
Abstract
Objective:
To examine the reasons why office-based physicians do or do not recommend four selected complementary health approaches to their patients in the context of the Andersen Behavioral Model.
Design:
Descriptive estimates of physician-level data from the 2012 National Ambulatory Medical Care Survey (NAMCS) Physician Induction Interview, a nationally representative survey of office-based physicians (N = 5622, weighted response rate = 59.7%).
Setting/Location:
The United States.
Outcome measures:
Reasons for the recommendation or lack thereof to patients for: herbs and other non-vitamin supplements, chiropractic/osteopathic manipulation, acupuncture, and mind–body therapies (including meditation, guided imagery, and progressive relaxation). Differences by physician sex and medical specialty were described.
Results:
For each of the four complementary health approaches, more than half of the physicians who made recommendations indicated that they were influenced by scientific evidence in peer-reviewed journals (ranging from 52.0% for chiropractic/osteopathic manipulation [95% confidence interval, CI = 47.6–56.3] to 71.3% for herbs and other non-vitamin supplements [95% CI = 66.9–75.4]). More than 60% of all physicians recommended each of the four complementary health approaches because of patient requests. A higher percentage of female physicians reported evidence in peer-reviewed journals as a rationale for recommending herbs and non-vitamin supplements or chiropractic/osteopathic manipulation when compared with male physicians (herbs and non-vitamin supplements: 78.8% [95% CI = 72.4–84.3] vs. 66.6% [95% CI = 60.8–72.2]; chiropractic/osteopathic manipulation: 62.3% [95% CI = 54.7–69.4] vs. 47.5% [95% CI = 42.3–52.7]). For each of the four complementary health approaches, a lack of perceived benefit was the most frequently reported reason by both sexes for not recommending. Lack of information sources was reported more often by female versus male physicians as a reason to not recommend herbs and non-vitamin supplements (31.4% [95% CI = 26.8–36.3] vs. 23.4% [95% CI = 21.0–25.9]).
Conclusions:
There are limited nationally representative data on the reasons as to why office-based physicians decide to recommend complementary health approaches to patients. Developing a more nuanced understanding of influencing factors in physicians' decision making regarding complementary health approaches may better inform researchers and educators, and aid physicians in making evidence-based recommendations for patients.
Introduction
Complementary health approaches include a diverse group of nondrug and noninvasive health practices encompassing nutritional, psychological, and physical approaches that may have originated outside of conventional medicine, many of which are being integrated into mainstream health care. These include natural products such as dietary supplements as well as mind and body approaches, such as yoga, meditation, spinal/joint manipulation, and acupuncture. 1 Out-of-pocket expenditure of these approaches was ∼$30.2 billion in 20122, and the use of complementary health approaches among U.S. persons has been well studied. 3 –8
The Andersen Behavioral Model of Health Services Utilization purports to discover the factors that facilitate or impede the utilization of health services by incorporating predisposing characteristics, enabling resources, and need for care, 9 and it has been used to inform the use of complementary health approaches. 10 –13 In the current study, we sought to investigate physicians' recommendations for complementary health approaches within the Andersen Behavioral Model.
The use of this model as a framework underpins the concept of complementary health use as a health behavior occurring within the context of the U.S. health care system. As such, items were categorized with: need-based reasons (physical symptoms, emotional symptoms, general health and well-being, and patient request); predisposing characteristics (personal experience); and enabling factors (patient reports; colleague recommendation and evidence in peer-reviewed literature).
Previous population-based research has shown that nearly 4 out of 10 U.S. adults use complementary health approaches. Although exceptions exist, 14 –18 the prevalence of use has been driven primarily by predisposing factors such as sex, age, and region 6 –8 as well as by enabling factors such as income, education, and health insurance. 19 –21 In addition, the need for care factors such as the number and types of painful health conditions has been found to be associated with increased use of and expenditure on complementary health approaches. 3,22 –27
Less studied is how the application of the Andersen Behavioral Model might apply to physician recommendations of complementary health approaches, interactions between patients and office-based physicians related to these approaches during office visits 28 –30 ; and reasons why office-based physicians may or may not recommend these to patients. Stussman et al. was the first study using a national probability sample of U.S. physicians, as well as descriptive estimates and multivariable regression to examine factors such as age and sex, predisposing a physician to recommend complementary health approaches to patients in an office-based setting. 31 It found that 53.1% of office-based physicians recommended at least one approach to their patients during the previous 12 months.
Female physicians recommended all individual approaches at a higher rate than their male counterparts, with the exception of chiropractic/osteopathic manipulation. General/family practitioners and internists recommended these approaches at higher rates than pediatricians. Stussman et al. also found that physician age had no effect on the recommendation of herbs and other non-vitamin supplements, chiropractic/osteopathic manipulation, acupuncture, and mind–body therapies.
Berman et al. 32 surveyed a random sample of rheumatologists to examine recommendations for complementary health approaches and found that a higher percentage of physicians felt that they had sufficient knowledge of acupuncture (vs. other complementary health approaches) to discuss with their patients. In addition, that study found that 46.9% of physicians did not make recommendations for complementary health approaches in the previous 12 months. Casbarro et al. 33 surveyed pediatric clinicians on knowledge, beliefs, and practices about complementary health approaches and found that results from randomized controlled clinical trials had greater influence on whether a physician made recommendations relative to personal experience, recommendations from colleagues, and clinical experience with patients.
Finally, a recent qualitative study probed academic physicians on the lack of routine recommendations to patients for Tai Chi despite a plethora of high-quality randomized controlled trials demonstrating its health benefits. 34 Physicians in that study mentioned lack of patient access and lack of physician and/or patient awareness about the approach.
Evidence-based guidelines for pain management have increasingly recommended the use of some complementary health approaches 35 –37 ; however, their implementation with standard medical practice remains unclear. Impediments may include a lack of patient access and health insurance coverage. 38,39 Other impediments may reside with both provider (e.g., lack of knowledge or personal experiences) and patient (e.g., lack of interest) levels. Despite these impediments, there is scarce literature that examines the reasons that physicians do or do not recommend these approaches.
To address this gap in the scientific literature, the current study examines, within the context of the Andersen Behavioral Model, the reasons that U.S. physicians do or do not recommend four common complementary health approaches: herbs and other non-vitamin supplements, mind–body therapies, chiropractic/osteopathic manipulation, and acupuncture. We also describe differences in these recommendations by physicians' sex and medical specialty.
Materials and Methods
Data
The 2012 National Ambulatory Medical Care Survey (NAMCS) Physician Induction Interview was approved by the National Center for Health Statistics (NCHS) Ethics Review Board (Protocol No. 2010-02). The NAMCS is conducted annually and is representative of nonfederal, office-based U.S. physicians. This interview consists of questions that screen for survey eligibility and collect data on physician and practice characteristics. The 2012 NAMCS Physician Induction Interview data are available from the NCHS Research Data Center. 40 Verbal consent was received from all physician participants.
The sampling frame for the 2012 NAMCS was composed of all physicians listed in the master files maintained by the American Medical Association and the American Osteopathic Association ∼6 months before the start of the survey year and who met the following criteria: (1) office-based; (2) principally engaged in patient care; (3) non-federally employed; (4) not in specialties of anesthesiology, pathology, and radiology; and (5) <85 years of age at the time of the survey. The core sample included 15,740 physicians: 14,931 Medical Doctors and 809 Doctors of Osteopathy. A total of 6166 physicians did not meet all of the eligibility criteria and were ineligible for the survey.
Of the 9574 eligible physicians, 5622 participated in the Physician Induction Interview, resulting in a weighted response rate of 59.7%. 41,42 Missing data were excluded from individual variables and comprised <5% of the 68 variables used in the current study. The number of participants with missing data for each variable are shown in Supplementary Table S5. We used the STrengthening the Reporting of OBservational studies in Epidemiology cross-sectional reporting guidelines shown in Supplementary Table S6. 43 The 2012 NAMCS Physician Induction Interview was the only year for which supplemental survey questions on physician recommendations of complementary health approaches were included.
Physician characteristic measures
Based on findings from previous relevant literature, 30,31 we stratified data by physician sex (male/female) and medical specialty (general/family practice, internal medicine, psychiatry, obstetrics/gynecology, pediatrics). For Table 1, which details the study population, a category for “all other specialties” is included. To avoid small cell sizes and unreliable estimates, we collapsed 12 physician specialties (general surgery, orthopedic surgery, cardiovascular diseases, dermatology, urology, neurology, ophthalmology, otolaryngology, oncology, allergy, pulmonology, and other specialties) into this “other specialty” category.
Characteristics of Nonfederal, Office-Based Physicians, by Sex: The United States, 2012
The number of physicians responding to this item was 5403 (4106 male; 1297 female). Not all physicians provided a response. Other race includes Black/African American, Native Hawaiian/Other Pacific Islander, American Indian/Alaska Native, multiple races, and unknown race.
Other specialties include general surgery, orthopedic surgery, cardiovascular diseases, dermatology, urology, neurology, ophthalmology, otolaryngology, oncology, allergy, pulmonology, and other specialties.
CI, confidence interval; DO, doctor of osteopathic medicine; KG, Korn-Graubard; MD, doctor of medicine; MSA, metropolitan statistical area; n, unweighted sample size; NA, not applicable; OB/GYN, obstetrics and gynecology.
Data source: National Ambulatory Medical Care Survey Physician Induction Interview, 2012.
The remaining analyses were limited to the five individual specialties for ease of interpretation/space constraints. To avoid small cell sizes and unreliable estimates, we collapsed the physician's age into four categories (<45, 45–54, 55–64, and ≥65 years) and race into three categories (white, Asian, and other). Ethnicity was not included, as there were not enough Hispanic respondents to produce reliable statistics.
Measures on recommendation of complementary health approaches
The NAMCS questionnaire fielded in this study underwent extensive cognitive testing with physicians from a variety of specialties. These in-depth, semi-structured interviews determined the survey items deemed most important to physicians when making decisions about the recommendation of complementary health approaches. 44
Three survey items were analyzed. The first two were asked of physicians who stated that they recommended specific complementary health approaches in the previous 12 months: (1) Did you recommend [approach] to patients for any of the following reasons? (reasons included: physical symptoms such as pain; for emotional symptoms such as stress or anxiety; for general health maintenance and well-being; because the patient asked for it); and (2) Which of the following factors influenced your decision to recommend [approach] to patients? (factors included: personal experience; patient reports to physicians about the complementary health approach [i.e., patients telling physicians about their use of complementary health approaches]; colleague recommendation; evidence in peer-reviewed literature).
Denominators for proportions representing these survey items include physicians who recommended the specific complementary health approach. The third survey item analyzed was answered by physicians who did not recommend a specific approach in the previous 12 months: Which of the following factors prevented you from recommending [approach] to patients? (factors included: limited health insurance coverage; lack of affordability for the patient; lack of information sources; lack of places/providers to refer patients; patient's lack of interest or openness to [approach]; lack of perceived benefit).
We present these variables within the framework of the Andersen Behavioral Model: predisposing characteristics (personal experience), enabling factors (patient reports; colleague recommendation; and evidence in peer-reviewed literature), and need factors (physical symptoms, emotional symptoms, general health and well-being, and patient asked for it).
Denominators for proportions representing this survey item include physicians who did not recommend the specific approach. Four approaches included in the assessment were: herbs and other non-vitamin supplements, chiropractic/osteopathic manipulation, acupuncture, and mind–body therapies (i.e., guided imagery, meditation, and progressive muscle relaxation, not including prayer). These four approaches are among the most highly used complementary approaches in the United States 7 and represent three primary therapeutic inputs: nutritional, psychological, and physical. 45
Statistical analysis
Bivariate analyses examined the relationships between selected physician characteristics and reasons for physicians recommending and not recommending these approaches. Analyses were conducted by using SUDAAN 11.0, 46 weighted to be representative of U.S. office-based physicians, and used survey design variables and proper subsetting to account for covariances resulting from NAMCS survey design. Percentages are accompanied by Korn-Graubard 95% confidence intervals (CIs) for complex surveys; these CIs are used to determine whether percentages meet NCHS presentation standards for reliability. 47 In addition, Wald Chi Squares were used to determine p-values for comparisons in the Results section.
Results
Physician characteristics
Among nonfederal, office-based U.S. physicians, 72.3% were male and 27.7% were female (Table 1). Approximately 60% of physicians fell into the two middle age groups. Male physicians tended to be older than female physicians. The majority of physicians were white (78.6%) followed by Asian (15.5%) and all other race groups, including unknown (5.9%); these patterns were generally consistent by sex. Additional physician characteristics can be found in Table 1.
Need-based reasons for recommending complementary health approaches
For the 53.1% of physicians who made recommendations, physical symptoms were the most frequently observed reason given for the recommendation of chiropractic/osteopathic manipulation or acupuncture (92.4%, 95% CI = 89.8–94.5 for chiropractic/osteopathic manipulation; 94.4%, 95% CI = 92.2–96.1 for acupuncture) (Table 2). The most frequently observed reason given for the recommendation of mind–body therapies was for emotional symptoms (89.0%, CI = 84.9–92.3). For each of the four approaches, >60% of physicians who recommended an approach did so because the patient asked for it, ranging from 63.6% for mind–body therapies (95% CI = 58.3–68.8) to 79.2% for chiropractic/osteopathic manipulation (95% CI = 75.5–82.6).
Need-Based Reasons, Predisposing and Enabling Factors for Recommending Complementary Health Approaches to Patients by U.S. Physicians Who Recommended the Approach in the Previous 12 Months
Overall, 53.1% of physicians made recommendations in the previous 12 months. Physicians were only asked about the reasons for recommendation or the factors that influenced recommendation for a specific complementary health approach if they recommended that specific complementary health approach in the previous 12 months. Physicians could answer yes or no to each reason and influential factor.
CI, confidence interval; KG, Korn-Graubard; n, unweighted sample size.
Data source: National Ambulatory Medical Care Survey Physician Induction Interview, 2012.
There were several significant differences in recommendations among female and male physicians (Fig. 1). A higher percentage of female physicians recommended herbs and other non-vitamin supplements or acupuncture for emotional symptoms compared with male physicians (53.6% [95% CI = 46.3–60.9] vs. 43.8% [95% CI = 38.2–49.5], Wald Chi-square p = 0.0315 for herbs and other non-vitamin supplements; and 46.7% [95% CI = 38.3–55.3] vs. 33.5% [95% CI = 27.7–39.7], Wald Chi-square p = 0.0112 for acupuncture).
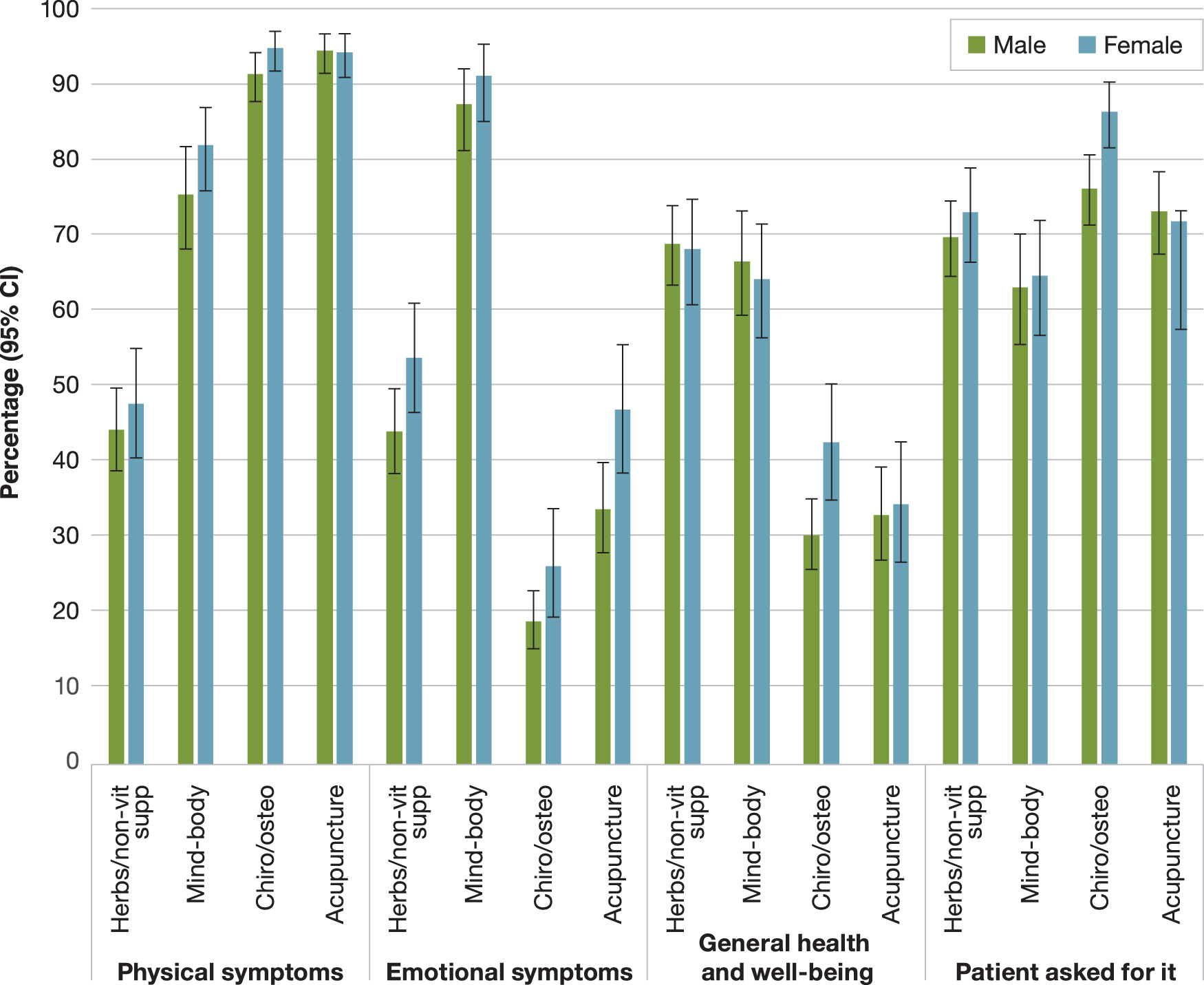
Need-based reasons for recommending complementary health approaches to patients by U.S. physicians who recommended the approach in the previous 12 months, by physician sex. Error bars represent 95% Korn-Graubard confidence intervals. Denominators for each individual complementary health approach includes only physicians who recommended the specific approach. Chiro/osteo, chiropractic/osteopathic manipulation; Herbs/non-vit supp, herbs and other non-vitamin supplements; Mind–body, mind–body therapies; OB/GYN, obstetrics and gynecology. Data source: National Ambulatory Medical Care Survey Physician Induction Interview, 2012.
In addition, compared with male physicians, a higher percentage of female physicians recommended chiropractic or osteopathic manipulation for the patient's general health and well-being (42.3% [95% CI = 34.7–50.1] vs 30.0% [95% CI = 25.5–34.8], Wald Chi-square p = 0.0068), and because the patient asked for it (86.3% [95% CI = 81.5–90.2] vs. 76.1% [95% CI = 71.2–80.5], Wald Chi-square p = 0.0018). No other significant differences were found in reasons for recommendations by sex.
Health reasons and influencing factors stratified by physician specialty are shown in Tables 3 and 4. Due to space constraints, we are unable to provide a full write-up of differences in recommending by physician specialties, but selected results are highlighted next. Among physicians who recommended mind–body therapies in the previous 12 months, the percentage of physicians who recommended them for emotional reasons ranged from 80.9% (95% CI = 61.2–93.3) of obstetricians/gynecologists to 99.2% (95% CI = 96.39–99.94) of psychiatrists.
Need-Based Reasons for Recommending Complementary Health Approaches to Patients by U.S. Physicians Who Recommended the Approach in the Previous 12 Months, by Approach and Specialty
Physicians were only asked about the reasons for not recommending a specific complementary health approach if they reported not recommending that specific complementary health approach in the previous 12 months.
CI, confidence interval; KG, Korn-Graubard; n, unweighted sample size; OB/GYN, obstetrics and gynecology.
Data source: National Ambulatory Medical Care Survey Physician Induction Interview, 2012.
Predisposing and Enabling Factors for Recommending Complementary Health Approaches to Patients by U.S. Physicians Who Recommended the Approach in the Previous 12 Months, by Approach and Specialty
Physicians were only asked about the reasons for not recommending a specific complementary health approach if they reported not recommending that specific complementary health approach in the previous 12 months.
CI, confidence interval; KG, Korn-Graubard; n, unweighted sample size; OB/GYN, obstetrics and gynecology.
Data source: National Ambulatory Medical Care Survey Physician Induction Interview, 2012.
Physicians across all five specialties who recommended herbs and other non-vitamin supplements frequently did so because the patient asked for it (77.2% [95% CI = 69.8–83.6] for general/family practitioners; 79.0% [95% CI = 67.16–88.1] for internists, 54.1% [95% CI = 39.6–68.1] for pediatricians; 84.6% [95% CI = 72.0–93.1] for obstetricians/gynecologists, and 60.6% [95% CI = 45.0–74.7] for psychiatrists).
Predisposing and enabling factors influencing physicians' decisions to recommend
Of the physicians who recommended a complementary health approach, >50% cited evidence in peer-reviewed journals as a reason for the recommendation of each of the four approaches, ranging from 52.0% (95% CI = 47.6–56.3) for chiropractic/osteopathic manipulation to 71.3% (95% CI = 66.9–75.4) for herbs and other non-vitamin supplements (Table 2). In addition, for each of the four approaches, >70% of physicians who recommended an approach cited feedback from patients as an influence in their decision to recommend, ranging from 69.7% (CI = 65.6–73.5) for herbs and other non-vitamin supplements to 75.6% (95% CI = 71.1–79.8) for acupuncture.
A higher percentage of female physicians who made recommendations cited evidence in peer-reviewed journals as factors for herbs and other non-vitamin supplements (78.8% [95% CI = 72.4–84.3] vs. 66.6% [95% CI = 60.8–72.2], Wald chi-square p = 0.0031) and chiropractic/osteopathic manipulation (62.3% [95% CI = 54.7–69.4] vs. 47.5% [95% CI = 42.3–52.7], Wald chi-square p = 0.0060), compared with their male counterparts (Fig. 2).

Predisposing and enabling factors for recommending complementary health approaches to patients by U.S. physicians who recommended the approach in the previous 12 months, by approach and sex. Error bars represent 95% Korn-Graubard confidence intervals. Denominators for each individual complementary health approach include only physicians who recommended the specific approach. Chiro/osteo, chiropractic/osteopathic manipulation; Evidence in journals, Evidence in peer-reviewed journals; Herbs/non-vit supp, herbs and other non-vitamin supplements; Mind–body, mind–body therapies; OB/GYN, obstetrics and gynecology. Data source: National Ambulatory Medical Care Survey Physician Induction Interview, 2012.
In addition, a higher percentage of female physicians were influenced by colleagues when making recommendations for herbs and other non-vitamins supplements (63.0% [95% CI = 55.8–69.8] vs. 48.3% [95% CI = 46.2–6.12], Wald chi-square p = 0.0011) and chiropractic/osteopathic manipulation (61.1% [95% CI = 53.6–68.2) vs. 50.2% [95% CI = 44.6–55.1], Wald chi-square p = 0.0153) compared with male physicians.
The final significant difference was that a higher percentage of female physicians cited patient reports as an influencing factor for recommending herbs and other non-vitamin supplements compared with male physicians (66.6% [95% CI = 60.8–72.2] vs. 74.7% [95% CI = 68.6–80.2], Wald chi-square p = 0.0389).
Reasons for not recommending complementary health approaches
For all four approaches, a lack of perceived benefit was the most frequently observed reason for not recommending among physicians who did not recommend the particular approach, with at least 4 in 10 of all physicians having chosen this as a reason (Table 5). A higher percentage of female versus male physicians who did not recommend cited lack of information sources as a reason for not recommending herbs and other non-vitamin supplements (31.4% [95% CI = 26.8–36.3] vs. 23.4% [95% CI = 21.0–25.9], Wald Chi Square p = 0.0030).
Reasons for Not Recommending Complementary Health Approaches to Patients by U.S. Physicians Who Had Not Recommended the Approach in the Previous 12 Months, by Sex
Physicians were only asked about the reasons for not recommending a specific complementary health approach if they reported not recommending that specific complementary health approach in the previous 12 months.
CI, confidence interval; KG, Korn-Graubard; n, unweighted sample size.
Data source: National Ambulatory Medical Care Survey Physician Induction Interview, 2012.
A higher percentage of female physicians who did not recommend cited a lack of affordability for the patient as a reason for not recommending mind–body therapies compared with male physicians (20.9% [95% CI = 17.0–25.4] vs. 14.6% [95% CI = 12.8–16.6], Wald chi-square p = 0.0067). Supplementary Tables S1–S4 show the percentage of physicians selecting each reason for not recommending complementary health approaches by physician specialty, for each complementary health approach.
Discussion
This article provides insights into physicians' reasoning behind the recommendation (or lack thereof) for four frequently used complementary health approaches. Physicians who recommend these approaches cite their own personal use of the approaches (predisposing characteristic) and evidence in peer-reviewed literature (enabling factor) as reasons for making recommendations. In addition, for mind–body therapies, chiropractic/osteopathic manipulation, and acupuncture, patient reports, the enabling factor was the most commonly observed influencing factor for making recommendations.
These findings suggest that physicians use a combination of personal experiences and scientific evidence when deciding to recommend, and physicians who recommend approaches may have some degree of trust for both their peers and patients. These findings agree with previous research emphasizing the importance of examining the intersection of the professional and personal worlds of mainstream health care providers to better understand their perceptions and behavior related to complementary health approaches. 48,49
Approximately 50%–70% of U.S. physicians who made recommendations indicated that they were influenced by scientific evidence in peer-reviewed journals (enabling factor). This is consistent with previous research showing that physicians rely heavily on scientific evidence when forming opinions about complementary health approaches. 50 Conversely, a lack of perceived benefit was a major reason for not recommending the four approaches examined. The fact that a large percentage of physicians were influenced by scientific evidence may have been expected, given the research highlighting physicians' desire for more information from randomized clinical trials and evidence-based educational opportunities related to complementary health approaches. 34,51,52
It has been demonstrated that clinicians might be more willing to discuss these approaches if they had formal education about them. 52 This lack of sufficient education might be contributing to incongruity between the level of scientific evidence supporting some complementary health approaches, such as Tai Chi, and the corresponding awareness of such evidence by physicians. 33,53
The current research found that a higher percentage of physicians use scientific evidence (an enabling factor) as a basis when recommending herbs and other non-vitamin supplements and mind–body therapies than for chiropractic/osteopathic manipulation and acupuncture. Research on physicians' assessment of effectiveness and willingness to recommend complementary health approaches has produced inconsistent results. Previous literature examining physician opinions of chiropractic manipulation among samples of physician groups (e.g., rheumatologists, primary care physicians, pediatricians) found that the legitimacy or benefit of chiropractic manipulation was rated below that of mind–body approaches such as relaxation techniques, hypnosis, or biofeedback. 54 –59
A previous national survey of U.S. rheumatologists found that more than half of the sampled physicians believed that chiropractic and acupuncture were very or moderately beneficial, whereas only 37% said herbal supplements were as beneficial. 60 Literature examining physician opinions of acupuncture has suggested that this approach may be considered as more legitimate or beneficial than chiropractic manipulation but less so than some mind–body approaches. 32,55 –57
A potential factor that may influence these findings was seen in a national survey of U.S. internists and rheumatologists that found that when presented with new evidence, physicians tended to hold onto their preexisting attitudes about specific complementary health approaches. 61 These authors hypothesized that extensive experience with these approaches may be more compelling to physicians than evidence offered by clinical research. Future research could further explore why physicians may use scientific evidence differently across individual complementary health approaches when making recommendations.
Although previous research has shown differences in physician versus patient attitudes toward the use of complementary health approaches, 62 the current findings suggest that patient feedback informs physician behavior. Approximately 70%–75% of physicians who recommended these approaches acknowledged the importance of patient reports (enabling factor), and patient reports ranked slightly higher overall for these approaches than evidence from peer-reviewed literature. The fact that patient reports were cited by the majority of physicians is of note, given a recent review and meta-analysis 63 that found that approximately two out of three users of complementary health approaches do not disclose this use to medical providers. It may be that a relatively small group of vocal patients are responsible for this influence.
Apart from patient reports, for all four approaches, physicians who recommend often did so because the patient directly asked for a recommendation (or a “need” in the Andersen Behavioral Model). This finding suggests that patients may take an active role in health care decision making, a finding supported by a systematic review that found a positive association between patient experience and effectiveness and safety of health care. 64 Shelley et al. 65 found that if patients perceive acceptance and nonjudgment from their physicians, they are more likely to disclose the use of complementary health approaches. The current findings suggest that such a collaborative relationship may be common with respect to discussions and decisions about complementary health approaches.
Finally, the current study found that for those physicians not recommending complementary health approaches, the most common reason given was a lack of perceived benefit to the patient. Although inadequate health insurance coverage and lack of affordability have been documented as a barrier to the use of complementary approaches, 66 –68 these reasons were chosen by <20% of all physicians who did not make recommendations for each of the four approaches examined. Together, these findings suggest that physicians in the United States may be more influenced to not recommend by whether they perceive a benefit than by health care access barriers.
Although our previous study using the same dataset 31 found that physician age had no effect on the four complementary health approaches examined in the current study, this may shift as demographic shifts in the United States occur and more scientific data emerge related to the use of complementary health approaches. Future research could benefit from the utilization of multivariable analyses to study the factors associated with physician recommendations beyond those examined in our previous work.
Study limitations
Because the current study is exploratory and employed bivariate analysis to examine relationships between selected physician characteristics and reasons for recommending complementary approaches, conclusions should be viewed with caution and for the purposes of hypothesis generation. For example, although our previous research found that physician age had no association with the four therapies examined in the current study, age was not adjusted for in the current descriptive analyses. Thus, age could be contributing to at least some of the noted differences.
Further, the data included only nonfederal, office-based physicians, so nothing can be said about complementary health approaches by physicians in hospitals, jails and prisons, Veterans Affairs medical facilities, or other non-office-based locations. Due to small cell sizes, estimates for some physician specialties and characteristics could not be presented. In addition, physicians in the specialties (including designated sub-specialties) of anesthesiology, pathology, and radiology are excluded from the survey.
The NAMCS does not collect information on other potentially important physician characteristics such as a physician's board certification, length of time practicing, and whether they had formal courses on complementary health approaches. The NAMCS data are cross-sectional, which precludes establishing causality.
Finally, we used 2012 NAMCS data as these are (to our knowledge) the only nationally representative data available for examining reasons for complementary health approaches recommendations by physicians. However, it is possible that the reasons for recommending these approaches have changed since 2012. Despite these limitations, our study lays the groundwork for future research by being the first to use a nationally representative dataset to present estimates on reasons that U.S. office-based physicians recommend complementary health approaches.
Conclusions
Scientific literature suggests that specific complementary health approaches have benefit for certain health conditions, such as acupuncture and yoga for back pain, and relaxation techniques for headaches. 69 Developing an understanding of the reasons for physicians' decision making about whether or not to recommend these approaches, and the factors influencing these decisions, could inform outreach efforts to researchers and educators to help physicians make appropriate determinations for patients. Similarly, a better understanding of the reasons that some physicians choose not to recommend approaches may help inform the understanding of physician decision making and potential barriers to the acceptance of evidence-based complementary approaches by office-based physicians.
Footnotes
Acknowledgments
The authors wish to acknowledge Drs. Angela Arensdorf and Dave Clark for their helpful comments on a previous version, and Bryan Ewsichek for technical assistance.
Authors' Contributions
B.J.S. designed the study, interpreted the data, and drafted the article. R.L.N. designed the study, interpreted the data, and revised the article. P.M.B. carried out the statistical analysis and interpreted the data. R.S., T.F., and B.W.W. interpreted the data and revised the article. All authors have read and approved the final version of the article and agree with the order of presentation of the authors.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the NCHS or the Centers for Disease Control and Prevention.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Four authors were employed by the U.S. Federal Government. No additional funding was provided.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.