
Abstract
Objective:
This meta-analysis evaluated the beneficial and potential adverse effects of Astragalus in the treatment of patients with type 2 diabetes mellitus (T2DM).
Methods:
The authors searched for randomized controlled trials of Astragalus treatment for patients with T2DM in the following databases: PubMed, Embase, Cochrane Library, China Knowledge Resource Integrated Database (CNKI), Wanfang Data, China Science and Technology Journal Database (CQVIP), and SinoMed. Two reviewers conducted independent selection of studies, data extraction, and coding, as well as the assessment of risk of bias in the studies included. Standard meta-analysis and, if appropriate, meta-regression were performed using the STATA, v.15.1, software.
Results:
This meta-analysis encompasses 20 studies and a total of 953 participants. Compared to the control group (CG), the observation group (OG) decreased fasting plasma glucose (FPG) (WMD = −0.67, 95% CI: −1.13∼−0.20, P = 0.005), 2 hours postprandial plasma glucose (2hPG) (WMD = −0.67 (95% CI: −1.13∼−0.20, P=0.005), glycated hemoglobin A1C (HbA1c) (WMD = −0.93, 95% CI: −1.22∼−0.64, P = 0.000), homeostatic model assessment for insulin resistance (HOMA-IR) (WMD = −0.45, 95% CI: −0.99∼0.99, P = 0.104), insulin sensitive index (WMD = 0.42, 95% CI: 0.13-0.72, P = 0.004). The total effective ratio of the OG is more effective than CG (RR = 1.33, 95% CI: 1.26-1.40, P = 0.000), the significant effective ratio (RR = 1.69, 95% CI: 1.48-1.93, P = 0.000).
Conclusions:
Astragalus may provide specific benefits for T2DM patients as an adjuvant treatment. Nonetheless, the certainty of the evidence and risk of bias fell short of optimal performance, indicating the need for additional clinical research to ascertain potential effects.
PROSPERO REGISTRATION NUMBER CRD42022338491.
Introduction
In Traditional Chinese Medicine, “Xiao Ke” refers to a syndrome that is similar to type 2 diabetes in Western medicine and is characterized by symptoms such as excessive thirst, frequent urination, polyphagia, and weight loss. According to the World Health Organization (WHO), diabetes was responsible for an estimated 1.5 million deaths in 2019. 1
It is noteworthy that diabetes can result in several severe complications such as cardiovascular disease, kidney disease, nerve damage, and blindness. These complications can significantly diminish the quality of life for individuals with diabetes and increase mortality rates. 2 The prevalence of diabetes in China has been increasing rapidly in recent years due to factors such as urbanization, changes in lifestyle behaviors, and an aging population.
As of 2020, it is estimated that 92.4 million people in China have diabetes and more than 90% of them suffer from type 2 diabetes. 2 Type 2 diabetes mellitus (T2DM) causes severe physical and psychological suffering for patients and their families and has led to a growing burden of diabetes-related complications and health care costs. 2 Therefore, it is important to prevent the growing epidemic and its impact on public health.
T2DM is a chronic condition affecting how the body processes glucose. 3 In this condition, the body either exhibits resistance to insulin's effects or fails to generate enough insulin to sustain standard glucose levels. 3 Over an extended period, elevated blood sugar levels can result in harm to the nerves, blood vessels, and organs. 4 T2DM is often associated not only with obesity, lack of physical activity, and poor diet but genetic and environmental factors also contribute to its development. 5
Symptoms of T2DM include increased thirst, frequent urination, fatigue, blurred vision, slow healing wounds, and tingling or numbness in the hands or feet. Treatment may include lifestyle changes such as regular exercise and a healthy diet, as well as medications to lower blood sugar levels.
Several types of drugs can be used to treat T2DM. Insulin sensitizers are the most common medications used to treat T2DM, for example, rosiglitazone, DPP-4 inhibitors, 6 SGLT2 inhibitors, 7 sulfonylurea, and metformin. 2,3,8 Although they effectively slow the progression of T2DM, these drugs can cause some side effects. Some common side effects of these drugs may include gastrointestinal symptoms, hypoglycemia, and increased risk of heart failure and bone fractures. 9 –12
Astragalus is an herb that has been used for centuries in Traditional Chinese Medicine to treat diabetes. In the Western Han Dynasty (206
In addition, it could potentially lower the risk of diabetes-related complications, including heart disease and kidney disease. 17 However, the exact active ingredients of Astragalus and its mechanisms for improving diabetes have not been fully understood. Therefore, the authors performed a meta-analysis on the available literature to assess the effectiveness and safety of Astragalus for treating patients with T2DM.
Methods
Protocol and registration
This meta-analysis has been registered in PROSPERO with registration number CRD42022338491.
Eligibility criteria
All published randomized controlled trials (RCTs) and semi-RCTs concerning the treatment of patients with T2DM using Astragalus were included. The publication language was limited to Chinese or English.
Inclusion criteria
All RCTs that assessed the effectiveness of Astragalus in treating T2DM were incorporated into the analysis.
Studies where all patients met the criteria of the WHO or American Diabetes Association for the diagnosis of T2DM.
Studies where the control group (CG) was treated with metformin for T2DM, while the observation group (OG) was treated with Astragalus on the basis of the CG.
Studies where the publication language was limited to Chinese or English.
Exclusion criteria
Duplicate publications.
Studies that lacked complete text or insufficiently described the clinical outcomes were excluded from the analysis.
Studies where the definition of exposure is quite different from most literature.
Studies with animal experiments.
Case reports.
Reviews or systematic review articles.
Search strategy
The authors searched multiple databases, including PubMed (
Data extraction
Two researchers conducted the literature search, screening, and data extraction independently. Any inconsistencies between the published versions were identified and highlighted.
Disagreements between authors were resolved through reaching a consensus or by seeking the input of a third author. For each included article, two types of data were extracted: (1) the essential characteristics of the studies, including author, publication year, type of intervention, sample size, sex, age, intervention measures, and outcome measures; and (2) the original data related to outcome indicators, such as significant efficiency ratio, total efficiency ratio, fasting blood glucose (FBG), 2-h postprandial plasma glucose (2hPG), glycosylated hemoglobin (HbA1c), homeostasis model assessment of insulin resistance (HOMA-IR), homeostasis model assessment of β-cell function (HOMA-β), homeostasis model assessment of insulin sensitivity, and any instances of side effect events.
Quality assessment
Results of this meta-analysis were presented in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines.
Two independent researchers evaluated the following items using the Review Manager 5.3 risk of bias assessment tool 18 : (1) random sequence generation (selection bias); (2) allocation concealment (selection bias); (3) blinding of participants and personnel (performance bias); (4) blinding of outcome assessment (detection bias); (5) incomplete outcome data (attrition bias); (6) free of selective outcome reporting (reporting bias); and (7) other problems that could have led to study bias (other bias).
Statistical methods
The STATA 15.1 software was used for data analysis. Relative ratio (RR) was used to evaluate differences in dichotomous data, and weighted mean difference (WMD) was used to evaluate the difference between continuous indicators, with 95% confidence intervals (CIs). I 2 was used to evaluate heterogeneity. If the heterogeneity test yielded a p-value of ≥0.1 and I 2 value of ≤50%, it suggested that the studies were homogeneous, and a fixed-effects model was employed for the combined analysis.
However, if the p-value was <0.1 and I 2 value was >50%, it indicated substantial heterogeneity, and a sensitivity analysis or subgroup analysis was conducted to identify the source of heterogeneity. If significant heterogeneity persisted, a random-effects model was used and the results were discarded, followed by a descriptive analysis. To assess the publication bias of each indicator, a funnel plot and Egger's bias test were utilized.
Results
Study selection
A total of 1587 articles were retrieved by conducting a search across various databases, including PubMed, Embase, Cochrane Library, CNKI, Wanfang Data, CQVIP, and SinoMed. After excluding duplicates, 867 articles remained. By further browsing through article abstracts, 722 articles were selected. Finally, 20 articles with full text were used for the meta-analysis (Fig. 1).
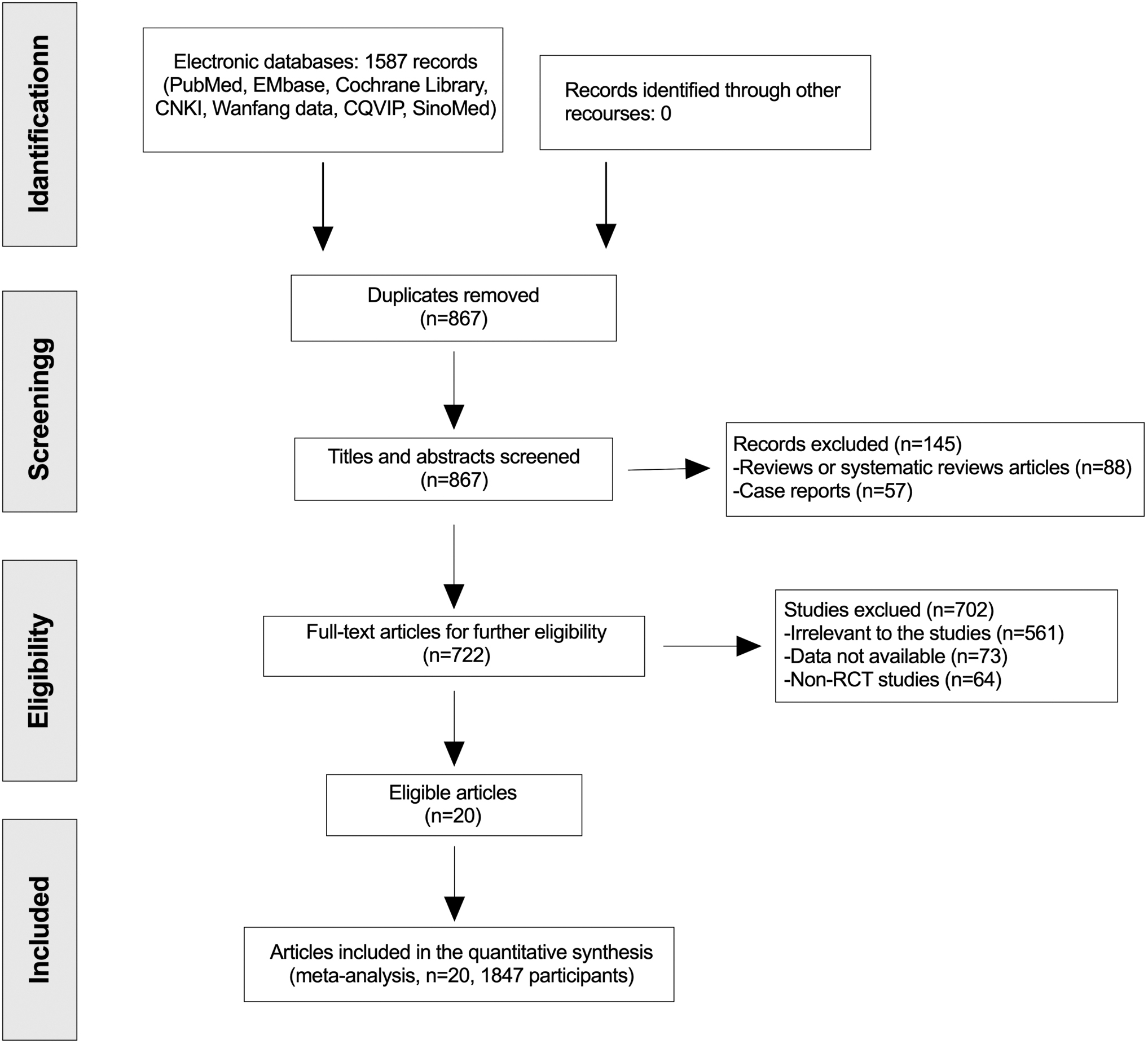
Flow diagram of the study design.
Basic information of included literature and evaluation of literature quality
Basic information
Twenty articles were included in this study, seven of which were RCTs. There were 953 patients in the experimental group and 894 patients in the CG. The CG was treated with metformin for type 2 diabetes, while the OG was treated with Astragalus on the basis of the CG. The dosage of Astragalus was between 10 and 50 g (Table 1).
Characteristics of the Studies Included in the Meta-Analysis of Type 2 Diabetes Mellitus
CG, control group.
Methodological quality of included studies
In this study, two studies were found to have a high risk of performance bias, three studies had a high risk of attrition bias, and four studies had a high risk of other bias. All other biases were assessed as low risk. All studies were assessed according to the risk of bias 2.0 tool (Figs. 2 and 3).
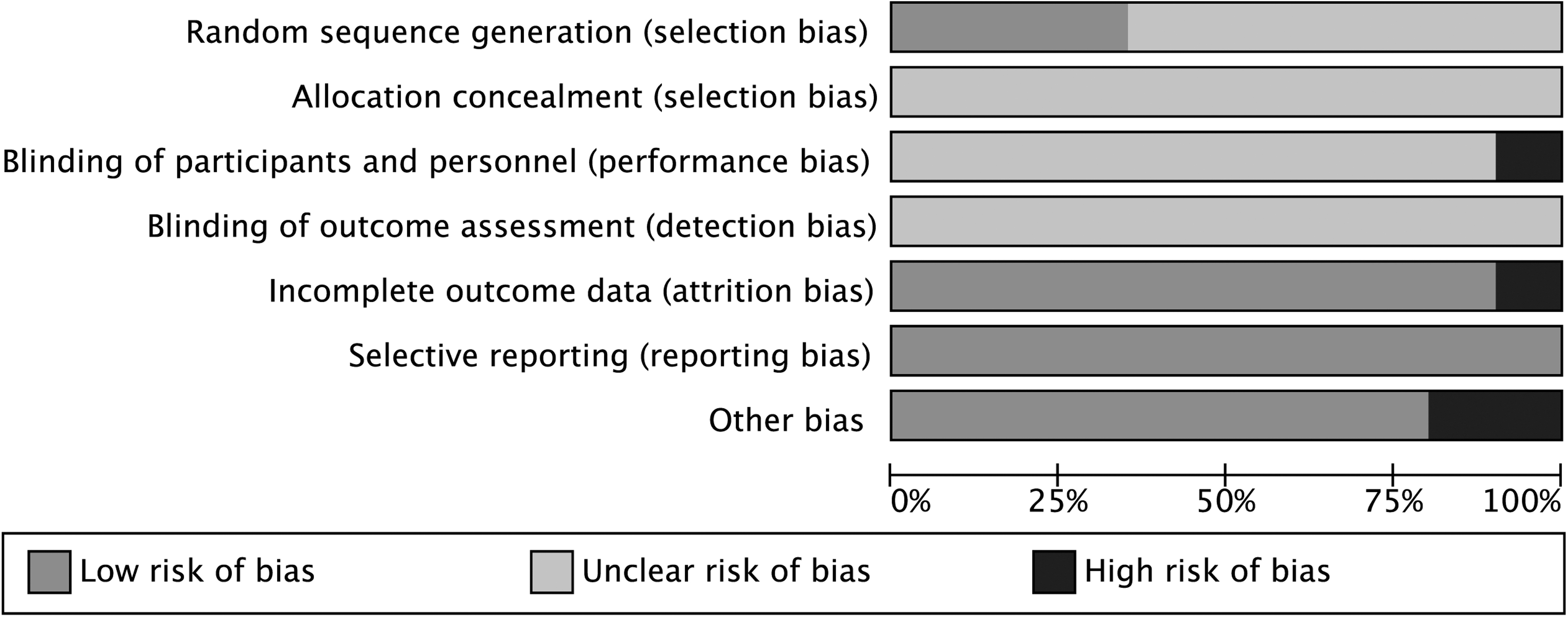
Summary of quality assessment items.

Risk of bias summary: authors' judgment about each risk of bias item for each included study. Low risk of bias;  unclear risk of bias; and
unclear risk of bias; and  high risk of bias.
high risk of bias.
Results of included studies
Total effective ratio
A total of 17 articles were included in this study. Since there was no significant heterogeneity (I 2 = 0.0%, p = 0.597), the study used a fixed-effects model to combine effect sizes. The pooled results yielded an RR of 1.33 (95% CI: 1.26 to 1.40, p = 0.000), and the results indicated that the total efficiency ratio of OG was higher than CG in T2DM (Fig. 4).

Total efficiency of Astragalus in patients with T2DM. T2DM, type 2 diabetes mellitus.
Significant effective ratio
A total of 17 articles were included in this study. Since there was no significant heterogeneity (I 2 = 0.0%, p = 0.597), the study used a fixed-effects model to combine effect sizes. The pooled results yielded an RR of 1.69 (95% CI: 1.48 to 1.93, p = 0.000), and results indicated that the total efficiency ratio of treatment with Astragalus combined with metformin was higher than with metformin in T2DM (Figs. 4 and 5).
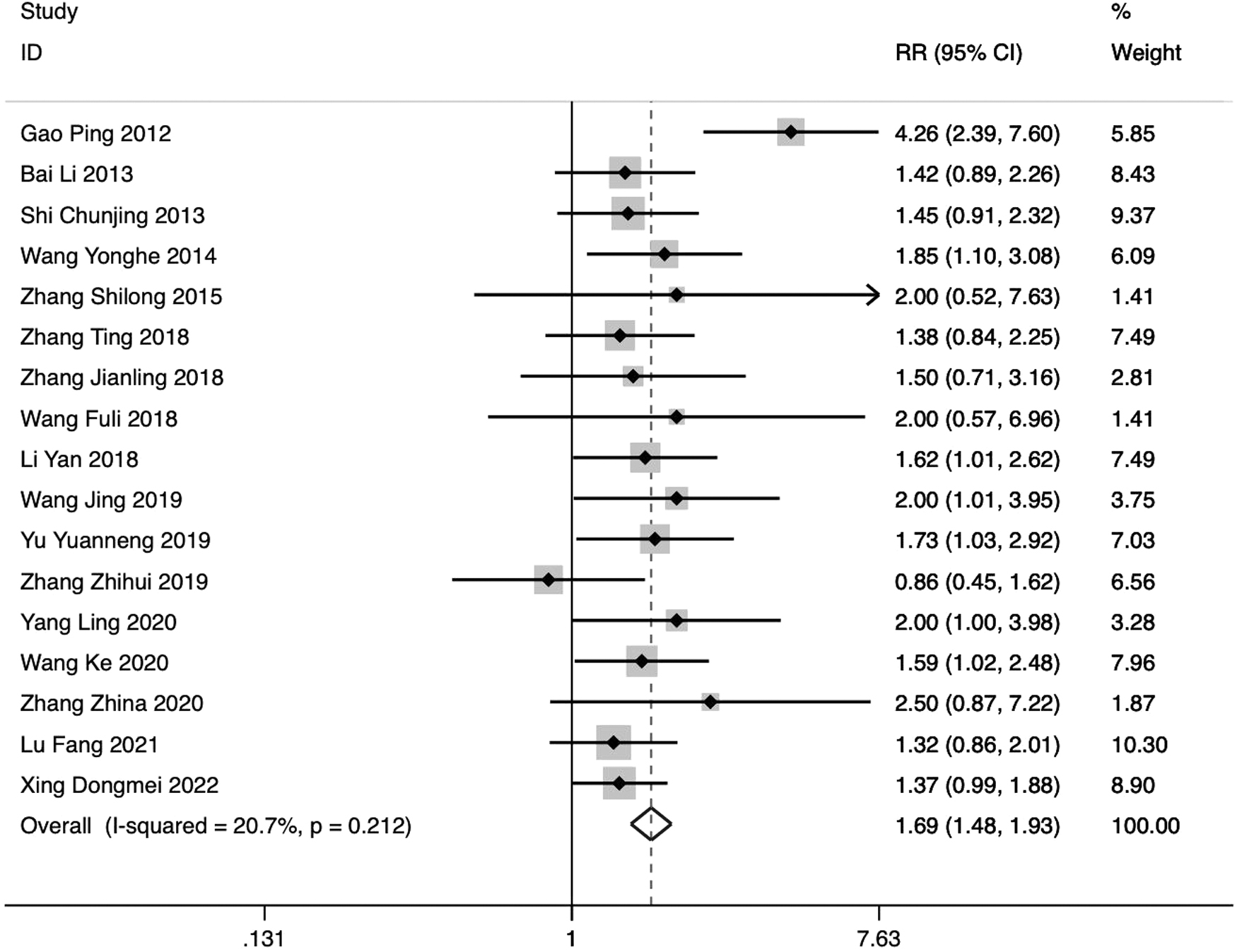
Significant effective ratio of Astragalus in patients with T2DM.
Fasting blood glucose
FBG is determined by measuring the blood glucose level in a plasma sample taken before breakfast, following an overnight fast of at least 8–10 h (excluding water). This test can reflect the function of pancreatic islet B cells and typically indicates the secretion function of basal insulin. It is the most frequently used test for diabetes. 2 A total of 14 articles were included in this study. Due to significant heterogeneity (I 2 = 95.2%, p = 0.000), the study used a random-effects model to combine effect sizes.
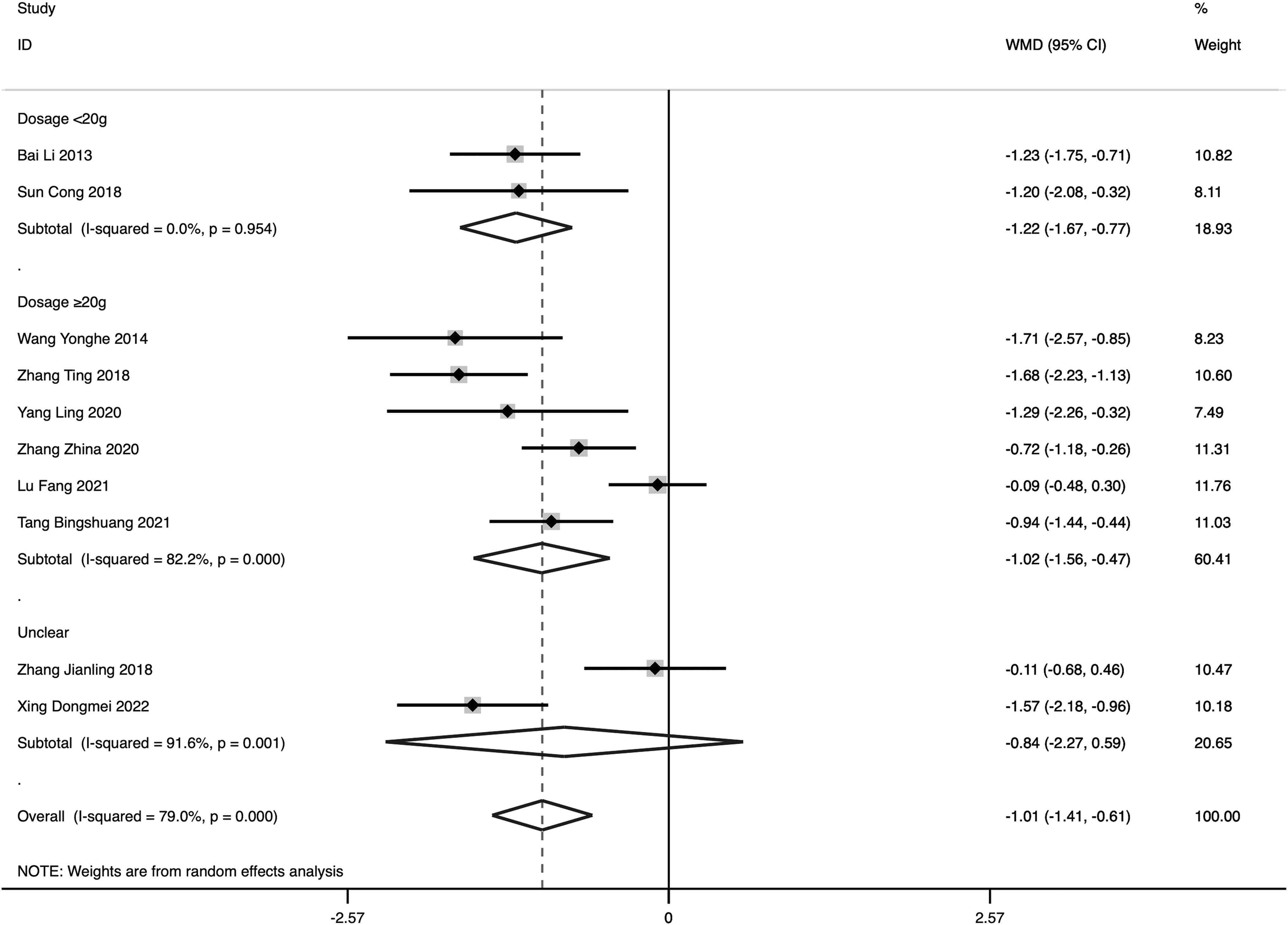
The pooled result yielded a WMD of −0.67 (95% CI: −1.13 to −0.20, p = 0.005) (Fig. 6). Studies were also divided based on dosage of Astragalus into the high-dose group (≥20 g) and low-dose group (<20 g) and a subgroup analysis was performed. Results of the subgroup analysis showed that heterogeneity of the low-dose group was significantly reduced (I 2 = 8.9%, p = 0.295), suggesting that the difference in doses of Astragalus among different studies was the source of heterogeneity (Fig. 7).
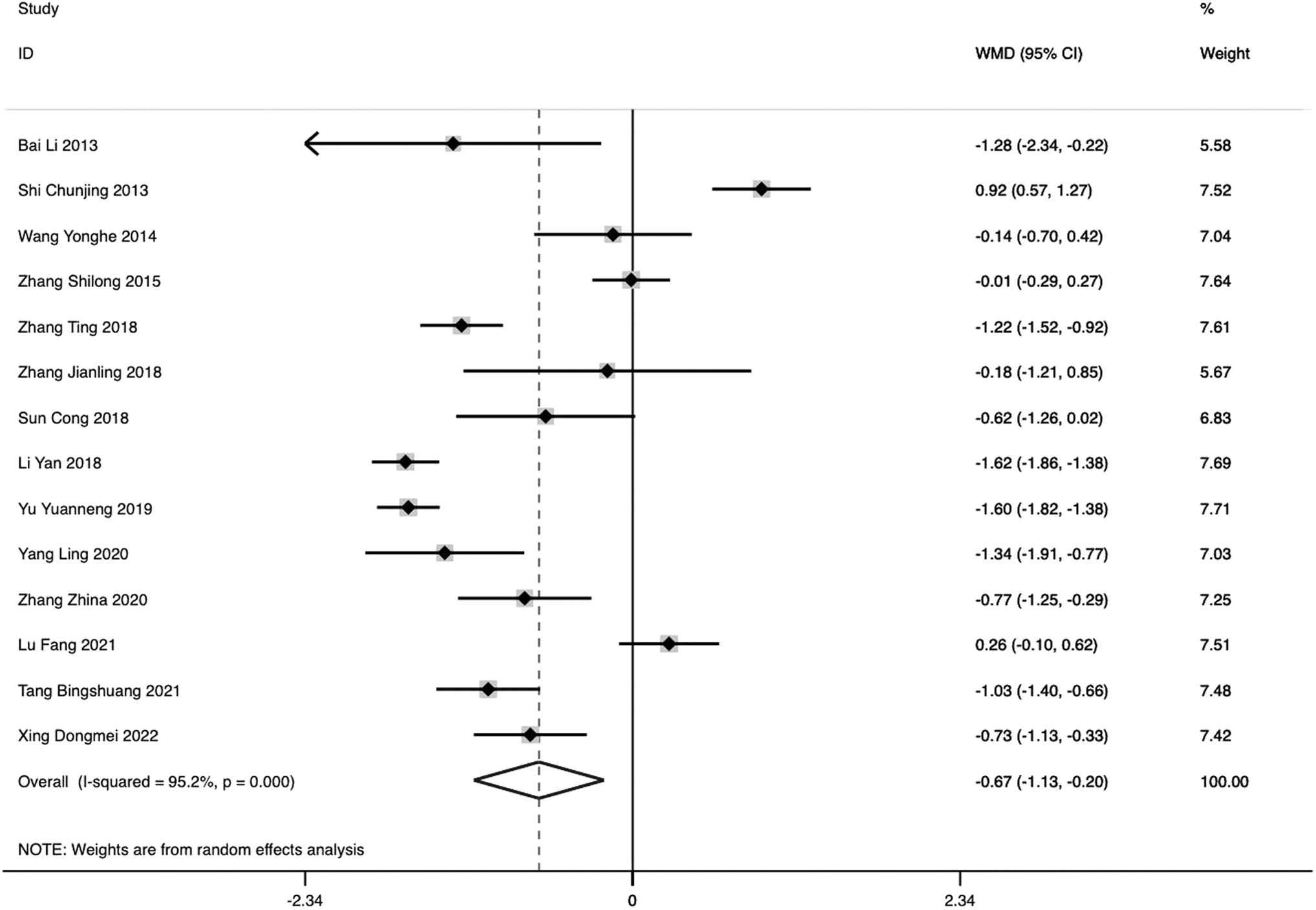
The impact of Astragalus on FPG levels in patients with T2DM. FPG, fasting plasma glucose; WMD, weighted mean difference.

Subgroup analyses of the impact of dosage of Astragalus on FPG in patients with T2DM.
The authors categorized the studies into distinct subgroups, based on the FBG level, as high-level (≥11.1 mmol/L), medium-level (7.0–8.4 mmol/L), and low-level (8.4–11.1 mmol/L) groups. Results of the study showed that Astragalus had a more significant effect on the high FBG-level group (Fig. 8). The results showed that the FBG level in the OG was significantly lower compared with the CG, which revealed that Astragalus combined with metformin can effectively treat T2DM.
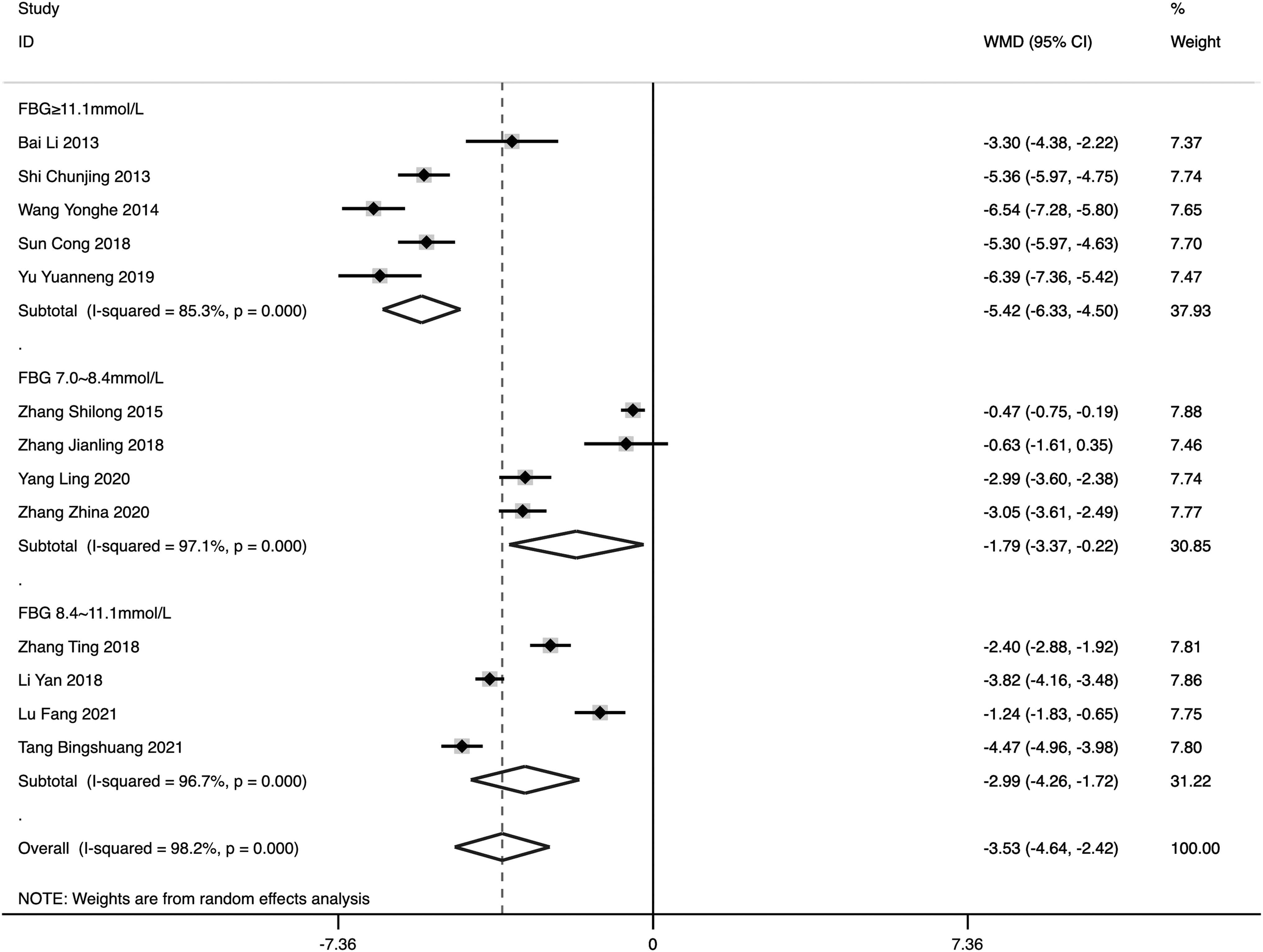
Subgroup analyses of different FBG levels in patients with T2DM. FBG, fasting blood glucose.
Two-hour postprandial plasma glucose
2hPG is the glucose value measured within 2 h after eating. In clinical practice, it can reflect insulin secretion and the body's sensitivity to insulin to a certain extent and is the most common method to screen and detect diabetic patients with normal fasting glucose. A total of 10 articles were included in this study. As the heterogeneity was found to be significant (I 2 = 95.2%, p = 0.000), a random-effects model was employed to combine the effect sizes in this study.
The pooled result yielded a WMD of −0.67 (95% CI: −1.13 to −0.20, p = 0.005), and results indicated that the 2hPG level was significantly lower in the OG compared with the CG (Fig. 9). The results of the subgroup analysis showed that the heterogeneity of the low-dose group was significantly reduced (I 2 = 8.9%, p = 0.295), suggesting that the difference in doses of Astragalus among different studies was the source of heterogeneity (Fig. 10).
The impact of Astragalus on 2hPG levels in patients with type T2DM. 2hPG, 2-h postprandial plasma glucose.
Subgroup analyses of the impact of Astragalus on 2hPG levels in patients with T2DM.
Glycated hemoglobin
In 2011, the WHO recommended the use of HbA1c for the diagnosis of diabetes in countries and regions where it is available. A reduction in HbA1c levels is strongly associated with reduction in microvascular complications in patients with diabetes, and a reduction in HbA1c from 10% to 9% has a greater impact on reducing the risk of complications than a reduction from 7% to 6%. A total of six articles were included in this study.
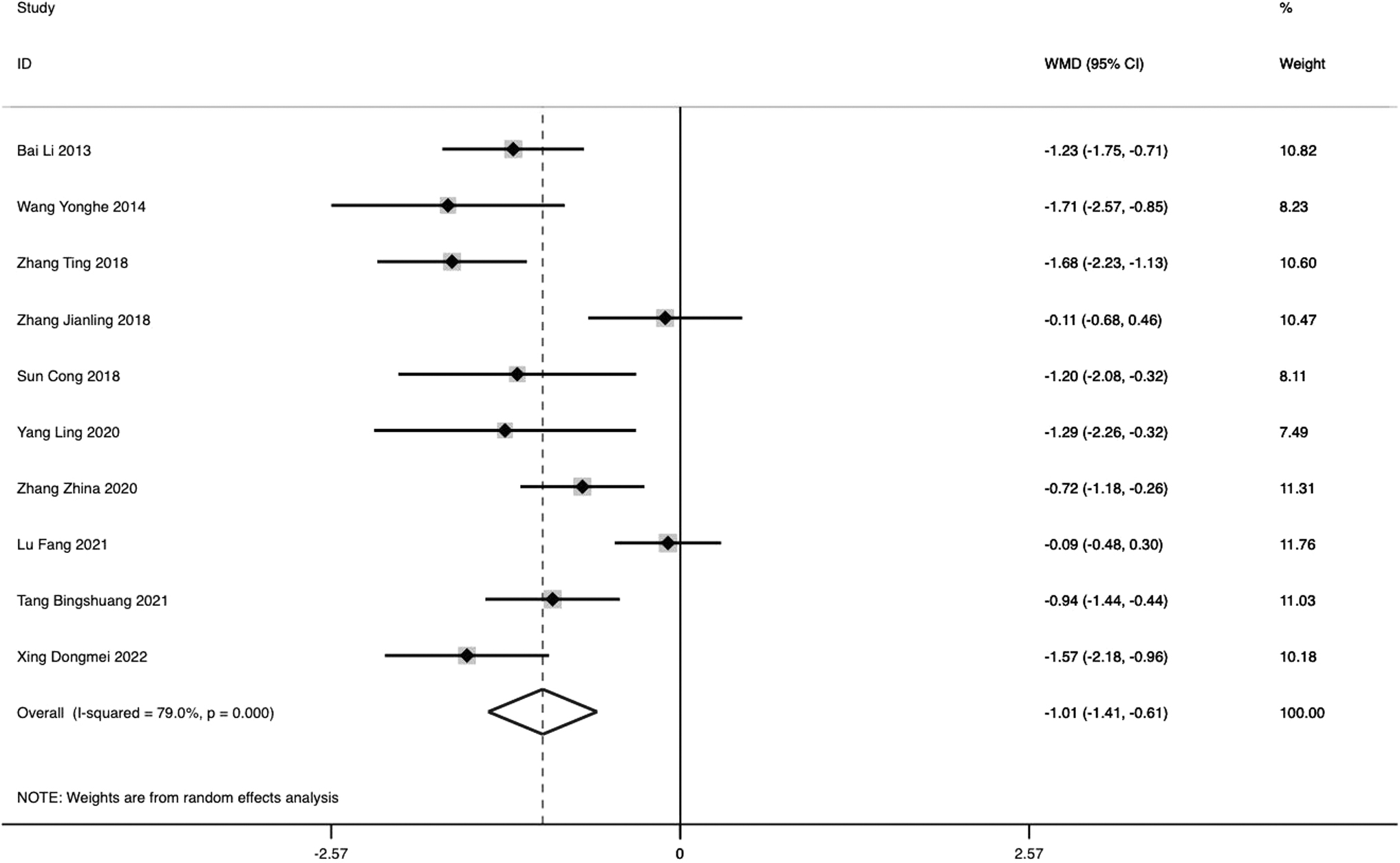
As significant heterogeneity was observed (I 2 = 77.0%, p = 0.000), a random-effects model was employed to combine the effect sizes in this study. The pooled result yielded a WMD of −0.93 (95% CI: −1.22 to −0.64, p = 0.000), and results indicated that the total efficiency ratio of treatment with Astragalus combined with metformin was higher than with metformin in T2DM (Fig. 11). Despite conducting a sensitivity analysis, the authors were unable to identify any data outliers.
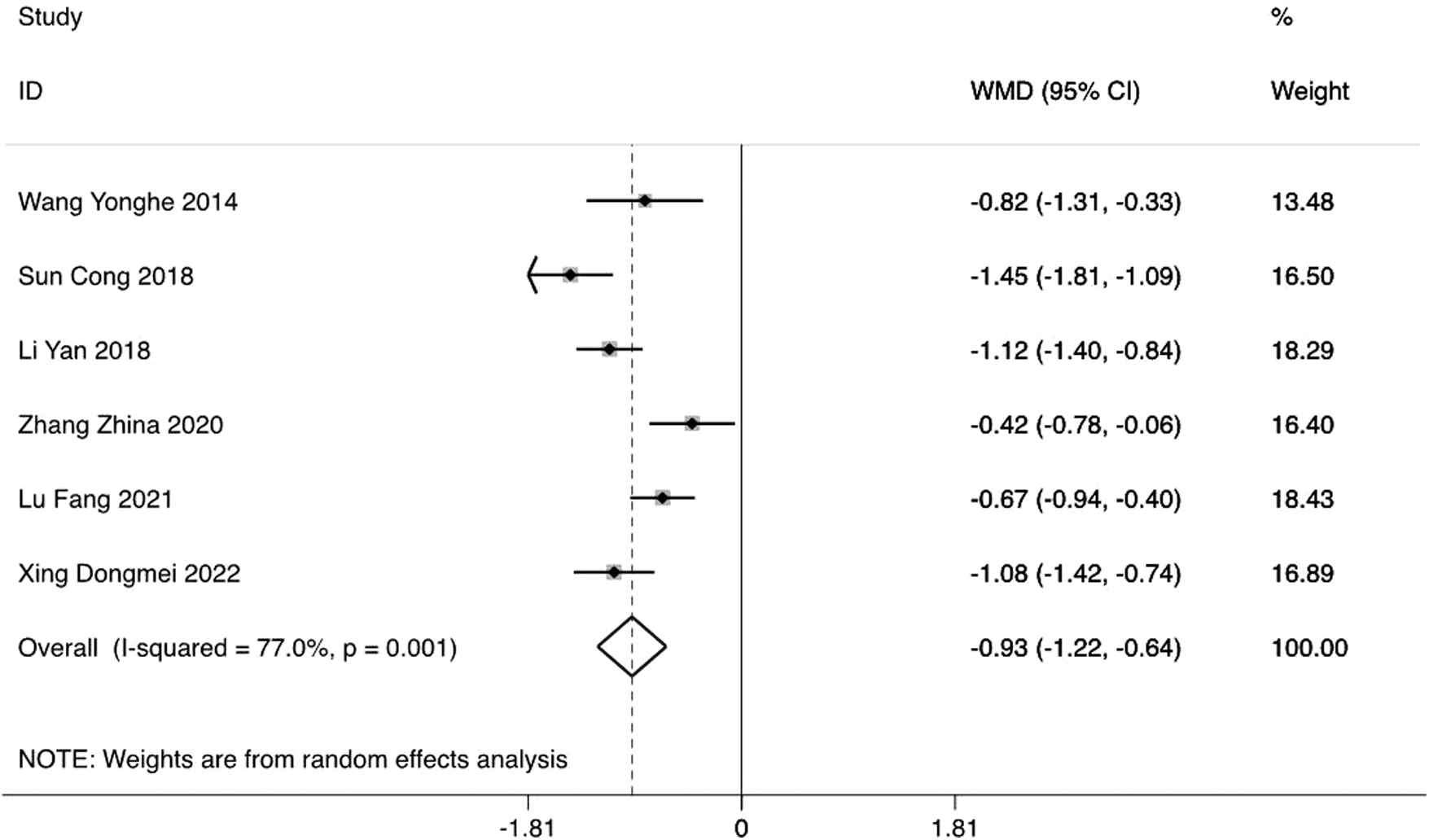
The impact of Astragalus on HbA1c levels in patients with T2DM. HbA1c, glycated hemoglobin.
Homeostatic model assessment for insulin resistance
The homeostasis model assessment (HOMA) is a technique used to measure β-cell function and insulin resistance (IR) based on fasting glucose and insulin or C-peptide concentrations. 19,20 HOMA-IR was calculated using the following formula: fasting insulin (microU/L) × fasting glucose (nmol/L)/22.5. 21 –23
Currently, there is no universally accepted criterion for the normal range of HOMA-IR. However, the upper limit of HOMA-IR varies across different populations and typically falls between 2 and 3. 24 –26 In southern Chinese populations, HOMA-IR cutoffs of 1.4 and 2.0 were found to effectively distinguish dysglycemia and T2DM from normal glucose tolerance. 26 A total of four articles were included in this study.
As significant heterogeneity was observed (I 2 = 89.0%, p = 0.000), a random-effects model was employed to combine the effect sizes in this study. The pooled result yielded a WMD of −0.45 (95% CI: −0.99 to 0.99, p = 0.104). Despite conducting a sensitivity analysis, the authors could not identify any data outliers.
β-Cell dysfunction index
A wealth of information is available regarding the impact of treatment on β-cell function. Lifestyle modification 27 using hypoglycemic drugs such as metformin, rosiglitazone, 28,29 sulfonylureas, 28 glinides, 30 GLP-1 receptor agonists, 31 dipeptidyl peptidase-4 inhibitors, 32 sodium–glucose cotransporter-2 inhibitors, 33 and insulin injection, 34,35 can improve glucose sensitivity of beta cells. This research found that the β-cell dysfunction index of treatment with Astragalus combined with metformin was higher than with metformin in T2DM.
As there was no significant heterogeneity (I 2 = 36.6%, p = 0.209), the study used a fixed-effects model to combine effect sizes. The pooled results yielded a WMD of 11.72 (95% CI: 8.75–14.69, p = 0.000).
Insulin sensitivity index
The insulin sensitivity index is currently regarded as a feasible noninvasive method for assessing systemic insulin resistance and is suitable for clinical use. One of the causes of T2DM is low insulin secretion and the other is low insulin sensitivity. When there is adequate insulin secretion, enhancing insulin sensitivity is considered a priority approach for treating diabetes. 36
This research found that the insulin sensitivity index of treatment with Astragalus combined with metformin was higher than with metformin in T2DM. As no significant heterogeneity was detected (I 2 = 86.2%, p = 0.007), a fixed-effects model was utilized to combine the effect sizes in this study. The pooled results yielded a WMD of 0.42 (95% CI: 0.13 to 0.72, p = 0.004).
Side effects
However, there are few reports of side effects of Astragalus. Side effects of Astragalus are uncommon and mild and mainly include rash, itching, nasal symptoms, or stomach upset. A total of 21 side effect cases occurred in 5 studies. Unfortunately, the authors could not conduct a systematic review of adverse reactions due to the lack of reports of severe side effects in clinical trials.
The results show that RR = 1.69 (I 2 = 1.3%, p = 0.399; 95% CI: 1.48 to 1.93, p = 0.000), which indicates that there is no statistical significance (Fig. 12).

Forest plot of the meta-analysis of side effects.
Publication bias
It can be seen from the funnel plots that the total effective rates of the treatment group and CG appear to be slightly asymmetrical, and the results of Egger's test indicate the possibility of publication bias in this study (p = 0.018 < 0.05). The funnel plots of the significant efficiency ratio, FBG, HbA1c, and side effects are almost symmetrical, and Egger's test results indicate no significant publication bias in these studies.
Discussion
Summary of main results
In this meta-analysis, the authors evaluated the efficacy and safety of Astragalus, a Traditional Chinese Medicine commonly used for treating T2DM, by analyzing 20 studies that involved 1847 participants. However, the available evidence on its efficacy and safety remains inadequate. The results indicate that Astragalus significantly reduced fasting plasma glucose (FPG), 2hPG, and HbA1c in patients with T2DM compared with CGs when used as adjuvant therapy.
Recent studies on blood glucose management have shown that using oral hypoglycemic agents as needed can reduce the incidence of macrovascular and microvascular disease. 37 –39 Based on current evidence, Astragalus may provide significant benefits as a complementary therapy for individuals with T2DM. It may help regulate blood glucose levels and potentially prevent the onset or progression of long-term complications associated with the condition.
Heterogeneity
The average age of patients in this study ranged from 30 to 77 years. The specific intervention strategy adopted by the CG was metformin. Moreover, the heterogeneity observed in this meta-analysis may be attributed to variations in the dosage and duration of treatment, the undefined risk of bias resulting from the concealment and blinding of patient allocation, and the absence of detailed reports regarding patient characteristics such as BMI.
However, some individuals might show more significant improvement than others. Due to the limited number of studies included in the analysis and the stratification of factors, the authors conducted a subgroup meta-analysis based on the treatment paradigm to reduce the risk of false positives as this factor is more likely to impact clinical outcomes. To derive more conclusive findings on the efficacy of Astragalus as a supplementary therapy for T2DM, it is imperative to incorporate additional clinical trials.
Given the current heterogeneity observed between studies, the authors could only arrive at preliminary conclusions, and a more comprehensive analysis could yield more conclusive results. The sensitivity analysis did not identify any outliers, and the outcomes indicated that none of the study results had a significant impact on the results of this meta-analysis, demonstrating the stability and reliability of the study's findings.
Potential bias
Publication bias may occur when studies with positive results are more likely to be published than those with negative results, leading to an overestimation of the effect size. Aside from the possibility of unclear bias in this study, the results of Egger's linear regression test (p > 0.05) did not suggest any statistical publication bias in this meta-analysis. Thus, the heterogeneity among the studies included in this analysis may underlie the observed asymmetry in the funnel plot.
Limitations
It is important to consider the limitations of the available evidence. While all the studies included in the analysis were purported to have a randomized controlled design, some of them lacked clear descriptions of their randomization, allocation concealment, and blinding procedures. Furthermore, the lack of specific clinical details hinders a comprehensive evaluation of the safety of Astragalus injection in the treatment of T2DM despite the existence of evidence suggesting adverse clinical reactions primarily associated with its use. 40 –42
Meanwhile, the search was constrained by language limitations as only Chinese and English databases were searched, and all of the studies included in this analysis were conducted in China. This may have implications for the generalizability of the findings. Consequently, the applicability of this evidence to other countries is uncertain.
Finally, the relatively small sample size for some indicators leads to poor statistical performance. In addition, due to the limited quality of existing research, its applicability may be limited.
Conclusions
The present evidence suggests that Astragalus may offer unique advantages as an adjuvant treatment for T2DM, potentially leading to reductions in FPG, 2hPG, HbA1c, and HOMA-IR and supporting blood glucose control in T2DM patients. Nevertheless, the validity of this conclusion is weakened by the presence of an indistinct risk of bias across the included studies. Therefore, this is a preliminary study.
To confirm the clinical efficacy and safety of Astragalus as an adjunctive therapy for T2DM, more rigorous RCTs are needed in the future, with large sample sizes, strict protocols, and multiple centers.
Therefore, it is recommended that future RCTs on the treatment of T2DM by combining Astragalus should pay more attention to improving the methodological quality by clearly describing the specific details of random assignment, allocation concealment, and blinded subjects; paying attention to the incidence of adverse effects, adequate extension of follow-up time, and documentation of the prognosis of T2DM; and standardizing clinical reporting to provide better evidence-based medical evidence for the subsequent clinical use of Astragalus in the treatment of T2DM.
Footnotes
Authors' Contributions
Y.-H.X. and D.-K.G. conceived and designed this study. K.-F.H. and P.-Y.L. performed the data extraction, analysis, and interpretation and wrote the initial draft. W.Z. assisted with data extraction and interpretation.
Author Disclosure Statement
The authors declare that there are no conflicts of interest regarding the publication of this article.
Funding Information
This work was supported by the Science and Technology Development Fund of Macau (File No.: 0055/2019/AMJ) and the National Key R&D Program of China (MOST: 2019YFE0110500).
Supplementary Material
Supplementary Table S1
Supplemental Data
PRISMA_2020_checklist.docx
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.