
Abstract
Introduction:
Auricular acupuncture at the “relaxation point” and lavender oil aromatherapy can reduce preoperative anxiety associated with increased mortality and morbidity. Data on the effect of combined auricular acupuncture and lavender oil aromatherapy in patients undergoing cardiovascular interventions with the use of local anesthesia or under conscious sedation are sparse. The authors sought to evaluate the efficacy of auricular acupuncture and lavender oil aromatherapy in reducing preinterventional anxiety in cardiovascular patients.
Materials and Methods:
Data of 80 consecutive patients undergoing diagnostic coronary angiography (n = 56) with or without percutaneous coronary intervention (n = 9) and right heart catheterization (n = 6), transcatheter aortic valve replacement (n = 17) and percutaneous mitral valve repair (MitraClip; n = 2) were analyzed. Patients were prospectively randomized to receive either preinterventional auricular acupuncture and lavender oil (Lavandula angustifolia) aromatherapy (verum group, n = 39) or combined sham auricular acupuncture and placebo oil aromatherapy (placebo group, n = 41). For the verum group bilateral auricular acupuncture was performed at the “relaxation point.” State anxiety and blood pressure were assessed before and at 30 min after acupuncture and presternal oil application. State anxiety was defined as primary outcome measure and assessed using the Spielberger State Anxiety Inventory (STAI) for Adults form Y6. Intervention-specific anxiety was assessed by a 10-point numerical rating scale, and perceived treatment success by a single dichotomous question. Clinical blood pressure was further assessed.
Results:
After the intervention, the verum group had significantly decreased anxiety on the STAI compared with the placebo group (Δ = −4.18; 95% confidence interval = −8.31 to −0.05; p = 0.047). Significantly more patients reported subjective treatment success in the verum group (87.2%) than in the placebo group (65.9%, p = 0.035). No significant differences were observed regarding intervention-specific anxiety and blood pressure between the two groups. No serious adverse events occurred in any group.
Conclusions:
Combined auricular acupuncture and lavender oil aromatherapy can decrease preinterventional anxiety in cardiovascular patients and requires further investigation.
German Clinical Trials Register
(registration no. DRKS00023686).
Introduction
Preoperative anxiety is common and has been associated with unfavorable outcome in patients undergoing operations under general anesthesia. 1,2 Conventional pharmacologic therapies (e.g., opioids and sedatives) are commonly used as anxiolytics to achieve better preoperative state by reducing anxiety. 3,4 Nevertheless, conventional treatment of preoperative anxiety has relevant side effects (e.g., bradycardia, hypotension, and respiratory depression) that can lead to prolonged patient recovery. 5 Data suggest that auricular acupuncture especially at the “relaxation point” can reduce anxiety in general. 6 In addition, studies have shown that acupuncture and lavender oil aromatherapy can significantly reduce preoperative anxiety associated with increased mortality and morbidity. 7 –9
Patients undergoing interventions due to cardiovascular or structural heart disease are frequently at high operative risk. Both transcatheter aortic valve replacement (TAVR) and percutaneous mitral valve repair (MitraClip) have evolved to the standard of care for patients with severe symptomatic aortic valve stenosis and severe mitral regurgitation at high risk for surgical treatment. 10 –13 Unwanted side effects of conventional anxiolytic pharmacologic therapy can be critical for frail older patients. 5 Data on the effect of combined biauricular acupuncture at the “relaxation point” and presternal lavender oil aromatherapy in patients undergoing cardiovascular interventions, mostly under conscious sedation and with the use of local anesthesia, are sparse. The purpose of this study was, therefore, to evaluate the efficiency of auricular acupuncture and lavender oil aromatherapy in reducing preinterventional anxiety in cardiovascular patients compared with placebo.
Materials and Methods
Design
This was a single-blind randomized controlled trial conducted at a single center, Department of Cardiology and Angiology, University Hospital Bergmannsheil, Ruhr University Bochum, Germany. The study had been approved by the Ruhr-University Bochum ethics committee (approval no. 18-6515-BR) and registered at German Clinical Trials Register. The study was conducted and reported in accordance with the CONsolidated Standards of Reporting Trials (CONSORT) 2010 guideline (Fig. 1). 14 The full trial protocol is available from the corresponding author on reasonable request.

Participant CONSORT 2010 flow diagram.
Patient population
Data of consecutive patients undergoing diagnostic coronary angiography with or without percutaneous coronary intervention and right heart catheterization, TAVR and percutaneous mitral valve repair (MitraClip) were eligible. Patients with a history of a major psychiatric illness, under anxiolytic therapy, and/or prior experience with acupuncture were not eligible. Patients with contraindications against auricular acupuncture (such as wounds in the treated area) or lavender aromatherapy (such as allergies) were further excluded.
Patients were randomly allocated to auricular acupuncture and lavender oil aromatherapy (verum group) or sham auricular acupuncture and placebo oil aromatherapy (placebo group) by block randomization with randomly varying block lengths. The randomization list was created by the biometrician, who was not involved in patient recruitment or assessment, using the Random Allocation Software. 15 The list was password-secured and no other person than the biometrician was able to access it. On this basis, he prepared sealed, sequentially numbered opaque envelopes containing the treatment assignments. After obtaining written informed consent and baseline assessment, the study physician opened the lowest numbered envelope to reveal that patient's assignment.
Acupuncture and oil aromatherapy
Patients in the verum group received preinterventional bilateral biauricular acupuncture at the “relaxation point.” This acupuncture point is located at the superior wall of the triangular fossa (Fig. 2). 6,7,16 Lavender oil (5% dilution of Lavandula angustifolia oil in olive oil) containing high proportions of esters responsible for the relaxant and sedative effect was applied on the skin of the presternal region. The diluted lavender oil was supplied by the hospital pharmacy. Patients in the placebo group received bilateral sham auricular acupuncture at the auricular lobulus and presternal placebo oil aromatherapy. The placebo oil consisted of fractionated coconut odorless carrier oil. Auricular acupuncture was performed according to standard sterile techniques by instructed medical staff in both groups. 6,13 The acupuncture needles were removed after 30 min.
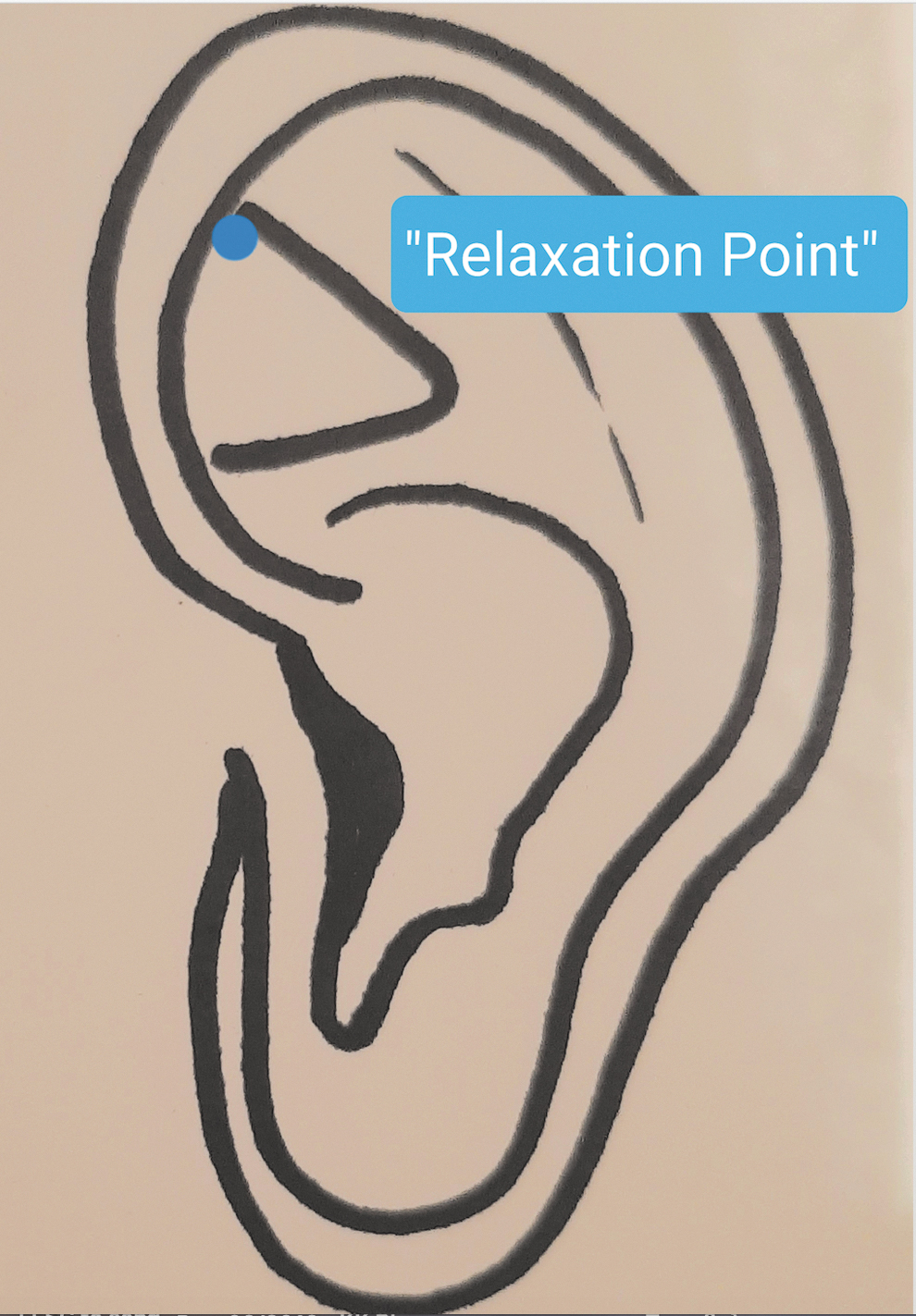
Auricular acupuncture at the “relaxation point”: This acupuncture point is located at the superior wall of the triangular fossa.
Outcome measures
Outcomes were assessed preinterventional before and at 30 min after needle insertion and oil application by an outcome assessor, who was not involved in patient recruitment and allocation, but involved in treatment. State anxiety was defined as the primary outcome measure and assessed using the Spielberger State Anxiety Inventory (STAI) for Adults form Y6. The STAI questionnaire is considered the “gold standard” in evaluating anxiety in preoperative patients and has been used in several peer reviewed studies. 6,9 In addition, intervention-specific anxiety was assessed on a 10-point numerical rating scale ranging from “no anxiety” to “maximal anxiety.” Blood pressure was measured by a sphygmomanometer. Blood pressure changes have been used in prior behavioral studies designed to evaluate anxiety. 6 Perceived treatment success was assessed by a single dichotomous question at 30 min after treatment, asking if a possible beneficial effect of the complementary treatment was noticed.
All adverse events occurring during the study period were assessed by the study physician
Sample size calculation and statistical analysis
The required sample size was calculated a priori assuming a large between-group effect of d = 0.8. A two-sided level 5% t test requires a total of 34 patients per group to detect a respective group difference with a statistical power of 80%. Accounting for a potential loss of power because of a maximum of 15% dropouts, it was planned to include at least 80 patients in this trial.
Categorical data are presented as frequencies and percentages; continuous variables are presented as means, standard deviation, and 95% confidence interval (CI). All analyses were based on an intention-to-treat basis, including all participants being randomized, regardless of whether or not they gave a full set of data or adhered to the study protocol. It was initially planned to multiply impute missing data by Markov chain Monte Carlo method. However, this was not necessary since all patients provided complete data sets.
Linear outcomes were analyzed by univariate analyses of covariance, which modeled the outcome after the study intervention as a function of the treatment group and the respective baseline value to produce overall effect size estimates, 95% CI, and p-values. The number of patients reporting perceived treatment success or lack thereof were compared between groups using Fisher's exact test.
All analyses were performed using the Statistical Package for Social Sciences software (IBM SPSS Statistics for Windows, release 22.0, Armonk, NY; IBM Group).
Results
Patient population
A total of 80 consecutive patients undergoing diagnostic coronary angiography (n = 56) with or without percutaneous coronary intervention (n = 9), right heart catheterization (n = 6), TAVR (n = 17), and percutaneous mitral valve repair (MitraClip; n = 2) were enrolled after providing informed consent and randomized to verum (n = 39) or placebo (n = 41) treatment. All patients received the allocated treatment, provided data at all time points, and were included in the final analysis (Fig. 1).
Baseline and procedural characteristics
This study cohort represents a typical cardiovascular patient population. Patients undergoing TAVR and MitraClip were at high risk for open heart surgery with symptomatic severe aortic stenosis or mitral regurgitation (Table 1).
Baseline and Procedural Characteristics
Values are reported as mean ± SD or n (%), as appropriate.
CAD, coronary artery disease, COPD, chronic obstructive pulmonary disease, LVEF, left ventricular ejection fraction, MI, myocardial infarction, TAVR, transcatheter aortic valve replacement; PCI, percutaneous coronary intervention, PVD, peripheral vasclar disease.
Outcome measures
From before to after the study intervention, the primary outcome measure state anxiety on the STAI decreased from 52.1 ± 10.9 to 36.4 ± 11.4 in the verum group and from 46.7 ± 11.9 to 37.3 ± 11.3 in the placebo group (Table 2); resulting in a significant group difference (Δ = −4.18; 95% CI = −8.31 to −0.05; p = 0.047).
Effects of Auricular Acupuncture at the “Relaxation Point” and Lavender Oil application on Patient-Reported Outcomes
Values are expressed as mean ± standard deviation.
CI, confidence interval; NRS, numerical rating scale; STAI, Spielberger State Anxiety Inventory.
No significant differences between the two groups were observed regarding intervention-specific anxiety or blood pressure (Table 2).
Significantly more patients in the verum group (n = 34, 87.2%) than in the placebo group (n = 27, 65.9%) reported perceived treatment success (p = 0.035). Adverse events did not occur in both groups.
Discussion
This study is the first to demonstrate that combined auricular acupuncture and lavender oil aromatherapy may decrease the preinterventional anxiety level in cardiovascular patients. Auricular acupuncture and lavender oil aromatherapy improved the patient's sense of well-being and decreased negative thoughts and consequently anxiety before cardiovascular intervention.
Conventional pharmacologic treatment of preoperative anxiety but also the use of general anesthesia can have relevant side effects especially in cardiovascular patients who are frequently at high operative risk. In such patients, percutaneous interventions are being performed under conscious sedation and with use of local anesthesia. 5,10 –13 Earlier studies have demonstrated that as well auricular acupuncture at the relaxation point as lavender oil aromatherapy is an effective method for the reduction of anxiety in patients undergoing surgery under general anesthesia. 7,8 Both intervention can be easily performed and are rarely associated with complications or adverse events. 6,8,9 The possible additive advantages of the combined interventions need to be taken into consideration especially for the frequently critical patients undergoing interventions due to cardiovascular or structural heart diseases. This study shows that performing combined auricular acupuncture and lavender oil aromatherapy can significantly reduce the preinterventional anxiety associated with increased mortality and morbidity without side effects or complications.
Effect of verum and placebo interventions
Approximately 60%–70% of adult patients experience high levels of anxiety before undergoing surgical treatment. 2,6 The commonly used conventional pharmacologic therapies (e.g., opioids and sedatives), however, may have unwanted side effects that can lead to prolonged patient recovery especially in older patients undergoing cardiovascular interventions. 5,6 Qualitative and quantitative assessment of anxiety of this analysis showed significantly reduced anxiety levels and blood pressure in all patients. It appears that patients overall responded positively to the added attention that was involved in participating in an acupuncture and aromatherapy trial. Therefore, without doubt, the placebo effect plays a significant role in clinical response to acupuncture and oil aromatherapy. Of note, the assumed placebo effect is to be considered as an additional positive feature of the complementary approach in terms of a real neurobiological phenomena and “the brain's inner pharmacy.” 17
However, further pre- versus postinterventional comparison using the primary outcome measure STAI revealed significantly improved postinterventional anxiety levels in the verum group compared with the placebo. Current data support the results of this analysis suggesting the possible influence of acupuncture in releasing neurotransmitters such as serotonin. 6,18,19 Serotonin may be key in determining the human emotional state. 18,19
In addition, significant reduction of anxiety levels after lavender oil aromatherapy due to the relaxant olfactory effect after topical administration has been discussed before. 8 Recent data suggest that the relaxant and sedative effect of high proportions of esters contained in lavandin show immediate onset after olfactory application, whereas after use on other topical areas effects can be observed after 10–90 min. 8 In this study, application of lavender oil on the skin of the presternal region could have been responsible for the relaxant effect in group 1, nevertheless this remains speculative.
According to this prospective randomized study, combined auricular acupuncture and lavender oil aromatherapy represents a safe and simple tool for treating preinterventional anxiety in patients undergoing interventions due to cardiovascular or structural heart diseases, who are frequently fragile and at high operative risk. The combined approach with its potential additive effect could have played an important role in improved response.
Limitations
It appears that patients overall responded positively to the added attention that was involved in participating in a trial, nevertheless STAI-evaluation revealed a significant further reduction of the anxiety level in the verum group. An important limitation of this study was the lack of additional groups to separate both treatment options from each other. Which intervention played a more important role in reducing anxiety levels remains speculative due to this oversight. Nevertheless, additional prospective randomized trials are necessary to further illuminate these promising findings. Auricular acupuncture and lavender oil aromatherapy might not be feasible for reducing preinterventional anxiety in emergency cardiovascular setting. Thus, patient selection is of great importance. Patients undergoing structural heart interventions need either conscious sedation or general anesthesia. This study included patients undergoing TAVR or MitraClip. Nevertheless, due to the small number of patients undergoing structural heart interventions, further studies are necessary to evaluate the possible effect of auricular acupuncture and lavender oil aromatherapy on reducing preinterventional anxiety isolated in patients undergoing cardiovascular interventions with conscious sedation or general anesthesia.
Conclusions
Combined auricular acupuncture and lavender oil aromatherapy significantly decreases preinterventional anxiety levels in cardiovascular patients, may reduce necessity of conventional anxiolytic pharmacologic therapies with unwanted side effects and requires further investigation.
Footnotes
Authors' Contributions
P.C.P., A.B.M.-P., and H.C. have conceived the study, acquired, analyzed, and interpreted the data and drafted the article. H.G.R., C.S., and D.U., have acquired and analyzed the data and have revised the article critically for important intellectual content. J.T.S., P.K.Z., G.J.D., and A.M. have made substantial intellectual contribution to conception and design of the study, and have revised the article critically for important intellectual content. All authors have approved the article version to be published and agree to be accountable for all aspects of the study in ensuring that questions related to the accuracy or integrity of any part of the study are appropriately investigated and resolved.
Author Disclosure Statement
P.C.P. is proctor for Edwards Lifesciences. The other authors report no conflict of interest.
Funding Information
No funding was received for this article.