
Abstract
Introduction:
In recent years, it has been reported that acupuncture is useful for alleviating the symptoms of patients with hematological malignancies, but the safety of acupuncture for such patients has not been established. This study evaluated the risk of bleeding from acupuncture in patients with hematological malignancies accompanying thrombocytopenia.
Methods:
The authors performed a retrospective investigation of the medical records of patients with hematological malignancies who received acupuncture during hospitalization at the hematology department of a single medical center in Japan. The bleeding risk at the acupuncture site was evaluated in the following four groups according to the platelet count measured on the day of acupuncture treatment: (1) <20 × 103/μL, (2) 20–49 × 103/μL, (3) 50–99 × 103/μL, and (4) 100 × 103/μL or more. Occurrence of grade 2 or higher bleeding according to the Common Terminology Criteria for Adverse Events, version 5.0, within 24 h from the acupuncture session or before the next session was defined as an event, and the risk of occurrence of bleeding was examined in each group.
Results:
Of 2423 acupuncture sessions conducted on 51 patients with hematological malignancies, 815 were included in the analysis. Ninety sessions were performed in the <20 × 103/μL platelet count group, 161 in the 20–49 × 103/μL group, 133 in the 50–99 × 103/μL group, and 431 in the 100 × 103/μL or more group. No bleeding event according to the authors' definition occurred in any of these groups.
Conclusions:
This study is the largest to date to assess the bleeding risk of acupuncture in patients with hematological malignancies accompanying thrombocytopenia. The authors considered that acupuncture could be safely performed without causing serious bleeding for patients with hematological malignancies accompanying thrombocytopenia.
Introduction
Patients with hematological malignancies such as leukemia and malignant lymphoma experience symptom burden equal to or greater than that of patients with metastatic solid tumors, and the majority of such patients have unsatisfied physical and psychological needs in their daily lives. 1 –3 Reflecting these, the use of complementary and alternative medicine is widespread among patients with hematological malignancies, and the percentages of patients using some form of complementary and alternative medicine are 42%–70% in Asia, 4,5 16%–44% in Europe, 6 –9 and 61%–89% in the United States. 10,11 Acupuncture is used globally as complementary and alternative medicine that involves insertion of fine needles into specific parts of the body.
In recent years, acupuncture has been reported to be effective for peripheral neuropathy during chemotherapy and for nausea, loss of appetite, and excessive analgesic use during hematopoietic stem cell transplantation. 12 –14 In response to these reports, the use of acupuncture is expected to increase in patients with hematological malignancies as palliative care; however, information on the safety of acupuncture for patients with hematological malignancies is insufficient.
Thrombocytopenia, defined as a decrease in platelet count, occurs frequently in patients with hematological malignancies due to the disease and its treatment. Guidelines on platelet transfusion recommend maintaining a certain platelet count before invasive procedures in patients with thrombocytopenia since such procedures can increase the risk of bleeding. 15 –18
A systematic review of acupuncture adverse events in the general population showed that the estimated risk of serious adverse events from acupuncture was very low at 7.98 per million treatments, and the most frequently observed adverse event was bleeding at the site where the acupuncture needle was inserted (estimated risk 4.92 per 100 acupuncture treatments). 19 There have been two reports so far regarding the bleeding risk of acupuncture in patients with thrombocytopenia.
Ladas et al. performed a retrospective examination of records of 237 acupuncture treatments performed on 32 pediatric patients (including 8 with hematological malignancies) under cancer treatment or stem cell transplantation. Of the 237 treatments, 112 were performed on patients whose platelet count was 100 × 103/μL or less. Of the 112 treatments, 48 were performed on patients with a platelet count of 20 × 103/μL or less. They reported that there were no adverse bleeding events. 20
In addition, Cybularz et al. 21 performed a retrospective investigation of the records of 2135 acupuncture treatments performed on 684 adult solid cancer patients and their platelet counts measured within 48 h of the treatment. Of the 2135 treatments, 98 were performed on patients whose platelet count was 100 × 103/μL or less. Of the 98 treatments, 9 were performed on patients with platelet count of 50 × 103/μL or less. They reported that there were no adverse bleeding events. 21
Since all of these previous reports were of a small number of acupuncture treatments for patients with thrombocytopenia and few patients with hematological malignancies were included, information on the safety of acupuncture in patients with hematological malignancies with thrombocytopenia is very limited.
Therefore, the purpose of this study was to evaluate the bleeding risk of acupuncture in patients with hematological malignancies accompanying thrombocytopenia.
Methods
Study design and patients
This study performed a retrospective review of the medical records of 51 patients with hematological malignancies who received acupuncture during hospitalization at the Department of Hematology, Aizu Medical Center, Fukushima Medical University, between May 2013 and August 2021. The groups were based on the platelet count measured on the day of the acupuncture session, and occurrence of bleeding events at the acupuncture site was assessed in each group.
This study was approved by the Institutional Review Board of Fukushima Medical University (number, 2021-324; approval date, April 19, 2022).
Grouping of thrombocytopenia patients at acupuncture treatment
The following four groups were based on the platelet count measured on the day of acupuncture treatment: (1) <20 × 103/μL, (2) 20–49 × 103/μL, (3) 50–99 × 103/μL, and (4) 100 × 103/μL or more.
The criteria for grouping were determined based on the following reasons: thrombocytopenia is generally defined as a platelet count of <100 × 103/μL or 150 × 103/μL, 22 all previous studies evaluating the bleeding risk of acupuncture in patients with thrombocytopenia used a cutoff of 100 × 103/μL, 19,20 and the American Society of Clinical Oncology and the American Society of Blood Banks recommend that the preoperative platelet count should be above 50 × 103/μL for highly invasive operations and 20 × 103/μL for less invasive operations. 15,16
To obtain accurate platelet counts for assessing the risk of bleeding, the authors excluded acupuncture sessions from the analysis when platelet count was not measured on the same day of acupuncture, when platelet transfusions were performed on the same day before acupuncture, when the time of either acupuncture or platelet transfusion was unknown, or when nonpenetrating acupuncture sessions (e.g., transcutaneous electrical acupoint stimulation) were performed.
Grouping was based on platelet count, not patient, and therefore individual patients could be included in multiple platelet count groups.
Evaluation of bleeding events
Data on bleeding and hematoma that occurred at the acupuncture site within 24 h immediately after each acupuncture session or by the next session were extracted from the medical records, and grade 2 or higher bleeding and hematoma according to the Common Terminology Criteria for Adverse Events (CTCAE), version 5.0, 23 were defined as bleeding events (Table 1).
Common Terminology Criteria for Adverse Events Grading for Bleeding Events
CTCAE, Common Terminology Criteria for Adverse Events.
The rationales for these outcome criteria were as follows: previous reports that evaluated the bleeding risk of acupuncture treatment had set the evaluation period from immediately after to 24 h after treatment 24 –26 ; the CTCAE are often used in the investigation of bleeding risk caused by invasive procedures, including acupuncture 26 –29 ; CTCAE grade 2 or higher bleeding can be extracted from medical records; and occurrence of bleeding that requires treatment can be a serious concern for acupuncture treatment as palliative care since it imposes an additional burden on the patient.
The procedure of acupuncture treatment
In each session, the style of acupuncture treatment, acupuncture points, and number of needles were determined at the discretion of the practitioner. Basically, the needle was inserted into the skin from the subcutaneous tissue to the depth of the muscle according to the patient's physique and then manually rotated for about 1 min. De qi was not always taken into account.
In many cases, electrical stimulation was then added through the inserted needles (electroacupuncture). Ohm Pulser LFP-4000A (Zen Iryoki Corporation, Fukuoka, Japan) was used for electrical stimulation, and the stimulation conditions were often set at a low frequency of about 2 Hz, an intensity at which the patient perceives stimuli without feeling pain, with a continuous wave for about 10 min. The needles used for acupuncture were mainly disposable stainless steel needles (Seirin Corporation, Shizuoka, Japan) with a diameter of 0.14–0.18 mm and length of 40–50 mm.
Each session lasted about 30 min, and basically 5–6 sessions per week were provided. All treatment sessions were conducted by 10 acupuncturists who were professionally qualified in Japan, with clinical experience ranging from 1 to 24 years.
Bleeding risk factors
In addition to patient characteristics such as age, gender, diagnosis, duration from diagnosis, and reasons for receiving acupuncture, the following possible bleeding risk factors for acupuncture (from previous reports on thrombocytopenia and other invasive procedures) were extracted from medical records for each treatment session: chemotherapy, coexistence of hypertension, fever (maximum body temperature 38.0°C or higher) on the day before acupuncture, oral administration of antifibrinolytic/antiplatelet/anticoagulant agents on the day before acupuncture, hemoglobin and serum creatinine levels from blood tests performed on the day of acupuncture, number of acupuncture needles used, electrical stimulation used, and years of experience of the practitioner. 30 –37
Statistical analyses
Statistical indicators (percentage, median, minimum value, maximum value, and interquartile range) were calculated for the overall study subjects and for each platelet count group. Bleeding risk factors were analyzed using the collected data only without imputation of missing values. If red blood cell transfusions were performed between the blood test and acupuncture or if the time of either blood cell transfusions or acupuncture was unknown, hemoglobin data were excluded from the analysis.
Bleeding risk was evaluated by counting the number of bleeding events of CTCAE grade 2 or higher in each platelet count group. If bleeding events were observed, the authors planned to calculate the risk difference and risk ratio of the three groups against the group with a platelet count of 100 × 103/μL or more, the statistical significance (p-value <0.05 in the two-sided test) by Fisher's exact test, and the multivariate-adjusted odds ratio and its 95% confidence interval using Firth's logistic regression model with bleeding risk factors as covariates. 38
All analyses were performed using STATA, version 16 (Stata Corp., College Station, TX).
Results
A total of 2423 acupuncture sessions were performed on 51 patients with hematological malignancies during the study period. Their ages ranged from 21 to 90 years and the male–female ratio was almost even. The most common diagnosis was non-Hodgkin lymphoma, followed by multiple myeloma, acute myeloid leukemia, and acute lymphocytic leukemia. The period from diagnosis ranged from 9 to 2886 days. Acupuncture was often given for musculoskeletal and tumor-induced pain and chemotherapy-induced numbness (Table 2).
Patient Characteristics
ALL/LBL, acute lymphoblastic leukemia/lymphoblastic lymphoma; AML, acute myeloid leukemia; HL, Hodgkin lymphoma; max, maximum; MDS, myelodysplastic syndromes; min, minimum; MPN, myeloproliferative neoplasm; NHL, non-Hodgkin lymphoma; PHN, postherpetic neuralgia.
Of the 2423 acupuncture sessions, 815 sessions for 51 patients were included in the analysis. These sessions were divided into four groups according to the platelet count (Fig. 1): 431 sessions for 38 patients were performed in the 100 × 103/μL or more platelet count group, 133 sessions for 28 patients in the 50–99 × 103/μL group, 161 sessions for 25 patients in the 20–49 × 103/μL group, and 90 sessions for 20 patients in the <20 × 103/μL group.
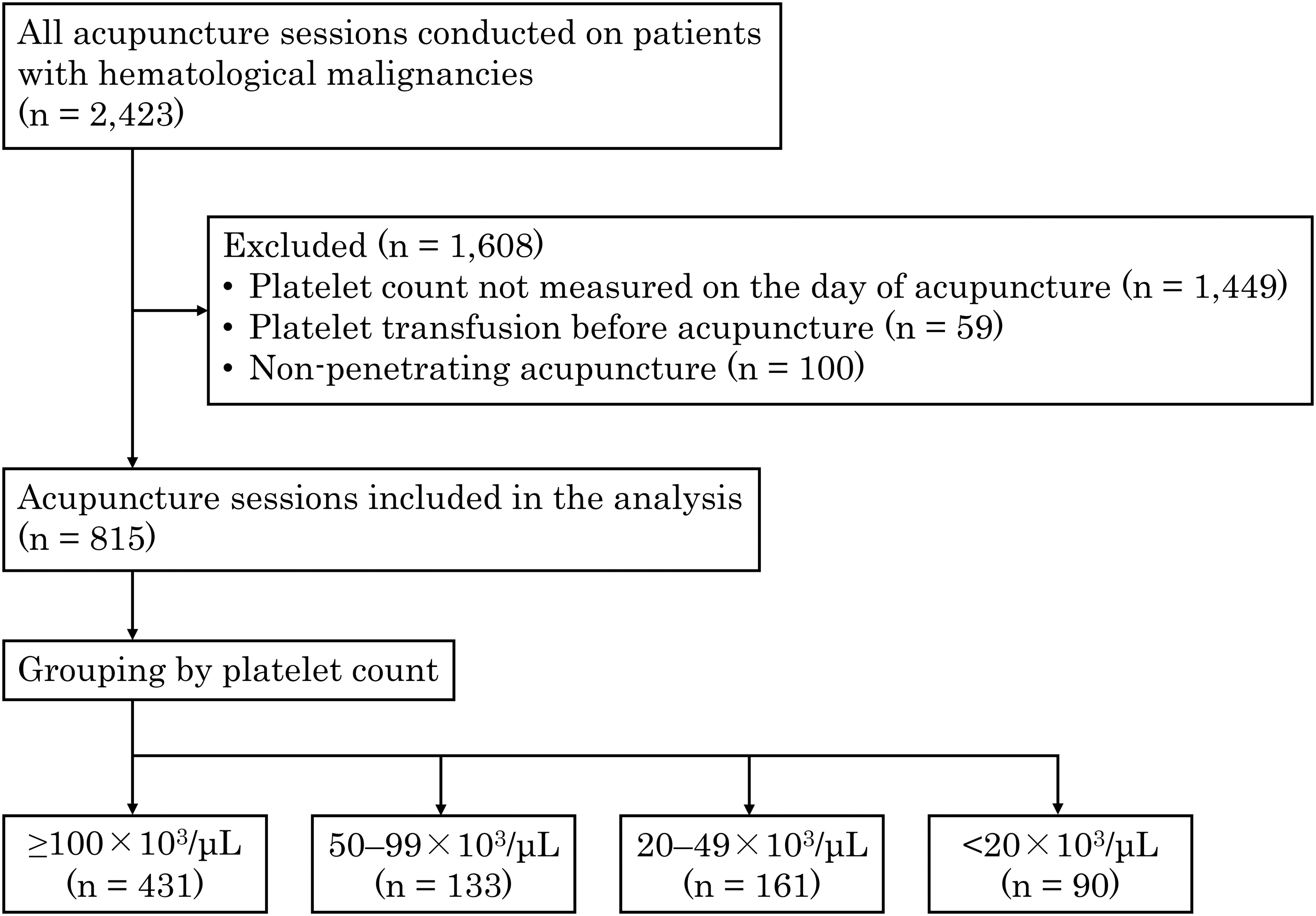
Flow chart of the study.
A summary of bleeding risk factors in each group is shown in Table 3. The groups of severer thrombocytopenia with platelet count <20 × 103/μL and 20–49 × 103/μL tended to have a higher rate of acute leukemia, lower rate of being under chemotherapy or oral anticoagulant agents, lower hemoglobin levels, and higher serum creatinine levels. As for the acupuncture methods, the frequency of electroacupuncture use and the number of acupuncture needles used were similar among the four groups.
Risk Factors By Platelet Count Group
Number of patients included were 38 in the 100 × 103/μL or more platelet count group, 28 in the 50–99 × 103/μL group, 25 in the 20–49 × 103/μL group, and 20 in the <20 × 103/μL group.
The numbers of sessions for which data were available are shown in parentheses.
IQR, interquartile range.
No bleeding events of CTCAE grade 2 or higher occurred at the acupuncture site in all four groups (Table 4). For reference, there were 24 records of grade 1 bleeding at the acupuncture site during the whole study period (13 records in the 100 × 103/μL or more platelet count group, 0 in the 50–99 × 103/μL group, 4 in the 20–49 × 103/μL group, and 7 in the <20 × 103/μL group). Statistical tests and subsequent multivariate analyses were not performed because no bleeding events of CTCAE grade 2 or higher (outcome defined by the authors) occurred.
Bleeding Events By Platelet Count Group
CTCAE, Common Terminology Criteria for Adverse Events.
Discussion
The authors performed a retrospective investigation of the medical records of patients with hematological malignancies who received acupuncture during hospitalization and evaluated the bleeding risk at the acupuncture site according to the platelet count in four groups. No bleeding events requiring treatment occurred in any of the groups.
The result of this study was similar to the previous case series examining the risk of acupuncture bleeding in patients with thrombocytopenia. 20,21 Some of the guidelines that refer to platelet transfusion criteria state that platelet transfusion is not necessary since procedures that allow compression hemostasis of the puncture site, such as bone marrow examination, have a lower risk of significant bleeding, and the majority of bleeding events are not associated with thrombocytopenia. 17,18
Acupuncture, which allows compression hemostasis of the puncture site and is probably less invasive than bone marrow examination, may be a safe treatment for patients with hematological malignancies accompanying severe thrombocytopenia.
On the other hand, it should be noted that the results of this study do not guarantee that all acupuncture methods are safe. For example, different needle thicknesses and manufacturers may affect the risk of bleeding. Lee et al. evaluated (by multivariate analysis) factors associated with 264 bleeding events that occurred after 6635 acupuncture sessions in a prospective observational study and found that the incidence of bleeding events increased as the diameter of the needles increased. 26
In addition, Xie et al. observed the surface of the needles of two popular acupuncture needle brands using a scanning electron microscope and found many scratches and lumps on the tips of the needles of one of the brands. They stated that these needles might cause bleeding during needle insertion. 39 The needle diameter used in the present study is similar to that used in a previous case series (0.16–0.20 mm) of patients with thrombocytopenia where no bleeding was observed 20,21 and is smaller than that commonly used in clinical trials in patients with nonbleeding disorders. 40 –43
In addition, the needles used in this study and previous reports were from the same manufacturer. 20,21 This commonality of methods between the previous reports and this study is noteworthy, and there is a possibility that the acupuncture method adopted at the authors' facility was the reason why there were no bleeding events requiring treatment.
The number of acupuncture treatments in patients with thrombocytopenia in this study was the largest ever. To assess bleeding risk with accurate platelet counts, the authors included acupuncture sessions in their analysis when platelet count was measured on the same day of acupuncture and when no platelet transfusions were performed right before the session. Previous case series reporting bleeding risk of acupuncture in thrombocytopenic patients did not mention the presence or absence of platelet transfusions. 20,21
This study, however, has some limitations. First, the assessment of bleeding events was limited to CTCAE grade 2 or higher bleeding. While CTCAE grade 2 or higher bleeding requires treatment such as invasive intervention or red blood cell transfusion (Table 1) and thus its occurrence is recorded accurately in the medical record, minor bleeding (lower than grade 2) may not be recorded. Therefore, whether thrombocytopenia affects the risk of minor bleeding from acupuncture could not be investigated.
Second, despite being the largest scale to date, the sample size of this study may still have been insufficient to conclude the association between thrombocytopenia and acupuncture-induced bleeding events. A previous large prospective study reported that of 229,230 members of the general population who received an average of 10 acupuncture treatments, only 2615 (1.14%) had bleeding that required treatment. 44 Therefore, if thrombocytopenia has a small effect on the bleeding risk of acupuncture, the sample size in this study may not be large enough to detect such an effect.
Third, although the authors obtained consistent results with previous case series, 20,21 the generalizability of the results may be limited because this study was based on data from a single center. It cannot be ruled out that along with the acupuncture methods and devices mentioned above, the baseline risk of bleeding specific to the target patients at the authors' institution could have affected the outcome. A larger, prospective multicenter study is needed to resolve these limitations.
Conclusions
Acupuncture caused no bleeding events requiring treatment in patients with hematological malignancies, regardless of platelet count. The authors considered that acupuncture could be safely used to treat patients with hematological malignancies without causing serious bleeding.
Footnotes
Acknowledgment
The authors thank research assistant Rika Ishizuka (Office for Gender Equality Support in Fukushima Medical University) for her assistance in manuscript preparation.
Authors' Contributions
T.K. and Masao.S. contributed to the conception and design of this study. T.K. collected and analyzed the data. T.K., Masao.S., and T.M. interpreted data on acupuncture treatments and their adverse events. Manabu.S., S.I., Masumi.S., S.T., and M.O. interpreted data on thrombocytopenia and bleeding risk factors. The draft of the manuscript was created by T.K. All authors reviewed and approved the final version of the manuscript.
Data Availability Statement
The dataset supporting the conclusions of this article is available from the corresponding author on reasonable request.
Author Disclosure Statement
T.K., Masao.S., and T.M. are supported by a grant from Seirin Corporation. All other authors declare no conflicts of interest.
Funding Information
No funding was received for this article.