
Abstract
Objective:
Both the United Nations and the World Health Organization have identified antimicrobial resistance as a significant threat to global health. The Centers for Disease Control and Prevention identified five pediatric respiratory conditions as requiring particular scrutiny in terms of antibiotic stewardship. This study sought to identify strategies used by experienced naturopathic practitioners to treat acute respiratory infections in children. The authors theorize that naturopathic strategies safely fill the gap between watchful waiting and antibiotic prescription, thus reducing the use of antibiotics.
Methods:
Naturopathic practitioners in Canada, the United States, and Australia with a minimum of 5 years of experience in clinical naturopathic care of children were recruited for a modified Delphi study. A 14-person panel of practitioners was selected to complete a series of four iterative surveys assessing agreement to statements in five domains of knowledge/attitudes, assessment/diagnosis, management, monitoring, and education. Items were deemed to have reached consensus if they reached a predetermined threshold of 70% agreement, or failed to reach a threshold of 40% agreement. Items between these boundaries were modified and retested until either consensus was reached or the four surveys had been completed.
Results:
Results yielded a large degree of agreement on core naturopathic approaches to the management of acute pediatric respiratory infections, especially lifestyle strategies, including adequate rest and dietary recommendations. The use of vitamins C and D was strongly supported, as were herbs, particularly echinacea and elderberry. Some hydrotherapy and topical applications specific to the individual focus on infection also reached consensus. Results suggested that most respondents, even if they have the authority to prescribe antibiotics, rarely deem it necessary to do so.
Conclusion:
Findings of this study provide (1) clarity on the role of naturopathic doctors in the management of pediatric health concerns and the stewardship of antibiotics; and (2) initial guidance to less experienced naturopathic practitioners. The findings also identify key priorities for research into the safety and effectiveness of naturopathic interventions to reduce the unnecessary prescribing of antibiotics.
Introduction
Both the United Nations 1 and the World Health Organization 2 have identified antimicrobial resistance as a threat to global health. 3 Judicious use of antibiotics in pediatric practice is particularly warranted. 4,5 The Centers for Disease Control and Prevention (CDC) has identified five acute pediatric respiratory infections (APRIs) requiring scrutiny. 6 Practice guidelines for these conditions suggest preserving antibiotic use only with clear indications of bacterial infection, 7 although these guidelines have limitations. 8 Clinicians must manage the risk of antimicrobial resistance with pressures of diagnostic uncertainty, time constraints, and patient expectations, 9 and may prescribe antibiotics when not indicated. 10 –12
The naturopathic profession has a key role to play in antibiotic stewardship. The principles, training, and practice of naturopathic medicine have been described, 13 and Porcino et al demonstrated how naturopathic doctors (NDs) approach the management of pediatric illnesses in general. 14 The objective of this study was to identify strategies used by naturopathic practitioners in the management of the five conditions prioritized by the CDC. The authors hypothesize that NDs are engaging in the space between watchful waiting and appropriate prescribing of antibiotics. They anticipate that NDs employ a variety of strategies to alleviate symptoms, support the immune system, and target infectious agents. They theorize that the results will identify opportunities for investigation of the safety and effectiveness of these approaches to improve antibiotic stewardship.
Methods
Design
A modified Delphi process, drawing upon a panel of experts in the field. 15
Participants
Participants were recruited between October and December 2019 through e-mail through professional associations in Australia, Canada, and the United States. Members were invited to nominate themselves or a colleague. Nominees receiving two or more nominations were invited to complete a demographic form. Inclusion criteria included the following: Graduate of an accredited naturopathic medical institution in North America OR a naturopath who is a member of a professional association that is a full or associate member of the World Naturopathic Federation. Received a minimum of 2 nominations, one of which could have been a self-nomination. Has a minimum of 5 years of recent experience in: an active pediatric-focused practice that provides direct care to the pediatric population and treats children who are suffering from respiratory tract infections OR research regarding the pediatric population and has performed scholarship related to the management of pediatric respiratory infections OR providing education regarding the management of children with respiratory tract infections, as a faculty member in a medical educational institution. Fluent in written English.
The authors sought 10–20 participants based on the recommendation of Turoff. 16,17 They used a deidentified process to create a panel that reflected diverse scopes of practice, training, and geographical contexts, and generated a wait-list of eligible participants should numbers fall below 12 in any given round.
Data collection and analysis
The process occurred over four rounds (see Delphi flow diagram in Fig. 1).

Flow diagram of the modified Delphi method.
The research team brainstormed questions to address the study objective, which were grouped into domains of knowledge and attitudes, diagnosis and assessment, management, monitoring, and education. The first survey contained open-ended questions and Likert-scale items. A convenience sample of five NDs and four senior naturopathic medical students piloted the questionnaire, reflecting on the feasibility, relevance, and comprehensiveness, which yielded minimal changes (Supplementary Appendix SA).
Consensus in rounds 1 and 2 was defined as greater than 70% of respondents or fewer than 40% of respondents choosing “agree” or “strongly agree.” These items were moved to the next survey. Open responses from survey 1 were coded and framed in survey 2 as Likert scales (as above) or dichotomous options (yes/no). Dichotomous items selected by more than 70% of participants or fewer than 40% were deemed to have reached consensus. Each domain included an invitation for feedback on items. Items that did not meet consensus or received sufficient commentary to warrant rephrasing were forwarded onto the subsequent round.
Items in rounds 3 and 4 asked participants to rate agreement on a 0–100 rating scale. Items with a mean of 70% or greater were deemed to have reached consensus. Items failing to reach at least a mean of 40% were excluded. Items in round 3 with a mean between 41% and 69%, or which received compelling comments from participants, were tested again in the final round. Items in round 4 that remained stable with a nonconsensus average between 41% and 69% were deemed to have not reached consensus.
Consent and ethics review
Initial consent forms were received between December 2019 and January 2020. Survey 1 was distributed in February 2020. When the COVID-19 pandemic commenced in March 2020, the original panelists were asked to reconfirm consent. The second survey was disseminated in May 2020, the third in November 2020, and the fourth in February 2021. Participants received two reminder e-mails, 2 weeks apart, to complete each survey administered using Research Electronic Data Capture (REDCap). The study was approved by the Research Ethics Board at the Canadian College of Naturopathic Medicine (CCNMREB026.Solomonian).
Results
Demographics
The panel consisted of 14 participants (Table 1). The average duration of practice was 14.6 years (range: 6–35 years). All were in clinical practice, with two engaged in medical teaching and one in research. None worked with medical doctors or registered nurses. Five participants lacked legal authority to prescribe pharmaceutical antibiotics. All other panelists practiced in jurisdictions in which NDs have the legal authority to do so.
Demographics of Panelists
Training Institutions: ACNT, Australasian College of Natural Therapies (Torrens University Australia); Bastyr, Bastyr University; Bridgeport, University of Bridgeport (no longer offered); CCNM, Canadian College of Naturopathic Medicine; NUHS, National University of Health Sciences; NUNM, National University of Natural Medicine; QINS, Queensland Institute of Natural Science; SCNM, Southwest College of Naturopathic Medicine; SSNT, Southern School of Natural Therapies (Torrens University Australia).
Professional Associations: AANP, American Association of Naturopathic Physicians; ANTA, Australian Natural Therapies Association; ATMS, Australian Traditional Medicine Society; BCNA, British Columbia Association of Naturopathic Doctors; CALND, California Naturopathic Doctors Association; CAND, Canadian Association of Naturopathic Doctors; CMA, Complementary Medicine Australia; ILANP, Illinois Association of Naturopathic Physicians; MANP, Montana Association of Naturopathic Physicians; MNDA, Maryland Naturopathic Doctors Association; NAPCP, Naturopathic Academy of Primary Care Physicians; NHAND, New Hampshire Association of Naturopathic Doctors; OAND, Ontario Association of Naturopathic Doctors; OANP, Oregon Association of Naturopathic Physicians; PedANP, Pediatric Association of Naturopathic Physicians.
CAM, complementary and alternative medicine; DC, District of Columbia; N, no; NSW, New South Wales; WA, Washington; Y, yes.
Attitudes and knowledge
Table 2 illustrates the final consensus for items related to attitudes and knowledge; full results can be found in Supplementary Appendix SB. There was early consensus on most items related to prioritizing a nonpharmaceutical approach, as well as the attitude that children should be treated with antibiotics when appropriate. There was agreement that naturopathic interventions can enhance the effectiveness of antibiotics and reduce adverse effects, and that early naturopathic intervention is adequate to effectively manage APRIs. There was good agreement with an evidence-based approach to the management of APRIs.
Final Status of Favorable Consensus for Domain of Attitudes/Knowledge
APRIs, acute pediatric respiratory infections; TCM, Traditional Chinese Medicine.
Diagnosis and assessment
Consensus was reached for the majority of items in round 2 regarding general assessment techniques for the diagnosis of APRIs (Table 3; full results can be found in Supplementary Appendix SB). Wording of some items was modified, and more specific techniques were included in round 3. Few of the new or modified items reached consensus by round 4. It was agreed that body temperature, general appearance, behavior, ear/nose/throat examination, discharge quality, and lymph node palpation were useful to assess for all five conditions.
Items That Reached Favorable Consensus Regarding the Domains of Assessment and Management of Acute Pediatric Respiratory Infections; Ranked for Each Condition
Participants were asked about indications of a bacterial infection. Consensus was reached on each item related to rhinosinusitis, pharyngitis, and bronchi/bronchiolitis by round 3. Only tympanic membrane rupture (for otitis media) and age (for pneumonia) failed to reach consensus by round 4. “Toxic systemic appearance (lethargy, poor perfusion, marked hypo/hyperventilation, and cyanosis)” reached consensus in round 3 for all conditions but pneumonia, which was excluded in error.
Interventions
“Rest” was universally recommended for all conditions and reached consensus after only one round. The majority of diet and lifestyle items reached consensus in round 2. Favorable consensus was reached for vitamins C and D for all APRIs (Table 3; full results in Supplementary Appendix SA).
The herb that reached the strongest consensus (71.43%–92.86%) was elderberry (Sambucus nigra). Echinacea (Echinacea sp.) reached over 71% agreement for use in rhinosinusitis, pharyngitis, and bronchiolitis. More than 70% of participants agreed that “warming socks” were useful for the treatment of otitis media, rhinosinusitis, and pharyngitis. Of the energetic options, only individualized homeopathy reached favorable agreement for all conditions.
“Herbal ear drops” and “garlic-mullein ear oil” were recommended by over 92% of participants for otitis media. “Salt water gargle” reached consensus for both rhinosinusitis and pharyngitis, and “chest compress or rub” reached agreement for both bronchiolitis and pneumonia. Over 75% of participants agreed that the Eustachian tube manipulation was beneficial for the treatment of otitis media, but no other manual intervention was agreed upon.
Monitoring
There was >92% agreement after round 2 that follow-up was recommended if symptoms worsened or failed to improve, but no consensus was reached regarding the time frame. After round 3, there was 90.6% agreement that the time line for requested follow-up depended on the severity of the condition. After four rounds, no consensus was reached on the timeliness or frequency of follow-up, and whether follow-up is best initiated by the practitioner or the guardian (Table 4; full results are in Supplementary Appendix SB).
Final Status of Consensus on Domain of Monitoring in Response to the Question, “When Do You Usually Request a Follow-Up Visit After the First Consultation for Acute Pediatric Respiratory Infection?”
APRI, acute pediatric respiratory infection.
Education
Participants were asked about the extent to which 14 different education strategies would help develop competence in the management of APRIs (summary in Table 5; full results in Supplementary Appendix SA). Agreement was reached on all 5 strategies targeting undergraduate naturopathic medical trainees, and 3 of the 5 aimed at practitioners.
Final Status of Favorable Consensus on Education Strategies in Response to the Questions, “How Important Are the Following Strategies for Developing Competence in the Management of Acute Pediatric Respiratory Infections for (A) Undergraduate Naturopathic Medical Education and (B) Continuing Naturopathic Medical Education?”
N/A, not applicable; ND, naturopathic doctor.
Discussion
The results of this study suggest that experienced naturopathic practitioners rarely prescribe or refer for antibiotics, and manage APRIs using an array of approaches. Health care providers may prescribe antibiotics when they are not indicated (Fig. 2). Naturopathic intervention may be useful in terms of bridging the gap between watchful waiting and antibiotic prescription (Fig. 3). As noted in panelists' responses, these approaches are utilized simultaneously with antibiotics when they are indicated.
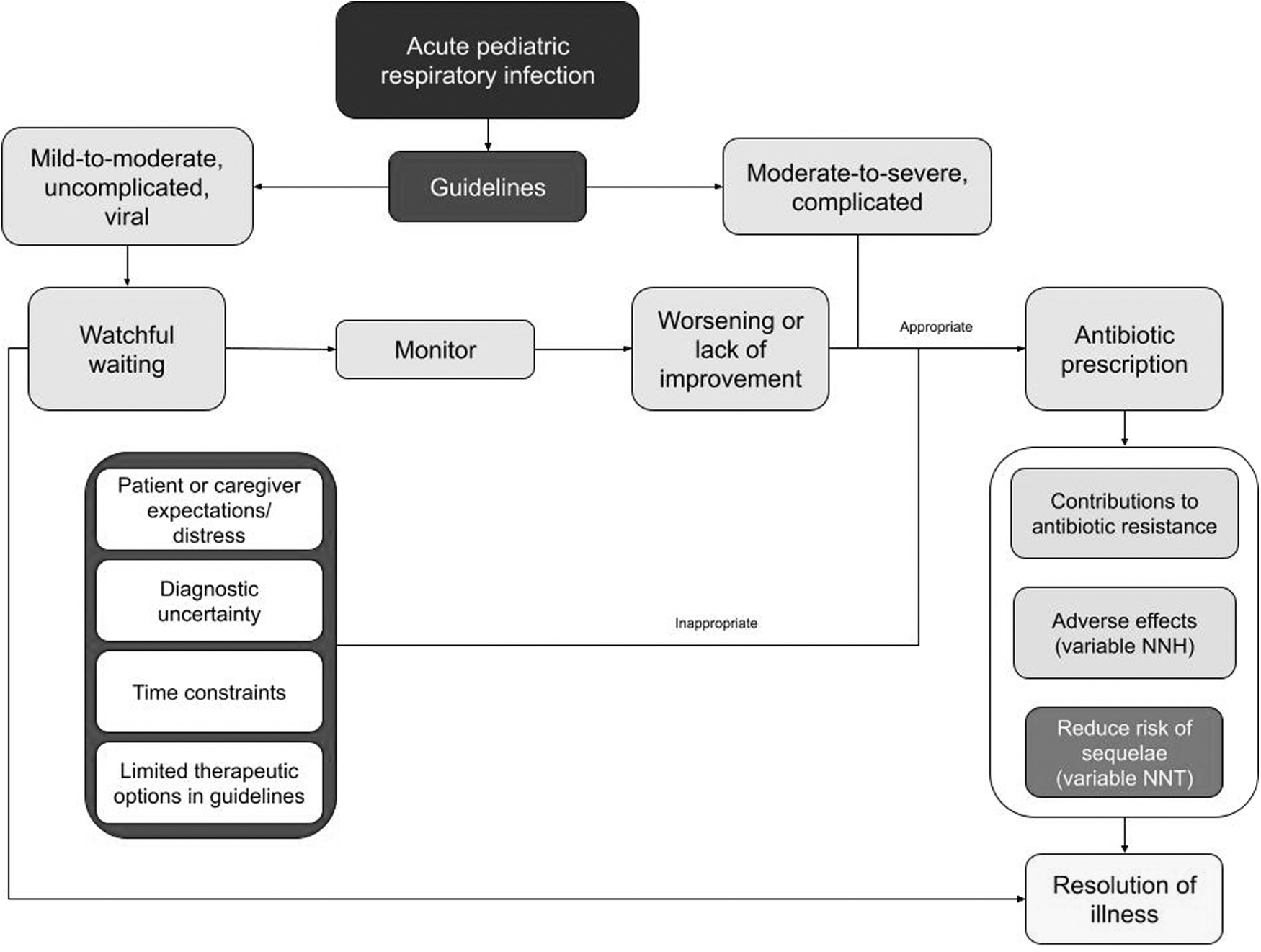
Conceptual framework for conventional biomedical approach to APRI management, with influences on and consequences from inappropriate prescribing of antibiotics. APRI, acute pediatric respiratory infection; NNH, number needed to harm; NNT, number needed to treat.

Conceptual framework for an integration of naturopathic with biomedical management of APRIs. APRI, acute pediatric respiratory infection; NNH, number needed to harm; NNT, number needed to treat.
There was little consensus on the use of patient/family preference, practice guidelines, clinical resource tools, or government and public health websites/documents to guide clinical decision-making. This suggests that participants may not be embracing all elements of the evidence-based practice (EBP) framework, 18 at least within the context of managing APRIs. The inconsistent use of evidence may be explained by barriers impacting EBP uptake in naturopathic medicine, such as the lack of sufficient evidence for some interventions, and insufficient EBP skills. 19 The apparent lack of consideration of patient preference, however, seems to misalign with the patient-centered approach characteristic of naturopathic practice. 20 It is possible that this may reflect a tension between EBP and naturopathic philosophy, with a number of respondents commenting that antibiotics should be appropriately recommended or not independent of patient preference. This warrants further investigation to better understand the nuances of naturopathic clinical decision-making.
Nonspecific diagnostic techniques, such as behavior, appearance, or body temperature, reached consensus for all conditions. Procedures more specific to certain APRIs were more likely to reach consensus where clinically relevant. There was a stronger consensus for diagnostic strategies aligned with biomedical assessment as opposed to techniques from other paradigms, such as spinal assessment, tongue and pulse evaluation, or electrodermal testing. There seemed to be a trend away from laboratory testing or imaging. This may be skewed by respondents who do not have access to or training in these procedures (i.e., in Australia). Since panelists were not surveyed about the degree to which they adhere to specific aspects of diagnostic guidelines, results could not be compared directly with these (e.g., from the American Association of Pediatrics, 21 or Institute for Clinical Symptom Improvement 22 ).
Due to the iterative process of the Delphi method, details of individual techniques were not adequately interrogated when consensus was reached for broad categories. For example, “ENT examination” reached consensus without this granulation, whereas guidelines are more specific about evaluation of the tympanic membrane, middle ear space, tonsils, pharyngeal exudate, or rhinorrhea. As was pointed out by one participant, “many of [these indicators] are case-specific.” NDs are trained to approach scenarios holistically, and most indicators of infection have a low likelihood ratio on their own. Despite not knowing the details of how participants select or interpret these examination findings, it is important to reinforce the use of evidence-based clinical guidelines in naturopathic training and continuing education to ensure NDs are using evidence-informed processes.
The results from this study reveal an array of interventions used by NDs, which appear to align with three main goals: alleviation of symptoms, supporting immune system function, and providing antimicrobial action.
Safe alleviation of symptoms may reduce the tendency to consider unnecessary antibiotics. Alleviating suffering also reduces distress in the child, allowing a more conducive state for rest and recovery. One example of this that emerged is the application of herbally infused oil to the external auditory canal to alleviate the pain of otitis media. The most recent systematic review of this approach concluded that it does appear to be helpful in alleviating pain, although there was insufficient evidence to determine the degree of effectiveness. 23 The review noted that this approach was well-tolerated by the children, suggesting that ear oil “offers an effective and accessible treatment option for children with AOM.” Nasal saline irrigation also reached consensus for rhinosinusitis and bronchial/bronchitis, an approach that dilutes and helps excrete mucus, theoretically alleviating discomfort from congestion.
A systematic review concluded that this approach improves symptoms and quality of life in children with acute rhinosinusitis, although, similar to the review of ear oil, no conclusions could be drawn about the degree of effectiveness. 24 Steam inhalation reached consensus for the same two conditions. Steam inhalations raise the possibility of safety concerns, 25 although despite the lack of consistent/conclusive evidence, this strategy may still be recommended in conventional pediatric practice. 26
A core principle of naturopathic medicine is to support the natural healing mechanism of the body. NDs are taught to provide education about the body's capacity to heal, the signs and symptoms of this effort (such as fever and lethargy), 27 and to encourage this process (when safe to do so) rather than suppress. When children and families understand their symptoms, and are offered options to support coping, it may promote resilience both immunologically, and psychologically. 28 Rest reached 100% agreement for all APRIs, which is supported by clinical practice guidelines. This contrasts with marketing for medications to get children “back to normal.” The countries where panelists practice are cultures in which productivity is encouraged, even in childhood. 29,30 Deprioritization of rest leads to allostatic burden, which impairs immune system function. 31
Other lifestyle strategies on which panelists agreed included emphasizing nutrient-dense foods, avoiding high glycemic index foods (which can impair immune system function), 32 and limiting dairy (which can aggravate the accumulation of respiratory tract mucus in some individuals). 33
Supplementation of vitamin D reached a strong consensus, for which there is evidence for reducing acute respiratory infections and overreliance on antibiotics. 34 Dosing vitamin D to serum adequacy rather than just supplementing a standard amount may have a more significant impact on immune function. 35,36 Supplementation of vitamin C also reached consensus. Despite the known biochemical role that vitamin C has in immune system function, 37 there is inconsistent evidence of the impact of supplementation on the prevention and treatment of respiratory infections, particularly in the pediatric population. Two separate Cochrane reviews concluded that given the low cost and safety of vitamin C, and its plausibility, there is minimal harm in using it. 38,39
“Warming socks” reached consensus for three of the infections. This approach consists of the application of a cold, wet compress to the feet, covered by an insulating layer. This induces vasodilation of the lower limb capillary beds, which supports the upregulation of cardiac output seen in the acute-phase response to infection. This physiologic response promotes circulation of leukocytes, and elimination of inflammatory debris. Although there is no peer-reviewed investigation of the effectiveness of this approach, the strength of the consensus suggests that practitioners and families find it feasible and anecdotally helpful. This approach too has a low cost and low risk of adverse effects.
Although the efficacy of homeopathy is not well-supported beyond placebo in the peer-reviewed literature, 40 individualized homeopathic treatment reached consensus for all five conditions, suggesting that panelists find it safe and effective. Given the self-limiting nature of most APRIs, homeopathic treatment may act as a placebo for parental anxiety. It is also very possible that homeopathy is effective but difficult to evaluate using conventionally accepted methods. In the context of an uncomplicated APRI, given its low cost and acceptability to children, 41 negligible direct harm, 42 and the person-centered approach, 43,44 the benefit of a homeopathic recommendation may outweigh the risk. This may be especially true if the alternative is a nonindicated antibiotic, which carries greater financial cost and health-related risk, or another natural intervention with greater financial or feasibility-related costs.
Many herbs have broad-spectrum actions against an array of viruses and bacteria. 45 Some also have demonstrated immunostimulant effects that may enhance their value for the management of infections. Elderberry (Sambucus nigra fructus) and echinacea (Echinacea spp.) reached consensus for multiple conditions in this study. Both these herbs have been shown to be safe and effective for the management of upper respiratory tract infections across multiple studies, 46 –49 although this conclusion is not universal. 50 A 2021 systematic review demonstrated that elderberry may reduce the duration and severity of viral respiratory illnesses. 51 Ogal et al demonstrated that echinacea prevented pediatric ARTI, thereby reducing antibiotic usage. 49
Some interventions that did not reach consensus, but had strong support, have traditional evidence for their use. Higher quality evidence supports the use of licorice (Glycyrrhiza glabra) to alleviate symptoms of viral respiratory infections. 52,53 Both marshmallow (Althaea officinalis) 54,55 and mullein (Verbascum thapsus) 56,57 are traditionally used for respiratory infections, with in vitro evidence suggesting biochemical mechanisms of action. Conversely, some herbs, which have been shown to be effective and safe in the scientific literature, did not emerge in this study; this is discussed below.
It appears as though the panelists were utilizing all three mechanisms (alleviating symptoms, supporting the body's natural capacity to heal, and directly targeting the infectious agent). It seems logical to imagine this is deliberate, given the emphasis on holistic, individualized care within the naturopathic paradigm. 13 The fact that a number of interventions did not reach consensus also suggests an individualized approach as opposed to a standardized one, a philosophy demonstrated by Lucas et al. 58 It appears as though practitioners adjust their recommendations to both the patient and the condition, as was also demonstrated by Porcino et al. 59
Viral respiratory infections are generally self-limiting in otherwise healthy children. It is difficult to know for sure to what degree the interventions used by naturopathic practitioners are directly effective. However, the strategies that reached consensus in this study tended to be cost effective, low risk, and plausible mechanistically. When comparing this risk profile to that of an antibiotic being used as a placebo, the value seems clear. The reassurance and education inherent in naturopathic practice likely provide value as well, empowering caregivers to actively engage in the well-being of their child, and reducing worry. 60
Monitoring progression of illness is critical. There was agreement among participants that they would recommend a follow-up visit if symptoms worsened or did not resolve. However, there was less consensus among participants regarding the timing and initiation of follow-up visits. This finding may reflect the variability of symptoms and conditions that are captured under the umbrella of APRI, 60 and the need to review each patient individually.
Participants appeared to support a multimodal approach to education of practitioners and trainees. There was considerable support for strategies that were pediatric specific, clinically applied, fostered mentorship, and facilitated clinical decision-making. The support for these strategies aligns with observations in other disciplines, which have shown mentorship, earlier clinical experiences, and improvements in the teaching-practice nexus to be useful in developing clinical competencies. 61
Because a Delphi approach is not a cross-sectional analysis of all practitioners, it does not allow assessment of what most NDs do in practice; it does, however, allow for an approach to collating expert perspectives, which may inform directions for practice guidelines, education, and research. It is unclear if the Delphi method promotes or mitigates the risk of groupthink. 15 In this modified approach, the asynchronous, deidentified, and aggregate results may have encouraged honesty. This study's strengths included its multiple rounds of quantifiable consensus-seeking. The validity of these results was limited by minor attrition, which was likely exacerbated due to the COVID-19 pandemic. The study design deliberately allowed for participants to guide the creation of the survey items. If the survey had been set up so that only guideline-based options were queried, it may have yielded results that could have been more easily compared with these.
Respondents were not asked about the outcome, and this study was not designed to assess the safety or effectiveness of the approaches used; nor is it within the scope of this study to systematically map results to the body of literature. It is possible that there are occasions in which APRIs are not effectively resolved using naturopathic approaches, and certainly when they are likely to resolve successfully without any intervention at all. This former possibility is a critical one to interrogate. As discussed, there is existing evidence for the safety and effectiveness for many of the strategies that reached consensus. It remains important, however, that practitioners critically evaluate their recommendations to ensure they are sound, and not simply reinforcing a confirmation bias. Regular review of emerging evidence for natural approaches to APRI is an important practice for reflective practitioners, and the skills of lifelong learning should be emphasized through educational strategies.
Some approaches that have been evaluated in the literature as safe and effective for the management of APRIs did not emerge in this study. For example, the review by Anheyer et al identified moderate positive evidence for Pelargonium sidoides (South African geranium), 50 and a 2021 trial affirmed its effectiveness in reducing symptom burden in children with upper respiratory tract infections. 62 A 2020 rapid review demonstrated the safety and effectiveness of common ivy (Hedera helix) in the management of viral respiratory infections (including reduced use of pharmaceutical antibiotics) in adults and children. 63 Neither of these herbal medicines were mentioned by study participants.
Indeed, the vast herbal pharmacopeia utilized in traditional medical paradigms around the world has much to offer the management of APRIs, reduce the global burden of antibiotic resistance, and respond to novel infectious agents such as COVID-19. Some of these substances have been subjected to the rigorous evaluation of controlled trials and systematic reviews, such as the 2022 study demonstrating the usefulness of Qinxiang Qingjie, a Chinese herbal formulation, in the management of pediatric influenza compared with a pharmaceutical antiviral medication. 64 Many herbs used in traditional practices globally have not been evaluated using conventional methods, resulting in “insufficient scientific evidence” for endorsed use. 65 In fact, there are multiple systemic barriers to the evaluation and integration of these traditional approaches into health care systems, including the tendency to reduce herbal medicines to their isolated constituents rather than use them in their whole form. 66
A 2020 commentary on the potential role of wormwood (Artemisia spp.) in the management of COVID-19 based on its traditional Chinese use argues that, “the specific pharmacologically active components need to be isolated, verified through proper pharmacological evaluation, and then possibly optimized through modern (hemi) synthesis strategies before being developed according to rigorous international guidelines for drug development.” 66 Traditional use of most herbs, however, is in their whole form (e.g., root, leave, flower) as opposed to a pharmacological reduction to isolated components. Part of the value of herbal medicine is the synergy between active constituents, 67 which makes rigorous evaluation and standardization difficult, including for wormwood. 68 It behooves clinicians to apply an evidence-informed approach to patient care, which includes accessing, interpreting, and integrating the best available evidence. There are many types of evidence besides the conventionally accepted hierarchy. 69
Given the multimodal and individualized approach typical of naturopathic practice, 70 future investigations would be wise to use a whole-systems methodology to assess the safety and effectiveness of a naturopathic approach to APRIs. 71 Existing systematic reviews of nonpharmaceutical approaches to these conditions (such as those by Wopker et al 72 and Lucas et al 73 ) offer a useful jumping off point for individualized application.
Relevance and future directions
This study could be significant for the purposes of:
clarity on the role of NDs in the management of pediatric health concerns and the stewardship of antibiotics;
initial guidance to less experienced naturopathic practitioners, and
informing research designs to generate evidence for the safety and effectiveness of naturopathic intervention to reduce the use of unnecessary antibiotics in the management of APRIs.
Future studies should assess the degree to which naturopathic approaches are safe and effective. Because a quantitative survey is limited in its ability to assess the holistic and multimodal approach typical of naturopathic care, other study designs may better capture behaviors and identify gaps in clinical practice. These may need to be geographic-specific to accurately represent licensure and scope of practice parameters. A whole-systems methodology may reveal useful data as to the effectiveness of naturopathic management of these conditions.
Conclusions
This Delphi study reveals strategies used by naturopathic practitioners that may support antimicrobial stewardship in the management of APRIs. The emphasis on the lifestyle and individualization of care underscores the patient-centered paradigm of naturopathic practice. These strategies warrant further investigation to determine the safety and effectiveness, using appropriate methodologies. Institutions that train naturopathic students should ensure that graduates are competent at assessing APRIs using evidence-informed strategies to appropriately prescribe or refer for pharmaceutical antibiotics when necessary.
Footnotes
Acknowledgments
The authors thank Gina Brown for her contributions to the background work. They also thank the panelists of this study who so generously gave of their time and experience. The authors extend their gratitude to the various professional associations that helped to disseminate the call for participation, and to the Pediatric Association of Naturopathic Physicians for the coverage of the article-processing fees.
Authors' Contributions
L.S. collaborated in the conceptualization and design of the study and data collection instruments, coordinated the data collection, carried out the analyses, contributed to drafting the initial article, and reviewed and revised the article. A.P. collaborated in the conceptualization and design of the study and data collection instruments, participated in the data collection, carried out the analyses, contributed to drafting the initial article, and reviewed and revised the article. J.B., L.G., M.L., and S.L. collaborated in the conceptualization and design of the study and data collection instruments, carried out the analyses, contributed to drafting the initial article, and reviewed and revised the article. A.G. contributed to the design of data collection instruments, carried out analyses, contributed to drafting the initial article, and reviewed and revised the article. M.W. participated in data analysis, contributed to drafting the initial article, and reviewed and revised the article.
All authors approved the final article as submitted and agree to be accountable for all aspects of the work.
Author Disclosure Statement
Other than being actively engaged in the practice, teaching, and research of naturopathic care, the authors have no conflicts of interest relevant to this article to disclose.
Funding Information
No specific grants or funding was provided for the support of this study, other than in-kind support from the authors' affiliated institutions.
Supplementary Material
Supplementary Appendix SA
Supplementary Appendix SB
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.