
Abstract
Objectives:
Although many studies have shown that acupuncture can improve sleep quality, there is no clear evidence by objective physiological measures. The authors investigated the effects of acupuncture on the autonomic indices of heart rate variability (HRV) during sleep.
Design:
The authors applied true acupuncture and sham-site stimulations in 10 healthy adult males (mean ± standard deviation age, 40 ± 9 years) and compared autonomic nerve indices of HRV during each sleep stage in a crossover design. The sleep stages were estimated by the combined analysis of an HRV maker of non-rapid eye movement (REM) sleep (HRV sleep index [Hsi]) and actigraphic body movement.
Results:
Heart rate was lower (true vs. sham acupuncture, mean ± standard error of the mean, 60.9 ± 1.8 vs. 61.7 ± 1.7 bpm, p < 0.0001) and the power of low-frequency and high-frequency components of HRV was higher (35.6 ± 2.0 vs. 34.7 ± 2.0 msec, p = 0.04 and 26.7 ± 3.2 vs. 25.8 ± 3.2 msec, p < 0.0001, respectively) after the true acupuncture compared with the sham-site stimulation throughout sleep. During non-REM sleep, heart rate was lower (59.6 ± 1.8 vs. 60.1 ± 1.8 bpm, p = 0.0004) and the power of low-frequency and high-frequency components were higher (27.7 ± 1.8 vs. 26.1 ± 1.8 msec p = 0.0004 and 28.4 ± 3.5 vs. 27.7 ± 3.5 msec, p = 0.004) after the true acupuncture than the sham-site stimulation. Whereas during REM sleep, there was no significant difference in either HRV indices between them, while heart rate was lower after the true acupuncture than the sham-site stimulation (60.8 ± 1.6 vs. 61.7 ± 1.6 bpm, p < 0.0001).
Conclusions:
Acupuncture increases parasympathetic HRV indices during sleep, especially during the non-REM stage.
Introduction
Sleep plays an important role in recovering from fatigue and repairing the nervous system and other organs. Long-term sleep deprivation or poor sleep quality has been linked to a number of physical and mental illnesses and dysfunctions, including lowered immunity, endocrine disorders, mood swings, lack of attention, poor work performance, and increased risk of accidents. 1
It is a common clinical experience that acupuncture has an improving effect on sleep. Many studies have been conducted on acupuncture for insomnia, and systematic reviews have shown that it is as effective as or more effective than existing medications, with fewer side effects. 2 The mechanism of action is thought to be the regulation of the hypothalamus–pituitary–adrenal system and the influence of neurotransmitters such as endorphins, gamma-aminobutyric acid, serotonin, norepinephrine, adrenocorticotropic hormone, cortisol, acetylcholine, substance P, and nitric oxide. 3 Studies using functional magnetic resonance imaging show that acupuncture modulates activity in specific brain regions associated with the sleep experience, including the frontal lobe, temporal lobe, parietal lobule, anterior cingulate gyrus, supramarginal gyrus, and precuneus. 4
Acupuncture is also thought to regulate autonomic nervous functions, and one of the treatment mechanisms of acupuncture is to increase parasympathetic nerve activity in particular. The authors have previously shown that acupuncture by the epifascial stimulation method (shallow stimulation that does not produce de qi, a characteristic radiating sensation of heaviness, numbness, paresthesia, prick and sting) to Danzhong (CV17) increases cardiac parasympathetic activity and decreases heart rate. 5 In studying the sleep-improving effects of acupuncture, it is important to investigate the effects on autonomic nervous function during sleep. However, few studies have examined the autonomic effects using objective measures.
Also, most previous studies used acupuncture stimulations that produced de qi sensations with needles inserted deeply through the subcutaneous fascia, or electroacupuncture. 6 There are no reports on the autonomic effects during sleep after the epifascial stimulation, which is commonly used in clinical practice. 5
In the present study, the authors investigated whether acupuncture to the basic points of Kurono's method of whole-body adjustment (CV12, LR14, ST25, CV6, BL10, GB20, BL11, GB21, BL13, BL14, BL20, BL23, and BL25) 7 with the epifascial stimulation method affects autonomic nervous functions during sleep and sleep quality. The effects of the acupuncture were evaluated by a crossover design comparing between true acupuncture and nonacupuncture (sham)-site stimulations. The autonomic nervous functions were objectively assessed by heart rate variability (HRV) analysis separately during non-rapid eye movement (REM) and REM sleep stages. The sleep stage was estimated using the HRV sleep index (Hsi), which detects non-REM sleep, and body acceleration, which discriminates between sleep and wakefulness. 8 The authors also investigated whether the effects of acupuncture on HRV during sleep differ depending on the sleep stage.
Methods
Study ethics
This study was performed according to the protocol approved by the Ethics Review Committee of the Nagoya City University Graduate School of Medical Sciences, Nagoya, Japan (No. 539).
Participants
The participants were 10 healthy males (mean ± standard deviation [SD] age, 40 ± 9 years) who applied for the recruitment at the Institute of Oriental Medicine. The eligibility criteria were as follows: (1) age: 20–60 years, (2) no medication for at least 2 weeks, and (3) normal ECG findings. Written informed consent for participation in this study was obtained from all participants.
Protocol
Subjects were divided into two groups, A and B, of five people each, by drawing one sealed envelope containing a tag marked A or B. After a 1-week treatment-free period without medication or acupuncture, the intervention was conducted in a crossover design, with group A receiving true acupuncture and sham-site stimulations in that order, and group B receiving them in the reverse order (Fig. 1). The two interventions were conducted with a 1-week washout period with no medication or acupuncture in between. Previous crossover studies 9,10 that evaluated the effects of acupuncture on insomnia had used a washout period of 1 week, and the washout period was also set at 1 week for the present study.
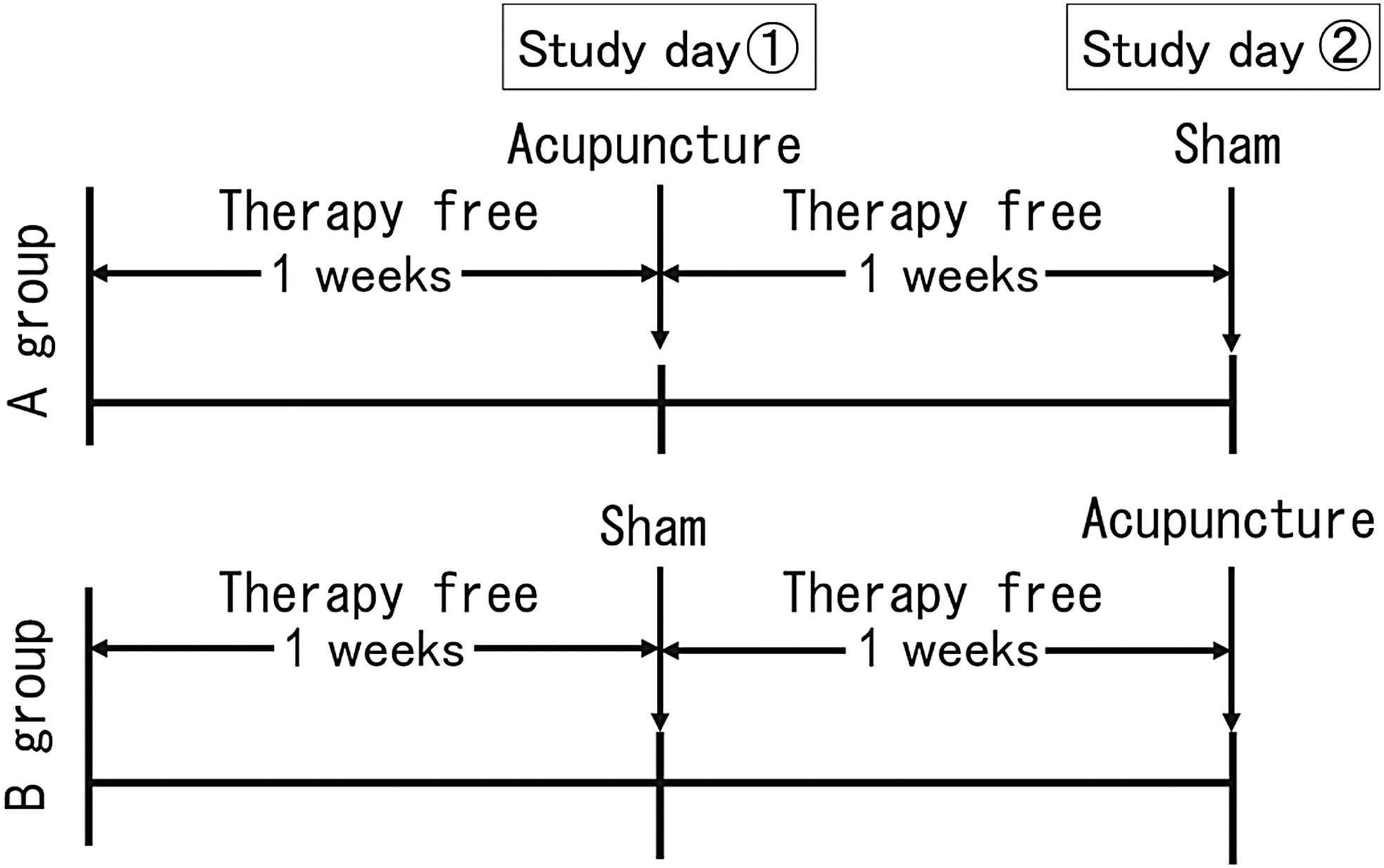
Study design.
On being selected to participate in the study, subjects were instructed to abstain from alcohol and tobacco from the day before each intervention day, and to go to bed by 24:00. All subjects confirmed that these instructions were followed. On each intervention day, subjects wore a Holter electrocardiograph (Cardy 303 pico; Suzuken Co., Ltd., Nagoya, Japan) with a built-in three-axis accelerometer before the intervention (14:00), and ECG and three-axis body acceleration were recorded until 12:00 the next day. The ECG was recorded digitally with a sampling frequency of 125 Hz and a resolution of 10 bits (20 μV/dig), and the acceleration was recorded digitally for each axis at 31.25 Hz and 13 bits (1.95 mG/dig). Subjects were instructed to go to bed by 24:00 without taking a bath on the intervention day.
Intervention
The true acupuncture was performed with the epifascial stimulation method to the basic sites of Kurono's method of whole-body adjustment (CV12, LR14, ST25, CV6, BL10, GB20, BL11, GB21, BL13, BL14, BL20, BL23, and BL25). 7 These basic acupuncture points were determined by an empirical study of the acupuncture points in 2083 patients treated over a 13-year period as the 13 acupuncture points used during more than 40% of the period (Fig. 2). 7 Both true acupuncture and sham-site stimulations were applied with the epifascial stimulation method, in which needles were inserted vertically to a depth of 5–7 mm with a pressure of 20 g on the fascia surface, and the needles are immediately removed within 1 sec after reaching the required depth (Fig. 3).

The basic acupuncture points of the Kurono method for total body adjustment and the points used for sham-site acupuncture stimulation.
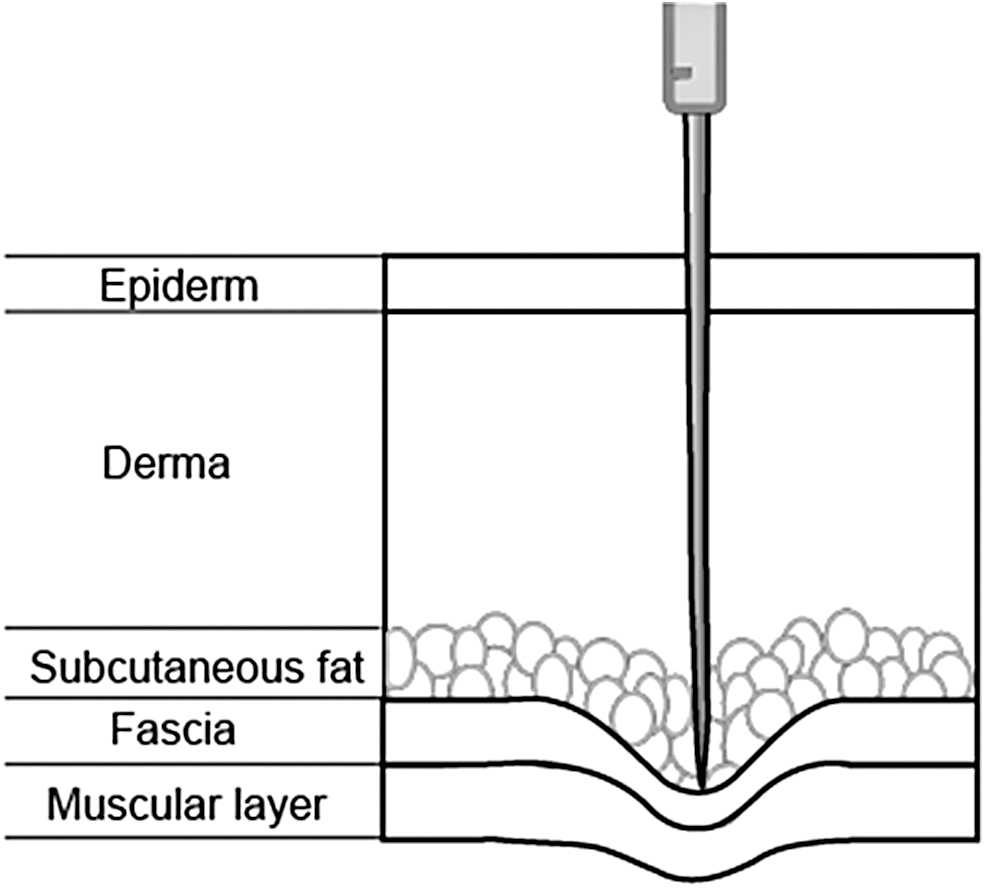
Schema showing the characteristics of acupuncture by the epifascial stimulation method. Acupuncture needles are inserted vertically so that they do not penetrate the muscle/periosteal fascia and apply about 20 g of pressure to its surface.
These acupuncture points and techniques are used in clinical practice. 5 For the sham-site stimulation, acupuncture needles were placed in the center of the anterior surface of the thigh (nonacupuncture site) at a depth of about 5 mm for 5 min.
The acupuncture needles were disposable stainless-steel needles (ϕ0.16 × 30 mm) sterilized by ethylene oxide (Nissin Medical Equipment Co., Ltd.). All acupuncture interventions were performed by one of the authors (T.I.), who is licensed as an acupuncturist by the Ministry of Health, Labour and Welfare, has 31 years of clinical experience, and a previous study (unpublished) has confirmed that she can reproduce the same 20 g strength acupuncture stimulation.
Data analysis
All QRS waves of ECG were detected and rhythms were classified by a Holter ECG scanner (Cardy Analyzer 05; Suzuken Co., Ltd.; Specified Maintenance Controlled Medical Equipment certified by Japanese Ministry of Health, Labor, and Welfare, No. 222AGBZX00225A01), and the time series of R-R intervals were obtained. Nonsinus beats and artifacts interfering R-wave detection were detected by the scanner, and the results were reviewed and edited by a skilled operator. Only consecutive sinus-rhythm R-R interval (N-N interval) time series were converted into a continuous function by step interpolation and resampled at 2 Hz into equidistantly sampled time series.
To analyze the temporal changes of HRV indices, the amplitudes of the low-frequency (LF, 0.04–0.15 Hz) and high-frequency (HF, 0.15–0.45 Hz) components in the obtained N-N interval time series were continuously demodulated by the complex demodulation (CDM) analysis, 11 and the time series of the amplitude of each frequency component was calculated. The time series of the power ratio (LF/HF) was calculated as the squared value of the ratio of the obtained LF and HF amplitudes. The CDM method was employed to analyze HRV at each sleep stage, which is not expected to be stationary and varies at various intervals. CDM continuously analyzes the dynamic changes in the amplitude of the LF and HF components as a function of time. The reliability of this method and the software used in this study have been previously reported. 11
The amplitude of cyclic variation of heart rate (Acv) was also determined by the autocorrelated wave detection with adaptive threshold method. 11 Acv reflects the chronotropic response to apneic stimuli due to sleep apnea episodes and is an indicator of the reflex parasympathetic function. 12
For the three-axis acceleration data, the inclination of the recorder in the three-axis direction was estimated from the direction of the gravity vector recorded in each axis when the subject was standing up, and the body position during the measurement was estimated from the acceleration data corrected for the effect of inclination. From the estimated body position, the authors detected the duration of the supine state during the night and estimated the bedtime and wake-up time. From the acceleration data of each axis, the low-pass filtered components below 0.25 Hz were excluded as the gravitational acceleration components, and the scalar of the composite vector of the components passed through the band-pass filter from 2 to 3 Hz and was averaged at 0.5-sec intervals to obtain the index of body motion.
The Hsi method 8 was used to estimate the sleep stage by ECG and acceleration. The N-N interval time series during bedtime obtained by the above method was analyzed, and the highest spectral peak in the frequency band from 0.15 to 0.4 Hz was detected as the HF peak, and the peak frequency was identified. The area under the curve was calculated as a function of the width of the frequency band, with the peak frequency as the center. Hsi is a measure of how much of the power of the HF component of HRV is concentrated in a narrow frequency range, reflecting the regularity of breathing. During non-REM sleep, respiration becomes more regular than during wakefulness and REM sleep because respiration switches from voluntary to involuntary breathing, and Hsi increases.
In the present study, the portion of Hsi that exceeded 70% during bedtime was determined to be non-REM sleep. For the rest of the bedtime, the periods were judged as arousal when the body movement index was >2.5 mG and the other periods were as REM sleep. 8
Time in bed, sleep period time, total sleep time, sleep latency, and sleep efficiency (% of total sleep time in time in bed) were indicators of sleep quality. Also calculated were the total length and % of non-REM, REM, and waking periods.
The mean values of heart rate, the amplitude of LF and HF components, and LF/HF were calculated for the time in bed and for each sleep stage. In this study, HRV in normal subjects during sleep in bed was analyzed. Therefore, the amplitude of LF component was interpreted as an index reflecting both sympathetic and parasympathetic nervous functions and HF component as an index of parasympathetic nervous functions. 11 In addition, the mean value of Acv during the sleeping period was calculated and used as an index of parasympathetic responsiveness. 12
Statistical analyses
The Statistical Analysis System (SAS, Cary, NC) was used for statistical analyses. In graphs of changes in heart rate and HRV indices over time, the mean and SD of all subjects' measurements were calculated every minute or every 5 min, separately for true acupuncture and sham-site stimulations. To evaluate the effect of true acupuncture against sham-site stimulation, the SAS mixed procedure was used to analyze the statistical significance of the effect of the type of acupuncture stimulation (true or sham site), group (A and B), and order (first and second) as fixed effects, and participants as random effects, using the Bonferroni method. The least-squares means and their standard errors were calculated for true acupuncture and sham-site stimulations adjusted for the effects of group and order.
Type 1 error level α was set to <0.05 and type error level β to <0.20. Based on the results of a previous study 5 on the effect of acupuncture on HF amplitude in HRV, the effect size and SD of acupuncture-induced changes in HF amplitude were estimated to be 3.5 and 3.0 msec, respectively, from which the number of subjects needed for paired comparisons was estimated to be 8. Thus, the authors employed 10 subjects in this study.
Results
Sleep quality
Since there were significant differences in sleep efficiency (F = 13.36, p = 0.006), total wake period (F = 12.51, p = 0.007), and %wake period (F = 22.34, p = 0.00) between groups A and B, the authors adjusted for these effects and analyzed the effect of true acupuncture against sham-site stimulation. The results showed that there was no significant difference between true acupuncture and sham-site stimulations in either sleep indices (Table 1).
Effect of Acupuncture on Sleep Quality
Least-square mean ± SEM adjusted for the effects of group and order.
Difference (acupuncture minus sham) ± SEM.
%NREM, %NREM period; %REM, %REM period; %Wake, %Wake period; NREM, total NREM period; REM, total REM period; SE, sleep efficiency; SEM, standard error of the mean; Sham, sham-site stimulation; SL, sleep latency; SPT, sleep period time; TIB, time in bed; TST, total sleep time; Wake, total wake period.
Autonomic indices during time in bed
After adjusting for the effects of group and order, the heart rate (F = 53.7, p < 0.0001) was lower, and the amplitude of LF (F = 3.95, p = 0.04) and HF (F = 26.48, p < 0.0001) was higher after true acupuncture compared with sham-site stimulation (Table 2 and Fig. 4). Acv was also higher after true acupuncture than after sham-site stimulation (F = 5.62, p = 0.04). LF/HF did not differ significantly between acupuncture and sham-site stimulations.
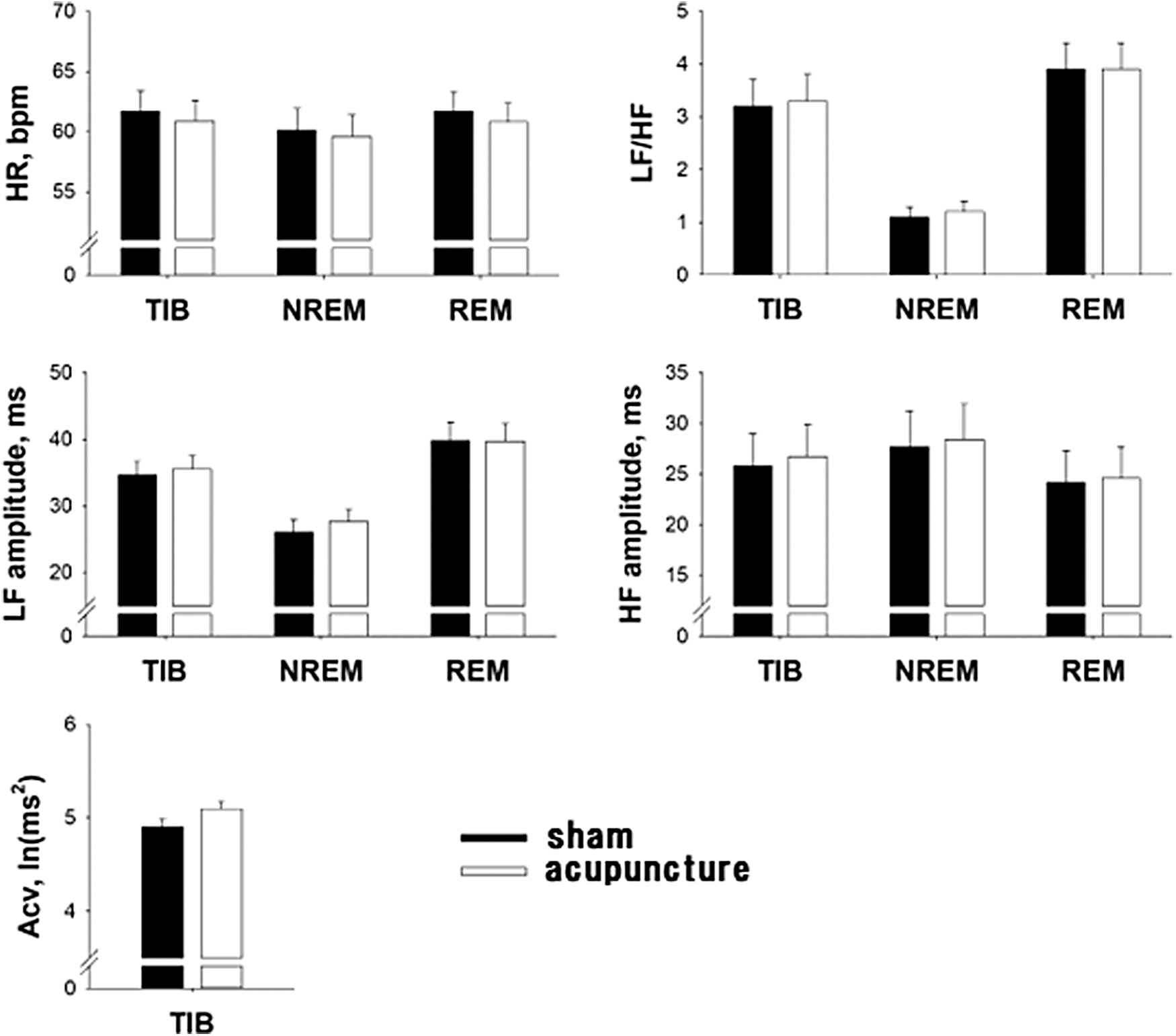
Effects of acupuncture and sham acupuncture stimulation on autonomic indices in each sleep stage. Values are least-square mean ± SEM adjusted for the effects of group and order. SEM, standard error of the mean.
Significance of the Difference in Autonomic Indices at Each Sleep Stage Between Acupuncture and Sham Acupuncture Stimulation
Difference (acupuncture minus sham) ± SEM.
Acv, amplitude of cyclic variation of heart rate; HF, high frequency; HR, heart rate; LF, low frequency; NREM, total NREM period; REM, total REM period; SEM, standard error of the mean; Sham, sham-site stimulation; TIB, time in bed.
Autonomic index during each sleep stage
Adjusting for the effects of group and order, the heart rate (F = 12.44, p = 0.0004) was lower, and the amplitude of LF (F = 12.77, p = 0.0004) and HF (F = 8.05, p = 0.004) was higher after true acupuncture than after sham-site stimulation during non-REM sleep. In REM sleep, the heart rate was lower after true acupuncture than after sham-site stimulation (F = 41.8, p < 0.0001), but the amplitude of LF and HF did not differ significantly between acupuncture and sham-site stimulations. Acupuncture had no significant effect on LF/HF in both non-REM and REM periods.
Associations between acupuncture effects on sleep quality and HRV
Correlation coefficients of the changes with true acupuncture between HRV and sleep parameters are presented in Table 3. Among the HRV indices that showed significant changes with acupuncture, significant correlations were observed between an increase in LF amplitude and a decrease in %REM period and between a decrease in heart rate (HR) during REM and increases in total sleep time and sleep efficiency.
Correlations of the Effects of True Acupuncture Between Sleep and Heart Rate Variability Parameters
Data are correlation coefficients.
Significant correlation coefficients.
%NREM, %NREM period; %REM, %REM period; %Wake, %Wake period; HF, high frequency; LF, low frequency; NREM, total NREM period; REM, total REM period; SE, sleep efficiency; SL, sleep latency; SPT, sleep period time; TIB, time in bed; TST, total sleep time; Wake, total wake period.
Discussion
This is the first study to evaluate the effects of acupuncture on autonomic activity during sleep in healthy subjects by analyzing HRV. It is also the first study to show that the effect of acupuncture on autonomic nerve activity varies with sleep stage. By the comparisons between true acupuncture and sham-site stimulations with a crossover design, the authors found that there was no significant difference in the parameters of overall sleep quality, but there was a decrease in heart rate and an increase in LF and HF amplitudes.
Together with the observation of no significant change in LF/HF, these indicated that acupuncture increases cardiac parasympathetic nerve activity during sleep. In addition, there was an increase in Acv, suggesting that acupuncture may also improve cardiac vagal responsiveness during sleep. The lack of change in the parameters of sleep quality could be because the subjects were healthy people with no sleep problems, and so, there was no room for improvement by acupuncture.
The evaluation of autonomic nerve activity during non-REM and REM sleep estimated by Hsi showed that during non-REM sleep, there was a decrease in heart rate and increases in LF and HF after acupuncture, while during REM sleep, only a decrease in heart rate was observed. This suggests that acupuncture may increase cardiac parasympathetic activity, 13 especially during non-REM sleep. It has been suggested that REM sleep is accompanied by increases in both sympathetic and parasympathetic activities. 14 These observations that acupuncture decreased heart rate in REM sleep without changing the parasympathetic indices of HRV may suggest the suppression of sympathetic activation during REM sleep by acupuncture.
The effect size of heart rate decrease with acupuncture was less than 1 bpm for overall sleep and non-REM sleep. Thus, its hemodynamic effects may be small, but there was an increase in the HF and LF of the HRV index. It has been shown that changes in heart rate and HRV indices during sleep may not coincide; there may be no difference in HF even if the heart rate decreases, or no difference in heart rate even if there is a difference in HF. 15,16 In this study, even though there was little change in heart rate, the results of the HRV index suggested that there was an increase in parasympathetic tone.
Studies examining autonomic activity during sleep in people with insomnia by HRV analysis have shown different results across studies and are inconclusive, but the majority of studies have shown increased heart rate and decreased HF in people with insomnia, suggesting that insomnia may be associated with decreased parasympathetic activity. 17 Studies of auricular acupressure therapy 18 and aromatherapy 19 for insomnia have shown that improvement in insomnia is associated with increased parasympathetic HRV indices at rest during wakefulness. A study examining the relationship between autonomic nerve activity during sleep and subjective sleep quality using the MA version of the Oguri Shirakawa Azumi (OSA) Sleep Questionnaire 20 showed that parasympathetic nerve activity during sleep correlated with Factor IV (recovery from fatigue). 21 The authors also reported in a previous study that subjective sleep quality using the MA version of the OSA Sleep Questionnaire improved with an acupuncture treatment similar to that of the present study. 22
The present study showed that the mechanisms of the effect of acupuncture involve increased parasympathetic nerve activity during sleep, especially during non-REM sleep.
In this study, the authors used Hsi to estimate REM and non-REM sleep. Generally, polysomnography is necessary to determine the sleep stage, but it could affect the autonomic nerve activity of the subject due to the wearing of many sensors. In this study, only a small Holter ECG recorder was used, minimizing the impact of the measurements on the subjects, and thus, the authors were able to evaluate the impact of acupuncture on autonomic nerve activity during sleep in a more physiological state.
Correlation analysis between acupuncture effects on HRV and sleep parameters showed significant correlations between increased LF amplitude and decreased %REM duration, and decreased HR during REM and increased total sleep time and sleep efficiency. Although some of these results may reflect the mechanisms of acupuncture effects, a causal relationship between sleep and autonomic function cannot be determined from the present study. Therefore, it is unclear whether the changes in HRV are the result of acupuncture-induced changes in sleep structure or the cause of changes in sleep structure.
Limitations
The current study has several limitations. First, the study was conducted in healthy men. The results may not be applicable to women or patients with mental illness, particularly insomnia. To prove the clinical effectiveness of this treatment on insomnia, studies on various populations need to be conducted. Second, since this study assessed autonomic nerve activity on the night of a single acupuncture session, the authors do not know the effects of continuous treatment or the time course of the effects. Future studies should be conducted to evaluate these factors.
Third, in this study, acupuncture stimulation to nonacupuncture points was performed as sham acupuncture. Therefore, the subjects were able to recognize the difference between the two interventions. Therefore, they cannot deny the possibility that the placebo effect in favor of acupuncture may have affected the results as a bias. Previous studies on acupuncture have attempted to eliminate the bias by conducting randomized controlled trials using various methods of sham acupuncture such as nonacupuncture, shallow acupuncture, and sham acupuncture. 23,24 However, there are many cases where it is not possible to exclude subjects from noticing sham acupuncture, and an appropriate method of sham acupuncture has not been established. In the future, it is necessary to explore research designs with appropriate sham acupuncture methods.
Finally, the effect size of acupuncture on nocturnal HR was small, and the change in HRV index may be only statistically significant. However, the clinical relevance of these findings cannot be determined in this study because the subjects were healthy subjects without sleep disorders. Future studies are desirable to examine the association between the changes in HRV indices and symptomatic or objective sleep quality.
Conclusion
The effect of acupuncture with the epifascial stimulation method on autonomic nerve activity during sleep was examined with a crossover design using sham-site stimulation as a placebo. Acupuncture increased parasympathetic nerve activity during sleep, especially during non-REM sleep.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to the Japanese Society for Biological Control, the Institute of Oriental Medicine, and Heartbeat Science Lab for their cooperation in this study.
Authors' Contributions
T.A., Y.K., M.M., and A.Y. participated in the conception and design of the study. J.H. participated in the acquisition of data and analyzed the data. T.A., J.H., and A.Y. provided the first draft of the article. The corresponding author confirms that all the authors have read and approved this article.
Author Disclosure Statement
None of the authors had any conflicts of interest to report for this study.
Funding Information
This study had no funding support.