
Abstract
Objective:
This systematic review aimed to document and describe how and when to assess patients' expectancies to acupuncture and the relationship between patients' expectancies and clinical effects.
Materials and Methods:
Three English databases, including PubMed, Cochrane Central Register of Controlled Trials, and EMBASE, and four Chinese databases, including the Chinese Biomedicine Literature Database, Chinese Journal Full-text Database, Chinese Scientific Journal Full-text Database, and Wanfang Database, were searched up to February 2020. Studies involving patients' expectancies to acupuncture were included. Based on the detailed situations of patients' expectancies, we made a standardized data extraction table that included the basic information of articles, study design details, and measurement of expectations. Based on the data, a descriptive analysis was performed, covering the characteristics of studies, measuring methods of expectations and the relationship between patients' expectancies and clinical effects. Methodology quality assessment was also performed by the risk of bias and the standards for reporting interventions in controlled trials of acupuncture.
Results:
There were 61 randomized controlled trials included in our analysis. The number of articles increased gradually over time and grew significantly after 2008. About half of trials focused on pain alleviation. Expectancies were measured before the treatment (N = 43), after the treatment (N = 3), and both before and after the treatment (N = 10), and five studies did not mention it. The measurement of expectancies used self-made questionnaires or scales (N = 27), the Acupuncture Expectations Scale (N = 6), and other scales (N = 11), while 17 studies did not describe what scale they used. The used questionnaires or scales mostly tried to ascertain the strength of confidence that acupuncture would help. Patients' expectancies and clinical effects were relevant in 19 studies, irrelevant in 21 studies, and were not mentioned in 21 studies.
Conclusions:
Patients' expectations to acupuncture have received increasing attention in recent years, but there is still no recognized measurement time and methods. It is critical to develop questions and answers regarding patients' expectations with better discrimination and reliability to accurately assess expectations and to explore the relationship between patients' expectations and acupuncture outcomes in future trials.
Introduction
Acupuncture is one of the most widely used complementary and alternative medicines. 1 Many studies have found that there is no significant difference between real acupuncture and sham acupuncture, which indicates that the effect of acupuncture may be a placebo effect. 2 Expectancy is the core of the placebo effect of acupuncture and plays an important role in acupuncture treatment efficacy. 3
Expectancy is an individual's nonvolitional, self-confirming “gut” reaction to a situation or behavior, and how an individual expects to respond to a treatment is likely to be mediated by previously held beliefs or perceptions and information received. 4,5 Peerdeman et al. found that expectancy was a predictor during pain treatment, and intervening in expectancy may influence the outcomes. 6 Positive expectancy could induce the secretion of endogenous opioids, which might inactivate the pain regulation system. 7
Acupuncture is a complex intervention in which patient-acupuncturist communication and patient acupuncture experience may affect expectancy and clinical efficacy. 8,9 In other words, it may affect research validity and bias the outcomes in clinical trials. Thus, it is essential to assess patient expectancies. It has been demonstrated that acupuncture clinical efficacy might be hampered by inadequate measures. 10 White et al. found that the higher the expectancy, the better the clinical effects of acupuncture for chronic neck pain. 11 There are other studies with inconsistent results showing that expectancy might have a negative correlation 12 or have no effect on the clinical effects of acupuncture. 13 The differences in studies and the inconsistent results across the identified studies raise important considerations regarding which methodological approach is best equipped to determine patient expectancies for acupuncture outcomes. The two pertinent methodological issues are whether and when to assess expectancies and how to accurately assess expectancies. Then, the relationship between expectancies and clinical effects can be clarified.
Therefore, we aimed to analyze published literature in the acupuncture field through a systematic review to report (1) how and when to assess patients' expectancies and (2) the relationship between patient expectancies and clinical effects.
Materials and Methods
Search strategy
The systematic review and meta-analysis were performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (Supplementary Data). The following sources were searched up to February 2020. We searched three English databases, including PubMed, Cochrane Central Register of Controlled Trials, and EMBASE, and four Chinese databases, including the Chinese Biomedicine Literature Database, Chinese Journal Full-text Database, Chinese Scientific Journal Full-text Database, and Wanfang Database.
The keywords were “acupuncture” OR “electroacupuncture” AND “expectation” OR “expectancy.” For example, the search strategies in PubMed were (((expect*[Title/Abstract]) OR (satisfaction[Title/Abstract]) OR (preference[Title/Abstract]) OR (motivation[Title/Abstract]) OR (attention[Title/Abstract]) OR (intention[Title/Abstract]) OR (belief[Title/Abstract]) OR (placebo[Title/Abstract])) AND ((acup*[Title/Abstract]) OR electroacupuncture [Title/Abstract]))). Each database was searched independently. Forward and backward searches were retrieved manually.
Inclusion/exclusion criteria
We searched for studies that met the inclusion criteria regarding patient expectancy. We did not place any restriction on the type of clinical trials (including observational studies and interventional studies) or expectancy. Expectancy was included regardless of how it was assessed. Original studies published in full text in Chinese and English were included. In addition, reviews and news reports were excluded.
Study selection
Two reviewers were trained to assess whether the studies should be accepted or excluded (T.L.W. and F.H.R.). Both reviewers independently assessed the studies, and disagreements were resolved by discussion with a third reviewer (X.Y.Y.) when necessary.
Data extraction and analysis
Based on the detailed situations of studies regarding the expectation of acupuncture, we made a standardized data extraction table that included the basic information of articles, study design details, and measurement of expectations. The data extraction table was independently completed by two authors (T.L.W. and Y.J.) and checked by another author (X.Y.Y.). A descriptive analysis was performed and then to undertake a meta-analysis if it would be possible due to the heterogeneity of these studies.
Study quality and risk of bias assessment
Two authors (T.L.W. and Y.J.) selected the eligible studies, extracted data independently, and assessed the methodological quality of the included trials using the Cochrane risk of bias (RoB) tool. The following items were evaluated: “Random sequence generation” (selection bias), “Allocation concealment” (selection bias), “Incomplete outcome data” (attrition bias), “Selective outcome reporting” (reporting bias), and “Other bias” (focused on differences in sample characteristics—sex, age, and baseline pain).
The standards for reporting interventions in controlled trials of acupuncture (STRICTA) checklist were used to assess the quality of evidence and completeness of acupuncture intervention. The two authors were trained before assessment, which allowed them to have a similar understanding of the items. Disagreements between the authors were resolved by discussion with the involvement of a third reviewer (X.Y.Y.).
Results
Study selection
We initially searched 15,687 potentially relevant articles including, 15,675 articles retrieved from databases and 12 articles from forward and backward searches. There were 11,319 articles left after duplicates were removed. A total of 11,187 articles were excluded based on the titles and abstracts. A total of 132 articles remained, and 62 articles were excluded according to the inclusion criteria and exclusion criteria, leaving 70 articles, including 4 studies mainly discussing the questionnaire, 5 observational studies, and 61 randomized controlled trials (RCTs). Finally, 61 studies on qualitative analysis were included as shown in Figure 1.

Study flow chart (Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2009 flow diagram for new systematic reviews). CNKI, China National Knowledge Infrastructure; VIP, China Science and Technology Journal Database. Color images are available online.
Study characteristics
The characteristics of the included clinical RCTs are reported in Table 1. Nineteen of the articles were published in Chinese, while 42 were published in English. Needling types included manual acupuncture (N = 46), electroacupuncture (N = 11), and other needling methods (N = 4). The controls included sham acupuncture (needles were located at the same acupoints as the accessory device, but were not inserted into the skin) (N = 28), treatment as usual control (N = 20), waiting list control (N = 6), and others, including placebos, combination therapies, behavioral therapy, and so on (N = 13). The median date of publication was 2002 (range 1979—2019). The number of articles increased gradually over time and grew significantly after 2008. Approximately half of the trials focused on pain alleviation, including osteoarthritis (N = 13), headache (N = 6), low-back pain (N = 6), and dysmenorrhea (N = 2). Gynecological disorders (N = 7) and digestive system diseases (N = 9) formed the next two largest groups. There were 51 trials in which participants were blinded, 6 trials were open label, and 4 trials did not describe the blinding method.
Study Characteristics of All Studies
Relevant indicated that there is no relationship between expectation and treatment.
Irrelevant indicated that there is relationship between expectation and treatment.
Acupuncture combined with other comprehensive therapies.
ABS, Acupuncture Belief Scale; AES, acupuncture expectancy scale; CI, confidence interval; ETCS, expectation and treatment credibility scale; NA, nonpoint acupuncture; OR, odds ratio; RSI, repetitive stress injury; SA, sham acupuncture; TAU, treat as usual control; VAS, Visual Analog Scale; WLC, waiting list control.
Measurement of expectancies
Measurement questionnaires or scales
Expectancies could be measured in a variety of ways. Some studies used a verbal question 31 or let patients grade their expectancies. 54 In most trials, the measurements of expectancies involved asking questions and then scoring the participants' answers. There were 27 studies that used self-made questionnaires or scales, 6 that used the Acupuncture Expectations Scale (AES), 72 and 17 studies that did not describe the scale used. Other studies (N = 11) used different scales, such as the credibility rating scale developed by Borkovec and Nau 73 (N = 4), and the Expectation Treatment Credibility Scale (ETCS) 74 (N = 2), the Acupuncture Belief Scale (ABS) 75 (N = 1), and Minnesota multiphasic personality inventory 76 and psychosocial questionnaire 77 (N = 1).
We sorted the problems mentioned in all articles and their response scales, which are summarized in Table 2. There were 21 different questions being raised. The most popular phrasing was a direct question concerning the presence or absence of a belief for treatment benefit, such as “[After the treatment/acupuncture, do you expect your …to be…?]/[How bothersome do you expect your … to be at the end of treatment?],” which was mentioned 15 times in total. Their response scales used a Likert scale (N = 15), a Numerical Rating Scale (NRS) (N = 10), a categorical scale (N = 22), an adjective scale (N = 23), or the 100 mm Visual Analog Scale (VAS) (N = 18). [Multiple questions on the same scale may use different answer scales, so the total was not 61.]
Measurement of Expectancies
Refers to included questions in Chinese, a, 4/5; b, 2/4; c, 1/1; d, 3/3; e, 1/1; f, 2/4; g, 1/1; h, 2/4; i, 2/3; j, 2/4; k, 2/2; l, 1/1; m, 1/1; n, 3/3; o, 3/3; p, 3/3; q, 3/4; r, 3/3; s, 4/4; t, 1/1; u, 1/1; v, 1/1; w, 4/4; x, 4/4; y, 1/1.
NRS, Numerical Rating Scale; VAS, Visual Analog Scale.
Due to the diversity of question phrasing, there were considerable variations in the anchors used within a response scale. For example, the Likert scales included anchors such as “Not confident” to “Very confident” and “Strongly agree” to “Strongly disagree,” and the adjectival scales used “Not certain at all” to “Very certain” and “Excellent” to “Poor.” For the questionnaires using a Likert scale, the expected score was often obtained according to the choice of subjects. For the NRS or VAS, scores were usually obtained by adding and converting numerical values. Among the included studies, three articles that used different answer scales described the proportion of patients with different responses, which are shown in Figure 2.
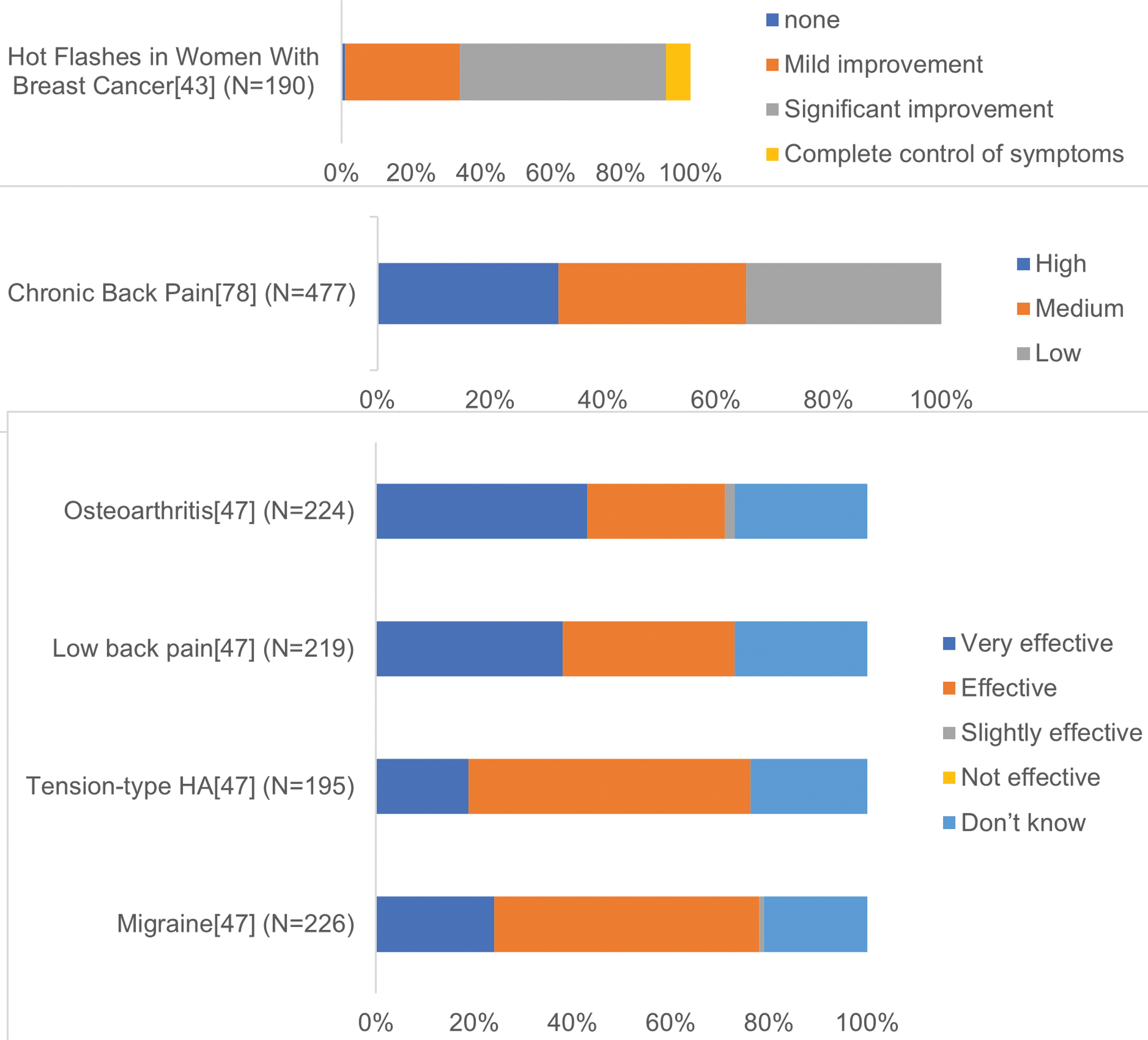
Response expectancies for acupuncture at baseline. Color images are available online.
Measurement time
According to Table 1, expectancies were measured before the treatment in 43 studies, after the treatment in 3 studies, and both before and after the treatment in 10 studies, and 5 studies did not describe when expectancies were measured. AES, ABS, ETCS, and other commonly used scales were almost measured before treatment.
Relationship between acupuncture expectancies and clinical effects
Of the articles included in this study, 21 articles found clinical effects and expectancies to be related. Nineteen articles indicated that the two were not related, and 21 articles did not address the issue (shown in Table 1). There was no consistent relationship that discriminated the effect of expectancies on outcomes.
Only nine trials evaluated expectations and grouped participants into “High-low expectations” or “High-Medium expectations” groups. Among them, four articles 35,46,50,58 showed that positive expectations lead to a better curative effect, four trials indicated no correlation between them, 18,24,33,59 and one did not mention the relationship between them. 55
Methodology quality assessment
RoB of included trials
Figures 3 and 4 show the assessment of the RoB in all included studies. Regarding selection bias, 56% of the studies reported that treatment allocation was random. Randomization was not mentioned in 4% of the studies (unclear RoB) and was incomplete or not performed at all in 40% of the studies (high RoB). Allocation concealment was reported adequately in 44% of the studies (low RoB); in four studies, allocation concealment was described insufficiently (unclear RoB). None of the other studies mentioned allocation concealment, but a high RoB was inferred if randomization was incomplete or not performed at all (50%). For the blinding method, 23% of the trials performed double-blinding using a special device (low RoB), while most of the included trials (76%) ensured only blinding to patients (high RoB). More than half of the studies (56%) were blinded to the outcome assessors. Among 79% of the studies, there were no signs of attrition bias due to incomplete outcome reporting (low RoB), as the protocol was available and the outcome had been reported in the prespecified way. Last, the risk of “other bias” was judged to be high in 27 studies because other bias was not mentioned in these articles.

Risk of bias graph: review authors' judgments about each risk of bias item presented as percentages across all included studies. Color images are available online.

Risk of bias summary: review authors' judgments about each risk of bias item for each included study. Color images are available online.
STRICTA assessment of the 61 included trials
The detailed assessment results are summarized in Table 3. Most of the included trials provided detailed descriptions of the acupuncture rationale (83.87%) and treatment regimen (77.42%). More than 45.9% of the trials provided a complete and comprehensive description of the needling details. A total of 72.58% of the trials mentioned the control interventions, but some of the descriptions were not precise. More than half of the trials (61.29%) mentioned practitioner background, but professional affiliation, years in acupuncture practice, or other relevant experience was not always described in detail.
Checklist of 61 Included Randomized Controlled Trials for Items in Standards for Reporting Interventions in Controlled Trials of Acupuncture 2010
Discussion
Through this systematic review, 61 RCTs mentioned measurements of acupuncture expectations, covering measurement time and questionnaires or scales. Approximately half of the included trials covered pain disorders, which was the disease most influenced by expectations. 78 Positive expectations may contribute to the alleviation of visceral pain and somatic pain, 79 while negative expectations may cause the nocebo effect and worsen symptoms. 80 Patients' expectations are significant factors that should be considered to obtain the maximum analgesic effect of acupuncture.
For the detailed measurement of expectation, most of the questions included in our review were trying to ascertain the strength of confidence that acupuncture would help, and both the wording of the question and the labels for the response options varied considerably. Approximately 24 studies used self-made questionnaires with single items, which lacked reliability and validity testing. The AES is specifically used for assessing acupuncture expectancies and consists of four items. However, the item generation and word phrasing might lead to positive guidance to patients. 72 The question phrasing (how confident one is and how much help might be obtained) may be a legacy of the original measurement developed by Borkovis and Nau. 81
As for the cognition of the concept, there are many types of expectations in the literature with ambiguous terminology. 82 Laferton et al. had summarized an integrative model of expectations of patients undergoing medical treatment. 83 In this model, behavior, treatment, and outcome related aspects of expectations were the most concerned part, while in acupuncture field, these included studies only focused on a single (usually the generalized expectations) or few aspects of expectations, which made it difficult to investigate the differential influence of expectation. 84 For the purpose of fostering understanding of the relationship between expectations and clinical effects, standardized and psychometrically evaluated measures are also needed for assessing patient expectations comprehensively and multidimensionally.
Most of the studies used Likert scales, the VAS, or NRS with a middle neutral category, which were used more often than unidirectional adjectival scales. For the most part, 5-point Likert-type scales were used, and these scales have substantially better statistical power than assessing expectancies through dichotomies or trichotomies. There were also scales with “don't know” as an extreme response.
In addition to the question and answer phrasing, the time at which expectancies are assessed should also be considered. The time at which expectancies were assessed varied by study. Most of the expectancy scales were administered before acupuncture treatment, while a few were administered after treatment. Expectancies may change during the course of treatment, which might also be affected by intervention. Expectations are a broad concept with various types. Different researches have different purposes, the time to measure expectations or ways to ask questions should be based on the purpose of researches. When the expectations were measured before the treatment, the prior belief in acupuncture might be examined. And after the treatment, it is appropriate to measure the patient's expectation for acupuncture response. Changes of expectation during the course of acupuncture could be assessed when measuring both before and after treatment. Therefore, it is important to clarify the aim of clinical research and choose the most appropriate time to measure a specific expectancy.
As for the relationship between patient expectancies and clinical, there is still no consistent conclusion through our preliminary qualitative analysis. This may be caused by variations in the measurement method or measurement times of expectancies. In addition, we also make an effort to do quantitative analysis such as meta-analysis, which failed because of the heterogeneity among all included studies. It is difficult to assure the effects of patients' expectations on clinical outcomes because of the heterogeneity of metrics and methods and the incomplete reporting of expectations. It may not always be practical to incorporate an expectancy manipulation into a trial of acupuncture, as this may require substantially larger samples to achieve the same level of power or may raise ethical considerations if deception is required. However, it is still critical and useful to develop recognized questions that better discriminate patient expectations reliably to accurately assess patient expectancies and explore the relationship between expectancy and treatment responses in future trials. 85
This systematic review was relatively comprehensive. The specific questions and answers of these scales were summarized, which provided quantitative data indicating a few methodological issues for future research. Although previous studies have systematically reviewed the literature in this field, our research is still unique. Compared with Prady et al., 86 the databases we searched included four native Chinese databases, and no restriction was placed on the types of included trials. Colagiuri and Smith 87 included only nine trials about the assessment and/or manipulation of expectations. Our research enlarged the number of trials to obtain more comprehensive information. Besides, measurement time and methods were also well summarized. In the above two reviews, it has been mentioned that consistent metrics and expectation questions need to be improved. Prady et al. 86 thought that comparison of expectations between trials was limited by the wide variety of response scales and word anchors. And Colagiuri and Smith 87 considered that to establish a good way to measure expectations, problems related to time and wording need to be solved first. It is necessary to summarize the existing response scales, answer scales used in the current questionnaires, and time of assessment comprehensively as we did in our study.
However, the relationship between acupuncture and expectancies was just preliminary qualitative, and the quality of the included studies assessed by STRICTA and ROB was not high. In addition, there was much selective reporting bias in which expectations were measured, but not reported, which could have contributed to our inconclusive findings. Finally, articles published only in Chinese and English were reviewed, which means that there may be other relevant studies published in other languages.
Patients' expectations as a core part of acupuncture placebo effects, its assessment and the relationship with clinical effects are crucially important. The timing and wording of the questions should be well designed to ensure the validity of these assessments. Other confounding factors that may influence expectancies, including previous treatment history, professional proficiency of acupuncturists, and acupuncturist-patient communication, should also be considered.
Conclusion
Patients' expectations to acupuncture have received increasing attention in recent years, but there is still no recognized measurement time and methods. It is critical to develop questions and answers regarding patients' expectations with better discrimination and reliability to accurately assess patients' expectations and to explore the relationship between patients' expectations and acupuncture outcomes in future trials.
Footnotes
Authors' Contributions
Research design: X.Y.Y. and T.L.W. Data collection: X.Y.Y., T.L.W., and F.H.R. Data extraction and analysis: X.Y.Y., T.L.W., and Y.J. Article preparation and revision: X.Y.Y., T.L.W., and H.L.J. All authors have reviewed and approved the article before submission.
Author Disclosure Statement
The authors declare that there is no conflict of interests regarding the publication of this article.
Funding Information
This work was supported by the Program of National Natural Science Foundation of China (Grant No. 81904063).
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.