
Abstract
Objective:
Bone marrow suppression is the most common side effect of chemotherapy that may lead to discontinuation for treatment pertaining to patients during the therapy course. Acupuncture may relieve bone marrow suppression with regulation hematopoietic function during chemotherapy. The purpose of this study is to evaluate the effectiveness of acupuncture in relieving chemotherapy-induced bone marrow suppression and determine the effects of acupuncture on bone marrow function.
Design:
PubMed, Embase, Cochrane Library, Medline OVID, CINAHL Plus, Web of Science, and Chinese articles in the Airiti Library and China National Knowledge Infrastructure databases were searched up to February 2023. Publications in both English and Chinese were eligible for inclusion without any limitations on the publication date. Only randomized controlled trials investigating the impact of acupuncture on chemotherapy-induced bone marrow suppression were considered. In addition, a trial sequential analysis was performed to assess the adequacy of the current sample size.
Results:
A total of 25 studies met the inclusion criteria. Acupuncture was found to increase the levels of hematopoietic cytokine granulocyte colony-stimulating factor (G-CSF) (Hedges' g = 0.79, p < 0.001), as well as stimulate the production of white blood cells (Hedges' g = 0.69, p < 0.001), red blood cells (Hedges' g = 0.37, p = 0.01), neutrophils (Hedges' g = 0.66, p < 0.001), absolute neutrophil count (Hedges' g = 0.89, p = 0.01), hemoglobin (Hb) (Hedges' g = 0.37, p = 0.02), platelets (Hedges' g = 0.50, p < 0.001), and natural killer (NK) cells (Hedges' g = 1.30, p = 0.02). Further, the levels of platelets and NK cells were observed to increase cumulatively over time.
Conclusions:
Acupuncture may improve chemotherapy-induced bone marrow suppression due to increasing levels of the hematopoietic cytokine, G-CSF and further relieving chemotherapy-induced bone marrow suppression.
PROSPERO Registration:
This review was registered with PROSPERO (International Prospective Register of Systematic Reviews: CRD42020185813).
Background
Bone marrow suppression is extremely prevalent during chemotherapy and may lead to discontinuation or delay when patients are undergoing a treatment course for cancer. 1 The major problem is that chemotherapy-induced myelosuppression is the fatal side effect of chemotherapy, which consequently leads to decreased production of red blood cells (RBCs), resulting in anemia, white blood cells (WBCs), resulting in neutropenia or granulocytopenia, and platelets, resulting in thrombocytopenia, which may delay the treatment or life-threatening to cancer patients. 2,3
Granulocyte colony-stimulating factor (G-CSF) subcutaneous injection is commonly used in clinical settings to prevent or manage chemotherapy-induced leukopenia. 4 However, that results in nausea, syncope, bones and muscles aching, and flushing. 5 Further, not all cancer patients can benefit from this treatment as the National Health Insurance in Taiwan only covers those with WBCs <1000/μL or absolute neutrophil count (ANC) <500/μL. 6
Acupuncture involves the stimulation of specific acupoints on the skin with needles and is a modality of traditional Chinese medicine (TCM) used to relieve various symptoms. It was proven to improve menopausal symptoms, 7 premenstrual syndrome, 8 and mood, such as depression and anxiety. 9 It was also certified to improve side-effects for treatment of cancer, such as postoperative arm lymphedema, 10 chemotherapy-induced leucopenia, 3,11 chemotherapy-related nausea and vomiting, 12 and chemotherapy-induced peripheral neuropathies. 13,14 However, the efficacy of acupuncture for chemotherapy-related myelosuppression remains unclear.
Many studies revealed the impacts of acupuncture on chemotherapy-induced leukopenia. 15 –18 Thus far, only a few kinds of literature focused on the chemotherapy-related myelosuppression, 1,19,20 among which, one of them was systematic review 19 ; one was a protocol for a systematic review and meta-analysis 20 ; another one study reported only blood values: WBCs, RBCs, hemoglobin (Hb) as an outcome variable. 1
The most recent meta-analysis was published in 2019, which only mentioned that TCM combined therapy may be associated with bone marrow suppression but did not report any specific indicators of blood cell counts. 21 Nonetheless, the mechanism for acupuncture stimulates anticancer immunity, promoting the protective effects of bone marrow or increasing the activity of serum colony-stimulating factors remain unclear nowadays.
Those reviews mostly focused on chemotherapy-induced leucopenia and are now outdated. In addition, the hematopoietic cytokine, G-CSF, in patients during chemotherapy and using a trial sequential analysis (TSA) to detect whether the sample size is enough has not been assessed in previous reviews.
Therefore, the purpose of this study was to systematically evaluate the effectiveness of acupuncture in relieving chemotherapy-induced bone marrow suppression and determine the mechanism for effects of acupuncture on bone marrow functions.
Methods
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement guidelines were followed in conducting this systematic review and meta-analysis. The review was registered with PROSPERO-CRD42020185813. For more details on PRISMA, please refer to Supplementary Data S1.
Literature sources and search strategy
The literature search for relevant studies was conducted until February 2023 using electronic databases such as Cochrane Library, Embase, PubMed, Medline OVID, Web of Science, CINAHL Plus, China National Knowledge Infrastructure, and Airiti Library. The search was limited to articles published in English or Chinese, involving human participants.
Further, we also explored pertinent literature in the references, government publications, and recommendations provided in the studies that were included. We also searched several websites, including
The search strategy applied a combination or separation of Medical Subject Headings (MeSH) terms and text words associated with several keywords such as G-CSF, granulocyte-macrophage colony-stimulating factor (GM-CSF), GM-CSF, stem cell factor (SCF), SCF, white blood cell, leukocyte, leukopenia, neutropenia, Hb, anemia, platelet, thrombocyte, thrombocytopenia, chemotherapy, and acupuncture. Please refer to Supplementary Table S1 for a detailed search strategy used for PubMed.
Inclusion criteria
We included randomized controlled trials (RCTs) published in English or Chinese languages, without any time restriction, that examined the use of acupuncture in managing chemotherapy-induced bone marrow suppression in cancer patients. Study participants with a cancer diagnosis undergoing chemotherapy, regardless of age, gender, or race, were considered eligible for inclusion.
Studies that assessed any type of invasive acupuncture, with or without electrical stimulation, and involved needle insertion at acupuncture points, were included in the analysis. To meet eligibility criteria, studies had to measure at least one hematopoietic outcome indicator, such as G-CSF, GM-CSF, SCF, WBCs, Hb, or platelets.
Exclusion criteria
Studies that were excluded from our analysis, such as cohort and case-control studies, observational studies, case reports, qualitative studies, non-RCTs, review articles, and laboratory studies involving animals. Moreover, studies that enrolled participants with hematopoietic diseases or those that had overlapping participants with other studies already included in our analysis were also excluded.
Data extraction and quality assessment
The titles and abstracts of the articles obtained through the search strategy were assessed by two researchers (Y.W.S. and M.H.W.) independently, who also extracted the pertinent information about the eligible studies. In the event of any discrepancies between the two investigators, a third researcher (H.T.T.) was consulted to resolve the issue through discussion.
We selected studies for further review based on the following criteria, also known as PICO: Population, Intervention, Comparator, and Outcome. The study population comprised individuals who had been diagnosed with cancer at any stage and were receiving chemotherapy treatment. The intervention included real acupoint stimulation using invasive techniques such as manual acupuncture, electro-acupuncture (EA), acupoint injection, or warm-acupuncture.
The outcome of interest was the investigation of at least one hematopoietic outcome indicator, including changes in G-CSF, GM-CSF, SCF, WBCs, Hb, and platelets, to evaluate the bone marrow function. We only included RCTs with at least one control group that received routine therapy, a placebo, or other appropriate controls. The primary outcomes of this study were hematopoietic relevant cytokines and blood indicators, including G-CSF, WBCs, RBCs, Hb, neutrophils, platelets, ANC, and natural killer (NK) cells. The secondary outcomes were the cumulative time-dependent responses of acupuncture, as well as subgroup analyses for various types of acupuncture.
Two reviewers (Y.W.S and M.H.W.) assessed the methodological quality of each study using the Cochrane Handbook for Systematic Review of Intervention's risk of bias assessment tool, version 5.1.0. 22 The reviewers evaluated various aspects of the studies, including random sequence generation, allocation concealment, blinding of participants and staff, blinding of outcome assessments, incomplete outcome data, and selective reporting.
In the event of any disagreements, a third reviewer (H.T.T.) was consulted to resolve the issue through discussion. The data from the studies were extracted independently by the two reviewers (Y.W.S and M.H.W.) and compiled in Table 1. Any discrepancies that arose were resolved through discussion or consultation with the third independent reviewer (H.T.T.).
Characteristics of the Included Studies
ADM, ÿdriamycin; ANC, absolute neutrophil count; AP, ÿdriamycin/cisplatin; BCNU, bis-chloroethylnitrosourea; BEP, bleomycin/etoposide/cisplatin; CAF, cyclophosphamide/ÿdriamycin/5-fluorouracil; CAP, cyclophosphamide/ÿdriamycin/cisplatin; CF, carboplatin; CHOP, cyclophosphamide, doxorubicin/hydroxydaunorubicin, vincristine/oncovin, prednisone/prednisolone; CMF, cyclophosphamide/methotrexate/5-fluorouracil; CTX, cyclophosphamide; DDP, cisplatin; FLO, fluorouracil/leucovorin/oxaliplatin; Folfiri, folinic acid/5-fluorouracil/irinotecan; Folfox, folinic acid/fluorouracil/oxaliplatin; 5-FU, 5-fluorouracil; G-CSF, granulocyte colony-stimulating factor; GM-CSF, granulocyte-macrophage colony-stimulating factor; GP, gemcitabine/cisplatin; Hb, hemoglobin; MMC, mitomycin C; MTX, methotrexate; MVP, mitomycin/vindesin/cisplatin; n/a, not applicable; NK, natural killer; NPC, nasopharyngeal carcinoma; PC, cisplatin/cyclophosphamide; RBCs, red blood cells; WBCs, white blood cells.
Statistical analysis
We calculated two-sided p-values, with a level of statistical significance set at p < 0.05. First, we obtained pre- to post-test score changes for both the intervention and control groups from each included study. Subsequently, we calculated the effect size for the difference between the intervention and control groups for each study. The Hedges' g was used to determine the effect size index, and it was calculated using the formula: g = d(1 − (3/(4(n1 + n2) − 9))). 23
We presented the results as the effect size (Hedges' g) with a confidence interval (95% CI). An effect size of Hedges' g ranging from 0.2 to 0.4 indicates a small effect, 0.5 to 0.7 represents a moderate effect, and an effect size of ≥0.8 represents a large effect. 24 A random-effects model was chosen due to the variation in the characteristics of the included studies, such as different cancer stages, types of cancer, types of acupuncture used (manual acupuncture or EA ), theoretical principles of acupuncture point selection (fixed or unfixed points), total treatment dose (min), and study quality.
To evaluate heterogeneity among the studies, Cochran's Q test was employed with statistical significance set at p < 0.1. Moreover, we utilized the I 2 statistic to determine the proportion of total variance in the pooled effect size that could be attributed to heterogeneity among studies. An I 2 value of 0% indicates no heterogeneity, 25% indicates low heterogeneity, 50% indicates moderate heterogeneity, and an I 2 value of ≥75% indicates high heterogeneity. 24
To identify the potential sources of heterogeneity, moderator analyses were conducted. When heterogeneity was observed, subgroup analyses were conducted for categorical variables, and meta-regression analyses were conducted for continuous variables. 25
The moderator analyses were limited to groups reported by at least two studies to ensure that sufficient data were obtained for analysis. 24 The sensitivity analyses were conducted to assess the robustness of synthesized results. The asymmetry of the funnel plot was evaluated using Egger's regression intercept test, and a p-value of <0.05 indicated the presence of publication bias.
To further account for possible bias in the overall log odds ratio, the trim-and-fill method was used to estimate the number of missing studies. Funnel plots were only generated if there were >10 studies. 26,27 Moderator analyses and all statistical analyses were performed using Comprehensive Meta-analysis version 3.0.
We employed TSA to calculate the optimal sample size to avoid Type I errors (α). By analyzing the cumulative Z-curve, we determined whether it intersected the trial sequential monitoring boundary or crossed into the futility area, which would indicate whether there was enough evidence to support the anticipated intervention effect, and whether further studies were unnecessary.
To determine the required sample size, we considered the mean difference and variance in changes in blood cell count levels, while setting the Type I error (α) and power (1 − β) at 0.05 and 80%, respectively. 28 TSA versus 0.9 beta software was used for the analysis.
Results
Study selection
Initially, a total of 1004 studies were searched, and 136 duplicate articles were eliminated. Subsequently, 601 articles were excluded from the study, as they did not meet the eligibility criteria: conference papers (n = 6), editorial letters/comments (n = 26), animal/cell studies (n = 174), meta-analyses or reviews (n = 87), study protocols (n = 8), and non-relevant outcomes (n = 300).
Thus, 267 studies remained for full manuscript review, of which 242 studies were excluded for various reasons: different target population (n = 174), non-invasive acupuncture approach (n = 53), non-RCT study design (n = 9), and data could not be extracted (n = 6). Ultimately, 25 studies were selected for further qualitative and quantitative analyses. 3,7,9,11,16,18,20,29 –46 Figure 1 depicts the review process in the form of a PRISMA flow diagram.

PRISMA flow diagram of the review process. RCTs, randomized controlled trials.
Characteristics of the included studies
A total of 25 studies were included in the analysis, with a combined sample size of 1974 participants. 3,7,9,11,16,18,20,29 –46 These studies employed a randomized controlled design and investigated various types of cancer, including lung cancer, gastric cancer, breast cancer, liver cancer, and lymphomas. The chemotherapeutic regimens utilized in the included studies were also diverse.
The publications covered a time period from 1991 to 2022, and among the 25 studies, 1 was conducted in Portugal, 11 1 took place in the United States, 16 1 in Australia 37 ; and most of them were carried out in China, 3,7,9,18,20,29 –36,38 –46 in which, some of the included studies were not described articles in English. 7,9,18,29 –31,33,35,36,38 –45 Various types of acupuncture interventions were utilized, which included eleven trials of manual acupuncture, eight trials of EA, two trials of acupoint injection, two trials of acupoint catgut-embed, and two trials of warm-acupuncture. Table 1 provides details characteristics of the included studies.
Methodological quality assessment
Table 2 presents data on the methodological rigor of the chosen studies. All of the studies analyzed in the review reported random sequence generation. Nonetheless, two studies failed to report allocation concealment or blinding of participants and personnel, leading to a higher risk of bias. 9,46 Most of the included studies had unclear risk for blinding of participants and personnel.
Risk of Methodological Bias of the Included Studies
H, high risk; L, low risk; U, unclear risk of bias.
Only four studies were classified as having high risk for blinding of the outcome assessment, 18,35,38,45 whereas the remaining studies were classified as having unclear risk. 3,7,9,11,16,20,29 –34,36,37,39 –44,46 In terms of addressing incomplete outcome data, three studies were classified as having high risk, 29,31,32 whereas the remaining studies had low risk. Finally, all of the studies had a low risk of selective reporting.
The overall effect of acupuncture on indicators of bone marrow function
The 25 studies demonstrated significant improvements in the counts of G-CSF white blood cells, RBCs, neutrophils, ANC, Hb, platelets, and NK cells through acupuncture during chemotherapy, as evidenced by the overall effect sizes. 3,7,9,11,16,18,20,29 –32,34 –46 The overall effect size was Hedges' g of 0.69, p < 0.001, I 2 = 70% for increased WBCs by acupuncture (Fig. 3).
A sensitivity analysis was performed by removing the study with the largest effect size. 44 The effect size of the acupuncture intervention remained statistically significant (Hedges' g = 0.61, p < 0.001) (data not shown). Hedges' g indicated statistical significance for outcomes of G-CSF (Hedges' g = 0.79, p < 0.001, I 2 = 0%) (Fig. 2), RBCs (Hedges' g = 0.37, p = 0.01, I 2 = 57%) (Fig. 4), neutrophil counts (Hedges' g = 0.66, p < 0.001, I 2 = 44%) (Fig. 5), the ANC (Hedges' g = 0.89, p = 0.01, I 2 = 0%) (Fig. 6), Hb counts (Hedges' g = 0.37, p = 0.02, I 2 = 69%) (Fig. 7), platelet counts (Hedges' g = 0.50, p < 0.001, I 2 = 56%) (Fig. 8), and NK cell counts (Hedges' g = 1.30, p = 0.02, I 2 = 85%) (Fig. 9).

Forest plot of the overall effect sizes for studies measuring G-CSF counts and acupuncture. Q = 0.09, p = 0.76, I 2 = 0.00. Fixed-effects Hedges' g = 0.79, p < 0.001. Random-effects Hedges' g = 0.79, p < 0.001. G-CSF, granulocyte colony-stimulating factor.
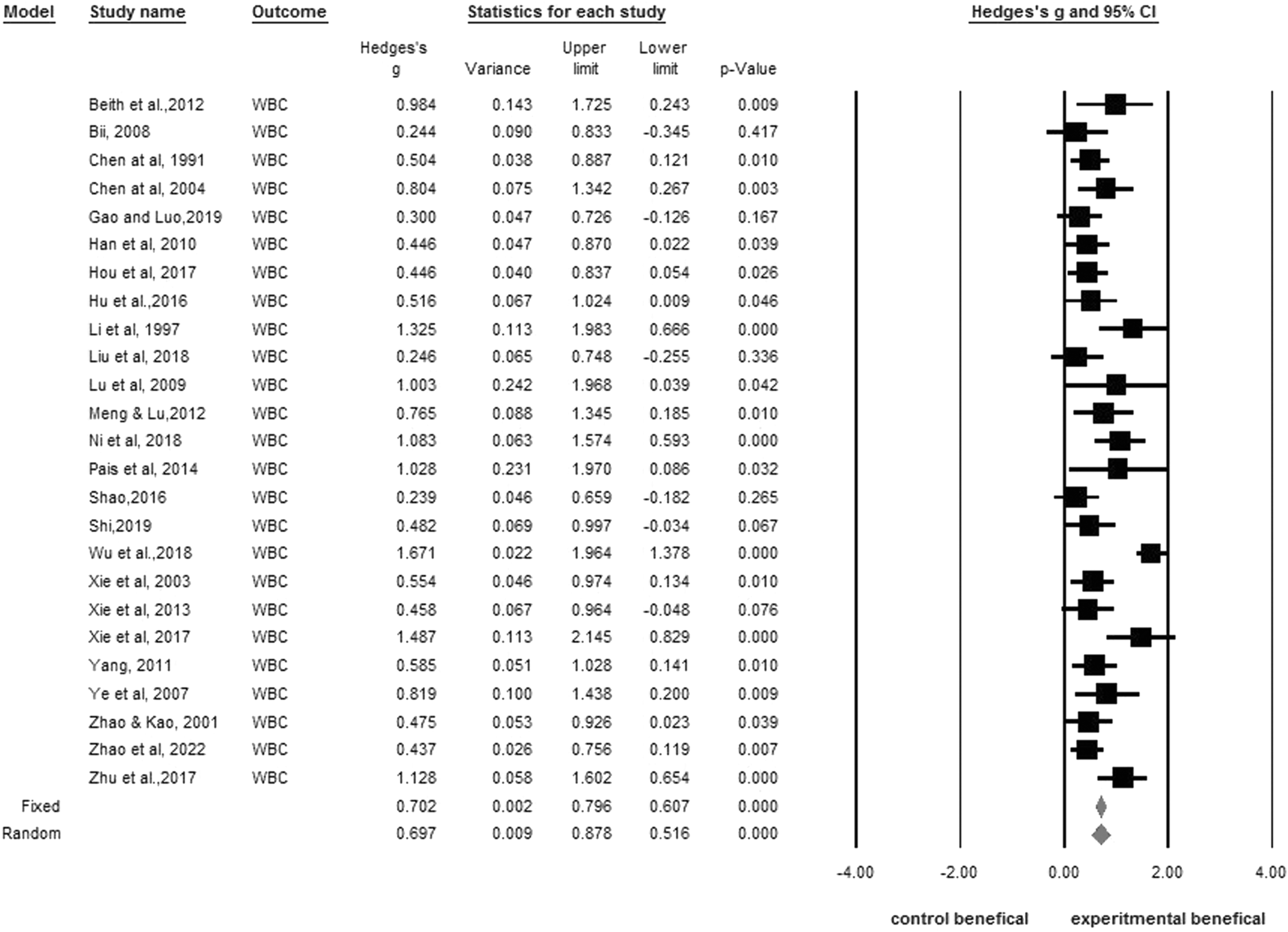
Forest plot of the overall effect sizes for studies measuring WBC counts and acupuncture. Q = 82.11, p < 0.001, I 2 = 70.77. Fixed-effects Hedges' g = 0.70, p < 0.001. Random-effects Hedges' g = 0.69, p < 0.001. WBC, white blood cell.

Forest plot of the overall effect sizes for studies measuring RBC counts and acupuncture. Q = 7.11, p = 0.07, I 2 = 57.79. Fixed-effects Hedges' g = 0.43, p < 0.001. Random-effects Hedges' g = 0.37, p = 0.01. RBC, red blood cell.

Forest plot of the effective response of neutrophil counts. Q = 7.24, p = 0.12, I 2 = 44.74. Fixed-effects Hedges' g = 0.63, p < 0.001. Random-effects Hedges' g = 0.66, p < 0.001.

Forest plot of the effective response of ANCs. Q = 0.06, p = 0.81, I 2 = 0.00. Fixed-effects Hedges' g = 0.89, p = 0.01. Random-effects Hedges' g = 0.89, p = 0.01. ANCs, absolute neutrophil counts.
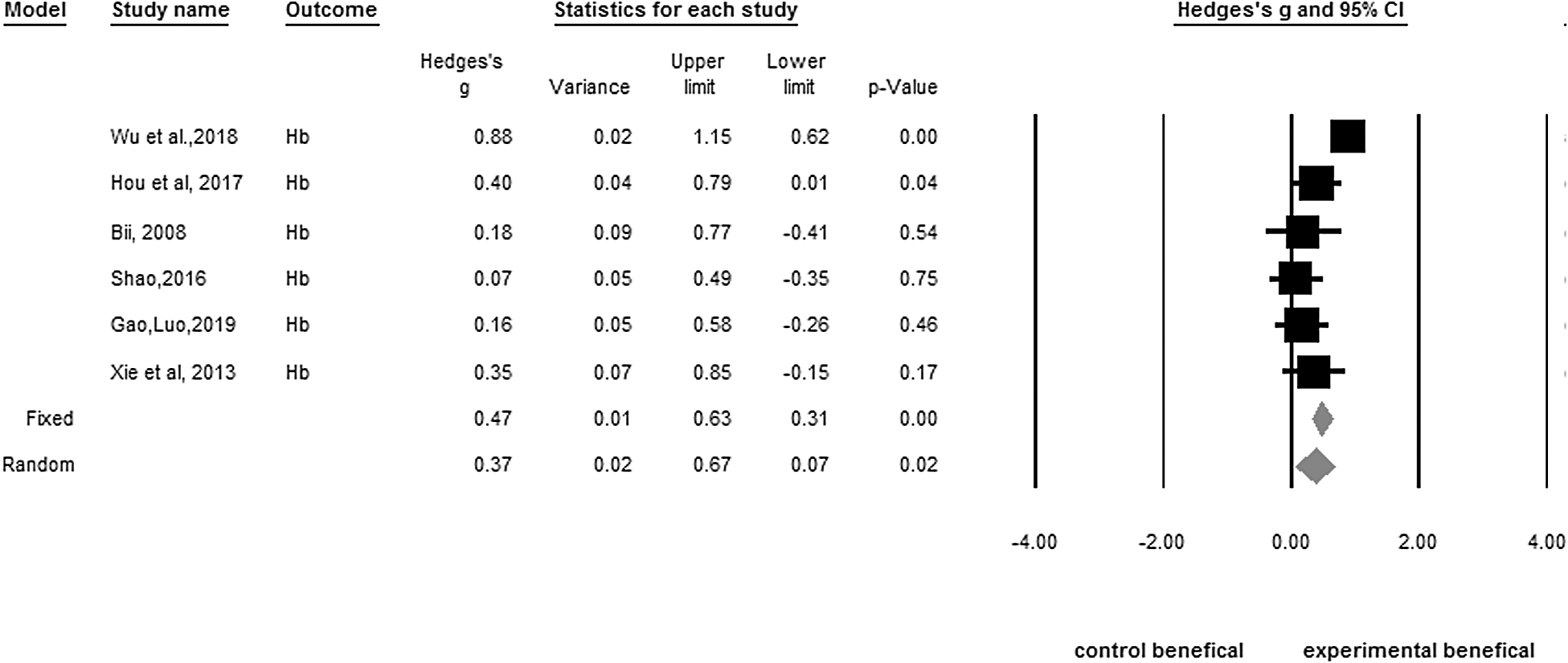
Forest plot of the effective response of hemoglobin counts. Q = 16.28, p = 0.01, I 2 = 69.28. Fixed-effects Hedges' g = 0.47, p < 0.001. Random-effects Hedges' g = 0.37, p = 0.02.
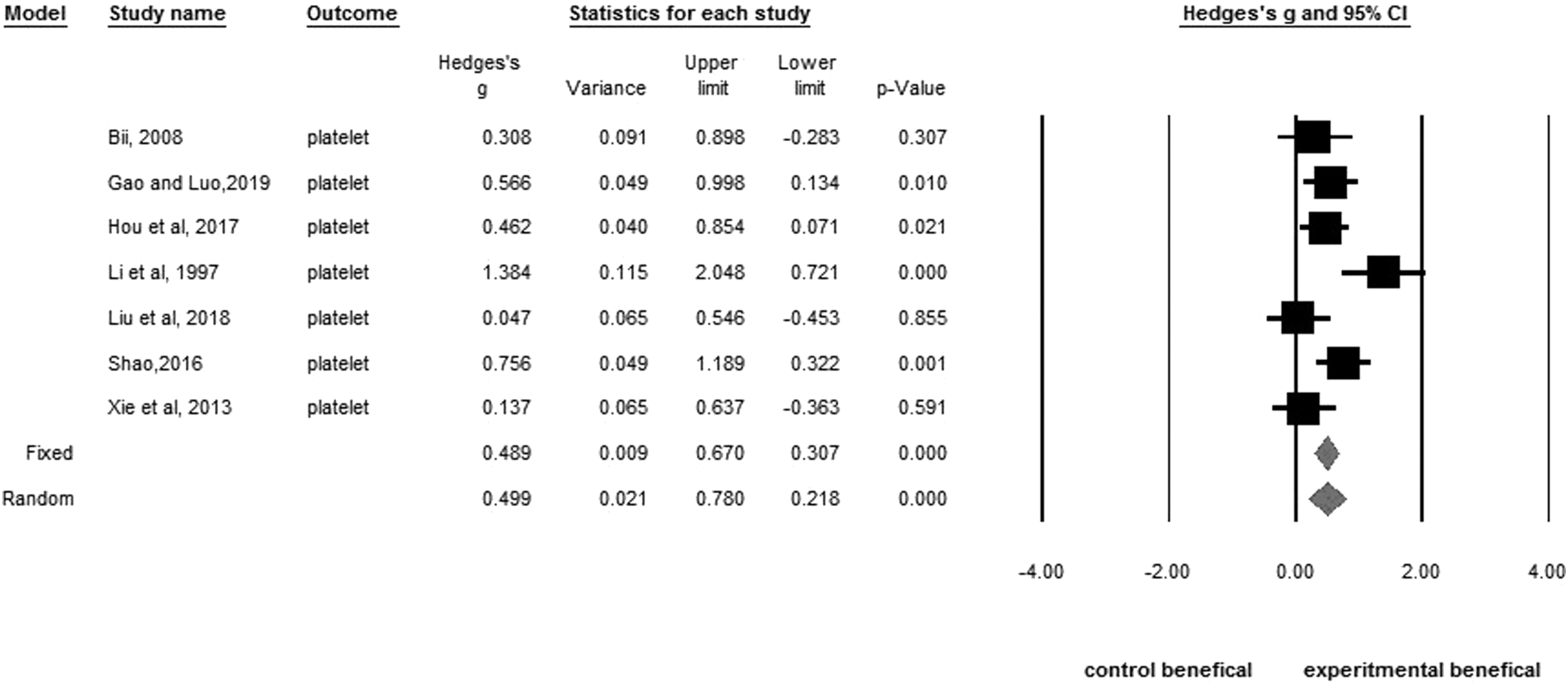
Forest plot of the effective response of platelet counts. Q = 13.86, p = 0.03, I 2 = 56.70. Fixed-effects Hedges' g = 0.49, p < 0.001. Random-effects Hedges' g = 0.50, p < 0.001.
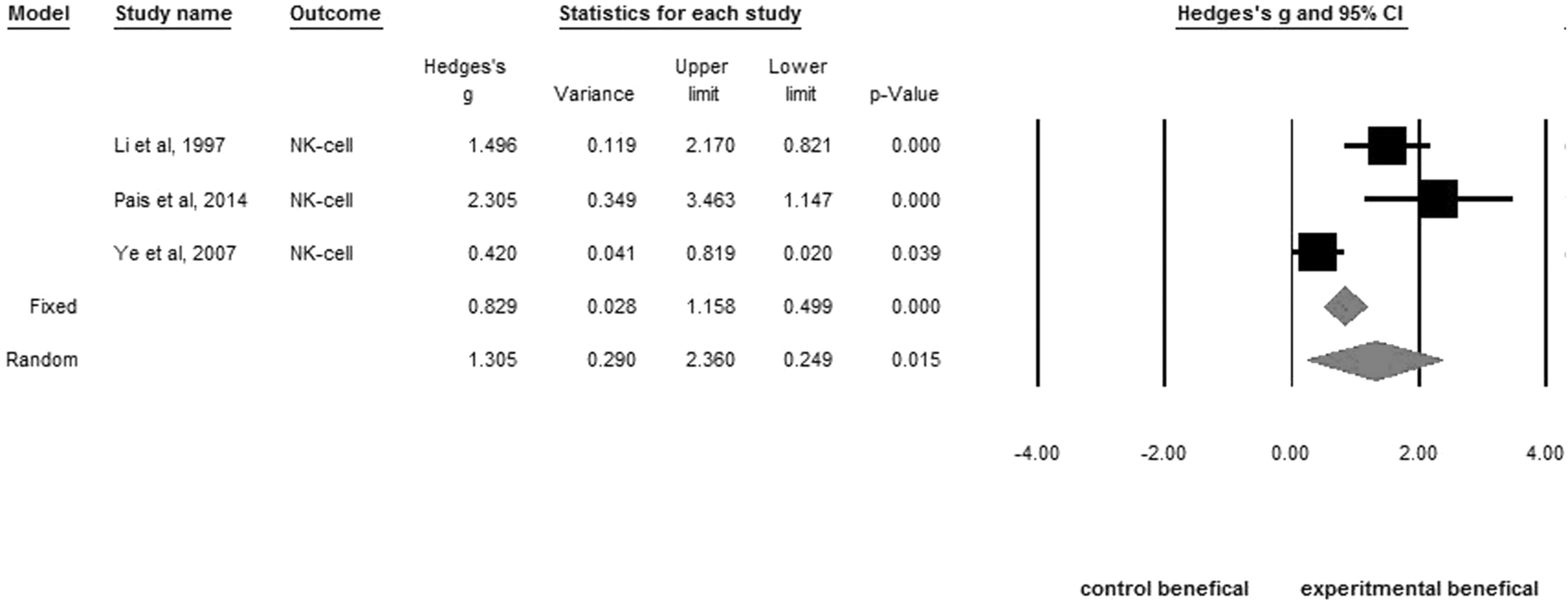
Forest plot of the effective response of NK-cell counts. Q = 14.02, p = 0.001, I 2 = 85.74. Fixed-effects Hedges' g = 0.83, p < 0.001. Random-effects Hedges' g = 1.30, p = 0.02. NK, natural killer.
Moderator analyses
I 2 statistics indicated moderate heterogeneity of WBC values (Q = 82.11, p < 0.001, I 2 = 70%), RBC (Q = 7.11, p = 0.07, I 2 = 57%), Hb (Q = 16.28, p = 0.01, I2 = 69%) and platelet values (Q = 13.86, p = 0.03, I 2 = 56%), and neutrophil (Q = 7.23, p = 0.12, I 2 = 44%) across the included studies. High heterogeneity of NK-cell values (Q = 14.02, p = 0.001, I 2 = 85%) was observed. In addition, the G-CSF and ANC was homogeneous. Therefore, subgroup analyses and a meta-regression were performed on NK cells to further explore factors that might have contributed to the heterogeneity.
Subgroup analyses
Regarding heterogeneity, the subgroup analyses examined different acupuncture types of WBCs, platelets, NK cells, and neutrophils. However, the mixed effects for types of acupuncture groups were not significant (WBC: Q = 5.04, p = 0.28; platelets: Q = 3.19, p = 0.07, NK cells: Q = 3.00, p = 0.08; neutrophils: Q = 4.37, p = 0.11). This suggested that regardless of the type of acupuncture, WBCs, platelets, NK cells, and neutrophils increased overall. Data are not shown.
Meta-regression analyses
For continuous moderators, the meta-regression analyses revealed that cumulative time-dependent responses of acupuncture and NK cells, platelets significantly increased (p = 0.005, and p = 0.001, respectively). This implied that the cumulative time-dependent responses of NK cells and platelets increased over time. The data are shown in Figures 10 and 11. The WBCs showed the trend increased over time but not statistically significantly. Other blood indicators were not significantly increased.
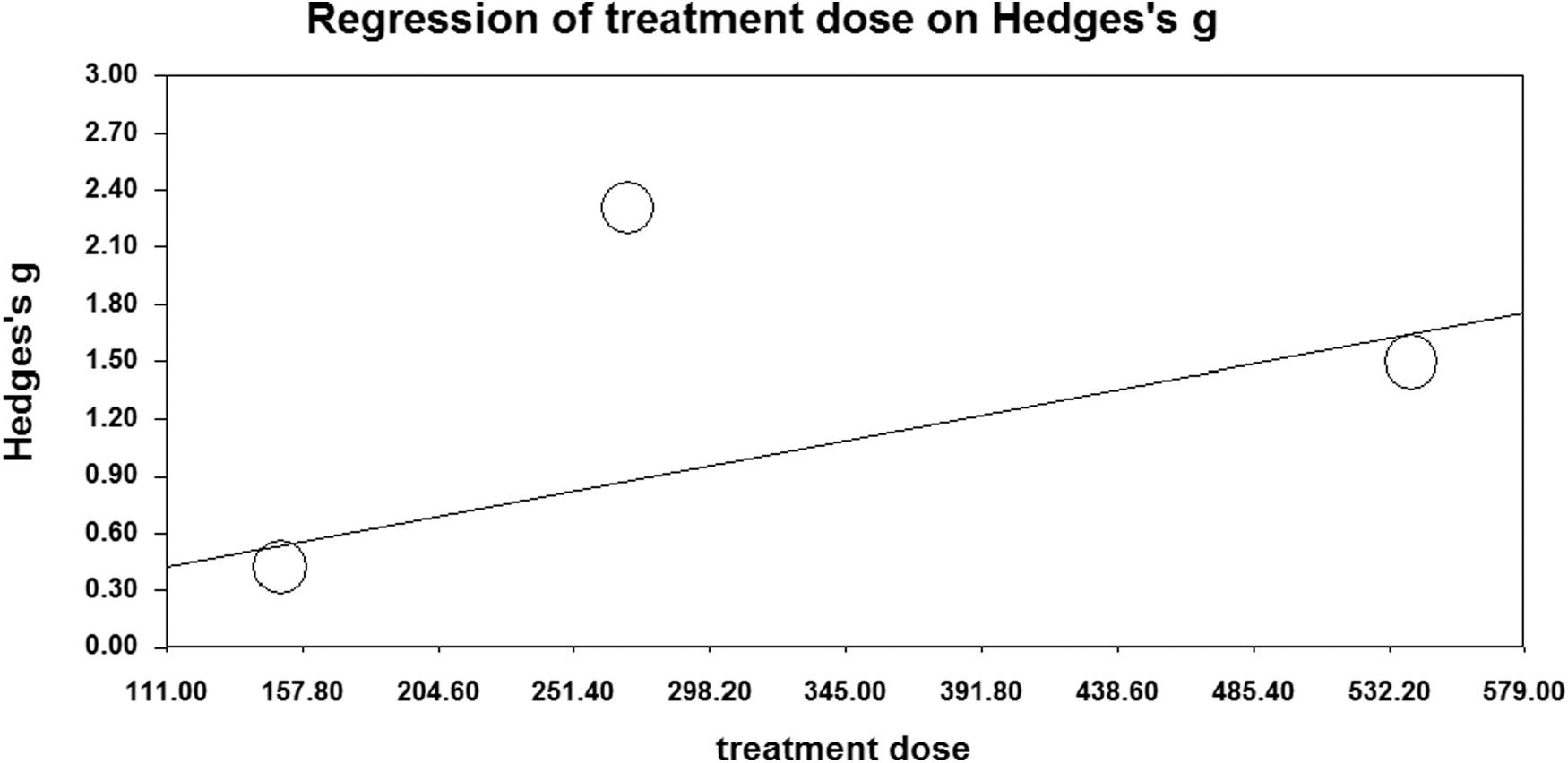
Meta-regression analyses performed by different total treatment doses (min) for NK cells. NK, natural killer.

Meta-regression analyses performed by different total treatment doses (min) for platelet counts.
Publication bias
No significant publication bias existed for the main blood indicators in WBC. The results of Egger's regression test are displayed in Figure 12, with a t-value of 0.06 and a p-value of 0.95. Publication bias was not evaluated for other blood indicators, because there were fewer than ten studies for the funnel plot.
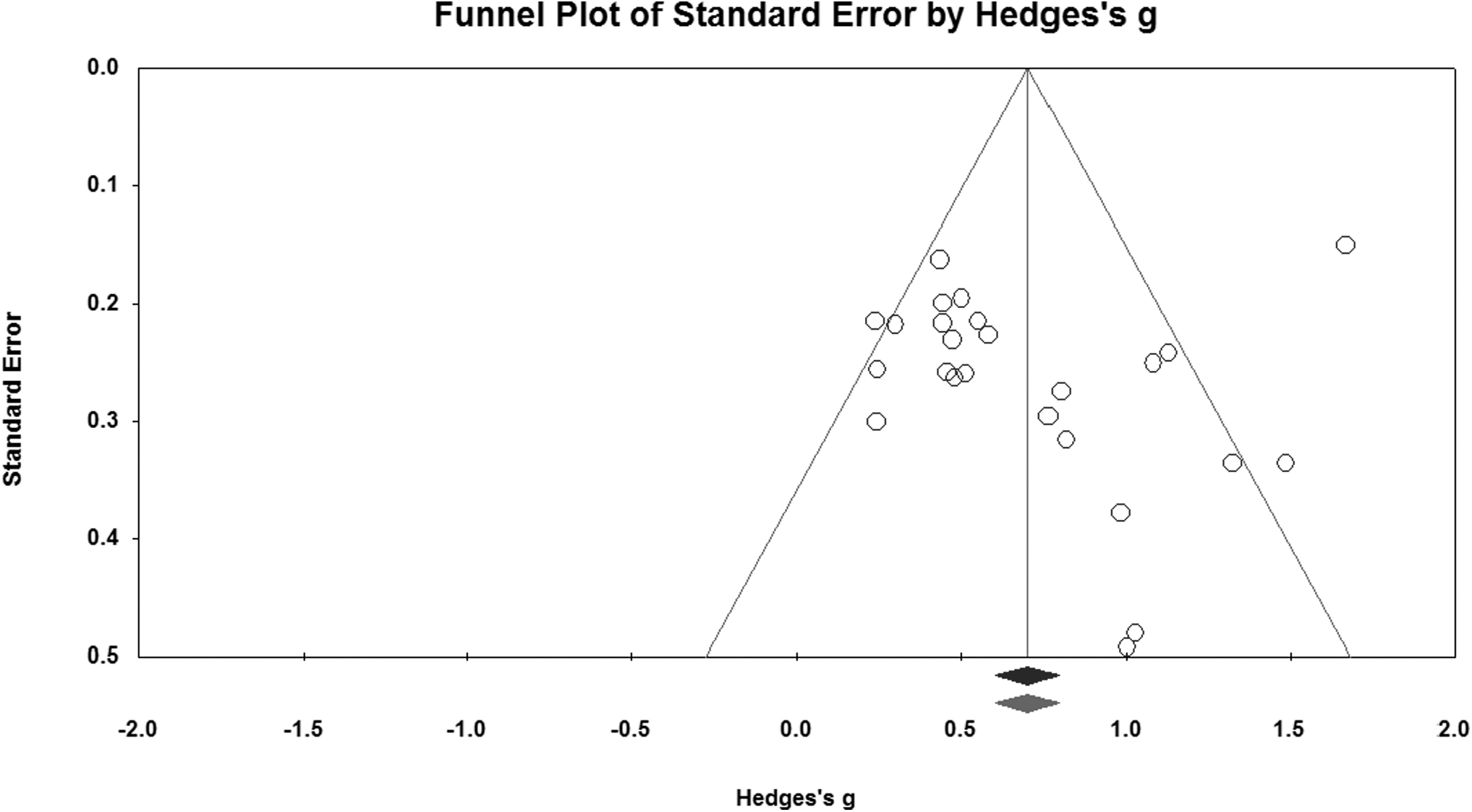
Funnel plot of the meta-analysis of included papers that examined WBC counts. Egger's test showed that the t value was 0.06, p = 0.95. WBC, white blood cell.
Trial sequential analysis
TSA was utilized to investigate the effects of acupuncture on bone marrow suppression across 14 trials 9,18,20,30,34,36,38 –45 A random-effects model was utilized to generate the cumulative z-curve, with an α value of 5% (two-sided) and β of 20%. The necessary information size was determined to be 263, and the z-curve intersected both the conventional and trial sequential monitoring boundaries, meeting the required information size. As a result, there is enough evidence to reach a conclusion (as depicted in Fig. 13). However, the TSA data only presented the impact of acupuncture on myelosuppression for the main outcome of WBCs, as there were insufficient data available for other indicators.
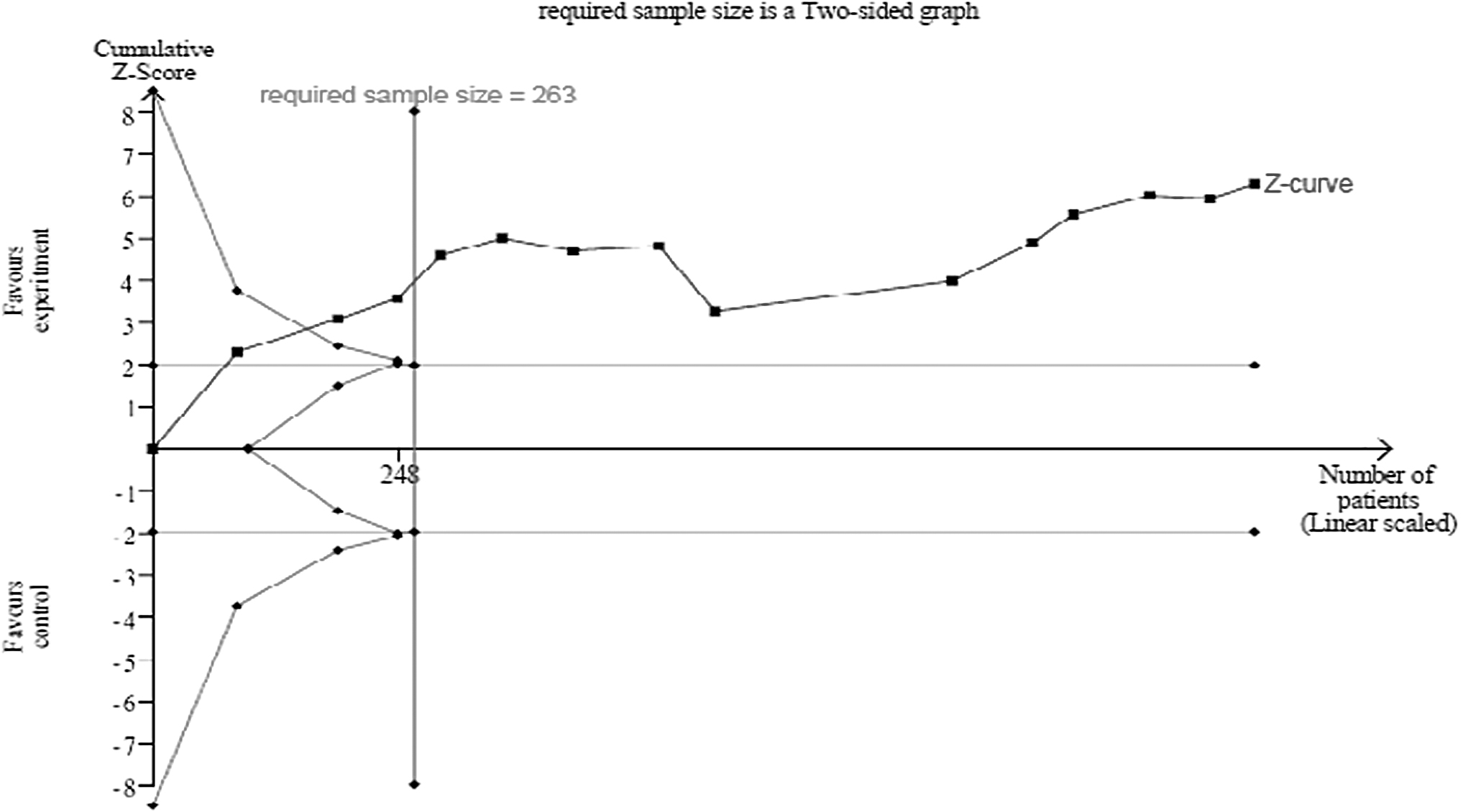
Trial sequential analysis of the effects of bone marrow suppression and acupuncture.
Discussion
The current meta-analysis consists of 25 RCTs indicated, the significant effect of invasive acupuncture for ameliorating myelosuppression when cancer patients are undergoing chemotherapy. 3,7,9,11,16,18,20,29 –46 Based on previous research, acupuncture may relieve bone marrow suppression and increase G-CSF production, thereby further improving hematopoietic function during chemotherapy. 47,48 The possible mechanism would be the G-CSF-stimulated increased neutrophil proliferation and differentiation, with blood cell counts for the ANC, WBCs, Hb, and platelets subsequently being enhanced.
The G-CSF is a kind of hematopoietic cytokine, and it has a vital role in modulating hematopoiesis. 49 The G-CSF stimulates hematopoietic stem cells to produce granulocytes and stem cells and release them into the bloodstream. The G-CSF also stimulates the survival, proliferation, differentiation, and function of neutrophil precursors and mature neutrophils via signal transduction pathways. 49,50
The G-CSF is a glycoprotein that has multiple functions in both physiological and pathophysiological conditions. 51 From a biological perspective, an increase in G-CSF levels might be a possible mechanism underlying the effectiveness of acupuncture in patients undergoing chemotherapy, and it would be valuable to hypothesize a causal pathway that might explain this association. 47
In addition, the primary concern of cancer patient's health status is chemotherapy-induced pancytopenia, which refers to myelosuppression. 10 The findings of the current meta-analysis of RCTs showed that acupuncture was associated with increased bone marrow function during chemotherapy.
Acupuncture has been found to increase granulocyte counts, including neutrophils and WBCs, as well as the ANC, according to a meta-analysis. A study by Pais et al. suggested that acupuncture is effective in boosting the immune system. Their RCT showed that acupuncture led to a statistically significant overall enhancement of WBCs, ANC, and NK cells in the acupuncture group (p = 0.036, p = 0.046, and p < 0.001, respectively). 11
In contrast, Lu et al.'s RCT consisted of 21 gynecologic cancer patients undergoing chemotherapy who were included and randomly assigned to either the acupuncture group or the sham acupuncture group. The sham acupuncture group involved inserting needles away from the usual TCM acupuncture points. The study evaluated the impact of treatment on WBCs, ANC, and G-CSF levels.
After six sessions, the WBC values were significantly higher in the acupuncture group (p = 0.04); however, no significant differences were observed between the acupuncture and sham groups for ANC and G-CSF values (p = 0.09 and p = 0.78, respectively). The study's small sample size (n = 21) may have contributed to the lack of significant differences in ANC and G-CSF levels. 16
The findings of this meta-analysis revealed that platelet values were higher than those of the control group due to the effect of acupuncture. This finding is consistent with a meta-analysis of 35 RCT studies by Li et al, 52 involving 2618 patients. They investigated the effect of acupoint stimulation on chemotherapy for non-small cell lung cancer, and leukocytopenia, thrombocytopenia, and immune function significantly improved overall.
Large effect sizes were exhibited in WBC values (Z = 7.45, 95% CI = 0.46–0.63) (p < 0.001), platelets (Z = 3.40, 95% CI = 0.36–0.76), and NK cells (Z = 4.08, 95% CI = 1.18–3.36), but not in Hb (Z = 1.32, 95% CI = 0.34–1.24, p = 0.19). 52 However, some scholars had contrary opinions, as an acupoint stimulation RCT study comprised 28 women with gynecological cancer revealed that Hb significantly decreased from (mean ± standard deviation [SD]) 11.6 ± 2.2 to 10.8 ± 1.6 mg/dL (p = 0.03) in the control group, compared with the experimental group (mean ± SD) 11.4 ± 1.0 to 10.9 ± 1.1 mg/dL (p = 0.29).
Those findings suggested that acupoint stimulation may be associated with preventing chemotherapy-induced myelosuppression hypochromia, 6 the results of which are similar to our findings.
Acupuncture can regulate immune function among cancer patients by two cytokines: interleukin (IL)-2 and interferon (IFN)-α, which then stimulate NK-cell proliferation and differentiation. 49 Johnston et al., 53 using normal rats with EA applied at the Zu-Sanli point (ST36) for 2 h daily on 3 consecutive days, found enhanced values of NK cells compared with the non-acupuncture control group. 53
In addition, a previous in vivo study suggested that acupuncture is useful in anticancer therapy either by actively stimulating immune activity or by preventing chemotherapy suppression of immune activity. 34 One study discovered that acupuncture treatment significantly increased NK-cell activity in mice with mammary cancer compared with the control group (p < 0.05) after eight sessions. 54
In addition, a recent study demonstrated that patients with stage IIb–IIIb cervical squamous cell carcinoma who underwent four cycles of cisplatin combined with EA treatment had increased NK cells in their peripheral blood and reduced tumor volumes. 55
To investigate further heterogeneity, a subgroup analysis was conducted to examine the effect of different types of acupuncture on the increase in WBCs. The analysis revealed that no matter of the manner for acupuncture used, there was an overall increase in leucocytes (mixed-effects model: Q = 5.04, p = 0.28). The current finding aligns with the outcomes of a prior meta-analysis that suggested that diverse types of acupuncture, such as needle insertion at acupoints, acupoint injection, plaster application, and moxibustion, can boost the immune response of cancer patients undergoing chemotherapy and improve myelosuppression via blood regulation. 56
In addition, different modalities of acupoint stimulation, such as EA, transcutaneous electrical acupoint stimulation (TEAS), and moxibustion, have been shown to improve myelosuppression and immunosuppression in patients undergoing chemotherapy. 1 There is a randomized control trial comprising 100 lung cancer patients, who were treated with chemotherapy and combined with TEAS for chemotherapy-induced immunosuppression.
The results indicated that the leukocyte and platelet counts were significantly enhanced within 2 weeks by TEAS. 20 And another pilot showed that acupuncture was an effective method for boosting leukocyte, neutrophil, and NK cells in patients with colorectal cancer after chemotherapy. 11 Thus, it can be concluded that the peripheral leukocyte and immune cell counts can be enhanced by acupoint stimulation, which is also an efficacious method of preventing myelosuppression and ameliorating immunosuppression in chemotherapy-related side effects.
The meta-regression analyses in this study revealed that levels of platelets and NK cells significantly increased in cumulative time-dependent manners, and the WBCs increased over time. A noteworthy discovery from an RCT is that acupoint stimulation had a significant interactive effect with time on SCF elevation. SCF is a cytokine that promotes the growth and differentiation of progenitor cells, and it is responsible for the maturation of granulocytes, lymphocytes, megakaryocytes, and erythrocytes. 6
They further indicated that the interactive effect was borderline significant after 3 weeks (p = 0.05), whereas the effect of the intervention on the group was significant after 6 weeks (p = 0.02). 6 This possibly implies that the efficacy of blood cells cumulatively time-dependently increases over time. Importantly, the cumulative time-dependent increased responses of WBCs, platelets, and NK cells were proven by the current meta-analysis results. Therefore, WBC, platelets, and NK cells increased due to acupuncture over time.
Anemia, thrombocytopenia, and pancytopenia are the most common symptoms of bone marrow suppression during chemotherapy. 21 The findings of the current study indicated that acupuncture improved bone marrow function during chemotherapy and increased values of WBCs, RBCs, neutrophils, the ANC, Hb, platelets, and NK cells. The possible mechanism is that acupuncture can enhance G-CSF. 57
The G-CSF is a key role in modulating hematopoiesis, and acupoint stimulation by acupuncture may increase the level of G-CSF, boosting the production of blood cells, and stimulate growth and differentiation of the megakaryocyte erythroid progenitor, which benefits the proliferation of erythrocytes, platelets, and the granulocyte-macrophage progenitor, which is associated with the production of mature blood cell components of neutrophils, the ANC, and WBCs. 57
The earlier mentioned findings summarize our findings that acupuncture is an effective approach to improve the production of the SCF, and further activate the G-CSF that prompts hematopoietic stem/progenitor cell proliferation, enhancing the production of blood cells, and eventually relieves chemotherapy-related myelosuppression.6,16,57 The mechanism of hematopoietic regulation on acupuncture ameliorates myelosuppressive-related chemotherapy may involve these two cytokines, particularly of G-CSF, which could be demonstrated in our study.
Limitations and recommendations
First, although all included studies used random allocation, only a few reported the specific method, which may introduce selection bias. In addition, many studies had unclear descriptions of double-blinding or blinding during outcome assessments, which could lead to performance and detection bias. However, it may be difficult to implement blinding of participants in clinical trials.
Second, there was poor consistency between the selection of acupoints and the chemotherapy regimens, doses, duration, and center setting among the included studies, resulting in heterogeneity in the meta-analysis. As a result, the validity of this study may be significantly undermined, and caution should be exercised when interpreting the results. Given the unclear risk of bias in the methodology of many included studies, additional high-quality and rigorous trials are needed.
Lastly, the effect was assessed by very few studies in many cases, and many of the studies suffered from methodological bias, which could threaten the validity of the meta-analyses. Therefore, conclusions drawn from these results should be made with caution.
Conclusions
This meta-analysis of acupuncture effects on chemotherapy-induced bone marrow suppression pooled together existing data of 25 relevant studies. Analysis of the pooled data with a random-effects model showed that chemotherapy-induced bone marrow suppression was relieved by acupuncture. The levels of G-CSF, WBC, neutrophil, ANC, Hb, platelet, and NK cell were increased significantly by acupuncture with cancer patients during chemotherapy.
In addition, despite acupuncture modalities, the levels of WBCs, platelets, and NK cells increased in a cumulative-time manner. These findings are actionable and provide for patients suffering from chemotherapy-related immunosuppression.
Footnotes
Authors' Contributions
The authors' roles in this project were as follows: Y.W.S. and H.T.T. contributed to the conceptualization, Y.W.S., M.H.W., and Y.A.R. were responsible for the methodology, including screening papers for eligibility, appraising study quality, extracting data, and seeking additional information. Y.A.R. worked on software, and C.W.C. conducted validation. Y.W.S. performed formal analysis, whereas Y.W.S., C.W.C., K.A.M., and H.T.T. contributed to the writing of the original draft, and Y.W.S., C.W.C., K.A.M., and H.T.T. participated in the writing-review and editing process. H.T.T. provided supervision. All authors have read and approved the manuscript's published version.
Availability of Data and Materials
Upon reasonable request, the corresponding author can grant access to all the data that were collected and analyzed during the study.
Ethics Approval and Consent to Participate
Not applicable.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by grant nos. MOST 109-2314-B-038-110-, MOST 110-2314-B-038-081-MY3 from the Ministry of Science and Technology, Taiwan, and The National Taipei University of Nursing and Health Sciences (111ntunhs-NT-01). The study design, data collection, data analysis, decision to publish, and manuscript preparation were not influenced by the funders.
Supplementary Material
Supplementary Data S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.