adolescence and into adulthood)
Muscle weakness, particularly in antigravity muscles, increased falls, inability to rise from the floor, unstable walking, dysarthria (slurred speech), and sensory neuropathy.
Patients with late-onset GM2 have more variability in the age of onset and rate of disease progression than patients with infantile or juvenile onset.
Roughly 30–50% of adults with Tay-Sachs experience psychiatric symptoms throughout the course of the disease.
MEETING OVERVIEW
This meeting was designed to highlight the patient and caregiver perspectives of GM2 across both childhood and adult forms, notably the impact of disease symptoms on their daily lives, as well as their hopes for future treatments. Because of the vast differences between childhood disease (infantile and juvenile) and adult disease (late onset), the meeting was divided up accordingly with separate medical overviews, testimonials, and discussions (see agenda in Supplementary Appendix SA1).
The meeting began with opening remarks by co-moderator Kathleen Flynn, CEO of NTSAD. She highlighted the severe impact that GM2 has on quality of life, affecting children and adults in ways that can be difficult for those outside of the GM2 community to fully understand. With no FDA-approved treatments, the hope is that this meeting will inform the development and approval of treatments that are urgently needed.
Jacqueline Karp, MD, Division of Rare Diseases and Medical Genetics, Center for Drug Evaluation and Research (CBER), FDA, highlighted the importance of EL-PFDD meetings to integrate patients’ perspectives, needs, and priorities into drug development and evaluation. She reinforced the importance of identifying and measuring outcomes in clinical trials that matter most to patients and caregivers.
James Valentine, JD, MHS, who helped launch the PFDD program at the FDA, served as co-moderator, outlining the meeting format/guidelines and conducting demographic polling.
The morning session explored the impact of GM2 on daily life, featuring in-depth medical presentations on both the childhood and late-onset forms. These insights were provided by Florian Eichler, MD, Director of the Center for Rare Neurological Diseases at Massachusetts General Hospital and Cynthia Tifft, MD, PhD, Deputy Clinical Director and Senior Clinician at the National Human Genome Research Institute of the National Institutes of Health, respectively. The afternoon session on current and future treatment approaches, as well as the morning session, included prerecorded patient/caregiver panels, audience polling (by phone, computer, or tablet), and moderated discussions.
The meeting concluded with a summary provided by Larry Bauer, RN, MA, a former member of the FDA Rare Diseases Program, and closing remarks from Kathleen Flynn and James Valentine.
Members of the GM2 community were invited to submit written comments both during the meeting and in the 30 days following, which were incorporated into this report as possible (Figure 1).
A recording of this EL-PFDD meeting in its entirety may be found at https://ntsad.org/gm2pfdd
REPORT OVERVIEW
This “Voice of the Patient” report intends to support the FDA’s and other key stakeholders’ understanding of patients’ experiences, perspectives, and needs living with GM2, including the impact on daily living along with patient and caregiver desires for future treatments. The hope is that these firsthand insights may help inform drug development and evaluation, including identifying meaningful endpoints and outcomes used in clinical trials.
This report aims to summarize the input graciously provided by patients and caregivers during the EL-PFDD meeting and is not meant to represent in any way the views and experiences of any specific group of individuals or entities. There may be symptoms, perspectives, or other aspects of GM2 that are not included in the report.
INFANTILE/JUVENILE GM2: SYMPTOMS AND IMPACT ON DAILY LIFE
Parents shared heart-wrenching experiences of caring for children with infantile or juvenile GM2, the most severe forms of the disease. Although children with Tay-Sachs or Sandhoff disease may initially meet typical milestones, they can suffer developmental arrest and regression. Families grapple with a range of debilitating symptoms, numerous hospitalizations, and various surgeries. Constant demands of GM2 include administering daily medications to control seizures, performing suctioning to manage secretions, and facilitating movement to prevent muscle contractions. Disability and death are prominent features of infantile and juvenile Tay-Sachs and Sandhoff diseases.
CHILDREN LOSE BASIC ABILITIES AS THE DISEASE PROGRESSES
Many children with GM2 are born seemingly healthy, reaching developmental milestones and thriving. However, this picture drastically changes when symptoms of Tay-Sachs or Sandhoff disease appear and children start to miss milestones or lose abilities they once had. Parents described the anguish of witnessing their children decline.
Rick wrote about his daughter Krystie who died from Tay-Sachs at age nine, saying that “she was perfect” when she was born but that “the dark clouds of GM2” set in when Krystie started falling behind in her development around 9 months of age.
Wendy wrote about her 3-year-old son Victor who has infantile Tay-Sachs: “Victor’s diagnosis was devastating for us, but seeing the progress of his illness little by little is even more so, how he smiled less and less every day, how he stopped moving little by little, how we realized that his eyesight is getting worse and worse. How this damn disease is stealing our beautiful son from us little by little is really hard, the hardest and most painful thing in life.”
Mandy, mother of young daughters Mollie and Madelyn who both have juvenile Sandhoff disease, said that although their disease journeys were different, “what they had in common was that they went from walking to school to needing wheelchairs. They went from eating their favorite treats by mouth to needing feeding tubes. They went from talking full sentences to just making sounds and occasional laughter. And instead of continuing to go to soccer practice and dance class, they go to therapies.”
PARENTS MOURN THE LIFE THAT COULD HAVE BEEN
Parents express the heartbreak of seeing their child deprived of a typical childhood along with having their own dreams of raising a healthy child crushed by GM2. They describe their pain around losing out on everyday moments and milestones.
“My two-year-old never played at a park. He never had the chance to be a kid. Tay-Sachs took that opportunity away from him. It also took away my motherhood experience that I had envisioned for my life,” said Kim, who lost her young Greyson to Tay-Sachs just before his third birthday.
Rennie wrote about her 6-year-old daughter with juvenile Tay-Sachs: “We have mourned for who Chloe would have been in the future, but we continue to mourn our Chloe now, who she was just a few months ago, weeks ago, and even days ago, as we slowly see her skills and abilities deteriorate.”
CHILDHOOD GM2 CAN PRESENT WITH A WIDE RANGE OF SEVERE SYMPTOMS
Participants described an array of symptoms their children endure, including weakness, motor deficits, difficulty swallowing, cognitive delays, and developmental delays/loss of milestones (Figure 2). Other common symptoms include hypotonia, decreased responsiveness, exaggerated startle response, seizures, and more. Symptoms can also evolve over time, with one mother remarking that every new or worsening symptom significantly affected her son’s quality of life and emotionally taxed the entire family unit as they adapted to changes. A meeting poll revealed that the daily life activities most impacted by GM2 were the ability to move/walk, eat, and talk (Figure 3).

Meeting Participants by the Numbers.

Participants ranked the most troublesome GM2-related health concerns that their loved one has ever had (they were asked to select up to three topics).
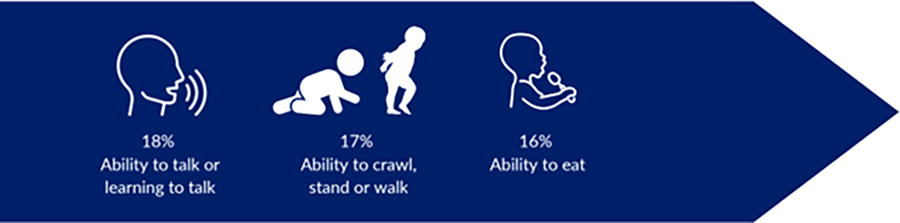
Participants selected the daily life activities that are important to their loved one that they are not able to do or struggle with due to GM2 (they were asked to select up to three topics).
DIFFICULTY SWALLOWING: A CONSTANT FEAR OF CHOKING, INFECTIONS AND MORE
Participants highlighted secretion management as a formidable challenge, with patients losing the natural ability to clear mucus from their airways and swallow on their own. This can result in liquid being aspirated into the airway, presenting serious respiratory risks such as infections, chronic coughing, and breathing difficulties. Parents also highlighted the substantial burden caused by continuous care required to manage secretions.
Crystal, mother to 4-year-old Cayden who passed away from infantile Sandhoff disease, said: “Secretion management is our biggest struggle…. Suddenly, one day the suction machine started coming with us everywhere we go. It had gotten so bad to a point where we couldn’t even leave the house because suctioning had to be constant or worse, when you’re driving in the car, everything is fine at the beginning until you’re constantly having to pull over to suction and eventually turn around to go home.”
Abby, mother to 3-year-old son Levi with infantile Tay-Sachs, noted that “issues with swallowing, secretion management, shallow breathing, need to be addressed repeatedly throughout the day.”
UNABLE TO EAT: A MAJOR SETBACK FOR CHILDREN AND A COMPLEX ISSUE FOR PARENTS
Parents discussed the challenge of maintaining their children’s independent eating while ensuring adequate nutrition. They shared the grief of transitioning to an assistive feeding device for children who were once “great eaters,” a decision that can be devastating for parents.
Yasmina, mother to 11-year-old Lily with juvenile Tay-Sachs, shared that her daughter greatly enjoyed food, including pizza, candy, and chocolate, but “it was getting harder and harder for her to swallow, and she would spit out her food, and she started choking and aspirating. It just gets stuck in the wrong spot and the coughing, and it’s harder for her to cough as the symptoms, as the disease takes over.”
Jennifer said that her 12-year-old daughter Madelyn who has juvenile Sandhoff disease also loves food: “I want her to be able to still experience that, the flavors, holding onto food with her hand and getting it to her mouth, even if she can no longer use utensils. But when we go to her doctor appointments and they say, ‘Well, she hasn’t gained weight’…. you start questioning….you want her to be happy and enjoy everything in life that normal children get to enjoy, but you also want her to have a healthy body.”
ONGOING SEIZURES: A CONSTANT CONCERN FOR MANY CHILDREN WITH GM2
Seizures are a common symptom of childhood GM2, particularly in the infantile form. They are often difficult to manage and can significantly impact the quality of life of patients and their families.
“The level of her seizure activity was cumbersome… even with multiple medications over the span of her entire life, we were never truly able to really get that in line. Positioning, noise, movement, even things like wind or rain, all of that could affect her seizures,” said Becky, whose young daughter Elliott died from infantile Tay-Sachs.
Abby wrote about her son Levi with infantile Tay-Sachs that “seizures have been the most difficult symptom to control and have had the most disruptive effect on his quality of life.” Kaitlyn shared a similar sentiment, whose young son Phillip passed away from infantile Sandhoff disease and suffered from “multiple seizures a day, making it difficult to do simple activities.”
MOBILITY DECLINE: CHILDREN BECOME UNABLE TO SIT, STAND OR WALK WITHOUT ASSISTANCE
While other children, and in many cases siblings, are outside playing, running, and jumping, children with GM2 are often physically disabled, with many confined to a wheelchair and unable to take part in normal childhood activities. Although some babies with the infantile form may never have learned to walk, children with the juvenile form may have enjoyed years of being active before GM2 gradually stripped away their ability to move, step by step.
“Lily used to be the fastest little child. She could run like no other. She could jump and play, and she did ballet for a couple of years and gymnastics, and she loved to do somersaults. And then all of a sudden, we noticed it was harder for her to run. Then it slowly began harder for her to walk…slowly all the things that were just so natural to her became unnatural to her,” recalled Yasmina, mother to 11-year-old Lily with juvenile Tay-Sachs.
“Madelyn has gone from being able to walk independently to needing a walker to requiring the use of a wheelchair daily. She can no longer walk or stand unassisted,” said Jennifer, about her 12-year-old daughter with juvenile Sandhoff disease.
COMMUNICATION CHALLENGES: FRUSTRATED CHILDREN AND CONCERNED PARENTS
The inability to communicate effectively results in a child being frustrated that they cannot express their needs and wants, while parents worry that they are not correctly assessing their pain or comfort levels. Providing care becomes particularly challenging once their child becomes (or remains) nonverbal. This necessitates an acute awareness of subtle clues to understand their needs, something that is often borne solely by the primary caregiver, as others may not as easily recognize these nuances.
“His regressed speech made the biggest impact. It started getting harder for him to get his words out,” said Kelly, whose 8-year-old son lives with juvenile Tay-Sachs. “Kipley mostly talks with one-word phrases, which is so sad because I have videos of him speaking clear and with sentences at a much younger age.”
“I think one of our things that we always worried about was her being able to communicate that pain level or the pain and what was going on,” said Nate, whose young daughter Olly Belle died from infantile Tay-Sachs. “I can’t tell you the number of times that the nurses would come in, especially early in her first hospital stay and ask, “Does she look like she’s in pain? What do you think? How do you think she feels right now?””
VISION LOSS AND BLINDNESS: CHALLENGES IN EARLY DETECTION
Several parents shared the challenges in recognizing vision loss in infants or nonverbal children affected by GM2. These children might have appeared aloof, disinterested in visual tasks, or discomfort due to other symptoms, leading their parents to initially overlook the possibility of vision impairment. Only upon careful reflection did these parents come to grasp the reality of their child’s vision loss.
Aaron, who lost his daughter Annabella to juvenile Tay-Sachs just after her fifth birthday, recalled: “I remember when she was very young, she had good eyesight and she liked to watch people. We didn’t find out she lost her eyesight until the last five months…She was just kind of staring off into space and we’d have her watch her favorite shows, but then I noticed she wasn’t really looking at the TV anymore.” Nate shared similar challenges in assessing vision loss with his daughter Olly Belle who also died from infantile Tay-Sachs.
RESPIRATORY ISSUES: CHALLENGES AND COMPLICATIONS
Respiratory issues present significant challenges and complications, impacting daily life and requiring constant vigilance and intervention. Families talked about coping with the demands of respiratory therapies and hospitalization, as well as facing hurdles in travel and managing necessary equipment to ensure their loved ones’ well-being.
COGNITIVE AND BEHAVIORAL ISSUES: CHILDREN STALL OR REGRESS IN THEIR ABILITIES
Children affected by GM2 may experience developmental delays, intellectual disability, behavioral challenges, and regression in skills they’ve already acquired.
“It has greatly impacted his learning abilities. In his last evaluation, he was functioning at three months old at the age of three years old,” said Kate about her 3-year-old son Felix with Tay-Sachs.
Kelly, whose 8-year-old son Kipley lives with juvenile Tay-Sachs, noted that he has been most affected by cognitive decline, particularly struggling in public settings where he “displays inappropriate behaviors,” often running and yelling with no regard to his surroundings or safety in addition to having “extreme emotional swings.”
CAREGIVING IS ALL-CONSUMING AND UPENDS EVERY ASPECT OF DAILY LIFE
Caregivers expressed the multitude of challenges when caring for a child with GM2. Managing fundamental necessities like eating, dressing, and toileting, as well as navigating numerous medical appointments and therapy sessions, is just the beginning. They face ever-evolving symptoms and care needs for their child, particularly challenging when children are nonverbal and are unable to ambulate independently.
“It really did truly affect our daily functioning and daily life for all of us … she needed 24-hour, very specialized care,” said Becky, whose daughter Elliott passed away from infantile Tay-Sachs. “Just navigating very small tasks that one may not think about otherwise were quite the challenge for us in many, many ways when caring for our daughter.”
Lorelei, mother to 13-year-old son Isaac with infantile Tay-Sachs, who had a stem cell transplant at 10 months old, said: “He doesn’t communicate verbally or directly with any communication device. We have to read him, we have to know with those little smiles or those little frowns or those little sounds if he’s happy or uncomfortable.”
PARENTS FEAR FOR THE FUTURE AND BRACE THEMSELVES FOR THE INEVITABLE LOSS
Without any treatments to slow the relentless progression of GM2, parents feel powerless as they witness their children’s decline. A meeting poll showed that the number one concern about the future is that their children’s symptoms will get worse (see Supplementary Appendix SA2). They grapple with worry over worsening symptoms or new manifestations, all while facing the inevitable outcome of the disease.
“I’m most afraid of what will happen next, the move to a feeding tube, the fact that she may become non-verbal or have seizures. Can you imagine knowing that your child will never say the words ‘I love you’ ever again, that instead they’ll be trapped inside of their body, a slave to this horrible disease?” said Jennifer, mother of 12-year-old Madelyn with juvenile Sandhoff disease.
“I can vividly remember tucking him in at night and saying, when you’re done, you go. When your body is done, you let go. Mommy and Daddy will survive, but you have to go when it’s your time. I should be reading him a bedtime story rather than having that conversation with him,” said Kim, mother to Greyson who died from infantile Tay-Sachs just before his third birthday.
LATE-ONSET GM2: SYMPTOMS AND IMPACT ON DAILY LIFE
Individuals with late-onset GM2 shared their experience with this progressively debilitating condition that is marked by a spectrum of symptoms, including extensive physical limitations. In addition, medical literature suggests that up to 50% of late-onset adults (more often late-onset Tay-Sachs) may develop severe psychiatric symptoms. The addition of the mental impact can result in isolation and further mental decline.
Unique to having GM2 over many decades, participants recounted experiences of symptom dismissal much earlier in their lives and enduring many years of misdiagnoses. Reflecting on the past, a patient shared that he felt bad about himself, saying, “I always felt that I was just out of shape and lazy, not knowing that it was Tay-Sachs, it was the problem.” Others echoed similar sentiments.
Living with late-onset GM2: Navigating daily challenges with careful planning
Many patients detailed the meticulous planning required to manage daily activities, reduce the risk of falls, and ensure that outings are equipped with accessible accommodations. Adults with late-onset GM2 shared their experiences navigating a world where every task, from visiting a friend’s house to completing daily activities like showering or getting out of bed, requires careful planning and consideration due to the physical limitations imposed by their condition.
Zoë, 36 years old, living with late-onset Tay-Sachs said: “It’s just sort of a constant battle of figuring out what’s going to be the next issue, and where I go whether it will be accessible or not, or if I can get in the parking lot, or can I use the bathroom there? Will that be accessible?” (Figure 4)
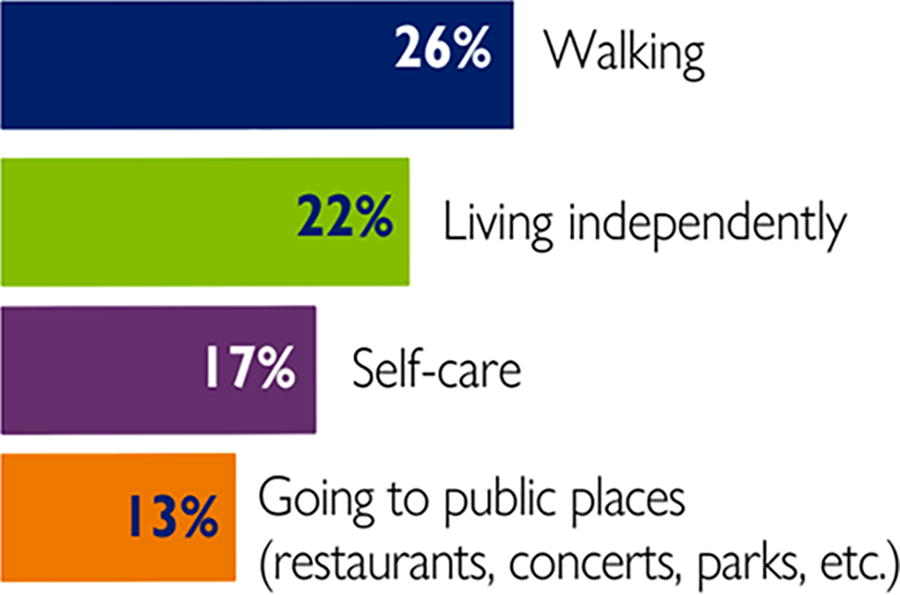
Participants were asked to select what daily life activities that are important to them or their loved one that they are not able to do or struggle with due to GM2.
Ken, 57 years old, living with late-onset Tay-Sachs: “I need to plan everywhere I go in advance. If I’m invited to a friend’s house, I need to evaluate if I have easy access or if the door accessible. How many stairs are there? Can I use the toilet? You realize as things get more difficult, you must plan everything you do in your life, and you must analyze everywhere you want to go.”
Adults face a range of physically limiting symptoms and devastating mental health issues
Adults living with late-onset GM2 ranked muscle weakness, motor deficits, and anxiety/depression as the most troublesome GM2 health-related concerns (see Figure 5). The interplay between the physical symptoms and the psychological stress appears to exacerbate the disease’s impact, making navigating late-onset Tay-Sachs and Sandhoff diseases particularly complex and multifaceted.
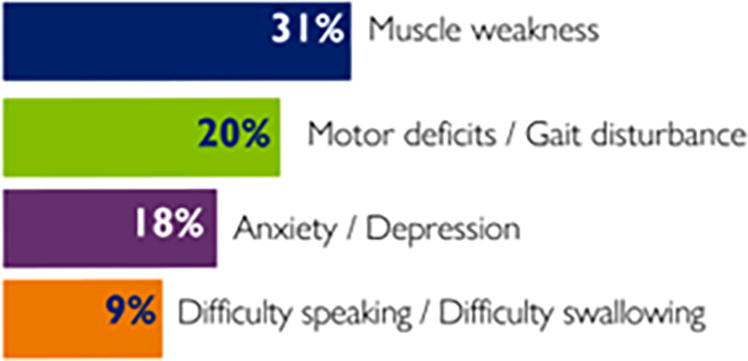
Participants ranked the most troublesome GM2-related health concerns that they or their loved one has ever had.
Mobility decline: Coping with muscle weakness and lack of mobility
Adults living with late-onset disease discussed the profound impact of mobility limitations on their daily lives. From struggles walking up stairs and getting up from chairs to relying on mobility aids like walkers and wheelchairs, their accounts shed light on the significant challenges faced with respect to ambulation and muscle weakness. Despite their efforts to stay active through exercises and adaptive strategies, the progressive nature of the disease presents ongoing obstacles to mobility and physical function.
Alan, a 50-year-old living with late-onset Tay-Sachs disease, shared the same sentiment, noting that his reduced mobility, along with stiff straight legs, balance, and energy levels, have the most significant impact on his life.
Michael, a 54-year-old with late-onset Sandhoff disease, talked about the impact on work, saying that “clients tend to meet me in their car parks or somewhere accessible as I cannot navigate stairs.”
Frequent falls: A common reality and constant threat
Caregivers and individuals affected by late-onset GM2 provided compelling insights into the pervasive fear of falls and the efforts required to mitigate potential risks. Their accounts detailed the constant vigilance needed to navigate everyday tasks safely, along with the realities of dealing with frequent falls.
“I fell down a flight of stairs at home at night breaking my big toe. I couldn’t understand why or how I fell. There was no warning prior to the fall, and I walked down the same stairs in the dark many times before without a problem,” said Michael, 54 years old and living with late-onset Sandhoff disease.
“When I was pregnant, I was leaving the supermarket. I had just finished unloading groceries, was on my way to return the cart and while holding on to the cart with both hands for balance with no warning, my legs finally gave out, and I fell, scraping both of my knees. I still have scars to this day,” said Rachel, who was diagnosed with late-onset Tay-Sachs at age 29.
Kirsten, who lives with late-onset Tay-Sachs, talked about the ongoing fear of falls, saying “I never knew when I was going to fall and that was very frightening to me.” She talked about how a previous fall caused her to “fracture both knees and patella tendons,” going on to say that “it’s really taken a toll physically, as well as emotionally, the fear of not knowing.”
Speech struggles: Dealing with speech difficulties
Adults living with late-onset disease shed light on the pervasive impact of speech difficulties on social interactions and professional opportunities. From enduring challenges in finding employment to facing social isolation, their accounts underscored the repercussions of speech impairment.
“Her speech problems and awkwardness affected her social life starting in middle school going through her entire life. It also affected her ability to find a job in spite of her good education. It was very difficult for her to be interviewed,” said Sophia, who takes care of her 50-year-old daughter Vera living with late-onset Tay-Sachs. “It not only interferes with her social life, it’s also dangerous that she would not be able to be understood if something happened.”
Rachel, living with late-onset Tay-Sachs, said that her speech is “very affected,” and that people think she has a hearing problem or intellectual disability, despite her holding two master’s degrees and being bilingual in Spanish and English. She noted that although her speech seems to be slowly improving due to speech therapy, “it still affects me mentally where people are nasty towards me just based off the way I speak.”
Inside the mind: Understanding the devastating mental impact
Panelists and participants shared the profound mental health impact of living with late-onset GM2. Their stories spanned everything from feelings of emptiness to managing severe psychiatric issues, highlighting the complex interplay between physical and mental health.
Katie, living with late-onset Tay-Sachs, said: “Some days I have a high and low of emotional breakdown, depression sometimes. Why me? Why does this happen? It’s not fair that it’s just so rare. Why does this happen to me?”
Patricia, mother to two adult children with late-onset Tay-Sachs, talked about the severe impact of mental health effects on her children, such as anxiety faced in going to places. “What can I do? How can I use the bathroom? Are people going to look at me? How are they going to think about me or see me or view me? That’s what it affects them every day.”
Struggling to connect: Missed moments and the emotional toll
GM2 can result in adults with late-onset GM2 feeling disconnected from others. Participants shared frustrations and fears around missing out on important activities, as well as the heavy emotional toll that the disease can bring.
“My son James plays football, and some of the fields can only be accessed by walking down a steep grass bank to reach the field. When James was younger, I could carefully walk down the inline sideways to lessen the gradient, but I can no longer do this and only now attend his game if I can park my car alongside the football field,” said Michael, 54 years old living with late-onset Sandhoff disease.
Lee wrote about her fears for daughter Allie, living with late-onset Tay-Sachs, “I worry that she will not be able to have her own babies. This is something that Allie wants with all her heart…to have children and be a mother.”
Jenny wrote about the impact that her adult son Stephen living with late-onset Tay-Sachs has had on the whole family. “It has been a very isolating experience having a family member diagnosed with a rare disease. There is no one to talk to that knows what he is going through.”
Fears for the future: Losing independenceand becoming a burden
Adults with late-onset GM2 and caregivers reveal their fears and worries for the future. Their accounts reveal deep uncertainties about losing independence, becoming dependent on others, and burdening loved ones.
Sophia explained how her 50-year-old daughter Vera had to go on disability when “she couldn’t drive, started to need help in everyday living and was getting tired very fast.” Sophia went on to say, “Vera’s conditions now are even more severe,” and that she often chokes while eating, needs help in and out of bed, and spends most of the time in a wheelchair.
Allie, 28 years old, a former college athlete now living with late-onset Tay-Sachs, said: “I’m a really independent person, really active, so it really scares me to think that those things could be slowly taken away from me.”
“Now I’m a caretaker for my daughters. If something happened to me, how will that affect them?” said Rachel, who was diagnosed at age 29 with late-onset Tay-Sachs when pregnant with her first child.
CURRENT AND FUTURE TREATMENTS FOR GM2
With no disease-modifying treatments available for GM2, patients and caregivers resort to a range of assistive devices and therapies to manage symptoms, all of which were deemed inadequate in controlling all symptoms sufficiently. In a meeting poll, 88% of participants say treatments for symptoms only help “somewhat” or “very little.” Parents and patients have hopes that future disease-modifying treatments will help them preserve even basic abilities to improve their quality of life, with many willing to take considerable risks in the quest for an effective treatment.
Symptom management is falling short
Meeting polls and discussions reflected a wide range of treatments being used, including seizure and pain medication, antibiotics, feeding tubes, nebulizer treatments, respiratory therapy, and antidepressants/antianxiety medications, along with other supplements. Physical and occupational therapy were often cited by parents and patients as being helpful for strength and flexibility, while Botox was cited by several parents as being helpful in secretion management. Additional therapies such as speech, music, equine therapy, and others provide further support. Despite diligent efforts to manage the disease, these interventions serve as temporary measures for a progressive condition that will inevitably worsen over time.
Mobility devices are a constant
Parents of children with GM2 and adults with late-onset GM2 talk about the range of mobility devices needed to support their daily lives. This includes ankle-foot orthosis to support the foot and ankle alignment, as well as canes, walkers, and wheelchairs (Figure 6).
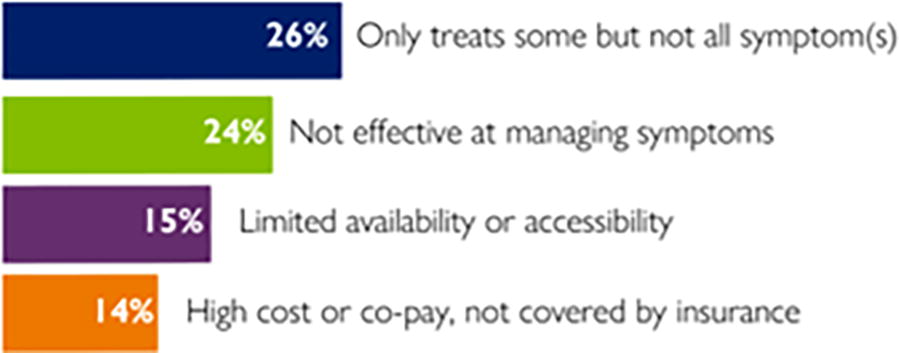
Participants were asked about the biggest drawbacks of their or their loved one's current treatment/symptomatic approaches.
“I have three walkers. I have one upstairs, one in the basement, and as well as an electric stair lift to get to the basement. I have a power wheelchair, and I keep one in my truck. That’s pretty much what my life has become,” said John, 59 years old, living with late-onset Tay-Sachs.
G-tubes become a way of life
Many parents discuss transitioning their children to a G-tube to guarantee proper nutrition. However, this decision is challenging for all involved, as it deprives the children of the joys of tasting and enjoying food, yet they may not be getting sufficient nutrients due to the challenges of eating. This leaves parents burdened with guilt for having to make such a choice.
Aaron, who lost his daughter Annabella to juvenile Tay-Sachs just after her fifth birthday, described the gradual decline in her ability to eat, leading to increased coughing and danger of aspiration. “Giving her the G-tube almost killed us, she was such a great eater before. She ate everything that we gave her, and she loved pizza or cookies… and she loved drinking juice, and then she couldn’t do that anymore. We tried to keep it going as long as we could until it was just getting too dangerous.”
“The child lives a life of therapy just so that we can keep her just sustaining because there is no way our children are going to make gains. The word ‘gain’ is not in our vocabulary. We sustain until we regress,” said Yasmina, mother to 11-year-old Lily with juvenile Tay-Sachs.
Challenges with medication trade-offs and administration
Parents talked about the trade-offs with certain medications, such as seizure medications causing extreme sleepiness and difficulties in dosing and administration.
Reita, mother of 18-month-old Palmer with infantile Tay-Sachs recounts that: “It is very hard to tell the right amount to help him, and it is constantly changing. These medications also tend to make him drowsy, which is a negative as he already has very low energy. We also had to thicken his medications when he was still consuming things by mouth as he would otherwise choke on them.”
Sonja talked about trade-offs, noting that, “For many adults with psychiatric disorders, the biggest problem is that many antipsychotics worsen neurological symptoms.”
Additional devices
Participants talked about a broad range of additional devices used to assist them in daily life, including communication devices, home modifications, oxygen machines, vital signs monitors, adaptive seating items, and much more.
Kirsten, who had previously worked as a parole officer, noted that now she cannot move around her home “without touching a wall, piece of furniture or using a four-wheeled walker,” and describes the various accommodations for her house. “My bathroom has been modified with a higher toilet, grab bars and a shower with a low lip. I cannot dress or undress without using a grab bar located right next to the shower. A mat on the shower floor gives me traction and stability along with two grab bars located within it.”
Some families choose the path of low intervention
With no treatments that can change the course of disease, some families focus on making the most of the time left rather than seeking extensive treatments for symptoms.
Carla, whose daughter Talia died from infantile Tay-Sachs at 23 months old, said: “Our family made the choice not to intervene with any life-extending treatments like a feeding tube, and instead to allow us to follow Talia’s body as her brain ceased functioning. The only intervention we allowed were those to mitigate pain. We enlisted the help of palliative care to help us see a path forward where our daughter could focus on the things that made her happy, like being held, going on hikes and laying in her bouncer chair at the family table where her siblings ate and laughed.”
Shannon wrote a similar sentiment, saying that although a high-intervention approach was recommended by the medical teams, they took a different approach and “chose to be as low intervention as possible.” She went on to question the “intense focus on keeping these kids alive as long as possible. At a certain point, the question becomes, at what cost? Why do we allow parents to admit these kids to the hospital for weeks when they get sick? That doesn’t seem humane when the outcome of this disease is always death.”
Hopes for future treatments
Parents and patients affected by GM2 share a common hope for future treatments that can halt or slow disease progression (Figure 7). To reach that goal, participants expressed a readiness to undertake greater risks in hopes of finding a disease-modifying treatment. Short of a cure, the significance of modest achievements—such as the capacity to grasp a hand, communicate thoughts effectively, or reduce the incidence of falls—cannot be overstated for individuals living with GM2. These small victories are profoundly meaningful, offering tangible improvements in quality of life and a sense of control against the condition (Table 1).

Participants were asked what top three specific things they would look for in an ideal treatment for GM2, short of a complete cure.
The chart below was assembled based on input from the GM2 EL-PFDD meeting on February 15, 2024, including discussion during the meeting, polls taken, and comments submitted afterward. This sample framework may help inform the FDA’s Benefit-Risk Assessment for urgently needed GM2 treatments
Desperation for a disease-modifying treatment that can slow or stop disease progression
With no treatment that can target the root cause of GM2, parents and patients experience profound frustration and helplessness as they grapple with the inability to halt the relentless progression of the disease.
“What frustrates me the most is that there’s no way for me to stop the progression of this disease. There is literally nothing I can do to save my son,” said Kate, mother to 3-year-old Felix who lives with infantile Tay-Sachs.
Allie, the 28-year-old former college athlete now living with late-onset Tay-Sachs, said: “I want to stop this so I can keep my life being as normal as I could, but it’s just getting worse and worse and worse.”
Jennifer, mother of 12-year-old Madelyn with juvenile Sandhoff disease said: “I wish that we could just stop, freeze time. Of course, I wish we could go back and regain when she could independently walk or run or do all of those things, but at this point there’s so few options that I just wish there was a way to just stop it or slow it down more so that she can keep these abilities…and we don’t lose our children more than we already have.”
Quality of life goals are different for everyone, but quality is the key
Amid the challenges of managing Tay-Sachs and Sandhoff diseases, a common goal is to preserve a patient’s quality of life. What that looks like differs from person-to-person but a common thread emerged, which was a desire for a life that allows children to engage with the world, enjoy simple pleasures, and minimize pain and discomfort, rather than merely surviving.
Carla, whose young daughter died from infantile Tay-Sachs at 23 months old said: “If the interventions could help Talia to have a healthy mind, to help her to know us and allow us to fully know her, then I would support it. If the interventions’ mark of success was the ability to keep her body functioning without addressing her mind’s deterioration, then it would not be something I would want for her.”
Kevin R., whose son Mathew died from infantile Tay-Sachs at 7 years old, said: “Quite frankly, a good day was when we weren’t in intensive care and we were able to have our child home with us.”
Kevin L., who has two adult children with late-onset Tay-Sachs said: “An ideal treatment would be to stop the slow deterioration and wasting away of leg muscles” along with an ability to “smooth out the rough mental health episodes.”
Small gains would have a big impact
Parents and patients underscored the profound significance of even modest advancements in quality of life. They expressed the relief and joy found in simple gestures and interactions. Whether it’s the ability to hold hands, enjoy time at home, witness a smile, or achieve basic motor skills, these accounts emphasize the transformative power of small gains amid the realities of GM2.
Lorelei, mother to a 13-year-old son Isaac with infantile Tay-Sachs, who had a stem cell transplant at 10 months old, said that for her a huge win would be “to see him smile consistently and/or verbalize anything would be amazing at this point” and for her son, he would most benefit from getting off some of his respiratory treatments which take up much of his day.
Abby, mother to young son with infantile Tay-Sachs wrote: “I think the biggest improvement to Levi’s quality of life would come from a greater ability to interact and respond to the people around him.”
Dan, father to Amélie who died from infantile Tay-Sachs disease at 8 years old, noted a key treatment goal would be “the ability to reach out and grab something, grab a toy, grab food, even holding a hand.” He goes on to talk about the importance that holding hands gives to both the child and the parent and how preserving that could make a big difference.
People are willing to take on more risks but need transparency
In the pursuit of treatments for GM2-related diseases, a prevailing sentiment among caregivers and patients emerged: the willingness to embrace risk in hopes of improving outcomes. A demand for transparency was also clear, not just around informed consent in the moment but also as a way to mitigate any future regrets the family may have about treatment choices.
Carla, whose young daughter died from infantile Tay-Sachs said that “parents are grasping at anything to improve survival even before we’re able to slow down and have real discussions about what survival truly means. There must be time built into any treatment for more than one fully transparent discussion before any life-altering treatment is given. Survival means something different to each family, and discussions that get to the heart of the patient’s wishes, while being transparent about the treatment’s ability to meet them, are almost as important as the treatment itself. Only with full transparency can future regret be mitigated, and regret can be more corrosive than grief.”
Lorelei, mother to 13-year-old Isaac who has infantile Tay-Sachs, said: “We knew 100% that Tay-Sachs was fatal if we didn’t do anything. 100%, we were going to lose him. So a 50% chance of losing him during this process [of a stem cell transplant] versus maybe saving his quality of life and giving him not just quantity but good quality, that was what tipped it for us.”
Heath said: “If a current trial has been paused because of seeing a possible side effect that patients experience anyway, why can parents not make the choice to continue with the trial? I would rather deal with a possible side effect from medication that could slow or stop the progression than have my child develop the same thing and not slow or stop the progression.”
Allie, a 28-year-old living with late-onset Tay-Sachs, said, “I’m willing to try anything. I’ve even thought about prosthetics, robotic limbs, as extreme as having an amputation in order to have legs that work that can carry me without fear of falling.”
And while some are willing to accept greater risks to gain a new treatment, others questioned clinical trial participation and what it means for them. Ken, 57 years old, with late-onset Tay-Sachs shared, “My biggest issue with clinical trials is that after I participated in one, then that eliminates me from any future trials. If there’s a washout period, that is fine. However, if I participate in a more serious type of trial that involves a more permanent change to me, then I’m no longer considered a prime candidate for any future trials, and this to me is hard to accept.”
Patients and parents beg for expedited timelines
Sophia wrote about the need for an expedited timeline for trials, asking, “Could a new system of testing be developed with shorter [timelines] (e.g., six months) with a small number of patients to try new medications? Patients are getting worse every day.”
Vera wrote, “As someone living with late onset Tay-Sachs, my condition is progressively getting worse, and I don’t have seven years to wait for a clinical study. I would like to have the ability to try medications or treatments approved for other conditions or perhaps take part in a smaller study. Because the longer I wait and let things continue ‘as is’, the greater chance I have of significant injury.”
Rick’s daughter Krystie, who had a stem cell transplant, passed away from infantile Tay-Sachs at the age of nine: “As more and more children are diagnosed with these horrible diseases, time is not our friend.”
Promise in new treatments
As experimental new treatments show some promise, a family impacted by GM2 shared their experience. Lauren writes, “We are five months post gene therapy and looking back we would make the same decisions to participate again. One of the biggest benefits we have seen from it is that Daphne is still able to take all her food and drink by mouth. Tay-Sachs has taken so much from our daughter and being able to maintain her ability to eat is a very important piece to her quality of life. We feel lucky at the timing of her diagnosis that she was able to receive gene therapy and hope that the research and availability is more widespread in the future.”
INCORPORATING PATIENT INPUT INTO A BENEFIT-RISK FRAMEWORK FOR GM2
Benefit-risk assessment is the foundation for FDA’s regulatory review of human drugs and biologics. This framework provides a context for regulatory decision-making and includes valuable information for weighing the specific benefits and risks of a particular medical product under review.
CONCLUSION
The EL-PFDD meeting on February 15, 2024, was an important platform for the FDA and others to hear directly from those impacted by the three different onsets of GM2 gangliosidosis. Parents and patients shared their intense journeys with Tay-Sachs and Sandhoff diseases while mourning a life that could have been. They shared their frustration at dealing with ineffective symptom management while watching themselves or their loved ones fade away until they finally succumb to GM2.
The desperate need for a treatment that can stop or slow the progression of GM2 is clear. Even the smallest improvements would make a huge difference in the lives of those impacted by Tay-Sachs and Sandhoff diseases.
NTSAD is grateful for this opportunity to share the experiences of patients and parents during the EL-PFDD meeting and in this “Voice of the Patient” report. We are continually inspired by the strength and courage of the GM2 community. We hope that learning about the love, loss, and legacy of these families will spark change and create a brighter future for those impacted by Tay-Sachs or Sandhoff diseases.
IN MEMORIAM
Soon after the EL-PFDD meeting on February 15, 2024, two families that participated in the meeting experienced a devastating loss that we see all too often in the GM2 community. The legacies of Cayden and Phillip will live on in our hearts and in this report.
Footnotes
ACKNOWLEDGMENTS
The authors are grateful beyond words to all caregivers and patients who participated, whether actively caring for someone with GM2, living with GM2, or mourning the loss of a loved one. Thank you to Florian Eichler, MD (Massachusetts General Hospital), and Cynthia Tifft, MD, PhD (National Institutes of Health), for providing insightful medical overviews of GM2. The authors deeply appreciate the participation of Jacqueline Karp, MD (FDA), for discussing the importance of integrating the patient/caregiver perspective into drug development and evaluation. NTSAD also acknowledges the collaboration and invaluable support of fellow patient advocacy community partners: Blu Genes Foundation, Cure Tay-Sachs Foundation, The CATS Foundation, Mathew Forbes Romer Foundation, and members of the Global GM1 & GM2 Alliance. Larry Bauer, RN, MA, and James Valentine, JD, MHS, offered indispensable assistance and support for the meeting. Hyman, Phelps & McNamara, P.C. is a law firm that represents sponsors who are developing drugs for rare diseases and patient advocacy organizations. The authors also extend their thanks to the team at Dudley Digital for providing seamless technical support.
AUTHOR DISCLOSURE
This meeting was organized by NTSAD with financial support from Sanofi, Cure Tay-Sachs Foundation, Mathew Forbes Romer Foundation, New York Area Fund at NTSAD, Azafaros, and JCR Pharmaceuticals. No pharmaceutical company was involved in the planning and coordination of the meeting.
FUNDING INFORMATION
No funding was received for this article.
SUPPLEMENTARY MATERIAL
Supplementary Appendix SA1
Supplementary Appendix SA2
Supplementary Appendix SA3
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.