
Abstract
Background and objectives:
The effect of auricular acupressure (AA) for maintenance hemodialysis (MHD) patients with insomnia has been controversial. This study assessed the efficacy and safety of AA for MHD patients with chronic insomnia.
Design, setting, participants, and measurements:
This was a multicenter, double-blind (participant and assessor), randomized sham-controlled trial. A total of 133 subjects were randomized to receive AA on active points (AA group, n = 64) or on sham auricular acupressure (SAA) points (SAA group, n = 69) for 8 weeks and followed up for 12 weeks. AA was provided by assigned qualified nurses who were not involved in assessment. The primary outcome was the clinical response rate, which was defined as the percentage of participants who reached a reduction of Pittsburgh Sleep Quality Index (PSQI) global score ≥3 in each group. Secondary outcomes included changes in PSQI scores over time, PSQI scores and hypnotics use at each visit, and changes in the weekly dose of hypnotics for drug-dependent subjects.
Results:
At week 8, the AA group yielded a higher clinical response rate than the SAA group (AA: 55% vs. SAA: 36%, odds ratio: 1.5, 95% confidence interval: 1.0–2.2, p = 0.033). Both groups showed a reduction in PSQI global scores during treatment and follow-up, compared with the baseline, respectively. A significant change of PSQI global score was observed over time (F = 28.387, p < 0.001). PSQI global score of the AA group was relatively lower than that of the SAA group at each visit (p < 0.05 at week 16 and 20). For those depending on hypnotics, AA reduced their consumption of hypnotics. The intervention was safe, and its adherence was satisfactory.
Conclusion:
AA could serve as a complementary or alternative therapy for MHD patients with insomnia by improving their sleep quality and reducing their use of hypnotics.
Clinical trial registration:
Clinicaltrials.gov, Identifier: NCT03015766.
Introduction
Insomnia is common in advanced chronic kidney disease (CKD) patients on maintenance hemodialysis (MHD), with the prevalence ranging from 44% to 68.2%. 1 –5 Insomnia has an adverse impact on patients' quality of life, 6,7 mental health, 8 and social anxiety. 9 Moreover, it has been associated with increased mortality among MHD patients. 10 –12
Hypnotics are usually taken to ease this situation. In a single-center cross-sectional study, 42.6% of hemodialysis patients were using benzodiazepines, and 20.0% were using other hypnotics. 13 Prolonged use of hypnotics is linked to potential adverse effects such as memory impairment, risk of falls, drug dependence, and addiction. 14 It is widely acknowledged that hypnotics should be limited to the lowest necessary dose and shortest necessary duration. 15,16 Thus, effective nonpharmacological interventions for insomnia management are always warranted.
Auricular acupressure (AA), a typical type of auriculotherapy, is popular in China and elsewhere around the world. AA adopts seeds, magnetic pellets, or lasers to stimulate specific acupoints on the auricle treating physical and psychosomatic dysfunctions. Dr. Paul Nogier, a physician in France, first proposed the inverted fetus map showing the relationship between the external ear and all parts of the whole body. In China, the Traditional Chinese Medicine (TCM) theory is integrated into this therapy in the aspect of acupoint selection.
From the TCM perspective, common pathophysiologic patterns of insomnia are summarized as non-interaction between heart and kidney, liver–stomach disharmony, hyperactivity of liver yang, and deficiency of both heart and spleen. Therefore, by stimulating points related to the involved inner organ, the yin yang harmony is expected to come to a balance, resulting in sleep quality improvement.
Based on this knowledge, we provided AA for MHD patients with insomnia as complementary therapy in clinical practice. Previously, we reported a 4-week AA intervention for MHD patients with severe insomnia, which led to significantly improved sleep quality and reduced sleep medication intake. 17 In a pilot study, MHD patients who received TCM-based AA had more responders (AA vs. control: 62.5% vs. 32.3%, p = 0.02). 18 In this study, we aimed at further clarifying the efficacy and safety of AA for insomnia in hemodialysis patients by a rigorously designed trial.
Methods
The trial was approved by the Ethics Committee of Guangdong Provincial Hospital of Chinese Medicine (No. B2016-137-01). The authors adhered to the tenets of the Declaration of Helsinki and its amendments. Written informed consent was taken from all individual participants. The trial was registered at
Study design
This was a multicenter, double-blind (participant and assessor), randomized controlled trial (RCT) of AA versus sham auricular acupressure (SAA) for MHD patients with insomnia conducted in dialysis centers of six tertiary care hospitals of TCM in Guangdong, China. The study duration consisted of an 8-week treatment period and an additional 12-week follow-up period without intervention.
Participants
Clinical physicians in Hemodialysis departments enrolled participants. Patients on MHD with a sufficient dialysis dose (weekly dialysis time ≥10 h) were eligible if they were 18–75 years old (either gender); had chronic insomnia diagnosed by a psychiatrist according to The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). 19 The MHD referred to a status for advanced CKD patients receiving twice or thrice weekly hemodialysis for ≥3 months. The diagnostic criteria of CKD followed the National Kidney Foundation (NKF) Kidney Disease Outcomes Quality Initiative (K/DOQI) clinical guidelines. 20
Exclusion criteria included: (1) the presence of comorbidities, including cancer, congestive heart failure, connective tissue disease, and hematological diseases; (2) dialysis adequacy parameter Kt/V (K for the dialyzer clearance of urea, obtained from the manufacturer; t for the duration of dialysis session; V for the volume of distribution of urea in the body) <1.20; (3) the presence of severe physical symptoms, such as bone pain, itchy skin, sleep apnea, and restless legs, which could potentially explain their sleep problem; and exhaustion caused by severe anemia (hemoglobin <60 g/L) or malnutrition (serum albumin <30 g/L); and (4) infection or abnormality in the external ear area.
Randomization and blinding
Randomization was stratified by site. It was performed to allocate eligible subjects to either AA group or SAA group at a 1:1 ratio. A web-based network (ResMan® Clinical Trial Management Platform) generated a random number sequence and allocation results by the simple randomization method, which were obtained through the network by the research coordinator of each trial center. This network system was controlled by a third party, so the random number sequence was concealed from researchers. Research coordinators applied for allocation information through this online system only when a new eligible participant was about to start treatment.
Both the participants and the assessors were blinded to the allocation and interventions. The participants had no previous knowledge about acupoints. They were told that we were comparing two AA protocols, and that both could be effective. Two nurses in each center were assigned to provide AA for patients. They had an equal chance to perform each protocol. All auricular points involved were named as numbers and letters.
They were required not to discuss the difference of two protocols or the effect of treatment. The nurses were not involved in assessment. Another investigator in each center was assigned to assess sleep quality in an interview. He/she had neither any interaction with participants during the treatment period, nor access to information on allocation and interventions. More details about randomization, concealment, and blinding have been stated in previously published study protocol. 21
Interventions
All participants received regular hemodialysis and instructions for self-manipulation of AA. Participants in both groups received sleep hygiene education as well as CKD-related health management, including regular hemodialysis. The interventions of the two groups were otherwise the same, except the acupoints selected. For the intervention group (AA group), participants received AA on specific acupoints, that is, Shen Men (Spiritual Gate, TF4), Jiao Gan (Sympathetic autonomic, AH6a), Xin (Heart, CO15), Pi Zhi Xia (Subcortex, AT4), and Nei Fen Mi (Endocrine, CO18).
For the control group (SAA group), the acupoints for AA were five helix points (HX 5–9) 22,23 (Fig. 1 and Supplementary Material: Rationale for Acupoint Selection). Treatment was provided by assigned research nurses who had gained qualification after training by acupuncturists (with more than 10 years of clinical experience in acupuncture). Research nurses administered auricular paster (size: 1.0 × 1.0 cm, with one bead inside for each point, i.e., Semen vaccariae) for participants and instructed them to press the beads with appropriate strength and rate (1–2 beats per second) for 1 min at each point.
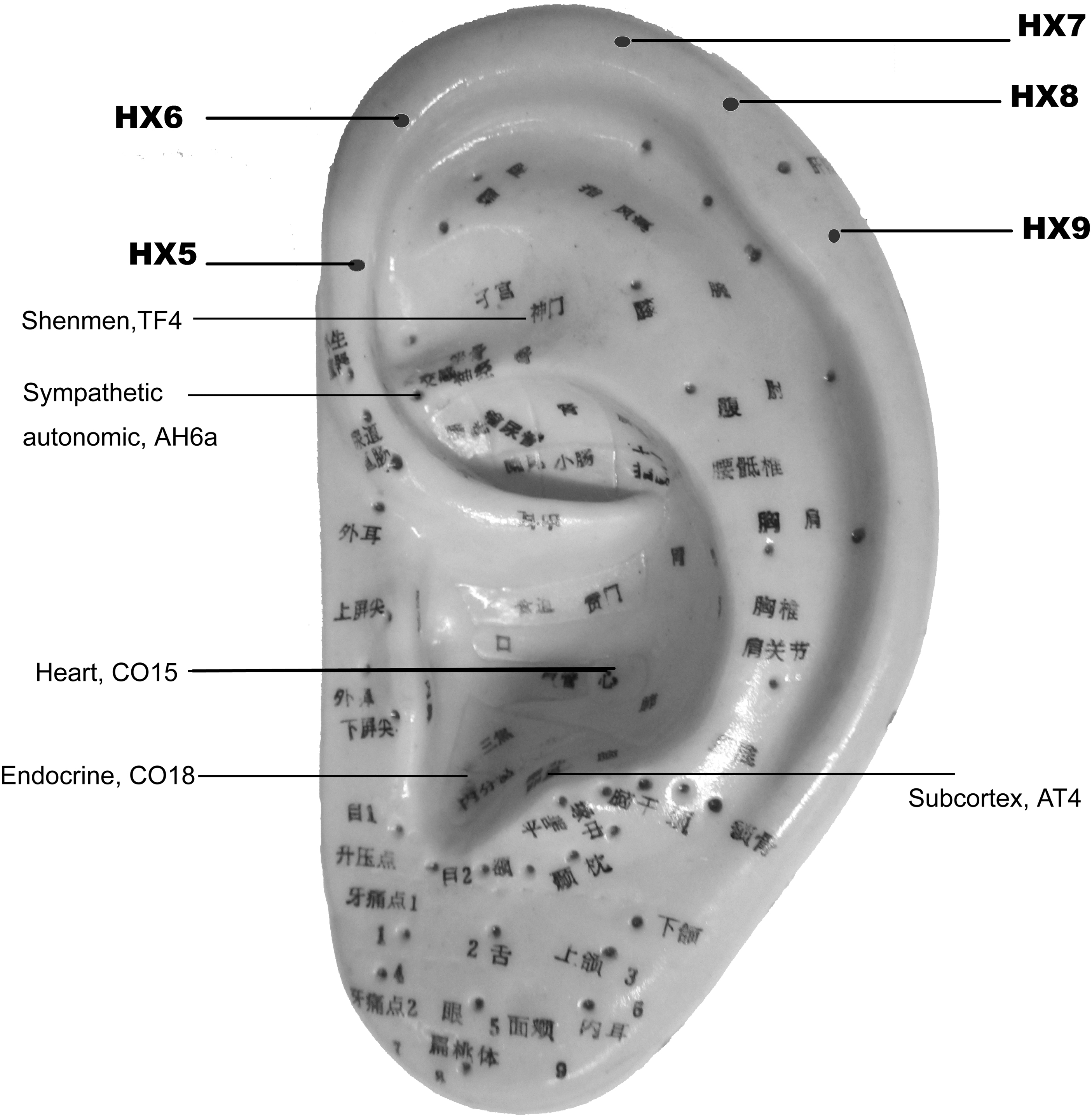
Auricular acupoints in this trial. AA group: Shen Men (Spiritual Gate, TF4), Jiao Gan (Sympathetic autonomic, AH6a), Xin (Heart, CO15), Pi Zhi Xia (Subcortex, AT4), and Nei Fen Mi (Endocrine, CO18). SAA group: HX 5, HX 6, HX 7, HX 8, HX 9.
This self-manipulation was done three times during the day and once in the evening. The replacement of auricular pasters was performed three times a week. The treatment continued for 8 weeks and included 24 sessions for each participant. Standard operating procedures of AA were demonstrated in the Supplementary Material.
Participants were encouraged to avoid using hypnotics. However, when they insisted their need for hypnotics, clinical physicians were allowed to prescribe Estazolam. Participants reported their consumption of Estazolam every time they applied for a new prescription. The information was documented in their medical records.
Outcome measurements
Sleep quality was measured by Pittsburgh Sleep Quality Index (PSQI) at baseline, end of the treatment (i.e., week 8), and every 4 weeks after the treatment. PSQI contains seven domains with scores from 0 to 3, yielding a total score ranging from 0 to 21, where a higher score indicates poorer sleep quality. 24 The reliability and validity of its Chinese version had been confirmed. A global PSQI score over 7 was able to distinguish normal subjects from patients with sleep quality problems with a diagnostic sensitivity of 98.3% and specificity of 90.2% (κ = 0.89, p < 0.01). 25
Primary outcome
The primary outcome was clinical response rate assessed by the change of PSQI global score at the end of treatment (week 8) from baseline. According to a literature review, clinical response was defined as a reduction of the PSQI global score ≥3. 24
Secondary outcomes
Secondary outcomes were (1) changes in PSQI scores (including global score and scores for each domain) at the end of treatment and at each follow-up visit compared with baseline; and (2) the weekly dose of Estazolam for drug-dependent subjects.
Safety outcome
Any adverse event throughout the treatment and follow-up periods.
Sample size
Sample size estimation was reported in published protocol. 21 This trial required a total of at least 112 subjects with a power of 90% and a significance level of 5%, taking a <15% dropout rate into account.
Statistical analyses
The intention-to-treat approach was used. Participants who withdrew from treatment were considered as ineffective cases. Missing data of the continuous variables were input by using the last observation carried forward approach. The primary outcome, clinical response, was analyzed by the Chi-squared test. Number needed to treat (NNT) was calculated to estimate the absolute beneficial effect of AA.
For secondary outcomes, repeated-measures analyses of variance (rANOVA) was conducted to evaluate the changes in PSQI scores over time and the impact of interventions. A comparison based on non-equidistant repeated measurement data was performed by using the SPSS syntax editor. Group differences of PSQI global and component scores at each visit were analyzed by the Independent-Samples Test or Mann-Whitney U Test depending on the distribution of data.
Reduction of the PSQI global score at the end of treatment was analyzed by the Mann-Whitney U test, and proportions of participants on hypnotics were analyzed by the Chi-squared test or Fisher's exact test. In addition, subgroup analyses for participants who were hypnotics dependent or hypnotics free were performed by using the approaches cited earlier.
Per-protocol analysis was conducted by using the data of participants who were fully compliant to the treatment protocols to assess the robustness of the study results. All of the analyses were processed in SPSS Statistics Software 22.0 (IBM Corp., Armonk, NY).
Results
Enrollment and participant disposition
A total of 242 MHD patients were screened during the periods of recruitment (May 2017–April 2018). Among them, 133 eligible subjects were enrolled and randomly assigned to either AA group (n = 64) or SAA group (n = 69) (Fig. 2).
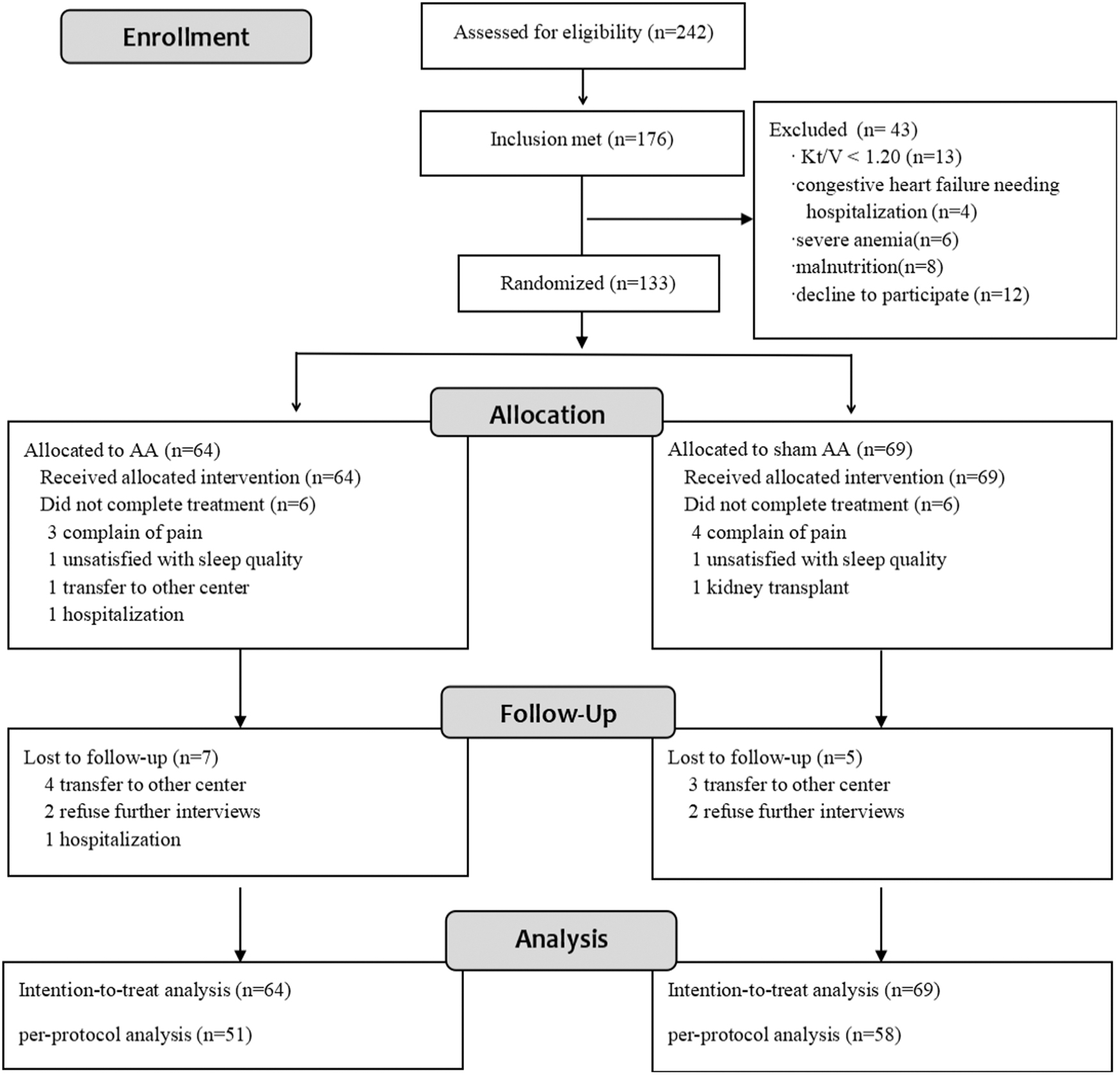
CONSORT diagram showing randomization and interventions of participants.
Twenty-four participants prematurely discontinued the study (12 in the treatment period and 12 in the follow-up period). Common reasons for discontinuation were pain accompanied with the intervention, transferring to other dialysis centers, and hospitalization. There were no major differences in the number of or reasons for premature discontinuation between the two groups.
Baseline participant characteristics
The mean age of participants was 54. They had been undergoing hemodialysis for 4 years on average. The baseline PSQI global score was 13.1 ± 3.0. Twenty-eight percent of them had been taking hypnotics when they entered the trial. There was no significant difference in baseline characteristic conditions between two groups, including age, gender, dialysis vintage, comorbidities, and laboratory tests such as hemoglobin, calcium, phosphorus, parathyroid hormone, albumin, etc. (Table 1).
Baseline Characteristics of Participants
Skewed distributed variable, presented as median (interquartile range); other quantitative variables were presented as mean (standard deviation); numeric variables were presented as n (proportion).
AA, auricular acupressure; HDL-c, high-density lipoprotein cholesterol; Kt/V, a parameter for adequacy of dialysis, which is defined as the dialyzer clearance of urea (K, obtained from the manufacturer in mL/min) multiplied by the duration of the dialysis treatment (t, in min) divided by the volume of distribution of urea in the body (V, in mL); LDL-c, low density lipoprotein-cholesterol; PSQI, Pittsburgh sleep quality index; PTH, parathyroid hormone; SAA, sham auricular acupressure; SCr, serum creatinine; TC, total cholesterol; TG, triglycerides.
Primary outcome
The participants who achieved a clinical response were 35 and 25 in the AA group and SAA group, respectively. The clinical response rate showed a statistically significant difference in favor of the AA group (55% vs. 36%, Relative Risk [RR]: 1.5, 95% confidence interval [CI]: 1.0–2.2, p = 0.033). NNT was 5.4 (95% CI: 2.8–54.3).
Secondary outcomes
Both groups showed a reduction in PSQI global scores at the end of the treatment and during follow-up. Significant changes of PSQI global score over time were observed (F = 28.387, p < 0.001). Significant difference was also found in the interaction between treatment effect and time effect (F = 2.701, p = 0.033), but not in the main effect of treatment (F = 2.451, p = 0.120). In respect to PSQI component scores, time effect was significant in all items, whereas a significant difference in treatment effect was only found in the item of daytime dysfunction (F = 6.328, p = 0.013) (Table 2).
Repeated-Measure Analysis of Variance for Pittsburgh Sleep Quality Index Global Score and Its Components
PSQI, Pittsburgh sleep quality index.
At week 8, PSQI global scores decreased to the minimum (mean reduction: 3.1, 95% CI: 2.4–3.9 in AA group and 2.0, 95% CI: 1.4–2.6 in SAA group). Between-group difference of the week 0–8 reduction did not show significance. During follow-up, PSQI global scores of both groups inclined slightly (Fig. 3). PSQI global score of the AA group was relatively lower than that of the SAA group at each visit, which was statistically significant at week 16 and week 20 (p < 0.05) (Table 3).
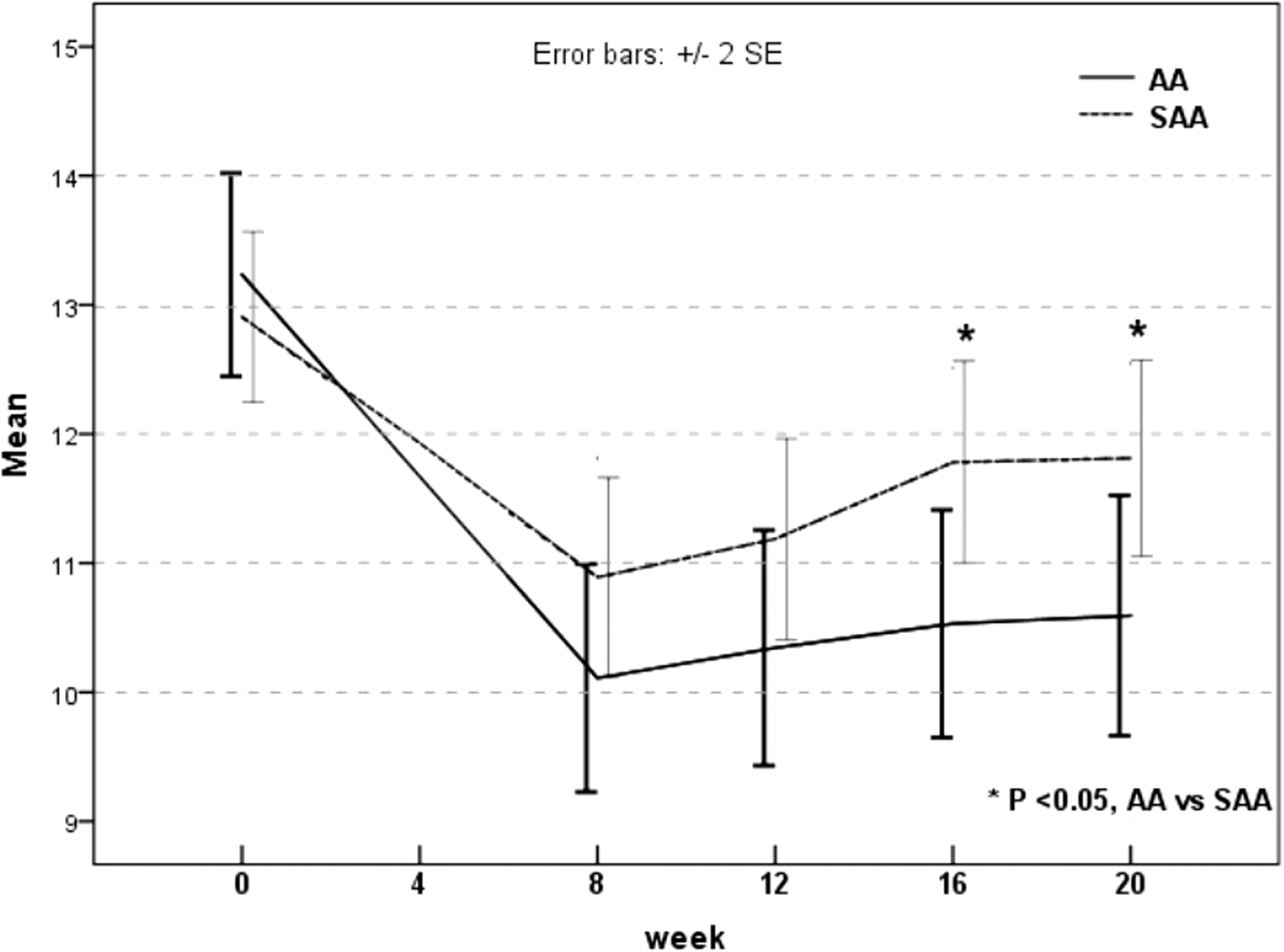
Changes of PSQI global score over time.
Pittsburgh Sleep Quality Index Global Score and Its Components at Each Visit
p < 0.05 versus SAA. Normally distributed data were presented as mean, standard deviation and compared by the independent-samples test; whereas those not fit for normal distribution were presented as median (Q25, Q75) and compared by the Mann-Whitney U test.
AA, auricular acupressure; PSQI, Pittsburgh sleep quality index; SAA, sham auricular acupressure.
Change over time and differences between groups of the weekly dose of Estazolam were not sufficient to show significance. The percentage of the participants taking hypnotics decreased from 31% to 22% at the end of the treatment and further decreased to 17% at the end of the follow-up in the AA group. It changed little during the study in the SAA group (25%, 22%, and 23%, respectively). A group difference of this percentage change was found at the end of the follow-up (AA 14% vs. SAA 1%, p = 0.007).
For those who did not require hypnotics at baseline, 44 were in the AA group and 52 were in the SAA group. It was more likely to be responders in the AA group than in the SAA group after treatment (AA: 59% vs. SAA: 35%, RR: 1.7, 95% CI: 1.1–2.7, p = 0.016). By rANOVA, a significant change of PSQI global score over time (F = 27.330, p < 0.001) and interaction between time and intervention (F = 2.690, p = 0.040) were observed. There were also significant differences between groups on PSQI global scores (F = 4.95, p = 0.03).
At all visits, subjects in the AA group had lower PSQI global scores compared with those in the SAA group (p < 0.05 for all) (Table 4). In this subgroup, there were two participants (one in each group) asking for hypnotics during the follow-up period and none during the treatment period.
Primary and Secondary Outcomes for Subjects Without Sleep Medication
AA, auricular acupressure; CI, confidence interval; PSQI, Pittsburgh sleep quality index; RR, relative risk; SAA, sham auricular acupressure.
For those who were dependent on hypnotics, 20 were in the AA group and 17 in the SAA group. There was a declining trend in the AA group where the number of nights with Estazolam and the average weekly dose of Estazolam were concerned, which was not seen in the SAA group. At the end of the follow-up, subjects in the AA group reported less nights with Estazolam and less consumption of Estazolam than the SAA group subjects, with a significant difference (p < 0.05). Moreover, there were more subjects who were able to quit hypnotics in the AA group than in the SAA group (Table 5).
Subgroup Analyses for Subjects with Sleep Medication
By analysis of variance (ANOVA).
p < 0.05 compared with baseline.
By Fisher's exact test.
AA, auricular acupressure; CI, confidence interval; RR, relative risk; SAA, sham auricular acupressure.
Sensitivity analyses confirmed these findings, providing similar results (Supplementary Material).
Safety outcome
The following suspected adverse reactions were reported during the whole study: pressure pain (n = 8), dizziness (n = 1), and palpitation (n = 1) in the AA group; and pressure pain (n = 9), bruise (n = 1) in the SAA group. No case of skin allergy, lesion, or infection was reported. Most symptoms were mild and bearable.
Adherence
A total of 121 participants completed scheduled treatment. Adherence rate was 91%. As for the adherence of self-manipulation, it seemed to decline slightly over time. In the first 4 weeks, 118 (89%) of the participants stated that they had practiced self-manipulation on auricular acupoints, whereas this number dropped to 91 (68%) in the second 4 weeks.
Discussion
In this trial, MHD patients with insomnia who applied AA designed in TCM principle experienced greater sleep quality improvement in comparison to those who received SAA as a control. After an 8-week AA, participants retained a relatively better sleep quality in the following 12 weeks, compared with those in the control group. For participants who were dependent on hypnotics, AA significantly reduced patients' need for hypnotics and helped more patients quit hypnotics in comparison to those receiving sham intervention.
The findings of this RCT were consistent with most other studies on this topic. A recent meta-analysis assessing AA for insomnia in MHD patients reported that AA was able to reduce PSQI scores compared with mental health education, or increase the response rate compared with Estazolam, SAA, mental health education, or routine nursing care alone. 26 What was distinct from other studies was that by comparing AA with SAA, it highlighted the crucial role of selecting appropriate acupoints.
The present AA protocol was developed following TCM Master Zhang Qi's suggestion and clinical practice. The points selected in this trial mainly aimed at targeting the heart and the spirit. From the TCM perspective, the heart, with a broader conception than the anatomically described organ, is the key system involved in insomnia due to its role as the “seat of consciousness,” the place where the spirit is housed. Sleep disorder is one of the symptoms reflective of disharmony of the heart and dysphoria of the spirit. 27
Both Xin (Heart, CO15) and Shen Men (Spiritual Gate, TF4) are key points of tranquilizing the mind, regulating the function of the cardiovascular system and the central nerve system. Jiao Gan (Sympathetic autonomic, AH6a), Pi Zhi Xia (Subcortex, AT4), and Nei Fen Mi (Endocrine, CO18) synergistically regulate the autonomic nerves, nourish the brain, and calm the mind.
Except for these points, the following acupoints are also frequently seen in literature reporting AA for insomnia: 28 –32 Gan (Liver, CO12), Pi (Spleen, CO13), Shen (Kidney, CO10), and Zhen (Occiput, AT3). Practitioners might choose one (usually TF4) or more (three to nine) acupoints for sleep disturbances. Their prescriptions varied to some extent but still shared something in common.
Almost all the main acupoints are located in the concave parts (i.e., the scaphoid fossa, triangular fossa, the superior and inferior concha), which are mainly innervated by the auricular branches of the vagus nerve (ABVN). It is believed that ABVN links the stimulus from the AA and autonomic nervous system. 33 The AA stimulus that originates from the cutaneous concha travels through the ABVN and reaches the nucleus of the solitary tract, where complex connections between the brain and the viscera exist.
Markers of autonomic tone, such as heart rate, high-frequency heart rate variability (HRV), and salivary amylase, were found to be associated with sleep disorders in Castro-Diehl C's study. 34 Wei et al. also found some correlation between poor sleep quality and autonomic dysfunction (decreased HRV parameters) in hemodialysis patients. 35 Armstrong et al. 36 reported that electroacupuncture treatment on ear points induced a measurable reduction in sympathetic stress, with subsequent improvement in vagal tone and HRV. Thus, we can speculate that AA raises the vagal tone, depresses sympathetic activity, and activates parasympathetic nerves, 37,38 thus targeting one of the critical pathways of sleep problems.
The AA is also applied in the treatment of substance dependence or addiction, but its value remains controversial. 39,40 In this trial, MHD patients in the AA group reported less nights needing hypnotics and a smaller dose of hypnotics without worsening their sleep quality, in comparison to the SAA group. In the end, nine participants in this AA sub-group succeeded in withdrawing from hypnotics.
This finding implied the value of AA as an alternative therapy to deal with dependence on hypnotics and added evidence for auriculotherapy in managing substance dependence. Physicians in dialysis centers could provide a non-drug therapy option for patients who initially require sleep medicine, or add AA to those who have been taking large doses of hypnotics.
The strengths of this trial are as follows: First, to avoid overestimating the effectiveness of AA and to separate the therapeutic effects of AA from placebo effects, we simulated AA in the control group and blinded both participants and assessors rather than setting a blank control. Second, to assess sleep quality properly and conveniently, we adopted PSQI, which was well known and globally accepted. Following the method by PSQI inventors, we defined the reduction of PSQI global score >3 to be a response as a primary outcome. By this method, improvement of sleep quality to be recognized should have both statistical and clinical significance.
This trial had its limitations. First, objective sleep quality measurements were not applied due to lack of equipment. As a compensation, a blinding design of both participants and assessors could limit the subjective bias of evaluation. Second, sleep quality might have been influenced by other clinical factors such as dialysate temperature, intradialysis complications, and any other accompanying symptoms. Third, this trial neither stopped patients' routine hypnotics in enrollment, nor prohibited hypnotics use during the trial. Although a clean environment for the observed intervention was preferred, it would increase patients' suffering and reduce their compliance. After cautious discussion before the trial, the authors decided to keep it close to the clinical practice. Lastly, CI of NNT has a wide range, probably due to the relatively small sample size and low event rate.
To conclude, the 8-week AA could reduce PSQI scores and hypnotics use for patients on MHD, with a retention effect in the 12 weeks post-treatment. This noninvasive intervention provided an option for MHD patients with insomnia.
Reporting Checklist
The authors have completed the CONSORT and STRICTA reporting checklist.
Footnotes
Authors' Contributions
Conception and design: C.Z., Y.W., Q.L., and X.L.. Administrative support: X.Q.W., Q.L., and X.L. Provision of study materials or patients: X.W., Q.L., L.W., D.Z., X.M., A.Q., and A.Y. Collection and assembly of data: Z.Z., L.L., Z.H., Y.L., X.F.W., B.F., H.M., C.C., and X.C. Data analysis and interpretation: Y.W., L.Y., and C.Z. Article writing: Y.W. and L.Y. Final approval of article: All authors.
Acknowledgments
The authors would like to thank Doctor Li Jianmin of the Acupuncture Department of Guangdong Provincial Hospital of Chinese Medicine for training and helpful discussions on topics related to this work.
Ethics Approval
Ethics Committee of Guangdong Provincial Hospital of Chinese Medicine, No. B2016-137-01.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by TCM Research Project of Guangdong Provincial Hospital of Chinese Medicine (grant no.: YN2015MS25), and Academic Studio of Zhang Qi's Clinical Experience (grant no.: E43712). The sponsors did not have a role in the design, conduct, or interpretation of the study, or in any decision to submit the article for publication.
Supplementary Material
Supplementary Material
CONSORT 2010 Checklist
STRICTA-2010-Checklist