
Abstract
Objective:
Systematic review and meta-analysis to assess the efficacy of Manual therapy and related interventions in the treatment of carpal tunnel syndrome (CTS) based on Boston carpal tunnel questionnaire.
Design:
Systematic review and meta-analysis.
Subjects:
Carpal tunnel syndrome.
Interventions:
Manual therapy and related interventions versus other therapies or manual therapy and related interventions plus other therapies versus other therapies.
Outcomes measures:
Boston carpal tunnel questionnaire.
Results:
A total of 6 studies were included, including 211 cases in the manual therapy group and 211 cases in the control group. The quality of the included articles was high, and the results of meta-analysis showed that manual therapy and related interventions were superior in terms of improving the Boston carpal tunnel questionnaire Symptom Severity score in patients with CTS (standardised mean difference [SMD] −1.13, 95% CI −1.40 to −0.87), were superior to control groups in terms of improving the Boston carpal tunnel questionnaire functional capacity scale in patients with CTS (SMD −1.01,95% CI −1.24 to −0.77).
Conclusion:
The results of this meta-analysis suggested that manual therapy and related interventions were better than control groups in treating CTS. Manual therapy and related interventions could relieve the symptoms of patients with CTS and promote the recovery of hand function. Manual therapy and related interventions should be considered clinically effective methods for treating CTS.
Registration:
The protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO; No. CRD 42020201389).
Contribution of the Article:
Manual therapy and related interventions could relieve the symptoms of patients with CTS and promote the recovery of hand function. Manual therapy and related interventions should be considered clinically effective methods for treating CTS.
Introduction
Carpal tunnel syndrome (CTS) is the most common peripheral nerve entrapment syndrome, 1 in which symptoms and signs are caused by the compression of the median nerve in the carpal tunnel. 2 Common symptoms of CTS are paresthesia in the affected limb, such as numbness, tingling, pain, and weakness of the nerve distribution in the distal carpal tunnel. 3,4 In the general population, 8% of people develop CTS at some point in their lives, 5 and women are more likely to experience it. 6 Studies have shown that diabetes, hypothyroidism, arthritis, obesity, and pregnancy are all high risk factors for CTS, 7 –11 along with body mass index and vitamin B12 deficiency. 12
Current treatments for CTS include laser therapy, pharmacotherapy, therapeutic ultrasound, musculoskeletal manipulation and splinting, complementary therapies, and surgical treatment. 13 Study showed that conservative treatment was more common than other treatment options. 14 The authors sought to objectively assess the potential role of manual therapy in the management of CTS. Therefore, they conducted a systematic review and meta-analysis of randomized controlled trials to establish the effect of manual therapy on the key outcomes of symptoms and function in patients with CTS.
Methods
All analyses were based on previous published studies, thus no ethical approval and patient consent are required.
The search strategy and selection criteria in this systematic review and meta-analysis are reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Statement and was registered at International Prospective Register of Systematic Reviews (No. CRD 42020201389).
The authors selected relevant studies published by searching Embase, PubMed, Cochrane, and Web of Science. They used the following combined text and MeSH terms: “Manual Therapy” and “carpal tunnel syndrome.” For the complete search used for PubMed see Table 1. They considered all potentially eligible studies for review, irrespective of the primary outcome or language. They also conducted a manual search, using the reference lists of key articles published in English.
Search Strategies in PubMed
Study selection and data extraction
Studies that met the following criteria were included in the study: (1) patients diagnosed with CTS, (2) manual therapy and related interventions versus other therapies, (3) manual therapy and related interventions plus other therapies versus other therapies, (4) the primary outcomes included symptom severity and functional status (Boston carpal tunnel questionnaire), and (5) randomized controlled trial design. Studies that met any of the following criteria were excluded from the study: (1) case reports, nonrandomized controlled trials, reviews, and animal trials; (2) unspecified procedures as part of the intervention; (3) treatment consisting of surgical procedures; (4) article data are not available and the full text is not available; and (5) trials involving patients with serious underlying conditions such as diabetes, hypertension, and heart disease.
Two independent investigators (H.J.D. and Q.Y.) reviewed study titles and abstracts, and studies that satisfied the inclusion criteria were retrieved for full-text assessment. Trials selected for detailed analysis and data extraction were analyzed by two investigators (J.A. and Q.D.) with an agreement value (κ) of 96 · 5%; disagreements were resolved by a third investigator (X.Y.Y.).
The authors extracted the following data from each selected study: general characteristics (first author, published year, sample size, Boston symptom severity scale, and Boston functional capacity scale) and outcomes based on Boston carpal tunnel questionnaire before and after the application of manual therapy.
Statistical analysis
The authors used Stata (version 15.0; Statacorp, College Station, TX) for all statistical analyses. Different statistical analyses were applied for different data types. Weighted mean differences and confidence interval (95% CI) were used to analyze continuous data. The mean and standard deviation were extracted from the authors of each article or calculated by other values. For statistical heterogeneity, the Cochrane Q test was used to assess heterogeneity, and the I 2 test for inconsistency. Sensitivity analyses were conducted by removing studies with high risk of bias was introduced if the value of I 2 > 50% or p < 0.1. Publication bias was not assessed for cases of <10 studies in a group.
Risk of bias
The Physiotherapy Evidence Database (PEDro) scale 15 was used to assess the methodology quality and risk of bias of studies included in this systematic review. It was assessed by two independent authors (Q.Y. and H.J.D.), and a third author (Q.D.) intervened in case of disagreement. One point is awarded if the criteria is clearly satisfied as assessed by the following cut points: 9–10, excellent; 6–8, good; 4–5, fair; and <4, poor.
Result
Literature search
After searching the database, 123 literatures were obtained, and 66 literatures were reconstructed. After preliminary screening and rescreening, of which six were published between 2012 and 201716–21 (with data for 422 participants) and included in the analysis (Fig. 1). 16 –21

The Screening flowchart.
The basic characteristics of included literature
A total of six articles were included, including 211 patients in the manipulation group and 211 patients in the control group. The treatment group comprised one to six treatment sessions, and intervention duration varied from 1 to 10 weeks. One study applied osteopathic manipulation, 16 two studies applied manual therapy, 17,21 one study applied massage techniques, 18 and two studies applied fascial manipulation, 19,20 The control group mostly used laser, physical, surgical, and other treatment methods (Table 2).
Characteristics of Included Trials
BF, Boston functional capacity scale; BS, Boston symptom severity scale; CG, control group; NOP, number of patients; OG, observation group; RCT, randomized controlled trial.
Risk of bias assessment
The methodological quality assessed by the PEDro scale indicated an overall high quality for the studies included in this systematic review. Four of the six studies scored between 8 and 11 with an average of 8. 16,17,20,21 One study scored a lower score of 6/11, 18 and another scored 7/11. 19 The principal bias found between all studies was that there was no blinding of the therapists who administered the therapies. However, due to the nature of the manual therapy techniques, it is not possible to completely blind a therapist (Table 3).
PEDro Scale
Item 1: eligibility criteria were specified; Item 2: subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received); Item 3: allocation was concealed; Item 4: the groups were similar at baseline regarding the most important prognostic indicators; Item 5: there was blinding of all subjects; Item 6: there was blinding of all therapists who administered the therapy; Item 7: there was blinding of all assessors who measured at least one key outcome; Item 8: measures of at least one key outcome were obtained from >85% of the subjects initially allocated to groups; Item 9: all subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analyzed by “intention to treat”; Item 10: the results of between-group statistical comparisons are reported for at least one key outcome; Item 11: the study provides both point measures and measures of variability for at least one key outcome.
PEDro, Physiotherapy Evidence Database.
Outcome A: Boston symptom severity scale before and after intervention
Six 16 –21 trials reported measurements from the Symptom Severity scale before and after intervention assessed through the Boston carpal tunnel questionnaire, with a total of 422 patients (211 from the experimental group and 211 from the control group) included in the analysis with high heterogeneity (p = 0.00, I 2 = 90.4%). Heterogeneity decreased after two trials 17,20 were removed (p = 0.82, I 2 = 0.0%) during sensitivity analysis. The pooled results showed that compared with control groups, manual therapy and related interventions were superior in terms of improving the Boston carpal tunnel questionnaire Symptom Severity score in patients with CTS (standardised mean difference [SMD] −1.13, 95% CI −1.40 to −0.87) (Fig. 2).
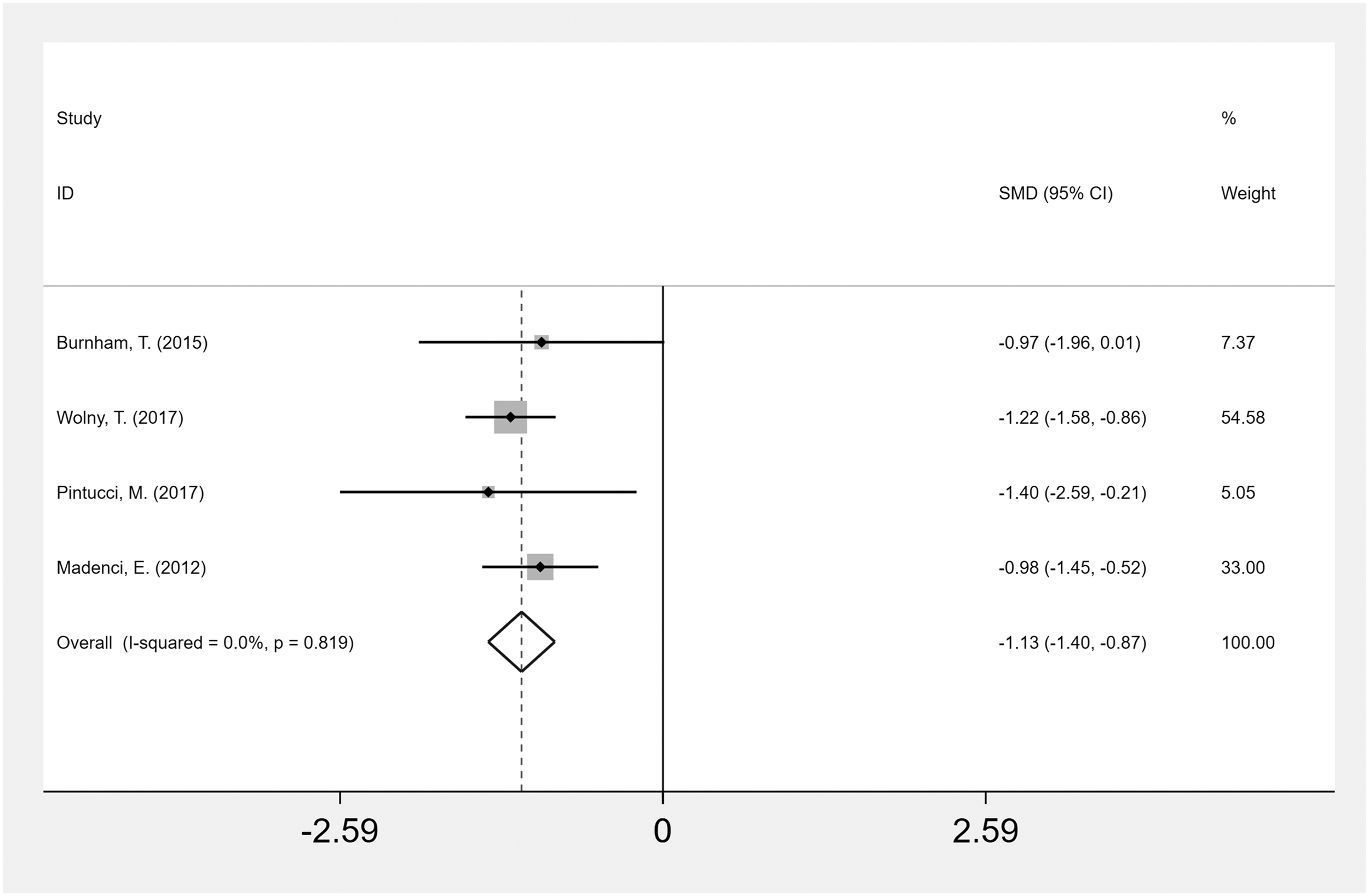
Boston symptom severity scale before and after intervention. CI, confidence interval.
Outcome B: Boston functional capacity scale before and after intervention
Six
16
–21
trials reported the functional capacity scale before and after intervention assessed through the Boston carpal tunnel questionnaire, with a total of 422 patients (211 in the experimental group and 211 in the control group) included in the analysis (p = 0.20, I
2 = 31.2%). Pooled results showed that compared with control group, manual therapy and related interventions were superior to control groups in terms of improving the Boston carpal tunnel questionnaire functional capacity scale in patients with CTS (SMD-1.01, 95% CI −1.24 to −0.77)
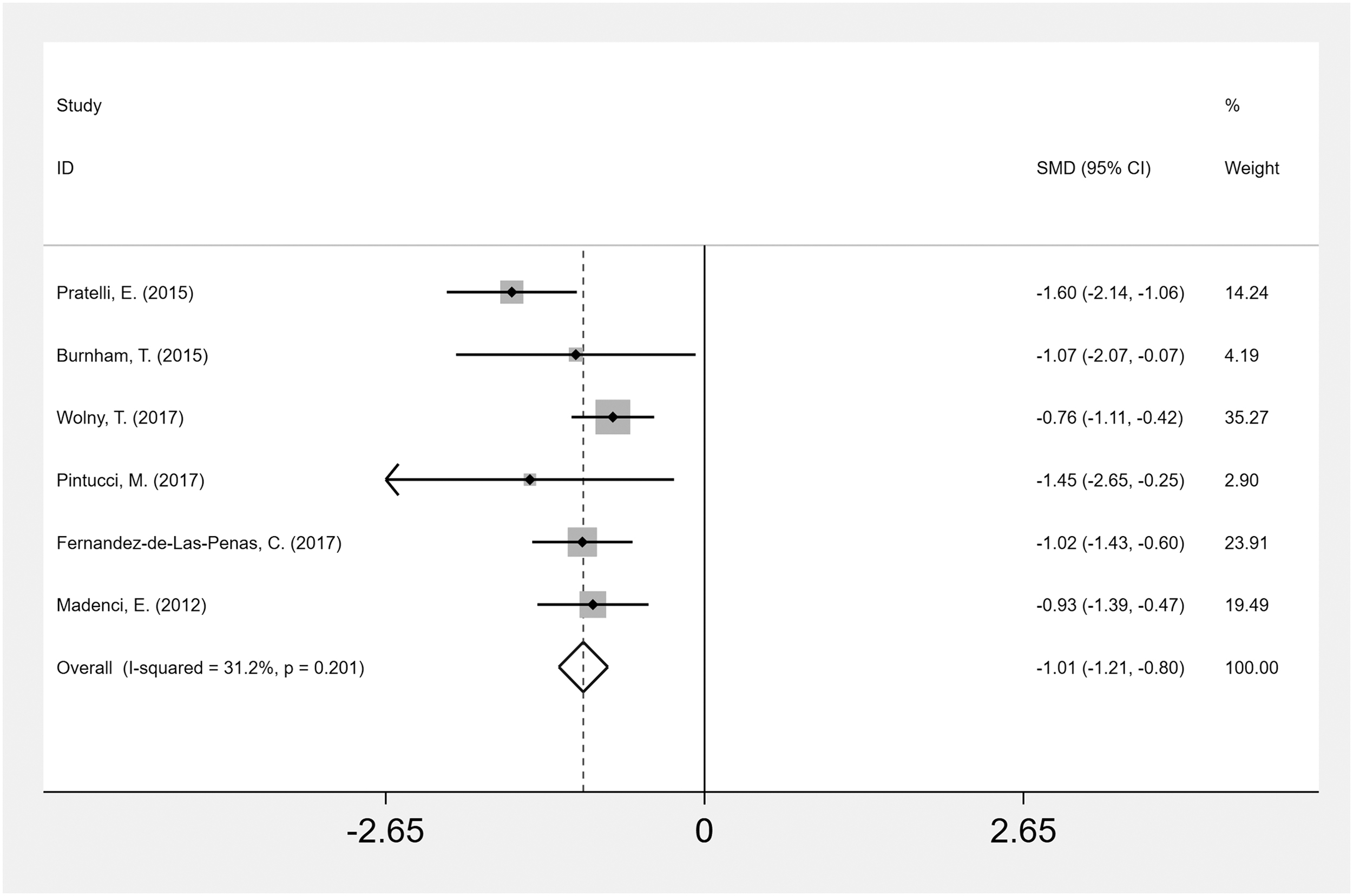
Boston functional capacity scale before and after intervention. CI, confidence interval.
Discussion
To the authors' knowledge, at the inception of this research, there was no systematic review and meta-analysis on this topic. Therefore, the authors believe that this study can provide us with new therapeutic options in clinical practice.
The results of this systematic review suggested that manual therapy and related interventions were effective in patients with CTS compared with controls. Based on the Boston carpal tunnel Questionnaire score, manual therapy and related interventions significantly relieved symptom severity and improved functional capacity in patients with CTS compared with the control group. The results support manual therapy and related interventions as an effective treatment strategy for CTS. The conclusion is consistent with the previous conclusion of Hernández-Secorún et al. 22
In fact, as a conservative therapy, manual therapy and its related interventions are widely used in the treatment of CTS. However, due to the lack of effective clinical evidence, there is no effective guidance for clinical practice. Therefore, it is necessary to explore the evidence of the effectiveness of manual therapy and related interventions for the treatment of CTS. The results of this meta-analysis are consistent with the previous systematic reviews that show manual therapy as effective for reducing pain intensity and improving function. 22,23,24 Evidence of the benefits of CTS for a diverse collection of exercise and mobilization interventions is limited and of very low quality. 25
Short-term low-level laser therapy (LLLT) has been shown to be more effective as a single intervention than placebo LLLT in patients with CTS, but medium- and long-term evidence is lacking, 26 but it offers limited additional benefits over splinting alone in terms of pain reduction, reduction of symptom severity, or improvement of functional status, 27 There is limited evidence that a splint worn at night is more effective than no treatment in the short term, but there is insufficient evidence regarding the effectiveness and safety based on variations in splint design or wearing regimen, or of the use of splint over other nonsurgical interventions for CTS.
Thus, more research is needed on the long-term effects of these interventions for CTS. 28 For example, platelet-rich plasma injection may be effective for mild to moderate CTS and superior to traditional conservative treatments in improving pain and function and reducing the swelling of the median nerve for a mid-to-long-term effect. 29,30 Shock-wave therapy could also be conducive to improved symptoms and increased hand function for patients with CTS; however, further research is needed to confirm the long-term effects and the optimal shock-wave therapy protocol for CTS. 31,32 Oral steroids and corticosteroid injections have also been shown to benefit patients with CTS, particularly in the short term; the benefits of oral pain medication and corticosteroid injections were not maintained in the long term. 33
In terms of pain relief and functional improvement, the effects of shock-wave therapy and local corticosteroid injection are not significantly different; however, shock-wave therapy is a noninvasive treatment with fewer complications and greater patient safety. 34 There is insufficient evidence to support increased benefit of one type of therapeutic ultrasound regimen over another or to support the use of therapeutic ultrasound as a treatment with greater efficacy compared with other nonsurgical interventions for CTS, such as splinting, exercises, and oral drugs 28 ; however, ultrasound-guided corticosteroid injection yields the most favorable results for reducing symptom severity, and improving functional status 2 in patients with CTS, showing more effectiveness than landmark-guided injection in symptom severity improvement. However, no significant differences were observed in functional status improvements between the two methods. 35
The meta-analysis in this study showed no significant heterogeneity between groups and no significant publication bias. One limitation of this meta-analysis is that although the authors systematically searched the relevant database, the sample sizes were relatively small. In addition, some tests had a high risk of bias, and the observation indexes were limited to symptoms and function without focus on physical function or nerve conduction. Meanwhile, given that the number of sessions and the total duration of treatment differed between the studies, the authors could not obtain evidence of the short-, medium-, and long-term effects of manual therapy and related interventions, most importantly, the interventions used in the control group were inconsistent, which may have led to heterogeneity in the results of the analyses.
Conclusion
The results of this meta-analysis suggested that manual therapy and related interventions were better than control groups in treating CTS. Manual therapy and related interventions could relieve the symptoms of patients with CTS and promote the recovery of hand function. Manual therapy and related interventions should be considered clinically effective methods for treating CTS. In the future, more high-quality randomized controlled trials will be necessary to verify the effectiveness of manual therapy and related interventions on CTS patients with different severities, as well as their short-, medium-, and long-term effects on CTS patients.
Footnotes
Acknowledgments
The authors would like to thank the researchers and study participants for their contributions.
Authors' Contributions
J.H.D., Q.Y., X.Y.W., and J.H.Q. were responsible for acquisition, interpretation, and drafting the article. J.A., Q.D., and X.Y.Y. extracted the data. B.J.X., H.Z.W., and J.L. substantially contributed to the data analysis and critically revised the study for important intellectual content. All authors provided final approval of the version to be published and agree to be accountable for all aspects of the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was supported by the Academic Viewpoints, Unique Diagnostic and Treatment Methods, and Major Diseases Prevention and Treatment Experience of Illustrious Senior Traditional Chinese Medicine Practitioners in Western China [No. 2018YFC1704104]; and Sichuan Administration of Traditional Chinese Medicine [No. 2021MS075], with no commercial entity involved. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the article.