
Abstract
Objectives:
In China, Xingnao Kaiqiao (XNKQ) acupuncture has been widely used for stroke treatment. However, its electrophysiological mechanism remains unclear. Hence, this study aims to study how XNKQ acupuncture modulates brain rhythm oscillations of stroke patients, and investigate its correlation with stroke recovery.
Design:
Randomized control trial.
Subjects:
Twenty (sub)acute ischemic stroke patients were enrolled and randomly assigned to two groups (an acupuncture group [AG] [n = 10] and a control group [CG] [n = 10]), and four patients (two patients in each group) dropped out of the study.
Interventions:
All patients received conventional treatments, and the patients in AG received additional XNKQ acupuncture treatment once a day for 10 consecutive days.
Outcome measures:
Before treatment, 14 days after, and 30 days after treatment onset, their movement impairments and neurologic deficits were measured using the National Institute of Health Stroke Scale (NIHSS), the Fugl-Meyer (FM) Scale, the Modified Rankin Scale (mRS), and the Modified Barthel Index (MBI), and their electroencephalogram data were recorded.
Results:
Compared with the CG, the AG showed more improvement in FM scores (p = 0.02), as well as decreased relative delta power and increased relative alpha power after 2 weeks' treatment. The decrease of the relative delta power and the increase of the relative alpha power in the ipsilesional frontal area were significantly correlated with the FM improvement (F5, F7, FC1, and Fz electrodes, all |r| > 0.517, p < 0.040).
Conclusions:
The curative effect of XNKQ acupuncture related to its electrophysiological modulation.
This study was registered at the Chinese Clinical Trial Registry (ChiCTR2000038560).
Introduction
Acupuncture therapy has been widely used for stroke treatment in China. One of acupuncture methods, that is, Xingnao Kaiqiao (XNKQ), was developed by Xuemin Shi in 1972 for the treatment of cerebral apoplexy. 1,2 Its safety and curative effect in stroke management, especially in the treatment of (sub)acute ischemic stroke, has been widely demonstrated by clinical studies. 3,4 A meta-analysis systematic review of 12 randomized clinical trials concluded that XNKQ acupuncture could significantly reduce the disability rate, elevate the activities of daily living, and had greater efficacy for treatment of (sub)acute ischemic stroke as compared with the control treatments. 3
Previous studies have led to substantial advances in our understanding of the neural mechanism underlying XNKQ acupuncture. One of such reviews deduced that XNKQ acupuncture could influence multiple serum molecules, and increase cerebral blood flow (CBF) and cerebral oxygen metabolism in stroke patients. 5 A recent functional magnetic resonance imaging (fMRI) study also suggested that XNKQ acupuncture could modulate the functional connectivity of motor areas. 6 XNKQ acupuncture has also been proven to modulate the brain's electrophysiological activities. For instance, acupuncture at one of the main acupoints of XNKQ, that is, nei guan (PC6), has been said to increase alpha power and synchronization, 7 evoke P300 component 8 and change the topology of the brain functional network. 9 However, these electrophysiological modulations were all observed in healthy subjects and remain unknown in stroke patients.
In a previous study, we investigated another acupuncture method (i.e., Jin's triple-needle acupuncture), and found an intermediate modulation on the alpha oscillations by acupuncture in stroke patients. 10 Nonetheless, the long-lasting electrophysiological effect of acupuncture is yet to be investigated to understand its mechanisms as a treatment for stroke. Considering the electrophysiological effect of XNKQ acupuncture in healthy subjects and other acupuncture methods in stroke patients, we hypothesize that XNKQ acupuncture could also modulate brain electrophysiological activities of stroke patients, and hereby show encouraging long-lasting effects with consecutive treatment sessions.
Electrophysiological evaluation based on electroencephalogram (EEG) or magnetoencephalogram is of great clinical significance for quantification and monitoring of neuronal changes in poststroke treatment and recovery. Various quantitative EEG (qEEG) measurements, such as frequency-specific power has been reported to be strongly associated with stroke outcome, suggesting their prognostic and predictive values in (sub)acute stroke. 11,12 Their evaluation and monitoring capabilities have also been well established, for example, during thrombolytic therapy or in brain–computer interface and transcranial direct current stimulation rehabilitation. 11,12 Therefore, in this study, we used a qEEG measurement (i.e., relative EEG power), and aimed to study the modulation of brain rhythm oscillations by XNKQ acupuncture and its correlation with stroke recovery.
Materials and Methods
Ethics statement
This study was approved by the Ethics Committee of the Minhang branch, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine. Before any study was performed, each subject or his/her legally acceptable representatives provided written informed consent in compliance with the Declaration of Helsinki.
Study design and subjects
This study was an assessor-blinded, pretest–posttest, randomized, controlled study. Twenty patients with (sub)acute cerebral infarction (≤14 days after stroke onset) were recruited from the Department of Neurology, Shanghai Minhang Hospital of Integrated Traditional Chinese and Western Medicine. They were randomly assigned to two groups at a ratio of 1:1, that is, an acupuncture group (AG, n = 10), in which patients received acupuncture treatment combined with conventional treatment, and a control group (CG, n = 10) with conventional treatment only. The allocation sequence was based on a computer-generated random number table. The fifth author enrolled the participants, and the eighth author allocated the patients to different groups.
Outcome measures
Movement impairments and neurologic deficits of patients were measured using the National Institute of Health Stroke Scale (NIHSS), the Fugl-Meyer (FM) Scale, the Modified Rankin Scale (mRS), and the Modified Barthel Index (MBI) before treatment (baseline), as well as and at 14 days after and 30 days after treatment onset by an independent physician who was blinded to the treatment condition.
The NIHSS is a 15-item impairment scale with a total maximum score of 42 points, which provides a quantitative measure of key components of a standard neurological examination. 13 A score of zero indicates no clinically relevant neurological abnormality, and a score ≥20 usually indicates a dense paralysis with impaired consciousness. The MBI measures ten basic aspects of activity related to self-care and mobility. 14 The normal score is 100, and lower scores indicate greater dependency. The mRS has been commonly used to assess disability after a stroke with seven different grades: 0–5 indicate from no symptoms to severe disability, and 6 indicates death. 15
The FM scale is an evaluative measure of recovery from hemiplegic stroke. 16 It covers five domains, and the motor domain was measured in this study. The motor domain includes items measuring movement, coordination, and reflex action about the shoulder, elbow, forearm, wrist, hand, hip, knee, and ankle, ranging from 0 (hemiplegia) to a maximum of 100 points (normal motor performance). It contains 33 items for the upper extremity and 17 items for the lower extremity, and each item is scored on a 3-point ordinal scale (0 = cannot perform, 1 = performs partially, 2 = performs fully).
Inclusion criteria
All patients (1) had to conform to Chinese acute ischemic stroke diagnosis and treatment guidelines 2018, 17 (2) first-ever stroke patients, (3) with infarction in the basal ganglia region diagnosed by CT or MRI, (4) conscious and stable vital signs, (5) 4 ≤ NIHSS ≤15, (6) less than 2 weeks after stroke onset, and (7) had to be in a stable medical condition, without aggravating symptoms.
Exclusion criteria
Patients with (1) a history of stroke, (2) cerebral tumor, (3) mental disorders, (4) extrapyramidal damage (such as Parkinson's syndrome), (5) cardiac arrhythmias, (6) severe primary cardiovascular, liver, kidney or hematopoietic diseases were excluded before the study. Patients with (7) prior neurologic deficits, (8) seizures, (9) hemorrhagic stroke, (10) needle phobia, (11) skin injury, eczema, infection, (12) skull defect, or (13) bedsore as well as (14) pregnant or lactating women were excluded.
Conventional treatment
All patients received conventional Internal Medicine treatment according to Chinese acute ischemic stroke diagnosis and treatment guidelines 2018, 17 including antiplatelet therapy, lipid-regulating therapy, plaque-stabilizing therapy, and other symptomatic treatments.
Acupuncture treatment
Patients in AG received additional XNKQ acupuncture treatment once a day for 10 consecutive days. The main acupoints included the bilateral PC6 points (nei guan), GV26 point (shui gou), and SP6 point on the affected side (san yin jiao). The auxiliary acupoints included HT1 point (ji quan), LU5 point (chi ze), and BL40 point (wei zhong) on the affected side. The matching acupoints included GB20, SJ17, and GB12 for dysphagia, LI4 for hand inflexible, RN23 and EX-HN12 for language disadvantage, and GB40 point-through-KI6 point for talipes varus.
PC6 is located 2 cm above the transverse crease of the wrist, between the tendons of radial wrist flexor and palmaris longus. GV26 is located at the junction of the upper one-third and middle one-third of the philtrum. SP6 is located 3 cm above the tip of the medial malleolus, behind the posterior border of the medial aspect of the tibia. HT1 is located in the middle of the axilla, where the axillary artery pulsates. LU5 is located on the transverse line of the elbow and on the radial side of the biceps tendon. BL40 is located at the midpoint of the transverse popliteal stria, between the biceps femoris tendon and the semitendinosus tendon.
The acupuncture treatment was delivered by an acupuncturist from Shanghai Minhang Hospital of Integrated Traditional Chinese and Western Medicine who had been trained in Beijing University of Traditional Chinese Medicine for 7 years and with 5 years of clinical experience. All patients were kept in a supine position during the acupuncture treatment. Sterile disposable stainless acupuncture needles (diameter: 0.3 mm, length: 40 mm, Guizhou Andi Acupuncture Instruments General Factory, Guizhou, China) were used. No electrical stimulation was applied to the needles. The acupuncture was delivered according to the procedure described by Shi. 18
First, PC6 was punctured bilaterally to a depth of ∼0.5–1 cm and stimulated with the reducing method by lifting and thrusting with simultaneous twirling manipulation for 1 min (twirling anticlockwise with the left hand and clockwise with the right hand). Then, GV26 was punctured obliquely toward the nasal septum to a depth of ∼0.3–0.5 cm with birdpecking needling until the eyes became wet or developed tears. Subsequently, SP6 was punctured on the affected side obliquely along with the medial border of the tibia to a depth of ∼0.5–1 cm, with lifting and thrusting reinforcing manipulation, thrusts with heavy strength and lifting with gentle strength for 1 min.
HT1 was punctured on the affected side ∼1 cm below the source point along the channel in avoidance of axillary hairs, and the needle was inserted perpendicularly for ∼1–1.5 cm, with the reducing manipulation by lifting and thrusting until the ipsilateral upper limb had three tics. The elbow on the affected side was flexed to 120° for acupuncture at LU5, and the needle was inserted perpendicularly for ∼1 cm, applying the reducing manipulation by lifting and thrusting until the ipsilateral upper limb had three tics. BL40 was punctured to a depth of ∼0.5–1.0 cm, and the reducing manipulation by lifting and thrusting was applied until the ipsilateral lower limb had three tics with straight leg elevation in the supine position. All the above acupoints were kept for 20 min before taking out.
EEG recording and processing
Ten minutes of resting EEG signals were recorded before treatment, 14 days after, and 30 days after treatment onset, respectively, using a 64-channel EEG cap with a wireless EEG amplifier (NeuSen.W64; Neuracle, Changzhou, China) at a sample rate of 1000 Hz. The vertical electrooculogram (VEOG) was recorded by an electrode beneath the right eye. All electrodes (including FP1, FP2, FPz, AF3, AF4, AF7, AF8, F1, F2, F3, F4, F5, F6, F7, F8, Fz, FC1, FC2, FC3, FC4, FC5, FC6, FT7, FT8, C1, C2, C3, C4, C5, C6, Cz, T7, T8, CP1, CP2, CP3, CP4, CP5, CP6, CPz, TP7, TP8, TP9, TP10, P3, P4, P5, P6, P7, P8, Pz, PO3, PO4, PO5, PO6, PO7, PO8, POz, O1, O2, Oz, and VEOG) were referenced to FCz, with impedance kept below 10 kΩ. The patients were seated on a comfortable chair, and they were instructed to be in a resting state with eyes closed for EEG recording.
The EEG signals were preprocessed offline with the EEGLAB script implemented in MATLAB (MATLAB R2018b; The MathWorks, Inc., Natick, MA, USA). The EEG data were first filtered with a 0.1–40 Hz band-pass filter and a 50 Hz notch filter. Then the EEG signals were re-referenced to the average of all scalp electrodes. One 3-min artifacts-free epoch at the middle of the 10-min resting EEG was selected for Fast Fourier Transform. Relative power in delta (1–4 Hz), theta (4–8 Hz), alpha (8–13 Hz), and beta (13–30 Hz) bands were calculated, respectively, for statistical analysis. All right lesions were flipped to the left side. Therefore, after flipping, the right side was tagged as the contralesional side, and the left side as the ipsilesional side.
Statistical analysis
Clinical scores and relative EEG power were compared between the two groups at each time point (i.e., before treatment, 14 days after treatment onset, and 30 days after treatment onset). Their changes in the first 14 days, between 15 and 30 days, as well as in the whole 30 days were also compared between the two groups. Between-group comparisons were carried out using independent t-tests (for the normally distributed data) or Mann–Whitney U tests (for the data significantly different from normal distributions). Chi-square test was performed to compare sex between the two groups.
Significant changes in clinical scores and relative EEG power during recovery in each group were obtained by comparing among different time points, which were carried out using paired t-tests (for the normally distributed data) or Wilcoxon matched-pairs signed-rank tests (for the data significantly different from normal distributions). The normality of variables was tested by Shapiro–Wilk's test.
To reduce the family-wise error rate, we used a cluster-based permutation test, 19 in which clusters are defined as groups of neighborhood electrodes, which had p < 0.1. The condition labels of EEG recordings were permutated randomly for 1000 times. Maximum cluster size (number of EEG electrodes in one cluster) was obtained in each permutation. The significance of test cluster was defined as the probability that the maximum cluster size of one permutation is larger than the size of test cluster, which was accepted as p < 0.05.
Correlation between the changes in relative EEG power and the improvement in clinical scores were tested using partial correlation analysis, in which age and days after stroke onset were used as covariates.
Results
Clinical outcomes
Two patients in AG and one patient in CG could not tolerate the acupuncture treatment and quitted the study, and another patient in CG died from a severe hematologic disease. Therefore, eight patients in AG (sex: 6M2F, age: 69.38 ± 7.21 years, lesion side: 7L1R, 5.25 ± 1.75 days after stroke onset) and eight patients in CG (sex: 7M1F, age: 69.38 ± 11.72 years, lesion side: 4L4R, 8.88 ± 4.61 days after stroke onset) were included in the analysis. There were no significant differences between the two groups in sex, age, days after stroke onset, and clinical scores before the treatment (all p > 0.11, Table 1).
Demographic and Baseline Clinical Characteristics of Participants
All the data are presented as mean ± SD.
AG, acupuncture group; CG, control group; FM, Fugl-Meyer; F, female; M, male; MBI, Modified Barthel Index; mRS, Modified Rankin Scale; NIHSS, National Institute of Health Stroke Scale; SD, standard deviation.
Both groups showed significant recoveries from clinical outcomes (Table 2). Compared with baseline (before treatment), both groups showed significant improvements in NIHSS, FM scale, mRS, and MBI at 30 days after treatment onset (all p < 0.05). However, earlier recovery in the first 14 days was only found in AG, since AG showed significant improvements in all scores (all p < 0.05), but CG showed significant improvements only in mRS in this period. The clinical improvements in the latter 15–30 days were found to be significant only in AG when measured using FM Scale.
Clinical Outcomes for the Treatments
p-Value for the independent t-test/Mann–Whitney U test when comparing between the two groups.
p < 0.05, ** p < 0.01, *** p < 0.01 for the paired t-test/Wilcoxon matched-pairs signed-rank test when comparing within each group; Posthoc power is provided in brackets; All the data are presented as mean ± SD.
Overall, the clinical improvements in AG were larger than CG, especially significant for NIHSS in the first 14 days (AG = 2.00 ± 1.60, CG = 0.25 ± 0.46, p = 0.02, posthoc power = 0.84), and FM score in the latter days (AG = 9.5 ± 5.86, CG = 2.5 ± 4.11, p = 0.01, posthoc power = 0.80), as well as in the whole 30 days of recovery (AG = 23.13 ± 9.57, CG = 9.13 ± 10.37, p = 0.02, posthoc power = 0.79).
EEG results
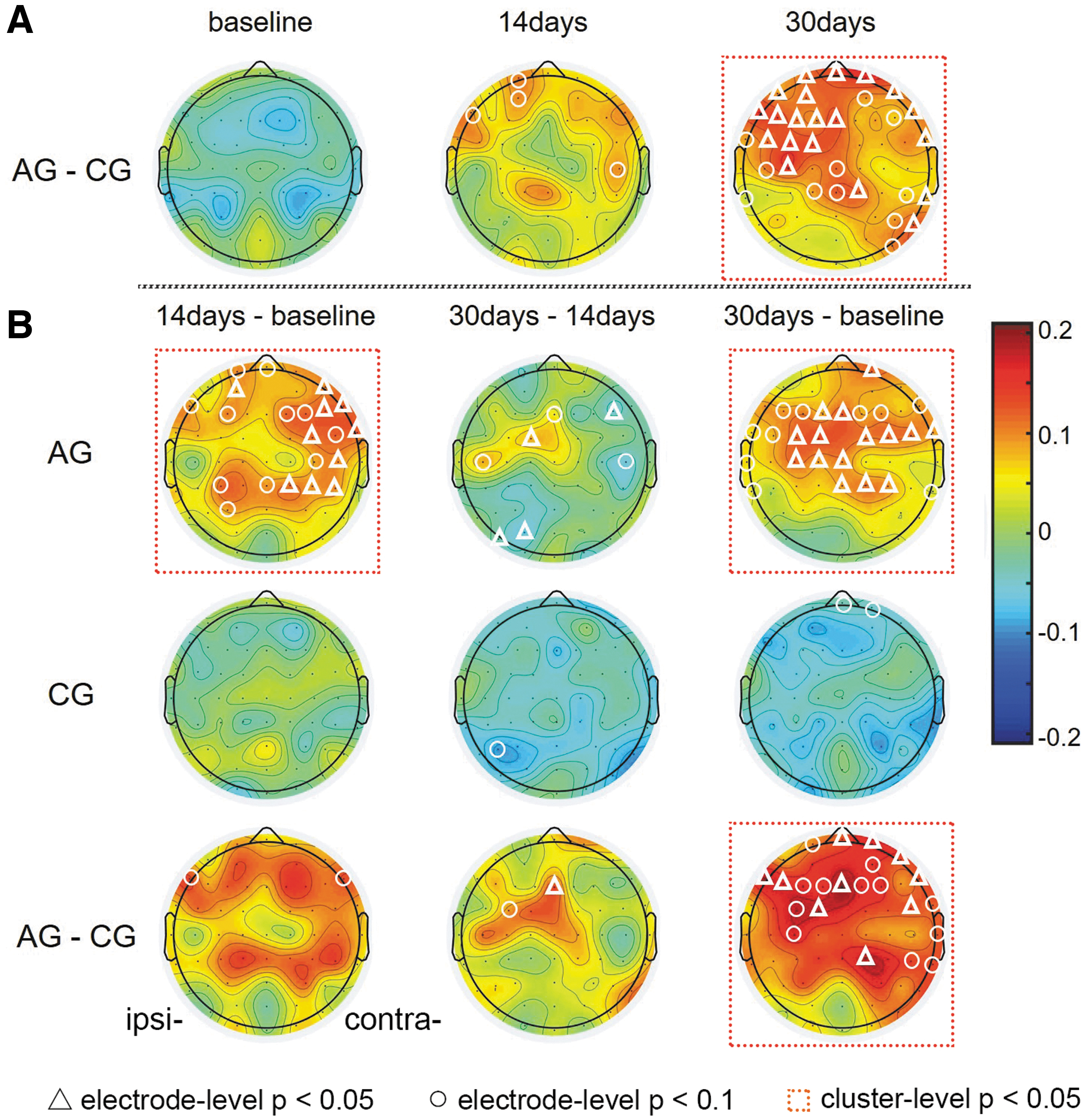
The delta band was found to be altered during the 30 days of treatment (Fig. 1 and Supplementary Table S1). The relative delta power was comparable between the two groups before treatment or at 14 days. However, at 30 days after treatment onset, the AG showed lower delta power than CG in almost all the cortical areas, which were significant in the ipsilesional frontocentral and contralesional areas (Fig. 1A). In the first 14 days, the relative delta power in AG was decreased in almost all the cortical areas, which were significant in the bilateral parietocentral areas (CP3, CP4, CP6, and Pz, all p < 0.05, average posthoc power = 0.64 ranging from 0.60 to 0.67). While in the latter days, the relative delta power in AG was significantly decreased only in the ipsilesional frontocentral area (FC1 and Fz, both p < 0.05, posthoc power = 0.85 and 0.67, respectively).

Relative delta power results.
Taking the whole 30 days into consideration (30 days vs. baseline), the relative delta power in AG was significantly decreased in the ipsilesional frontocentral area (FC1, FC3, C3, Cz, and CPz, all p < 0.05, average posthoc power = 0.78 ranging from 0.66 to 0.92). However, almost no significant changes in the delta band were observed for CG during the whole period. During the 30 days of treatment, the two groups showed significantly different changes at FP2, Fz, FC1, F5, and F7 electrodes (all p < 0.05, average posthoc power = 0.67 ranging from 0.57 to 0.80). Only the group difference at 30 days can pass the cluster-based permutation test (Fig. 1B).
Our results also reflect significant changes in the alpha band (Fig. 2 and Supplementary Table S2). Similar to the delta band, the alpha band also showed comparable relative power between the two groups before treatment or at 14 days, but at 30 days after treatment onset, the AG showed higher alpha power than CG in almost all the cortical areas, which was significant in the frontal and central areas (Fig. 2A). In the first 14 days, the relative alpha power in AG was increased in almost all the cortical areas, which was significant in the contralesional frontal, central, and parietal areas (AF8, F6, F8, FC4, FT8, C6, CP2, CP4, and CP6, all p < 0.05, average posthoc power = 0.73 ranging from 0.59 to 0.88). Meanwhile in the next 15 days, not much changes were observed in AG.
Relative alpha power results.
Taking the whole 30 days into consideration, the relative alpha power in AG was significantly increased in the bilateral frontal and central areas (FP2, F1, Fz, FC1, FC2, FC3, FC4, FC6, FT8, Cz, C1, C3, CPz, CP2, and CP4, all p < 0.05, average posthoc power = 0.73 ranging from 0.61 to 0.96). Different from the increment in AG, the relative alpha power was decreased in CG after treatment, but no significant results were obtained. During the 30 days of treatment, the two groups showed significantly different changes at FPz, FP2, AF8, F8, FC6, CP2, Fz, FC1, F5, and F7 electrodes (all p < 0.05, average posthoc power = 0.67 ranging from 0.59 to 0.90). The group difference in the ipsilesional frontal and central areas at 30 days, the increment in AG in the first 14 days or whole 30 days, as well as different group changes in the frontocentral area can pass the cluster-based permutation test (Fig. 2B).
Both groups showed no significant changes in the theta and beta bands (all p > 0.05).
Correlation results
Considering that the relative power in the delta and alpha bands showed distinct changes between the two groups in 30 days of treatments, these EEG indices were further correlated with the improvement in the FM scale to test whether the different changes in EEG relative power reflect electrophysiological mechanism of curative effect of acupuncture. Those electrodes with significant group differences (i.e., FP2, Fz, FC1, F5, and F7 for the delta band; FPz, FP2, AF8, F8, FC6, CP2, Fz, FC1, F5, and F7 for the alpha band) were selected for correlation analysis (Fig. 3).

Partial correlations between the change of relative EEG power
We found that the decrease of the relative delta power in the ipsilesional frontal area was significantly negatively correlated with the FM improvement (F5, F7, FC1, and Fz, all r < −0.517, p < 0.040). Also, the increment of the relative alpha power in the bilateral frontal area was significantly positively correlated with the FM improvement (F5, F7, FC1, Fz, F8, and FC6, all r > 0.531, p < 0.034).
Discussion
In this study, using clinical scores and electrophysiological measures, we investigated the modulation of brain rhythm oscillations by XNKQ acupuncture, which correlates with stroke recovery. To the best of our knowledge, this is the first study exploring the long-lasting electrophysiological effect of acupuncture treatment in stroke patients.
First, better recovery was obtained by use of XNKQ acupuncture treatment in (sub)acute ischemic stroke patients, which were in line with dozens of previous clinical comparative studies. 2,3 It should be noted that the effect of XNKQ acupuncture seems most evident on FM score. One possibility is that the enrolled patients were all with lesions in the basal ganglia area and with main symptoms of sensorimotor dysfunction, and it is well proven that patients suffering from motor deficits react especially well to XNKQ acupuncture. 20 As FM score is more focused on the sensorimotor dysfunction, while MBI and mRS involve more questions on daily activities and special functional defects, and NIHSS evaluates the whole neurological deficits, such as consciousness, visual field, cranial nerves, cerebellar, sensation, and speech, it makes more sense that FM score reflects more sensitivity for the efficacy of XNKQ acupuncture. MBI also has “well-recognized floor and ceiling” effects, 21 –23 that is, items for assessment are too difficult or easy to sensitively detect clinical changes.
Second, XNKQ acupuncture treatment showed long-lasting modulation on EEG oscillations. The AG showed decreased relative delta power and increased relative alpha power after treatment, whereas no significant changes were found in the CG.
Previous studies have found a rapid appearance of high-amplitude delta oscillations after ischemic stroke, which even occurs within 24 h after onset of symptoms, followed by depression of alpha or beta oscillations. 12 More specifically, alpha and delta power are closely related to the recovery of cerebral infarction and have been suggested as independent predictors of the prognosis after stroke. 11,24 These EEG oscillations seem to be modulated by acupuncture. Muchtadi et al. found that the EEG power was higher in the alpha and theta bands during acupuncture, hence, indicating its relaxing effect on the human mind. 25 Yu et al. showed a higher synchronization in the delta and alpha bands by acupuncture at the “Zusanli” acupoint. 26 Chang et al. demonstrated that acupuncture at one of the main acupoints of XNKQ (i.e., PC6) could increase alpha power and synchronization. 7
The modulation of EEG by acupuncture has not only been evident in healthy subjects but also observed in stroke patients. In our previous study, we found an intermediate effect of Jin's triple-needle acupuncture on the alpha oscillations in stroke patients. The alpha amplitude increased when inserting and removing the needles, with its high amplitude remaining during retention and after removal of the needles. 10 Our current study goes further to demonstrate that the immediate effect of acupuncture on EEG oscillations could be accumulated by consecutive treatment sessions. After XNKQ acupuncture treatment, the delta oscillations decreased and the alpha oscillations increased at the same time.
The simultaneous changes in alpha and delta oscillations might be two reflections of CBF improvement by XNKQ acupuncture. The delta activity was found to have the strongest correlation with regional CBF in unilateral cerebral infarction patients. 27 A simultaneous fMRI and EEG study also displayed a close spatial correspondence between CBF and changes in alpha power, and the alpha power was significantly correlated with the CBF amplitude. 28 Especially in cerebral infarction patients, the alpha power showed a positive correlation with regional CBF. 28 On the other hand, previous studies have found that acupuncture stimulation could increase CBF. For instance, a PET study concluded that acupuncture stimulation at the ‘Deqi’ acupoint increased blood flow in the hypothalamus, insula, and subcortical structures. 29 In stroke patients, the average blood flow velocity in the brain showed an increase during acupuncture treatment (needle retention) and after needle removal. 30 After 4 weeks of XNKQ acupuncture treatment of chronic cerebral infarction, the CBF velocity in the middle cerebral artery was increased. 31 –33 We speculate that XNKQ acupuncture could also increase the CBF in the (sub)acute ischemic stroke patients and simultaneously induce a decrease in the delta oscillations and an increase in the alpha oscillations. However, the CBF was not measured simultaneously with EEG, which is a limitation of this study.
The increase of alpha oscillations and decrease of delta oscillations may also indicate a relief of subcortical and cortical injury by XNKQ acupuncture, since the abnormal delta activity has been found to reflect cortical deafferentation due to subcortical injury, whereas the alpha activity disturbances, such as attenuation or slowing, are generally indicative of cortical injury. 34
It should be noted that the decrease in the relative delta power and the increase in the relative alpha power were regionally distinct between the first 0–14 days and in the latter 15–30 days. Both changes in the delta and alpha bands occurred initially in the intact hemisphere and later partly transferred to the peri-infarct cortex. Similarly, functional brain imaging studies suggested that lost functions would initially shift toward the intact hemisphere and later, as the inflammation subsides and blood flow improves, those functions are taken over by the peri-infarct cortex. 35,36 Furthermore, the improvement of FM score was significantly correlated with the degree of delta decrease and alpha increase in the ipsilesional frontal area, suggesting that the better recovery obtained by XNKQ acupuncture treatment was related to its modulation on EEG oscillations with main targets localized in the ipsilesional frontal area.
There are some limitations to this study. First, the sample size is small in this study and therefore hinders the power of statistical analyses. Only some significant differences were observed in independent or paired comparison for each electrode. However, cluster-based permutation test with a relatively loose p-value threshold (<0.1) suggested that some electrodes with significant results formed clusters, which might not be accounted for random fluctuation. Second, most of the recruited patients are male. The low number of female participants might impair the generalizability of our conclusion. Future studies with more female participants are needed to confirm our results. Third, this study did not design a CG with sham acupuncture and therefore could not exclude the effect of simple sensory stimulation by needling. Furthermore, we only followed up the patients for 30 days, the long-term outcome and electrophysiological effect of XNKQ should be investigated in future with a longer follow-up.
Conclusion
From our limited sample size, XNKQ acupuncture treatment showed a tendency to obtain better motor recovery in (sub)acute ischemic stroke patients, which is correlated with its electrophysiological modulation manifested by decreased relative delta power and increased relative alpha power. The results extend the knowledge of XNKQ acupuncture treatment to its electrophysiological mechanism, and suggest XNKQ acupuncture as an effective intervention for (sub)acute ischemic stroke patients, especially for those with significant changes in EEG delta and alpha oscillations. Since the electrophysiological response can reflect the treatment efficacy, it also provides a possibility to use EEG to help tailor individualized acupuncture treatments, such as selection of best acupoints or optimal manipulations for each patient.
Footnotes
Authors' Contributions
X.G. and J.Z. designed the study. X.G. and X.Z. drafted the article and all the other authors revised the article. X.Z., L.Y., M.S., and C.Q. collected EEG data, and X.G., L.Y., M.S., and C.Q. analyzed EEG data. J.Z., W.X., Y.X., and Z.J. enrolled the participants and performed clinical assessments. T.X. discussed results and revised the article. All coauthors have reviewed and approved of the article before submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Natural Science Foundation of China (No. 61771313), Shanghai Jiao Tong University Grant (No. YG2021ZD23), Clinical Research Program Foundation of Shanghai Health and Family Planning Commission (No. 201840320), Natural Science Research Project of Minhang District, Shanghai (No. 2020MHZ085), and Research Project of Traditional Chinese Medicine of Shanghai Health and Family Planning Commission (No. 2020_LP042).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.