
Abstract
Objectives:
Mindfulness-based stress reduction (MBSR) has been found effective for improving chronic low-back pain (cLBP). However, little data exist regarding how attractive this technique is to Americans as a therapy for cLBP.
Design:
Survey of randomly selected persons with cLBP.
Settings/Location:
Respondents were recruited from Kaiser Permanente Washington and one-time surveys were completed online.
Patients:
Adults 18–80 years of age with cLBP.
Surveys:
The study was conducted between December 2019 and August 2020.
Outcome measures:
The survey described an evidence-based classic MBSR course and then asked respondents about their sociodemographic characteristics, their current back pain, previous back pain treatments, behavioral risk factors for back pain, and four outcomes indicative of intention to engage in MBSR.
Results:
Four-hundred fifty-seven respondents completed the survey. Respondents were primarily women, white, educated, and with back pain for more than 5 years. About half had previously used a mind-body therapy for their pain. Overall, they reported moderate to high intention to try mindfulness classes and practice at home (median of 5 with 50% of the observations between 4 and 6, and 5.7, 50% of the observations between 4.3 and 6.3, respectively, on a 7-point scale). They reported a willingness to spend a median of 3 h/week learning mindfulness and 3.5 h/week practicing mindfulness techniques (for both outcomes, 50% of the respondents reported between 2 and 5 h). Few patient characteristics predicted intention to engage in MBSR, with no variable predicting all outcomes. The magnitude of the effect associated with significant predictors was small.
Conclusion:
Classic MBSR appealed to many survey respondents, in that they reported high interest in learning MBSR and intention to practice at home. The amount of time they reported being willing to spend learning MBSR and practicing at home is consistent with the time commitment in the original course.
Introduction
Globally, low-back pain is a leading cause of disability 1 and is common, 2 costly, 3 and often persistent. 4,5 Frequently, the cause of the pain is unknown 6 and biomedical treatments may not be effective, 7 complicating its management. In response to the burgeoning opioid epidemic, recent guidelines issued by the Centers for Disease Control and Prevention (CDC) 8 note that nonpharmacological therapies are the preferred treatment for patients with chronic noncancer pain. The American College of Physicians' recent evidence-based 9 clinical practice guideline 10 for low-back pain recommended various nonpharmacologic treatments, including mindfulness-based stress reduction (MBSR), as the first line of therapy for chronic low-back pain (cLBP), given “moderate quality evidence” from a recent systematic review that included several large trials. 9 Despite the clear benefits of MBSR efficacy studies, patients in most need may struggle to fully participate, given the intensive time commitment (e.g., 28 h of class 11 ).
As part of a program of research on mindfulness, we set out to explore for which cLBP patients MBSR would be most attractive, and factors that may be targeted to increase willingness to participate in MBSR. To this end, we conducted a survey that captured data on respondents' demographics, cLBP, and beliefs about MBSR, as well as intentions to engage in MBSR training. The Theory of Planned Behavior guided our study, given robust evidence that intentions are one of the strongest predictors of actual behavior. 12 The Theory of Planned Behavior hypothesizes that people's attitudes and self-efficacy for engaging in a behavior influence their intentions and intentions to engage in a behavior, such as MBSR training. Because demographic, disease, and behavioral characteristics, as well as prior treatments, can also affect intentions, identifying these potential factors could inform strategies to improve attitudes, perceived norms, and self-efficacy, as well as intentions for MBSR.
Previous characteristics of U.S. meditation practitioners, 13 –15 including those with cLBP, 16 focused a set of possible predictors included in our models (i.e., age, 17,18 sex, 17,18 race, 17,18 body mass index (BMI), 18 pain interference, and physical function 16 ), whereas others were included for exploratory purposes, given the relatively nascent state of the science. In this article, we first characterize the degree to which patients with cLBP would be willing to engage in MBSR and next identify those characteristics of patients predicting greater likelihood of engaging in the evidence-based version of MBSR as tested in efficacy trials. Such information could help identify potential barriers to MBSR that coupled with an understanding of any inequity in access is essential for understanding the reach of classic MBSR.
Materials and Methods
Study design and respondents
We conducted an online survey designed to ascertain intentions of respondents to try classic mindfulness training for their cLBP. Survey respondents received a description of classic mindfulness classes as typically delivered in MBSR, which includes 2 h of weekly in-person classes for 8 weeks and 20 min of guided home practice on nonclass days, along with an introduction describing the scientific evidence supporting mindfulness for cLBP.
This survey was conducted at Kaiser Permanente Washington (KPWA), an integrated health care system with roughly 660,000 members in Washington State. The institutional review board approved the study. Consent was obtained online before the survey started. The survey was programmed in DatStat Illume.
Potential respondents were adults between 18 and 80 years of age, who met the NIH Task Force definition for cLBP (i.e., back pain persisting at least 3 months with pain on at least half the days in the past 6 months). 19 All received primary care from a KPWA provider and had a diagnosis consistent with uncomplicated LBP in the last year. In addition, respondents reported at least moderate pain-related activity limitation (≥3 on a 0–10 scale). We excluded individuals who had complicated back pain (i.e., cancer, infectious or inflammatory causes, sciatica, vertebral fractures, or due to pregnancy), or were seeking compensation for their back pain.
We mailed a study letter to potential respondents who appeared to meet eligibility criteria from their electronic health record. We described the study as designed to “assess interest in different mind-body treatment programs for cLBP.” It encouraged all letter recipients to complete the survey regardless of their interest in trying this type of program. It included a web address for an online web survey. Recipients answered additional six questions to confirm their eligibility (age, 3 months or more of cLBP, frequency/interference from cLBP, litigation, or pregnancy), read a consent form, and indicated approval by checking a box. The survey was then accessible and asked them to answer the questions, while imagining that the program described was available as part of their health plan, even though it was not.
Classic MBSR description
Before beginning the survey, respondents read a 730-word description of mindfulness training. The description was drafted using knowledge of the course and the scientific literature and then refined during focus groups and cognitive interviews with representative cLBP patients. It defined mindfulness, discussed the scientific evidence for mindfulness training, outlined key class features (including the component techniques and the steps to learning them), noted that mindfulness is a complex skill requiring practice at home, and ended with a one-sentence summary (see Appendix File A1 for a copy of the description).
Measures
Our survey included questions recommended by the NIH Task Force on Research Standards for Chronic Low-Back Pain 19 as well as questions designed to assess constructs from the Theory of Planned Behavior. 20
We used the NIH Task Force 19 -recommended questions to describe our participants' sociodemographic characteristics (age, gender, race, ethnicity, and employment), current back pain (duration of cLBP, weekly frequency of pain, pain interference, physical function, and sleep disturbance), previous use of selected back pain treatments (including opioids, injections, exercise therapy, and psychological counseling), and behavioral risk factors for cLBP (including BMI, smoking, excessive use of drugs or alcohol, symptoms of depression, and avoidance of exercise due to fear and catastrophizing beliefs about their back pain).
The NIH Task Force recommended the use of 4-item PROMIS scales to measure pain interference, physical function, sleep disturbance, and depression. We used these scales for three domains, but chose to substitute the patient Health Questionnaire 2 (PHQ-2) 21 as a measure of depressive symptoms as the PHQ-2 has a validated cutoff point for a positive depression screen. We also added questions about previous use of mindfulness, yoga, and other mind-body therapies.
To measure intentions to engage in MBSR, we followed established guidelines. 20 Three focus groups were conducted with people experiencing cLBP to outline the concept of intentions for MBSR for back pain in participants' own words. Feedback was reviewed by the study team who then drafted questions assessing intentions. Five people with back pain then participated in cognitive interviews, confirming that they understood the questions as intended. This resulted in four outcome variables: (1) intention to try mindfulness training (classes); (2) intention to try mindfulness home practice; (3) hours willing to spend on mindfulness training per week; and (4) hours willing to spend on mindfulness home practice per week. Because another study aim was to test different descriptions of mindfulness, we reduced participant burden by asking only 25% of the sample to complete the home practice questions.
Sample size
Our aim was to enroll 400 survey respondents, which would provide 80% power to detect a realistic effect through linear regression for an individual predictor of a change in R 2 = 0.019 or 1.9% of the variability in intentions to take MBSR. 22
Statistical analysis plan
We included all survey respondents in the analyses. We summarized respondents' sociodemographic and cLBP characteristics, use of prior treatments for cLBP, behavioral risk factors for cLBP, and intentions to engage in MBSR as frequencies and percentages for categorical variables and means and standard deviations for continuous variables. Spearman and Pearson correlations between all four MBSR intention variables were calculated. To explore the relationship between each measured patient-level variable and each of the MBSR intention outcomes, we fit unadjusted, bivariate linear regressions to each outcome and patient characteristic pairing.
To relax homoscedasticity and normality of error assumptions, generalized estimating equations (GEE) with an independent working correlation structure were used to estimate regression parameters, robust standard errors, 95% confidence intervals, and p-values. To allow for flexibility in bivariate relationships between continuous respondent characteristics (e.g., age and BMI) and MBSR intention outcomes, two regressions were fit for each covariate, one with the variable as a linear predictor and one with the variable as an ordinal categorical predictor.
As per a priori hypotheses, age, 17,18 sex, 17,18 race, 17,18 BMI, pain interference, and physical function 16 formed the basis of four separate multivariable linear models, one for each MBSR intention outcome. Additional measured predictor variables were added to each multivariable model if the two-sided p-value for that predictor in a bivariate regression was 0.10 or less. Multivariable model estimates were computed using GEE with an independent working correlation structure and robust standard errors.
Respondent age and BMI were included in all models as ordinal categorical variables to facilitate interpretation of associations across clinically relevant categories. For categorical variables like race and employment status, some categories were aggregated to avoid small cell sizes and conserve model degrees of freedom. To assess the presence of impactful multicollinearity, the variance inflation factor was calculated and assessed for each variable in each multivariable regression model. All tests were two sided with p < 0.05 indicating statistical significance in these models.
Results
Recruitment
We sent 10,450 invitation letters in 15 batches to potentially eligible members of KPWA between December 9, 2019, and June 17, 2020. The batch size varied between 249 and 4499 letters. Between December 11, 2019, and August 4, 2020, 733 potential survey respondents accessed the website (7%). All, but 23 completed enough screening questions so their eligibility could be determined. Of those, 247 were ineligible, 6 refused, and 23 started, but failed to complete the survey, while 457 respondents completed the survey (4.4%).
Characteristics of the sample population
Sociodemographic variables
Respondents ranged in age from 18 to 80 years with a mean of 53.3 years (Table 1). Most respondents were women, non-Hispanic white, college educated, and either working (51%) or retired (30%).
Baseline Characteristics of Study Sample
PROMIS scales have a mean of 50 and an SD of 10, which represent U.S. population norms.
BMI, body mass index; cLBP, chronic low-back pain; NA, not applicable; SD, standard deviation.
Current cLBP
Slightly more than half of respondents reported their back pain lasted for over 5 years and a slightly smaller fraction reported pain almost daily in the preceding 6 months (Table 1). PROMIS measures indicated that pain interference was higher than the national norm, sleep disturbance resembled the norm, and physical function was substantially worse.
Previous back pain treatments
Study respondents reported use of a variety of previous treatments. Exercise therapy was most common (88%), followed by any mind-body therapy (54%), opioid prescriptions (45%), and yoga (44%). Previous mindfulness experience was infrequent (12%).
Behavioral risk factors for cLBP
The average BMI was 29.5, with 41% of respondents being obese (21%) or morbidly obese (20%). Only 5% were current smokers. In the past year, most participants reported they never drank/used drugs more than they meant to (69%) and never felt the need to cut back on drinking/drug use (73%). About 18% reported depressive symptoms. While only 15% indicated fear avoidance for physical activity, about twice as many reported catastrophic thinking about their cLBP.
Outcome measures
On the 7-point scale of intention to try mindfulness training or practice at home (where 7 is most likely to try it), respondents reported a median of 5 (with 50% between 4 and 6) and 5.7 (with 50% between 4.3 and 6.3), respectively. They reported a willingness to spend a median of 3 h/week learning mindfulness and 3.5 h/week practicing mindfulness techniques (for both outcomes, 50% of respondents between 2 and 5 h).
Correlations were high between intention to try mindfulness training and to practice at home (r = 0.82; Appendix Table AT1) and between hours willing to spend learning mindfulness and hours willing to spend practicing it (r = 0.87; Appendix Table AT1) with more modest correlations among other outcomes (range of 0.35 to 0.46; Appendix Table AT1).
Bivariate models
Six variables were associated with greater intention to try mindfulness classes in bivariate models at the level of p ≤ 0.1; these were being female, no prior injections, prior use of other mind-body therapies for back pain, ever drinking more than desired, ever feeling the need to cut down on drinking, and endorsing depressive symptoms (Table 2).
Bivariate Models with a Single Predictor and each of Four Outcome Variables

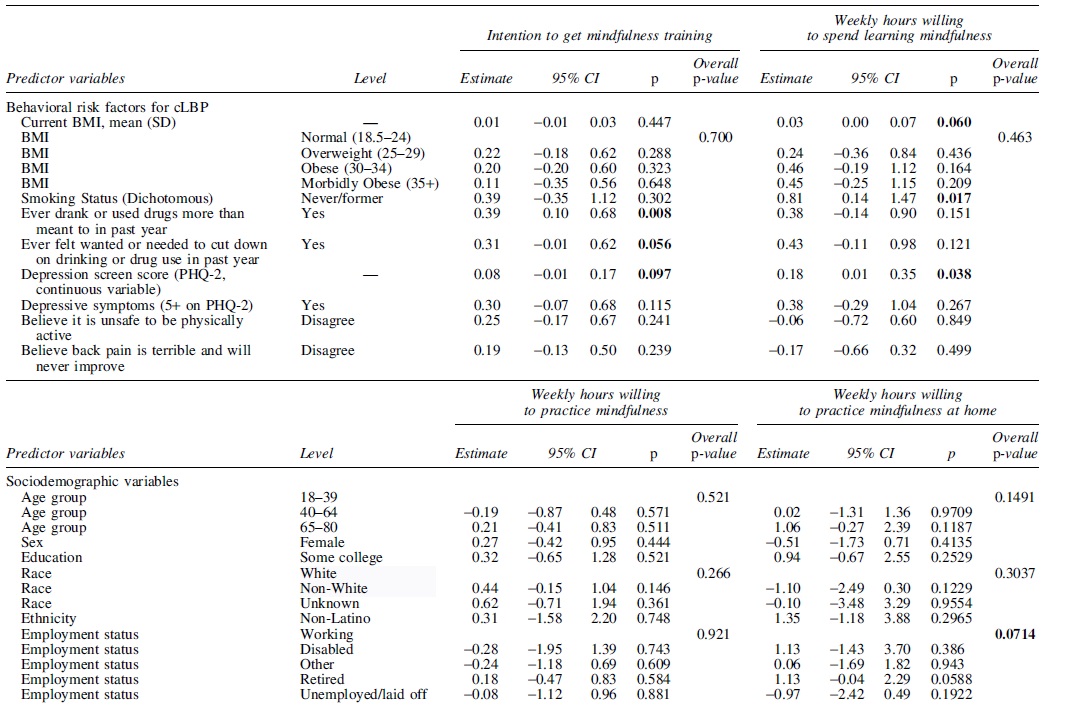
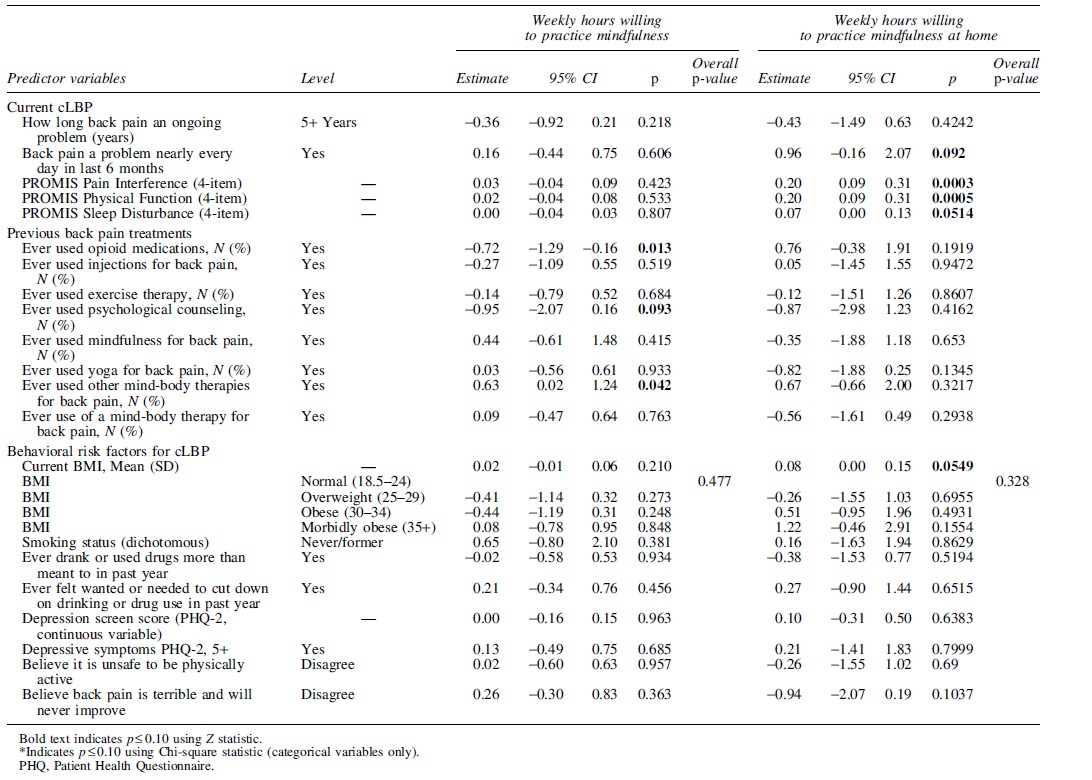
Ten variables were associated with a willingness to participate in a greater number of hours learning mindfulness at the level of p ≤ 0.1. These were older age, having had back pain for at least 5 years, reporting back pain nearly daily or daily in the last 6 months, higher levels of back pain interference with life, higher levels of physical function, prior use of opioids or of other mind-body therapies for low-back pain, higher BMI (continuous measure), not current smoker, and endorsing a greater number of depressive symptoms.
Three variables were associated with greater intention to practice mindfulness at home in bivariate models at the level of p ≤ 0.1; these were never user of opioids for back pain or of cognitive behavioral therapy and prior users of other mind-body therapies for low-back pain.
Six variables were associated with greater number of hours per week willing to practice mindfulness (p ≤ 0.1). These predictor variables were being retired, back pain nearly all or all days in the last 6 months, higher levels of back pain interference with life, higher levels of physical function, higher levels of sleep disturbance, and higher BMI (continuous measure).
Multivariate models
We had a priori hypothesized that women, older patients, patients who were white, those reporting worse pain interference, and worse physical function would endorse greater intention to learn MBSR and to spend more time learning MBSR, to practice MBSR at home, and to spend more time practicing (Table 3). We also hypothesized that respondents with higher BMI would be less likely to learn MBSR, would practice at home, and would endorse willingness to spend less time learning and practicing at home. These six variables were therefore included in all four final multivariate models. In addition, for each outcome, we included those additional predictor variables that were significant at the 0.1 level in the relevant bivariate model.
Final Multivariate Models with Each of the Four Outcome Variables


Three of 11 potential predictors remained statistically significant (p < 0.05) in the model with intention to learn MBSR as the outcome variable. Age 65–80 years old, being female, and drinking or using drugs more than desired were associated with greater intentions to try MBSR.
One of 12 potential predictors remained significant in the model with the dependent variable of hours willing to learn MBSR. Being a never or former smoker was associated with willingness to spend more hours learning MBSR compared to current smokers.
Three of nine potential predictors remained significant when the outcome was intention to practice MBSR at home. These were prior use of injections, associated with higher intentions, and prior use of opioids or counseling, both associated with lower intentions.
Only one of nine potential predictors remained significant, older age, with the dependent variable of weekly hours willing to practice MBSR at home.
Overall, few variables were statistically associated with one of the four outcomes. Among the six a priori hypothesized predictor variables, four were never significant in any of the final models. Among the two other variables, gender only predicted outcomes in the intention to try MBSR model and age only predicted two of four outcomes. Among the other five bivariate predictors, they only predicted one outcome. The effect sizes of significant predictors were very small. For example, for the intention to get mindfulness training outcome, age, sex, and having drank more than you wanted to in the past 12 months were statistically significant in the multivariable model. The largest of those associations is with age where, holding other variables constant, the average intention for 65–80-year olds is 0.53 points higher than those 18–39 (7-point scale) years of age.
Discussion
There was surprisingly no demographic factor that consistently distinguished among cLBP patients' willingness to try MBSR. Neither our a priori hypothesized characteristics nor other patient characteristics were consistently associated with greater intention to engage with mindfulness training and home practice (and hours intending to spend on these). Moreover, effective sizes of significant predictor variables were small. These findings are quite positive when coupled with the surprisingly high levels of willingness to engage in mindfulness training and home practice. Prior surveys of the U.S. population have found that women are more likely to report the practice of meditation, 18 the practice of mindfulness, 17 and if they also have back or neck pain of mind-body therapies. 16
Among adult Americans, age is inconsistently related to prior practice of meditation (higher in younger adults), mindfulness (age slightly higher in mindfulness practitioners), or mind-body therapies (no relationship between age and practice among those with back or neck pain). However, we are unaware of other surveys that report interest in learning mindfulness.
Our relatively high levels of willingness to engage in mindfulness training and home practice could explain the lack of statistically significant predictors. Although this could reflect an inflated intention, we are confident in our measurement of the theory of planned behavior constructs, 23 and the robust literature that specific intentions are strong predictors of actual behaviors. The way that mindfulness training was described in this study may have led to these high levels of intention, given that the language was informed by focus groups with target patients and was intended to be quite accessible. This possibility is supported by the dissemination literature, which emphasizes the importance of packaging evidence-based interventions to promote adoption decisions. 24
Our survey instructions asked respondents to assume that MBSR was offered by their health system and covered by insurance. That could have removed the major barriers to engaging with MBSR (i.e., more secular and cost is covered). If so, this suggests that the major barriers to practice are structural rather than attitudinal. In addition, mindfulness has become quite common in popular culture, 16 so conceivably many of the attitudinal barriers are greatly diminished, leaving logistics as the major barrier to engagement. Many of our respondents had moderate to severe cLBP and had pain for over 5 years, which may suggest they would be motivated to try anything and this could override the influence of other patient characteristics.
Our study benefitted from a large sample size with a robust age range of respondents, many men as well as women respondents, and a robust assessment of demographic, back pain, and behavioral characteristics, as well as prior treatments for back pain. A major limitation is our inability to accurately compute a survey response rate for patients with chronic back pain, who met our study inclusion criteria. By selecting patients with electronic health record information for a condition in which a minority of those patients would meet our inclusion criteria, we are unable to completely assess the representativeness of our survey sample.
However, our data on prior treatments and age distribution suggest that this population had more long-standing back pain and was at least moderately impaired, and that a substantial fraction had behavioral risk factors for worse prognosis. 25,26 Reflecting the population of KPWA, most respondents were non-Hispanic whites and college educated. While some prior surveys find that Hispanic and black adults are less like to report a meditation or mindfulness practice, Koch and Cramer 16 found that race and ethnicity were not associated with the practice of mind-body therapies in adults with back or neck pain. The survey time frame largely overlapped with the beginnings of the COVID-19 pandemic; the impact of this on our findings is unknown.
Our findings suggest future work is warranted to better understand how factors beyond those encapsulated in the Theory of Planned Behavior might predispose patients to learn and practice mindfulness, ideally revealing malleable targets that could inform customizing treatment to individual patients.
Conclusion
Classic MBSR appealed to many survey respondents in that they reported high interest in learning MBSR and intending to practice at home. The amount of time they reported being willing to spend learning MBSR and practicing at home is consistent with the time commitment in the original course, and no patient characteristic differentiated willingness to engage in MBSR in this population of patients that included more impairing back pain.
Footnotes
Authors' Contributions
K.J.S., S.M.W.J., and C.C.L. contributed to the conception and design of the study and the creation of the questionnaires. K.J.S. was involved in the creation of the stimulus and recruitment materials. R.D.W. performed the statistical analyses, and all authors were involved in the interpretation of the data. K.J.S. drafted most of the article with important additions from all authors. All authors have read and approved the final version of the article and agree with the order of presentation of the authors.
Acknowledgments
We thank the Survey Research Program at KPWA for building and testing the survey and for sending recruitment letters to members of various Kaiser Permanente Washington health plans. We thank Julia Anderson for programming the survey, Kristin Delaney for creating the data sets, and Zoe Bermet for project management support.
Disclaimer
The contents are the sole responsibility of the authors and do not necessarily reflect the official view of NCCIH.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project was supported by grant R21 AT010170 from the National Center for Complementary and Integrative Health.